The Biological Responses to Magnesium-Based Biodegradable Medical Devices


1
National Science Foundation-Engineering Research Center for Revolutionizing Metallic Biomaterials, North Carolina Agricultural and Technical State University, Greensboro, NC 27401, USA
2
FIT BEST Laboratory, Department of Chemical, Biological, and Bioengineering, North Carolina Agricultural and Technical State University, Greensboro, NC 27401, USA
3
Department of Anesthesiology, School of Medicine, Yale University, New Haven, CT 06519, USA
*
Author to whom correspondence should be addressed.
Metals 2017, 7(11), 514; https://doi.org/10.3390/met7110514
Submission received: 20 September 2017
/
Revised: 16 November 2017
/
Accepted: 18 November 2017
/
Published: 21 November 2017
(This article belongs to the Special Issue Biodegradable Metals)
Abstract
:The biocompatibility of Magnesium-based materials (MBMs) is critical to the safety of biodegradable medical devices. As a promising metallic biomaterial for medical devices, the issue of greatest concern is devices’ safety as degrading products are possibly interacting with local tissue during complete degradation. The aim of this review is to summarize the biological responses to MBMs at the cellular/molecular level, including cell adhesion, transportation signaling, immune response, and tissue growth during the complex degradation process. We review the influence of MBMs on gene/protein biosynthesis and expression at the site of implantation, as well as throughout the body. This paper provides a systematic review of the cellular/molecular behavior of local tissue on the response to Mg degradation, which may facilitate a better prediction of long-term degradation and the safe use of magnesium-based implants through metal innovation.
1. Introduction
The degradability of magnesium-based materials (MBMs) makes these biomaterials a great choice for clinical devices, especially for orthopedic and cardiovascular applications. The biocompatibility of MBM refers to their ability to interact with the body organic tissues without causing an unacceptable degree of harm. From a biological perspective, human tissue can not only tolerate, but can even benefit from the interaction with MBM implants by proper responses. On the other hand, the interaction between MBMs and organic tissue in vivo has also been shown to cause phenomena that are not observed in vitro. In an aqueous environment, whether that be organic tissue or in vitro cell culture, Mg reacts with water, generating magnesium hydroxide (Mg(OH)2) and molecular hydrogen (H2). The biological responses of Mg-based materials have been studied both in vivo and in vitro [1,2,3,4,5]. In vivo, MBM implantation results in the formation of gas pockets in tissue containing different concentrations of H2, O2, CO2, and/or N2; a high deposition of calcium phosphate (Ca-P), which acts as a mineral layer between tissue and MBM implants; and an increase in the local pH of body fluid [2,6,7,8]. In contrast, there is no formation of gas pockets in vitro since it is freely released, while in vivo, the gas pockets are trapped by local tissue. Instead, molecular hydrogen escapes to the atmosphere, and cell-adhesion behavior on the surface of MBM implants indicates biocompatibility [1,3]. As a product of MBM corrosion, H2 was also found to be a potential antioxidant that is involved in cell signaling and has a novel role in preventive and therapeutic applications [9,10,11]. Furthermore, the Ca-P mineral layer that is associated with magnesium can promote osteoinductivity and osteoconductivity, which aids in the biocompatibility of magnesium alloys as a bone regenerative material [12]. The increase in pH has a positive correlation in hemoglobin picking up oxygen in the blood based on the Bohr effect and a negative correlation in cell-mediated bone resorption by rat osteoclasts in vitro [13,14]. To better understand the biological response to MBMs both in vivo and in vitro, the mechanism of these phenomena should be investigated on the molecular/cellular level.
Like many non-degradable biomaterials, the surface of MBMs is adhered to via protein integrins (heterodimeric receptors in the cell membrane) from the extracellular matrix, within nanoseconds after contact with tissue. Integrins are also involved in intracellular signaling and thus participate in a diverse range of cell functions [15,16,17]. For cardiovascular applications, MBMs are subject to the Vroman effect, which is exhibited by the absorption of blood serum proteins to the biomaterial surface [18]. However, unlike non-degradable biomaterials, at the time of protein adhesion, Mg reacts with the aqueous environment to generate hydrogen gas (H2) and Mg(OH)2, thus increasing the concentration of Mg2+. It is known that the physiologically active form of Mg2+ serves as a catalyst for over 300 enzymes, including those for ATP synthesis, as well as those that use other nucleotides to synthesize DNA and RNA [19]. Both MBMs and permanent biomaterials, such as Titanium-based alloys, are mixed with biocompatible elements (e.g., rear earth, Nb) [20,21]. However, the biological responses to the added elements and the molecular mechanisms that need to be determined by in vitro and in vivo cytotoxicity evaluation.
When MBMs are implanted into the lesion area, a layer of proteins rapidly adsorbs from the blood (or serum). These proteins effectively translate the structure and composition of the foreign surface into biological signals. The signals that are generated by the recognition of the foreign MBM implant are then transmitted from the extracellular environment to the interior of the cell to regulate gene and protein expression; thus, initiating and mediating cellular behaviors like migration, proliferation, differentiation, and apoptosis in different cell types [22,23,24]; in addition to stimulating constructive responses that favor wound healing and tissue integration. This layer of proteins determines the activation of the coagulation cascade, complements system, platelets, and immune cells, and guides their interplay, which results in the formation of a transient provisional matrix and the onset of an inflammatory response from the immune system [25,26]. Further research should be done on this protein layer and its expression profile to better understand its involvement in the biological response to MBMs.
Finally, the immune response leads to an encapsulation of the implants, which also indicates the growth of tissue. The regular foreign body reaction process of encapsulation includes inflammation, granulation and regeneration, and fibrosis. It has been shown that Mg2+ on bioceramic surfaces substantially affects the phenotype of osteogenic cells in vivo and in vitro [27,28,29,30]. A number of studies have demonstrated that Mg2+ plays a critical role in bone remodeling and skeletal development [31]. The mechanism of these phenomena is not yet known, but the function of Mg2+ in protein synthesis and molecular regulation is a possible explanation. Knowing which genes and proteins are expressed differently due to the influence of MBM implants and how these molecules are affected will not only give further insight into the biocompatibility of MBMs, but will also indicate whether MBMs influence other biological functions involving these proteins. This is of great importance to modern MBM implant design, which should make full use of these differentially expressed molecules to improve implant integration [32]. In this article, these molecules from local molecular/cellular response to the degradation of Mg-based alloys are categorized and reviewed based on their involvement in four functions: cell adhesion, transportation signaling, immune response, and tissue growth.
2. Degradation of Mg-Based Alloys
The degradation behavior of MBMs has been studied and reviewed [33,34,35,36]. The mechanism of MBMs degradation involves the reaction of magnesium with its aqueous environment, which produces magnesium hydroxide (Mg(OH)2) and hydrogen gas (H2). A general summary of the corrosion reaction kinetics that takes place is given below [34,37]:
2Mg → 2Mg+ + 2e− (anodic reaction)
2H2O + 2e−→ H2 + 2OH− (cathodic reaction)
2Mg2+ + 2H2O → 2Mg2+ + 2OH− + H2 (chemical reaction)
Mg + 2H2O → Mg2+ + 2OH− + H2 (overall reaction)
Mg2+ + 2OH− → Mg(OH)2 (product formation reaction)
Mg(OH)2 → Mg2+ + 2OH− (product dissolution reaction)
Mg degradation is a dynamic process, including (1) degradation initiation, (2) degradation rate, (3) degradation product formation, (4) the composition of degradation products, (5) removal of the product from flow-induced shear stress, and (6) localized pitting with hydrogen evolution. This complex process is constantly interacting with local tissue, which involves a typical foreign body reaction composed of macrophages and foreign body giant cells formation [38]. A local physiological environment, such as loading and flow affects Mg degradation and finding the most important factors that influence degradation is the key. These dynamic reactions not only produce corrosion products, such as solid Mg(OH)2 and H2 gas, but also generate charged molecules that might affect cellular and molecular responses. For example, it has been studied that responding to different concentrations of Mg2+, osteosarcoma (U2OS) cells have different gene expression related to cell growth, apoptosis, inflammation, and migration [39]. While Mg degrades in the body, the neighboring tissue is expected to regenerate and sustain normal functions. The active interface between degrading MBMs’ surface and regenerating local tissue should be monitored and controlled to address the medical concern of biocompatibility [40].
3. Protein-Mediated Cell Adhesion
The MBM implants enhance the adhesion of surrounding cells that are mediated by proteins in the extracellular matrix. It is known that cell adhesion and morphology influence their proliferation and differentiation [41]. The ability of biomaterials to adsorb the proteins from serum in a favorable conformation determines their ability to support cell adhesion and spreading [42]. The MBMs have this ability, indicating an important aspect of their relative biocompatibility with adjustable biodegradation [43]. For example, α5β1- and β1-integrin were found to mediate cell adhesion to biomaterial surfaces. The expression of α5β1-integrin receptor was increased in human bone-derived cells (HBDC) responding to Mg2+-enriched substrates [44]. It has also been shown that the presence of Mg in bioceramics can significantly increase the expression of β1-, α5β1-, and α3β1-integrins that are vital for osteoblast activity [44,45]. Mg2+ promotes cell adhesion via 5β1- and β1-integrin-associated signal transduction pathways, which are involved in the enhanced activation of the key signaling adaptor protein Shc (Src homology collagen), resulting in the enhanced gene expression of extracellular matrix proteins [46,47]. In our recent studies, we found that platelets have a different adhesion rate on different MBMs surfaces in dynamic conditions [5]. The major platelet integrin αIIbβ3 in relation to MBMs has not been studied. This integrin is required for platelet interactions with proteins in plasma and the extracellular matrices (ECM) that are essential for platelet adhesion and aggregation during hemostasis and arterial thrombosis [48].
Surface chemistry modification with Mg2+ also plays an important role in focal adhesion kinase (FAK; pp125FAK)-mediated signal transduction via cell surface integrin-ECM interaction [44]. It has been shown that FAK expression is enhanced in osteoblasts growing on Al2O3-Mg2+, suggesting that tyrosine phosphorylation of signaling proteins was enhanced by binding to Mg2+-supplemented bioceramics [44]. In addition to Shc and FAK, other key proteins, such as collagen type 1, vitronectin, and fibronectin, are also highly expressed by osteoblast cells in the presence of Mg [47]. In vitro, osteoblastic cells and other cell types have been shown to depend primarily on adsorbed vitronectin or fibronectin for initial adhesion and spreading on various materials, including tissue culture polystyrene, titanium, stainless steel, and hydroxyapatite [49,50,51]. Furthermore, vitronectin and/or fibronectin have been detected among the proteins adsorbed from whole blood and plasma in vitro and in vivo by implanted surfaces [52,53,54,55]. According to the Vroman effect, under stagnant conditions, initial protein deposition takes place in this sequence: albumin, globulin, fibrinogen, fibronectin, factor XII, and HMWK [18]. It has been studied that Mg2+ improves smooth muscle cells adhesion at 10 mM with certain interaction time. This study revealed some genes that related the influence of Mg2+ to cell adhesion (SERPINE 1) and inflammation (HMOX1, IL-1β) functions [56]. One exception to the adhesion-promotion effects of Mg2+ is the rapid formation of hydrogen bubbles that accumulated next to the MBM surfaces [57], which physically occupy the position for cell attachment [5]. However, this effect can be moderated by the Ca-P mineral layer coating the surface of MBM implants, which has been shown to enhance cell attachment and spreading [58]. It has also been demonstrated that pH-related proteins near isoelectric pH adsorb more on uncharged biomaterial surfaces [59,60,61]. Thus, the increasing pH of the surroundings and surface ion change caused by MBM corrosion might decrease cell adhesion.
4. Transportation Signaling
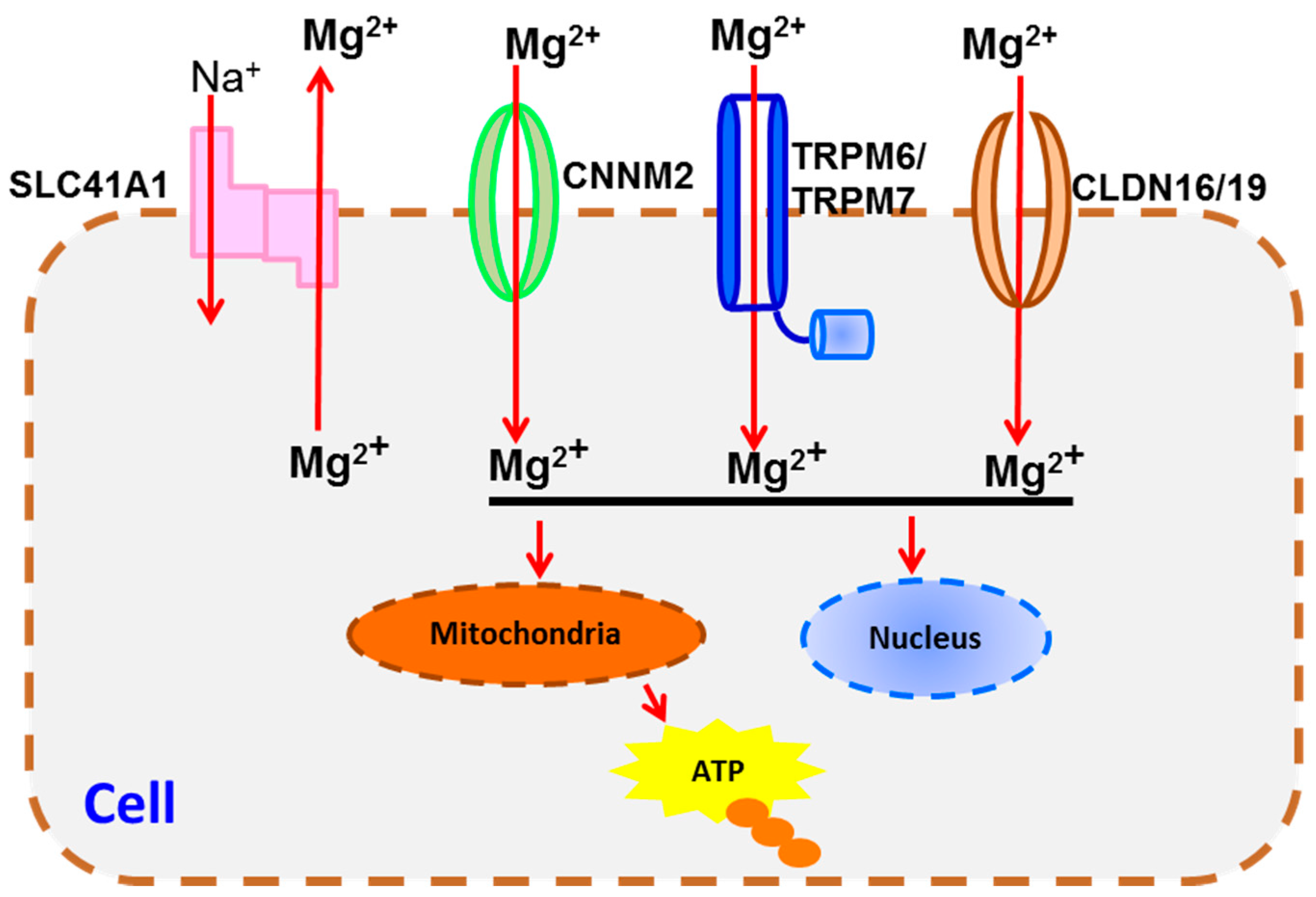
MBM implants increase the concentration of Mg2+, which may modify its transportation signaling pathway between intracellular and extracellular space. Intracellular Mg2+ concentration incorporating with Mg2+ channels is related to cell growth [62,63,64,65]. Mg2+-related functions in the nucleus and mitochondria, such as ATP synthesis, will change due to the increased amount of Mg2+ transported by cell membrane magnesium transporters (Figure 1): transient receptor potential melastatin (TRPM) 6 and 7, SLC41A1, CNNM2, and Claudin-16 and 19 (CLDN 16/19). Calcium homeostasis may also be altered (Figure 2).
TRPM6 and TRPM7 were characterized as magnesium “gatekeepers” on the cell membrane that monitor cellular magnesium homeostasis [66]. TRPM7 is responsible for intracellular Mg ion homeostasis in osteoblast cells and plays an important role in osteoblast proliferation and survival [67]. Thus, tight regulation of magnesium homeostasis is crucial for bone health. Another Mg2+ transporter is SLC41A1, which was found to be expressed in all of the human tissues tested, but at varying levels, with the heart and testis having the highest expression of the gene [68]. No explanation of the expression pattern has been given with regard to Mg2+-related physiology, though it has been suggested that SLC41 proteins are likely to be the metazoan equivalent of the Mg transporter E (MgtE) that is found in bacteria [68]. This will need to be verified using one of the now standard experimental systems for examining transport, especially in terms of the interface between tissue and MBM implants. Ancient conserved domain protein 2 (ACDP2) is encoded by CNNM2 and regulates physiological magnesium homeostasis in humans [69]. It belongs to the ACDP family and is widely expressed in human tissues, with the highest levels of expression in the brain, kidney, and placenta [70]. Furthermore, studies provide evidence for its involvement in magnesium transport [71,72]. Claudins allow for Mg2+ transport via the paracellular pathway; that is, that they mediate the transport of Mg ions through the tight junctions between cells that form an epithelial cell layer. In the claudin family, Claudin-19, which is encoded by the CLDN19 gene, has been implicated in magnesium transport [73,74]. Claudin-16 allows the selective re-uptake of Mg2+ in the kidney [75]. Defects in CLDN16 and CLDN19 can cause primary hypomagnesemia, which is characterized by massive renal magnesium wasting and hypercalciuria, resulting in nephrocalcinosis and renal failure [76].
Federica I. Wolf et al. suggested that the magnesium-deficient condition led to the increased cells percentage in the G0/G1-phase and the decreased cells percentage in the S-phase of the cell cycle [77]. Hypermagnesemia is uncommonly reported because the kidney is very efficient in excreting excess magnesium, thus we believe that patients with renal dysfunctions may not be suitable candidates for MBM implants. Besides this, hypomagnesemia and increased pH also affect cell morphology. Echinocytes (red blood cells with a spike-like cell membrane) can be seen with mild hemolysis in hypomagnesemia and are caused by an increase in pH in vitro [78]. At the site of MBM implantation, the Mg2+ concentration and pH are increased, and it has not been clearly reported whether MBM implants will increase the number of echinocytes [79], thus causing acanthocytosis. It seems that host tissue has regulation on the magnesium transporters overcompensate for the increase in magnesium ion concentration during the corrosion. However, evidence, such as channels behaviors before, during, and after Mg-based alloys implantation need to be studied.
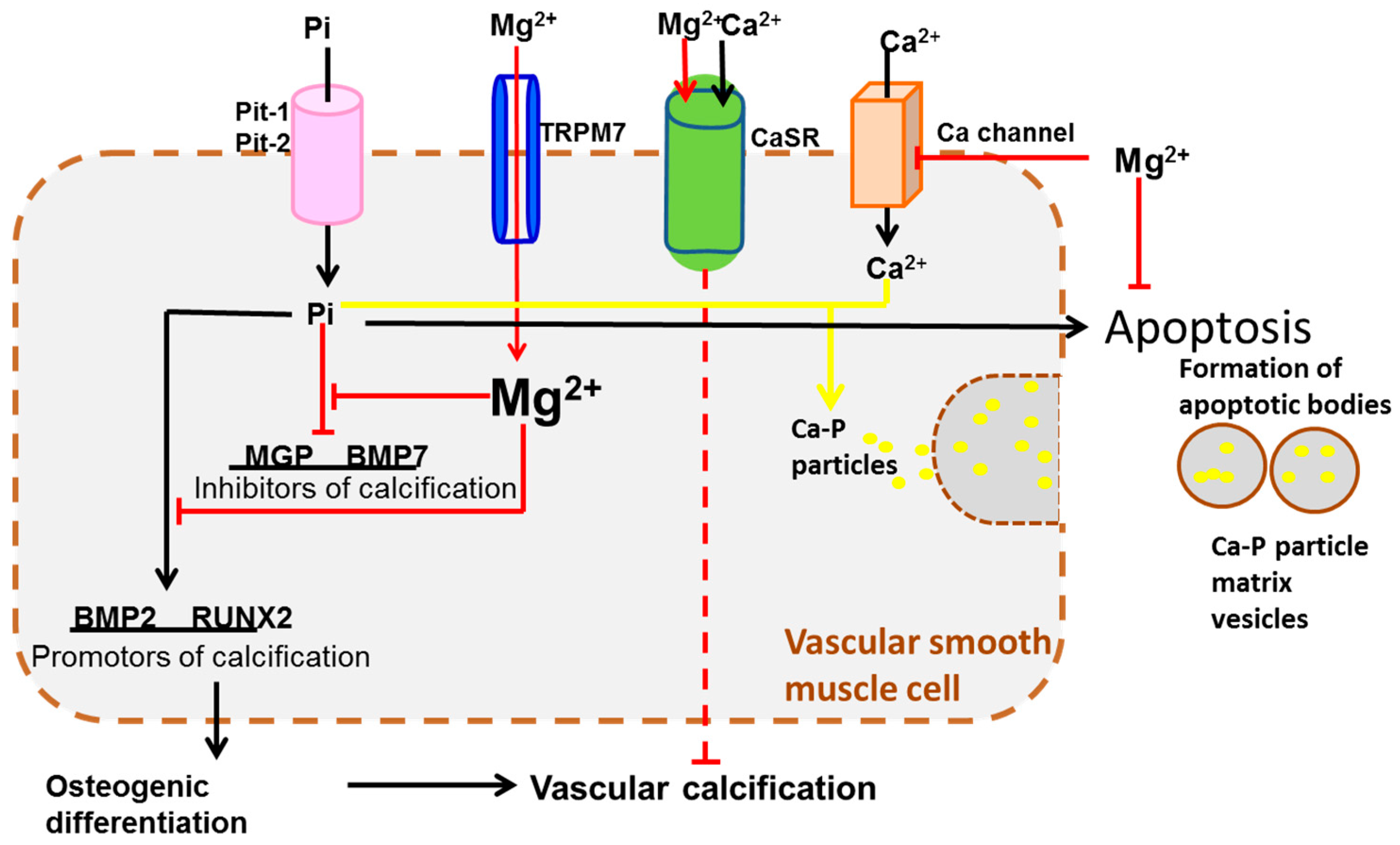
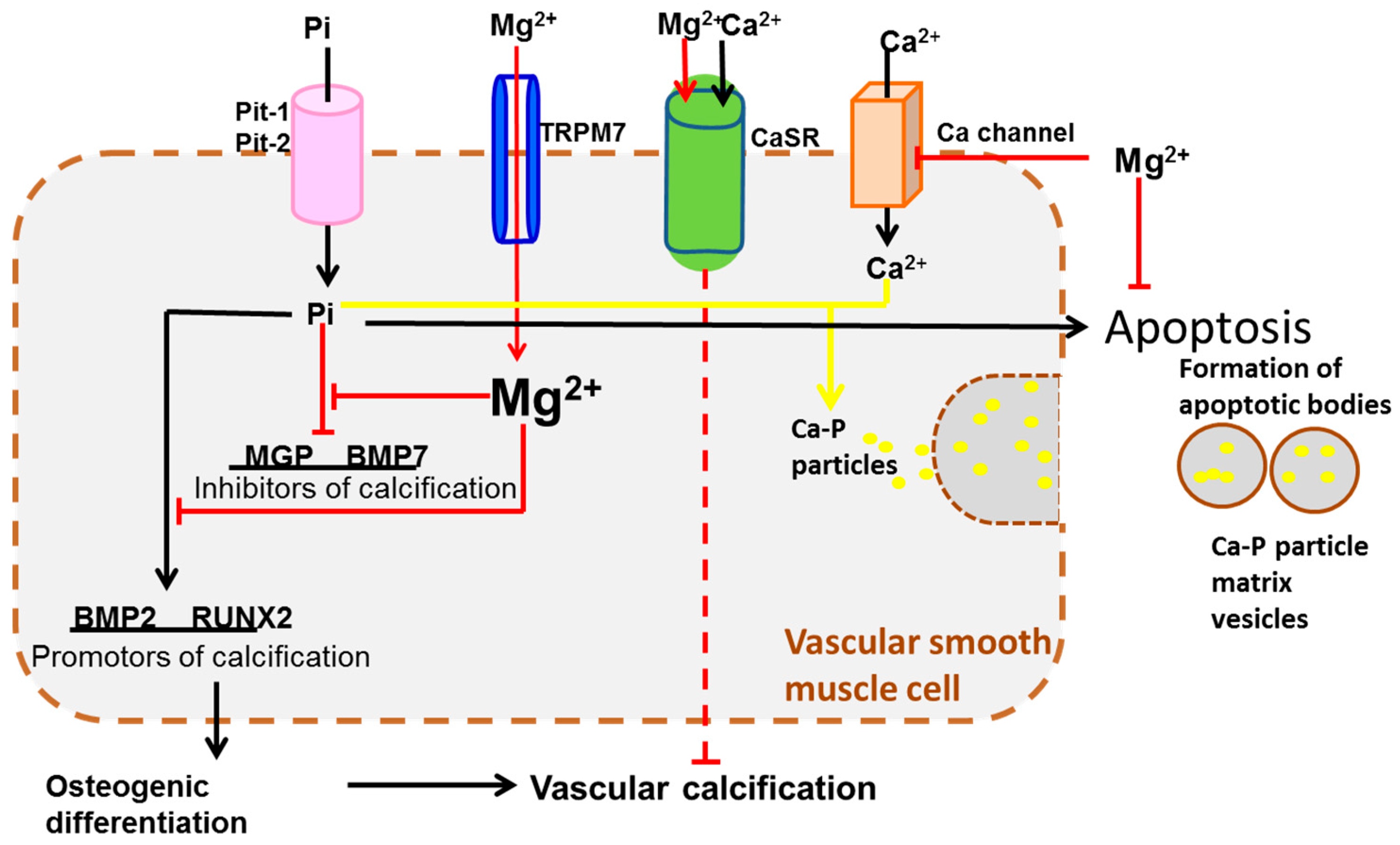
The layer of Ca-P deposition formed between the host tissue and MBM implants indicates the transportation of Mg2+ has a tight connection with Ca2+ transportation. TRPM7 by itself appears to be a Ca2+ channel [80], but in the presence of TRPM6, the affinity series of transported cations places Mg2+ above Ca2+ [67,81]. It has been found that the intestinal absorption and the renal excretion of the two ions are interdependent [82]. Furthermore, the Ca-P layer is the direct cause of vascular calcification [83]. Studies have shown that magnesium reduces calcification in bovine vascular smooth muscle cells (BVSMC) in a dose-dependent manner. Higher magnesium levels prevented BVSMC calcification and inhibited the expression of osteogenic proteins, apoptosis induced by β-glycerophosphate (BGP), and further progression of already established calcification [84]. It has been demonstrated that Mg2+ interferes with calcium homeostasis and Ca-P deposition in vascular smooth muscle cells (Figure 2) in the following ways: (1) Mg2+ can stabilize the Ca-P complex and inhibit the apatite transformation from Ca-P, instead forming more soluble magnesium-substituted whitlockite [85,86,87]; (2) Mg2+ suppresses apoptosis resulting in the formation of fewer apoptotic bodies; (3) Mg2+ blocks the entry of Ca2+ into the cells by being transported into cells as a Ca2+-channel antagonist [88], and then impedes the formation of Ca-P particles and Ca-P particle matrix vesicles; (4) Mg2+ enters cells through TRPM7 to balance the expression of calcification promotors and inhibitors by suppressing the negative effect of Pi (inorganic phosphate, transported by Pit-1 and Pit-2) on calcification inhibitors (MGP and BMP7) and regressing the activating effect of phosphate on calcification promotors (RUNX2 and BMP2) [89]; (5) Due to the effect of Mg2+ on these two calcification promotors, vascular smooth muscle cells are prevented from undergoing osteogenic differentiation and vascular calcification by the same pathway [84]; and, (6) Mg2+ activates calcium-sensing receptor (CaSR), which inhibits vascular smooth muscle cell calcification [90,91]. Theoretically, Mg2+ should prevent the formation of the Ca-P layer. In reality, however, a Ca-P layer is still formed between MBM implants and host tissue and its deposition to tissue depended on the Mg degradation rate [4].
5. Immune Responses
As an implantation biomaterial, MBMs should induce injury, blood-material interactions, provisional matrix formation, inflammation, chronic inflammation, granulation tissue development, foreign body reaction, and fibrosis/fibrous capsule development [38,92,93,94,95]. Immune cytokines, such as IL-4 and IL-13, may be involved to induce monocytes adhesion on MBMs surface and monocytes/macrophage fusion to form foreign body giant cells [38]. However, because of the degradability of MBMs, the immune responses are affected by the corrosion products and surface changes of MBMs. Magnesium ions participate in immune responses in numerous ways: as a cofactor for immunoglobulin synthesis, C'3 convertase, immune cell adherence, antibody-dependent cytolysis, IgM-lymphocyte binding, macrophage response to lymphokines, T helper cell-B cell adherence, binding of substance P to lymphoblasts, and antigen binding to macrophage RNA [96]. As biocompatible materials, MBMs do not elicit a detrimental immune response. In fact, some of the immunological responses that are generated by MBMs reflect their beneficial properties.
In one in vitro study, the expression of inflammation-related genes (IL-8, PDGF, TGF-β1, Angio1, βFGF, VEGF, ET-1, CXCR-1, HIF-1α) was either increased or decreased with different magnesium ion concentrations [39]. In magnesium-deficient rodents, TNFα, IL-1, and IL-6 are increased in both the serum and bone marrow microenvironment [97]. Low extracellular magnesium increases endothelial secretion of growth factors and cytokines, such as interleukin 1 (IL-1), which perpetuates cell dysfunction and affects smooth muscle cell functions [98]. These factors have important roles in the immune system. For example, IL-1α and IL-1β are cytokines that participate in the regulation of immune responses, inflammatory reactions, and hematopoiesis [99]. Interleukin 6 (IL-6), also referred to as B-cell stimulatory factor-2 (BSF-2) and interferon beta-2, is a cytokine involved in a wide variety of immune functions, such as antibody secretion, acute phase reaction, and inflammation [100]. Interleukin 8 (IL-8), known as a neutrophil chemotactic factor, is a chemokine produced by macrophages and other cell types, including epithelial cells, airway smooth muscle cells [101], and endothelial cells.
The most significant aspect of MBMs that are related to the immune response is hydrogen gas production [102]. The expression of several pro-inflammatory factors can be decreased by molecular H2, including TNF-α, IL-6, IL-1β, CCL2, IL-10, TNF-γ, IL-12, CAM-1 [103], HMGB-1 [104], PGE2 [105], and nuclear factor-κB (NF-κB) [106]. The design of MBM implants should make use of the immune response to improve implant integration while avoiding its perpetuation, leading to chronic inflammation and foreign body reactions, and thus loss of intended function [32].
6. Tissue Growth
MBMs implanted into living tissue initiate host immune responses that reflect the first step of tissue growth [107] and fibrous encapsulation [38]. There were concerns about tissue damage because of the evolved hydrogen bubbles and alkalization of solution that are caused by magnesium degradation [43,108]. In some cases, hydrogen bubbles from a degrading MBM surface can be accumulated next to the implant and separate tissues and tissue layers, which will delay the healing of the surgery region and lead to the necrosis of tissues [58]. However, promising studies of magnesium-based biodegradable materials in vivo have shown that they can enhance new bone formation in the vicinity of implantation, including the enhanced local formation of the periosteum and endosteum, two distinct membrane layers that cover the outer and inner surfaces of the bone [109]. MBMs have been shown to be non-toxic and can stimulate bone tissue healing because a high concentration of magnesium ions can lead to bone cell activation [12]. For cardiovascular tissue growth, we recently studied Magnesium implantation in arteries both ex vivo and in vivo. Though there are gas pockets in intima around the implanted Mg wire, the tissue showed normal morphology [4]. A complex signaling network of growth factors includes epidermal growth factor (EGF), fibroblast growth factor (FGF), granulocyte macrophage colony stimulating factor (GM-CSF), transform growth factor-β (TGF-β), vascular endothelial growth factor (VEGF), and platelet derived growth factor (PDGF). This signaling network controls adhesion, migration, proliferation, and differentiation of fibroblasts, keratinocytes, and endothelial cells in wound healing [110]. According to Vroman Effect [18], during the vascular wound healing process, blood proteins will deposit on MBMs surface in a provisional matrix manner, which provides structural, biochemical, and cellular components to processes wound healing [38].
Increased expression of collagen I extracellular matrix protein was found in human bone-derived cells (HBDC) responding to Mg2+-enriched substrates [44], further suggesting that magnesium promotes bone growth. In addition to magnesium, studies have shown that the Ca-P layer that is generated by MBM implants can also promote tissue growth during the biodegradation process both in vivo and in vitro [12,111]. This layer has been proven to facilitate the differentiation and proliferation of osteoblastic cells in a Ca-P ratio-dependent manner, indicating that the Ca-P layer promotes bone formation [112]. There is also Ca-P layer formation due to blood-triggered corrosion of magnesium alloys [113]. The molecular mechanism of this effect has not been discovered yet; however, it might be related to the ability of the Ca-P layer to increase cell adhesion and spreading.
There are still some molecules that have not been related to MBM implants that are associated with tissue growth. For example, Damsky has suggested a role for the integrin molecules α5α1 and α3α1 in bone formation [114]. It has also been shown that inhibitor of κB kinase–nuclear factor-κB (IKK-NF-κB) inhibits osteoblastic bone formation by restricting the expression of Fos-related antigen-1 (Fra-1), an essential transcription factor that is involved in bone matrix formation in vitro and in vivo [115]. Therefore, targeting IKK–NF-κB, α5α1, and α3α1 may help to promote bone formation and treat bone resorption that occurs due to the inflammatory response after MBM implantation.
7. Systematic Integration
The biodegradation of Mg elicits an increase of Mg2+, hydrogen gas, and other corrosion products to homeostasis. The molecules that have been proved or might be related to the responses to these corrosion products are converged in Table 1. The molecules generally function in cell adhesion, transportation signaling, immune responses, and tissue growth. The further study of key molecules that are involved in the in vivo and in vitro response to MBM implants, including their functions and pathway, are advanced approaches to understand the biocompatibility of MBMs.
8. Conclusions
The biocompatibility and degradation properties of Mg alloys make them remarkable implant materials. The most significant problem with MBMs is the difference in their corrosion behavior between in vitro and in vivo studies, which reflects the difficulty in predicting the biological responses of MBMs in the in vitro studies. Another problem is the rapid corrosion of MBMs and the products generated as a result. Systematically understanding the cellular/molecular responses to MBMs implants in the aspect of cell adhesion, transportation signaling, immune responses, and tissue growth are innovative strategies to evaluate their long-term safety for clinical use.
Acknowledgments
This work was supported by NIH NIGMS grant (ISC3GM113728), National Science Foundation (NSF) EAGER grant (1649243), and Engineering Research Center (ERC) for Revolutionizing Metallic Biomaterials (NSF-0812348) at North Carolina A & T State University.
Author Contributions
Lumei Liu conceptualized, wrote and edited the paper; Juan Wang, Teal Russell and Yeoheung Yun revised the paper; Juan Wang gave idea and advice; Jagannathan Sankar and Yeoheung Yun gave instructions and directions.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Kuhlmann, J.; Bartsch, I.; Willbold, E.; Schuchardt, S.; Holz, O.; Hort, N.; Höche, D.; Heineman, W.R.; Witte, F. Fast escape of hydrogen from gas cavities around corroding magnesium implants. Acta Biomater. 2013, 9, 8714–8721. [Google Scholar] [CrossRef] [PubMed]
- McBride, E.D. Absorbable metal in bone surgery: A further report on the use of magnesium alloys. J. Am. Med. Assoc. 1938, 111, 2464–2467. [Google Scholar] [CrossRef]
- Zhang, S.; Li, J.; Song, Y.; Zhao, C.; Zhang, X.; Xie, C.; Zhang, Y.; Tao, H.; He, Y.; Jiang, Y. In vitro degradation, hemolysis and mc3t3-e1 cell adhesion of biodegradable Mg–Zn alloy. Mater. Sci. Eng. C 2009, 29, 1907–1912. [Google Scholar] [CrossRef]
- Wang, J.; Liu, L.; Wu, Y.; Maitz, M.F.; Wang, Z.; Koo, Y.; Zhao, A.; Sankar, J.; Kong, D.; Huang, N. Ex vivo blood vessel bioreactor for analysis of the biodegradation of magnesium stent models with and without vessel wall integration. Acta Biomater. 2017, 50, 546–555. [Google Scholar] [CrossRef] [PubMed]
- Liu, L.; Koo, Y.; Collins, B.; Xu, Z.; Sankar, J.; Yun, Y. Biodegradability and platelets adhesion assessment of magnesium-based alloys using a microfluidic system. PLoS ONE 2017, 12, e0182914. [Google Scholar] [CrossRef] [PubMed]
- McCord, C.P.; Prendergast, J.J.; Meek, S.F.; Harrold, G.C. Chemical gas gangrene from metallic magnesium. Ind. Med. 1942, 11, 71–75. [Google Scholar]
- Edwards, J.D. Application of the Interferometer to Gas Analysis; Government Publishing Office: Washington, DC, USA, 1919.
- Song, G.; Song, S.-Z. A possible biodegradable magnesium implant material. Adv. Eng. Mater. 2007, 9, 298–302. [Google Scholar] [CrossRef]
- Ohsawa, I.; Ishikawa, M.; Takahashi, K.; Watanabe, M.; Nishimaki, K.; Yamagata, K.; Katsura, K.-I.; Katayama, Y.; Asoh, S.; Ohta, S. Hydrogen acts as a therapeutic antioxidant by selectively reducing cytotoxic oxygen radicals. Nat. Med. 2007, 13, 688–694. [Google Scholar] [CrossRef] [PubMed]
- Salganik, R.I. The benefits and hazards of antioxidants: Controlling apoptosis and other protective mechanisms in cancer patients and the human population. J. Am. Coll. Nutr. 2001, 20, 464S–472S. [Google Scholar] [CrossRef] [PubMed]
- Liu, H.; Colavitti, R.; Rovira, I.I.; Finkel, T. Redox-dependent transcriptional regulation. Circ. Res. 2005, 97, 967–974. [Google Scholar] [CrossRef] [PubMed]
- Witte, F.; Kaese, V.; Haferkamp, H.; Switzer, E.; Meyer-Lindenberg, A.; Wirth, C.J.; Windhagen, H. In vivo corrosion of four magnesium alloys and the associated bone response. Biomaterials 2005, 26, 3557–3563. [Google Scholar] [CrossRef] [PubMed]
- Arnett, T.R.; Dempster, D.W. Effect of ph on bone resorption by rat osteoclasts in vitro. Endocrinology 1986, 119, 119–124. [Google Scholar] [CrossRef] [PubMed]
- Bohr, C.; Hasselbalch, K.; Krogh, A. Concerning a biologically important relationship—The influence of the carbon dioxide content of blood on its oxygen binding. Skand. Arch. Physiol. 1904, 16, 402. [Google Scholar] [CrossRef]
- Schwartz, M.A.; Schaller, M.D.; Ginsberg, M.H. Integrins: Emerging paradigms of signal transduction. Annu. Rev. Cell Dev. Biol. 1995, 11, 549–599. [Google Scholar] [CrossRef] [PubMed]
- Grzesik, W.J. Integrins and bone—Cell adhesion and beyond. Arch. Immunol. Ther. Exp. 1996, 45, 271–275. [Google Scholar]
- Damsky, C.H.; Ilić, D. Integrin signaling: It’s where the action is. Curr. Opin. Cell Biol. 2002, 14, 594–602. [Google Scholar] [CrossRef]
- Vroman, L.; Adams, A.; Fischer, G.; Munoz, P. Interaction of high molecular weight kininogen, factor XII, and fibrinogen in plasma at interfaces. Blood 1980, 55, 156–159. [Google Scholar] [PubMed]
- Coté, C.J.; Lerman, J.; Todres, I.D. A Practice of Anesthesia for Infants and Children E-Book: Expert Consult: Online and Print; Elsevier Health Sciences: Amsterdam, The Netherlands, 2012. [Google Scholar]
- Ehtemam-Haghighi, S.; Liu, Y.; Cao, G.; Zhang, L.-C. Phase transition, microstructural evolution and mechanical properties of Ti-Nb-Fe alloys induced by fe addition. Mater. Des. 2016, 97, 279–286. [Google Scholar] [CrossRef]
- Ehtemam-Haghighi, S.; Prashanth, K.; Attar, H.; Chaubey, A.K.; Cao, G.; Zhang, L. Evaluation of mechanical and wear properties of Ti-xNb-7Fe alloys designed for biomedical applications. Mater. Des. 2016, 111, 592–599. [Google Scholar] [CrossRef]
- Hynes, R.O. Integrins: Versatility, modulation and signaling. Cell 1992, 69, 11–25. [Google Scholar] [CrossRef]
- Zhu, X.; Ohtsubo, M.; Böhmer, R.M.; Roberts, J.M.; Assoian, R.K. Adhesion-dependent cell cycle progression linked to the expression of cyclin D1, activation of cyclin E-cdk2, and phosphorylation of the retinoblastoma protein. J. Cell Biol. 1996, 133, 391–403. [Google Scholar] [CrossRef] [PubMed]
- Van der Flier, A.; Sonnenberg, A. Structural and functional aspects of filamins. Biochim. Biophys. Acta (BBA) Mol. Cell Res. 2001, 1538, 99–117. [Google Scholar] [CrossRef]
- Wilson, C.J.; Clegg, R.E.; Leavesley, D.I.; Pearcy, M.J. Mediation of biomaterial-cell interactions by adsorbed proteins: A review. Tissue Eng. 2005, 11, 1–18. [Google Scholar] [CrossRef] [PubMed]
- Gorbet, M.B.; Sefton, M.V. Biomaterial-associated thrombosis: Roles of coagulation factors, complement, platelets and leukocytes. Biomaterials 2004, 25, 5681–5703. [Google Scholar] [CrossRef] [PubMed]
- Howlett, C.R.; Zreiqat, H.; Wu, Y.; McFall, D.W.; McKenzie, D.R. Effect of ion modification of commonly used orthopedic materials on the attachment of human bone-derived cells. J. Biomed. Mater. Res. 1999, 45, 345–354. [Google Scholar] [CrossRef]
- Zreiqat, H.; Evans, P.; Howlett, C.R. Effect of surface chemical modification of bioceramic on phenotype of human bone-derived cells. J. Biomed. Mater. Res. 1999, 44, 389–396. [Google Scholar] [CrossRef]
- Bilek, M.; Evans, P.; Mckenzie, D.; McCulloch, D.; Zreiqat, H.; Howlett, C. Metal ion implantation using a filtered cathodic vacuum arc. J. Appl. Phys. 2000, 87, 4198–4204. [Google Scholar] [CrossRef]
- Kokubo, T. Bioceramics and Their Clinical Applications; Elsevier: Amsterdam, The Netherlands, 2008. [Google Scholar]
- Anast, C.S.; Mohs, J.M.; Kaplan, S.L.; Burns, T.W. Evidence for parathyroid failure in magnesium deficiency. Science 1972, 177, 606–608. [Google Scholar] [CrossRef] [PubMed]
- Williams, D.F. On the mechanisms of biocompatibility. Biomaterials 2008, 29, 2941–2953. [Google Scholar] [CrossRef] [PubMed]
- Neil, W.; Forsyth, M.; Howlett, P.; Hutchinson, C.; Hinton, B. Corrosion of magnesium alloy ZE41—The role of microstructural features. Corros. Sci. 2009, 51, 387–394. [Google Scholar] [CrossRef]
- Song, G.L.; Atrens, A. Corrosion mechanisms of magnesium alloys. Adv. Eng. Mater. 1999, 1, 11–33. [Google Scholar] [CrossRef]
- Smith, C.E.; Xu, Z.; Waterman, J.; Sankar, J. Cytocompatibility assessment of mgznca alloys. Emerg. Mater. Res. 2013, 2, 283–290. [Google Scholar] [CrossRef]
- Atrens, A.; Liu, M.; Abidin, N.I.Z. Corrosion mechanism applicable to biodegradable magnesium implants. Mater. Sci. Eng. B 2011, 176, 1609–1636. [Google Scholar] [CrossRef]
- Witte, F.; Hort, N.; Vogt, C.; Cohen, S.; Kainer, K.U.; Willumeit, R.; Feyerabend, F. Degradable biomaterials based on magnesium corrosion. Curr. Opin. Solid State Mater. Sci. 2008, 12, 63–72. [Google Scholar] [CrossRef]
- Anderson, J.M.; Rodriguez, A.; Chang, D.T. Foreign body reaction to biomaterials. In Seminars in Immunology; Elsevier: Amsterdam, The Netherlands, 2008; pp. 86–100. [Google Scholar]
- Yun, Y.; Dong, Z.; Tan, Z.; Schulz, M.J. Development of an electrode cell impedance method to measure osteoblast cell activity in magnesium-conditioned media. Anal. Bioanal. Chem. 2010, 396, 3009–3015. [Google Scholar] [CrossRef] [PubMed]
- Yun, Y.; Dong, Z.; Lee, N.; Liu, Y.; Xue, D.; Guo, X.; Kuhlmann, J.; Doepke, A.; Halsall, H.B.; Heineman, W. Revolutionizing biodegradable metals. Mater. Today 2009, 12, 22–32. [Google Scholar] [CrossRef]
- Ingber, D.E. Tensegrity ii. How structural networks influence cellular information processing networks. J. Cell Sci. 2003, 116, 1397–1408. [Google Scholar] [CrossRef] [PubMed]
- Steele, J.G.; Dalton, B.A.; Johnson, G.; Underwood, P.A. Adsorption of fibronectin and vitronectin onto primaria™ and tissue culture polystyrene and relationship to the mechanism of initial attachment of human vein endothelial cells and BHK-21 fibroblasts. Biomaterials 1995, 16, 1057–1067. [Google Scholar] [CrossRef]
- Song, G. Control of biodegradation of biocompatable magnesium alloys. Corros. Sci. 2007, 49, 1696–1701. [Google Scholar] [CrossRef]
- Zreiqat, H.; Howlett, C.R.; Zannettino, A.; Evans, P.; Schulze-Tanzil, G.; Knabe, C.; Shakibaei, M. Mechanisms of magnesium-stimulated adhesion of osteoblastic cells to commonly used orthopaedic implants. J. Biomed. Mater. Res. 2002, 62, 175–184. [Google Scholar] [CrossRef] [PubMed]
- Gronthos, S.; Stewart, K.; Graves, S.E.; Hay, S.; Simmons, P.J. Integrin expression and function on human osteoblast-like cells. J. Bone Min. Res. 1997, 12, 1189–1197. [Google Scholar] [CrossRef] [PubMed]
- Shakibaei, M.; Schulze-Tanzil, G.; de Souza, P.; John, T.; Rahmanzadeh, M.; Rahmanzadeh, R.; Merker, H.-J. Inhibition of mitogen-activated protein kinase kinase induces apoptosis of human chondrocytes. J. Biol. Chem. 2001, 276, 13289–13294. [Google Scholar] [CrossRef] [PubMed]
- Schlaepfer, D.D.; Hanks, S.K.; Hunter, T.; van der Geer, P. Integrin-mediated signal transduction linked to ras pathway by GRB2 binding to focal adhesion kinase. Nature 1994, 372, 786–791. [Google Scholar] [CrossRef] [PubMed]
- Shattil, S.J.; Newman, P.J. Integrins: Dynamic scaffolds for adhesion and signaling in platelets. Blood 2004, 104, 1606–1615. [Google Scholar] [CrossRef] [PubMed]
- Steele, J.G.; McFarland, C.; Dalton, B.A.; Johnson, G.; Evans, M.D.; Rolfe Howlett, C.; Underwood, P.A. Attachment of human bone cells to tissue culture polystyrene and to unmodified polystyrene: The effect of surface chemistry upon initial cell attachment. J. Biomater. Sci. Polym. Ed. 1994, 5, 245–257. [Google Scholar] [CrossRef]
- Howlett, C.R.; Evans, M.D.; Walsh, W.R.; Johnson, G.; Steele, J.G. Mechanism of initial attachment of cells derived from human bone to commonly used prosthetic materials during cell culture. Biomaterials 1994, 15, 213–222. [Google Scholar] [CrossRef]
- Kilpadi, K.L.; Chang, P.L.; Bellis, S.L. Hydroxylapatite binds more serum proteins, purified integrins, and osteoblast precursor cells than titanium or steel. J. Biomed. Mater. Res. 2001, 57, 258–267. [Google Scholar] [CrossRef]
- Bale, M.D.; Wohlfahrt, L.A.; Mosher, D.F.; Tomasini, B.; Sutton, R.C. Identification of vitronectin as a major plasma protein adsorbed on polymer surfaces of different copolymer composition. Blood 1989, 74, 2698–2706. [Google Scholar] [PubMed]
- Fabrizius-Homan, D.J.; Cooper, S.L. A comparison of the adsorption of three adhesive proteins to biomaterial surfaces. J. Biomater. Sci. Polym. Ed. 1992, 3, 27–47. [Google Scholar] [CrossRef]
- Babensee, J.E.; Cornelius, R.M.; Brash, J.L.; Sefton, M.V. Immunoblot analysis of proteins associated with hema-mma microcapsules: Human serum proteins in vitro and rat proteins following implantation. Biomaterials 1998, 19, 839–849. [Google Scholar] [CrossRef]
- Rosengren, Å.; Pavlovic, E.; Oscarsson, S.; Krajewski, A.; Ravaglioli, A.; Piancastelli, A. Plasma protein adsorption pattern on characterized ceramic biomaterials. Biomaterials 2002, 23, 1237–1247. [Google Scholar] [CrossRef]
- Ma, J.; Zhao, N.; Zhu, D. Biphasic responses of human vascular smooth muscle cells to magnesium ion. J. Biomed. Mater. Res. Part A 2016, 104, 347–356. [Google Scholar] [CrossRef] [PubMed]
- Meyer-Lindenberg, A.; Windhugen, H.; Witte, F. Medical Implant for the Human or Animal Body. U.S. Patents US20,040,241,036 A1, 2 December 2004. [Google Scholar]
- Maxian, S.H.; Zawadsky, J.P.; Dunn, M.G. Effect of Ca/P coating resorption and surgical fit on the bone/implant interface. J. Biomed. Mater. Res. 1994, 28, 1311–1319. [Google Scholar] [CrossRef] [PubMed]
- Norde, W. Driving forces for protein adsorption at solid surfaces. In Macromolecular Symposia; Wiley Online Library: New York, NY, USA, 1996; pp. 5–18. [Google Scholar]
- Ohno, Y.; Maehashi, K.; Yamashiro, Y.; Matsumoto, K. Electrolyte-gated graphene field-effect transistors for detecting pH and protein adsorption. Nano Lett. 2009, 9, 3318–3322. [Google Scholar] [CrossRef] [PubMed]
- Dee, K.C.; Puleo, D.A.; Bizios, R. An Introduction to Tissue-Biomaterial Interactions; John Wiley & Sons: Hoboken, NJ, USA, 2003. [Google Scholar]
- Maier, J.A.; Bernardini, D.; Rayssiguier, Y.; Mazur, A. High concentrations of magnesium modulate vascular endothelial cell behaviour in vitro. Biochim. Biophys. Acta (BBA) Mol. Basis Dis. 2004, 1689, 6–12. [Google Scholar] [CrossRef] [PubMed]
- Moomaw, A.S.; Maguire, M.E. The unique nature of Mg2+ channels. Physiology 2008, 23, 275–285. [Google Scholar] [CrossRef] [PubMed]
- Günther, T. Concentration, compartmentation and metabolic function of intracellular free Mg2+. Magnes. Res. 2006, 19, 225–236. [Google Scholar] [PubMed]
- Bo, S.; Pisu, E. Role of dietary magnesium in cardiovascular disease prevention, insulin sensitivity and diabetes. Curr. Opin. Lipidol. 2008, 19, 50–56. [Google Scholar] [CrossRef] [PubMed]
- Schlingmann, K.P.; Waldegger, S.; Konrad, M.; Chubanov, V.; Gudermann, T. TRPM6 and TRPM7—Gatekeepers of human magnesium metabolism. Biochim. Biophys. Acta (BBA) Mol. Basis Dis. 2007, 1772, 813–821. [Google Scholar] [CrossRef] [PubMed]
- Nadler, M.J.; Hermosura, M.C.; Inabe, K.; Perraud, A.-L.; Zhu, Q.; Stokes, A.J.; Kurosaki, T.; Kinet, J.-P.; Penner, R.; Scharenberg, A.M. Ltrpc7 is a Mg·ATP-regulated divalent cation channel required for cell viability. Nature 2001, 411, 590–595. [Google Scholar] [CrossRef] [PubMed]
- Wabakken, T.; Rian, E.; Kveine, M.; Aasheim, H.-C. The human solute carrier SLC41A1 belongs to a novel eukaryotic subfamily with homology to prokaryotic MgtE Mg2+ transporters. Biochem. Biophys. Res. Commun. 2003, 306, 718–724. [Google Scholar] [CrossRef]
- Meyer, T.E.; Verwoert, G.C.; Hwang, S.-J.; Glazer, N.L.; Smith, A.V.; van Rooij, F.J.; Ehret, G.B.; Boerwinkle, E.; Felix, J.F.; Leak, T.S.; et al. Genome-wide association studies of serum magnesium, potassium, and sodium concentrations identify six loci influencing serum magnesium levels. PLoS Genet. 2010, 6, e1001045. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wang, C.-Y.; Shi, J.-D.; Yang, P.; Kumar, P.G.; Li, Q.-Z.; Run, Q.-G.; Su, Y.-C.; Scott, H.S.; Kao, K.-J.; She, J.-X. Molecular cloning and characterization of a novel gene family of four ancient conserved domain proteins (ACDP). Gene 2003, 306, 37–44. [Google Scholar] [CrossRef]
- Goytain, A.; Quamme, G.A. Functional characterization of ACDP2 (ancient conserved domain protein), a divalent metal transporter. Physiol. Genom. 2005, 22, 382–389. [Google Scholar] [CrossRef] [PubMed]
- Will, C.; Breiderhoff, T.; Thumfart, J.; Stuiver, M.; Kopplin, K.; Sommer, K.; Günzel, D.; Querfeld, U.; Meij, I.C.; Shan, Q.; et al. Targeted deletion of murine cldn16 identifies extra-and intrarenal compensatory mechanisms of Ca2+ and Mg2+ wasting. Am. J. Physiol.-Ren. Physiol. 2010, 298, F1152–F1161. [Google Scholar] [CrossRef] [PubMed]
- Naeem, M.; Hussain, S.; Akhtar, N. Mutation in the tight-junction gene claudin 19 (CLDN19) and familial hypomagnesemia, hypercalciuria, nephrocalcinosis (FHHNC) and severe ocular disease. Am. J. Nephrol. 2011, 34, 241–248. [Google Scholar] [CrossRef] [PubMed]
- Konrad, M.; Schaller, A.; Seelow, D.; Pandey, A.V.; Waldegger, S.; Lesslauer, A.; Vitzthum, H.; Suzuki, Y.; Luk, J.M.; Becker, C. Mutations in the tight-junction gene claudin 19 (CLDN19) are associated with renal magnesium wasting, renal failure, and severe ocular involvement. Am. J. Hum. Genet. 2006, 79, 949–957. [Google Scholar] [CrossRef] [PubMed]
- Hou, J.; Renigunta, A.; Konrad, M.; Gomes, A.S.; Schneeberger, E.E.; Paul, D.L.; Waldegger, S.; Goodenough, D.A. Claudin-16 and claudin-19 interact and form a cation-selective tight junction complex. J. Clin. Investig. 2008, 118, 619. [Google Scholar] [CrossRef] [PubMed]
- Hou, J.; Renigunta, A.; Gomes, A.S.; Hou, M.; Paul, D.L.; Waldegger, S.; Goodenough, D.A. Claudin-16 and claudin-19 interaction is required for their assembly into tight junctions and for renal reabsorption of magnesium. Proc. Natl. Acad. Sci. USA 2009, 106, 15350–15355. [Google Scholar] [CrossRef] [PubMed]
- Wolf, F.I.; Cittadini, A. Magnesium in cell proliferation and differentiation. Front. Biosci. 1999, 4, D607–D617. [Google Scholar] [CrossRef] [PubMed]
- Hoffman, R.; Benz, E.J., Jr.; Silberstein, L.E.; Heslop, H.; Weitz, J.; Anastasi, J. Hematology: Basic Principles and Practice, Expert Consult Premium Edition-Enhanced Online Features; Elsevier Health Sciences: Amsterdam, The Netherland, 2012. [Google Scholar]
- Wang, J.; He, Y.; Maitz, M.F.; Collins, B.; Xiong, K.; Guo, L.; Yun, Y.; Wan, G.; Huang, N. A surface-eroding poly (1,3-trimethylene carbonate) coating for fully biodegradable magnesium-based stent applications: Toward better biofunction, biodegradation and biocompatibility. Acta Biomater. 2013, 9, 8678–8689. [Google Scholar] [CrossRef] [PubMed]
- Runnels, L.W.; Yue, L.; Clapham, D.E. The TRPM7 channel is inactivated by PIP2 hydrolysis. Nat. Cell Biol. 2002, 4, 329–336. [Google Scholar] [CrossRef] [PubMed]
- Monteilh-Zoller, M.K.; Hermosura, M.C.; Nadler, M.J.; Scharenberg, A.M.; Penner, R.; Fleig, A. TRPM7 provides an ion channel mechanism for cellular entry of trace metal ions. J. Gen. Physiol. 2003, 121, 49–60. [Google Scholar] [CrossRef] [PubMed]
- Paunier, L. Effect of magnesium on phosphorus and calcium metabolism. Monatsschr. Kinderheilkd. Organ Deutsch. Ges. Kinderheilkd. 1992, 140, S17–S20. [Google Scholar]
- Massy, Z.A.; Drüeke, T.B. Magnesium and cardiovascular complications of chronic kidney disease. Nat. Rev. Nephrol. 2015, 11, 432–442. [Google Scholar] [CrossRef] [PubMed]
- Kircelli, F.; Peter, M.E.; Ok, E.S.; Celenk, F.G.; Yilmaz, M.; Steppan, S.; Asci, G.; Ok, E.; Passlick-Deetjen, J. Magnesium reduces calcification in bovine vascular smooth muscle cells in a dose-dependent manner. Nephrol. Dial. Transplant. 2011, 27, 514–521. [Google Scholar] [CrossRef] [PubMed]
- LeGeros, R. Formation and transformation of calcium phosphates: Relevance to vascular calcification. Z. Kardiol. 2001, 90, 116–124. [Google Scholar] [CrossRef] [PubMed]
- Cheng, P.-T.; Grabher, J.; LeGeros, R. Effects of magnesium on calcium phosphate formation. Magnesium 1987, 7, 123–132. [Google Scholar]
- Peters, F.; Epple, M. Simulating arterial wall calcification in vitro: Biomimetic crystallization of calcium phosphates under controlled conditions. Z. Kardiol. 2001, 90, 81–85. [Google Scholar] [CrossRef] [PubMed]
- Altura, B.; Altura, B.; Carella, A.; Gebrewold, A.; Murakawa, T.; Nishio, A. Mg2+-Ca2+ interaction in contractility of vascular smooth muscle: Mg2+ versus organic calcium channel blockers on myogenic tone and agonist-induced responsiveness of blood vessels. Can. J. Physiol. Pharmacol. 1987, 65, 729–745. [Google Scholar] [CrossRef] [PubMed]
- Montezano, A.C.; Zimmerman, D.; Yusuf, H.; Burger, D.; Chignalia, A.Z.; Wadhera, V.; van Leeuwen, F.N.; Touyz, R.M. Vascular smooth muscle cell differentiation to an osteogenic phenotype involves TRPM7 modulation by magnesium. Hypertension 2010, 56, 453–462. [Google Scholar] [CrossRef] [PubMed]
- Brown, E.M.; Gamba, G.; Riccardi, D.; Lombardi, M.; Butters, R.; Kifor, O.; Sun, A.; Hediger, M.A.; Lytton, J.; Hebert, S.C. Cloning and characterization of an extracellular Ca2+-sensing receptor from bovine parathyroid. Nature 1993, 366, 575–580. [Google Scholar] [CrossRef] [PubMed]
- Ivanovski, O.; Nikolov, I.G.; Joki, N.; Caudrillier, A.; Phan, O.; Mentaverri, R.; Maizel, J.; Hamada, Y.; Nguyen-Khoa, T.; Fukagawa, M. The calcimimetic R-568 retards uremia-enhanced vascular calcification and atherosclerosis in apolipoprotein E deficient (apoE−/−) mice. Atherosclerosis 2009, 205, 55–62. [Google Scholar] [CrossRef] [PubMed]
- Anderson, J.M. Biological responses to materials. Annu. Rev. Mater. Res. 2001, 31, 81–110. [Google Scholar] [CrossRef]
- Anderson, J.M. Multinucleated giant cells. Curr. Opin. Hematol. 2000, 7, 40–47. [Google Scholar] [CrossRef] [PubMed]
- Gretzer, C.; Emanuelsson, L.; Liljensten, E.; Thomsen, P. The inflammatory cell influx and cytokines changes during transition from acute inflammation to fibrous repair around implanted materials. J. Biomater. Sci. Polym. Ed. 2006, 17, 669–687. [Google Scholar] [CrossRef] [PubMed]
- Luttikhuizen, D.T.; Harmsen, M.C.; Luyn, M.J.V. Cellular and molecular dynamics in the foreign body reaction. Tissue Eng. 2006, 12, 1955–1970. [Google Scholar] [CrossRef] [PubMed]
- Galland, L. Magnesium and immune function: An overview. Magnesium 1988, 7, 290–299. [Google Scholar] [PubMed]
- Mazur, A.; Maier, J.A.M.; Rock, E.; Gueux, E.; Nowacki, W.; Rayssiguier, Y. Magnesium and the inflammatory response: Potential physiopathological implications. Arch. Biochem. Biophys. 2007, 458, 48–56. [Google Scholar] [CrossRef] [PubMed]
- Maier, J.A.; Malpuech-Brugère, C.; Zimowska, W.; Rayssiguier, Y.; Mazur, A. Low magnesium promotes endothelial cell dysfunction: Implications for atherosclerosis, inflammation and thrombosis. Biochim. Biophys. Acta (BBA) Mol. Basis Dis. 2004, 1689, 13–21. [Google Scholar] [CrossRef] [PubMed]
- Sims, J.E.; March, C.J.; Cosman, D.; Widmer, M.B.; MacDonald, H.R.; McMahan, C.J.; Grubin, C.E.; Wignall, J.M.; Jackson, J.L.; Call, S.M.; et al. cDNA expression cloning of the IL-1 receptor, a member of the immunoglobulin superfamily. Science 1988, 241, 585–589. [Google Scholar] [CrossRef] [PubMed]
- Hirano, T.; Yasukawa, K.; Harada, H.; Taga, T.; Watanabe, Y.; Matsuda, T.; Kashiwamura, S.-I.; Nakajima, K.; Koyama, K.; Iwamatsu, A.; et al. Complementary DNA for a novel human interleukin (BSF-2) that induces b lymphocytes to produce immunoglobulin. Nature 1986, 324, 73–76. [Google Scholar] [CrossRef] [PubMed]
- Hedges, J.C.; Singer, C.A.; Gerthoffer, W.T. Mitogen-activated protein kinases regulate cytokine gene expression in human airway myocytes. Am. J. Respir. Cell Mol. Biol. 2000, 23, 86–94. [Google Scholar] [CrossRef] [PubMed]
- Seitz, J.M.; Eifler, R.; Bach, F.; Maier, H.J. Magnesium degradation products: Effects on tissue and human metabolism. J. Biomed. Mater. Res. Part A 2014, 102, 3744–3753. [Google Scholar] [CrossRef] [PubMed]
- Buchholz, B.M.; Kaczorowski, D.J.; Sugimoto, R.; Yang, R.; Wang, Y.; Billiar, T.R.; McCurry, K.R.; Bauer, A.J.; Nakao, A. Hydrogen inhalation ameliorates oxidative stress in transplantation induced intestinal graft injury. Am. J. Transplant. 2008, 8, 2015–2024. [Google Scholar] [CrossRef] [PubMed]
- Xie, K.; Yu, Y.; Pei, Y.; Hou, L.; Chen, S.; Xiong, L.; Wang, G. Protective effects of hydrogen gas on murine polymicrobial sepsis via reducing oxidative stress and hmgb1 release. Shock 2010, 34, 90–97. [Google Scholar] [CrossRef] [PubMed]
- Kawasaki, H.; Guan, J.; Tamama, K. Hydrogen gas treatment prolongs replicative lifespan of bone marrow multipotential stromal cells in vitro while preserving differentiation and paracrine potentials. Biochem. Biophys. Res. Commun. 2010, 397, 608–613. [Google Scholar] [CrossRef] [PubMed]
- Chen, H.; Sun, Y.P.; Li, Y.; Liu, W.W.; Xiang, H.G.; Fan, L.Y.; Sun, Q.; Xu, X.Y.; Cai, J.M.; Ruan, C.P.; et al. Hydrogen-rich saline ameliorates the severity of L-arginine-induced acute pancreatitis in rats. Biochem. Biophys. Res. Commun. 2010, 393, 308–313. [Google Scholar] [CrossRef] [PubMed]
- Franz, S.; Rammelt, S.; Scharnweber, D.; Simon, J.C. Immune responses to implants—A review of the implications for the design of immunomodulatory biomaterials. Biomaterials 2011, 32, 6692–6709. [Google Scholar] [CrossRef] [PubMed]
- Song, G. Recent progress in corrosion and protection of magnesium alloys. Adv. Eng. Mater. 2005, 7, 563–586. [Google Scholar] [CrossRef]
- Zhang, E.; Xu, L.; Yu, G.; Pan, F.; Yang, K. In vivo evaluation of biodegradable magnesium alloy bone implant in the first 6 months implantation. J. Biomed. Mater. Res. Part A 2009, 90, 882–893. [Google Scholar] [CrossRef] [PubMed]
- Barrientos, S.; Stojadinovic, O.; Golinko, M.S.; Brem, H.; Tomic-Canic, M. Growth factors and cytokines in wound healing. Wound Repair Regen. 2008, 16, 585–601. [Google Scholar] [CrossRef] [PubMed]
- Li, L.; Gao, J.; Wang, Y. Evaluation of cyto-toxicity and corrosion behavior of alkali-heat-treated magnesium in simulated body fluid. Surf. Coat. Technol. 2004, 185, 92–98. [Google Scholar] [CrossRef]
- Hulshoff, J.; Van Dijk, K.; De Ruijter, J.; Rietveld, F.; Ginsel, L.; Jansen, J. Interfacial phenomena: An in vitro study of the effect of calcium phosphate (Ca-P) ceramic on bone formation. J. Biomed. Mater. Res. 1998, 40, 464–474. [Google Scholar] [CrossRef]
- Geis-Gerstorfer, J.; Schille, C.; Schweizer, E.; Rupp, F.; Scheideler, L.; Reichel, H.P.; Hort, N.; Nolte, A.; Wendel, H.P. Blood triggered corrosion of magnesium alloys. Mater. Sci. Eng. B 2011, 176, 1761–1766. [Google Scholar] [CrossRef]
- Damsky, C.H. Extracellular matrix-integrin interactions in osteoblast function and tissue remodeling. Bone 1999, 25, 95–96. [Google Scholar] [CrossRef]
- Chang, J.; Wang, Z.; Tang, E.; Fan, Z.; McCauley, L.; Franceschi, R.; Guan, K.; Krebsbach, P.H.; Wang, C.-Y. Inhibition of osteoblastic bone formation by nuclear factor-κB. Nat. Med. 2009, 15, 682–689. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
An illustration of the main magnesium transporters on the cell membrane.
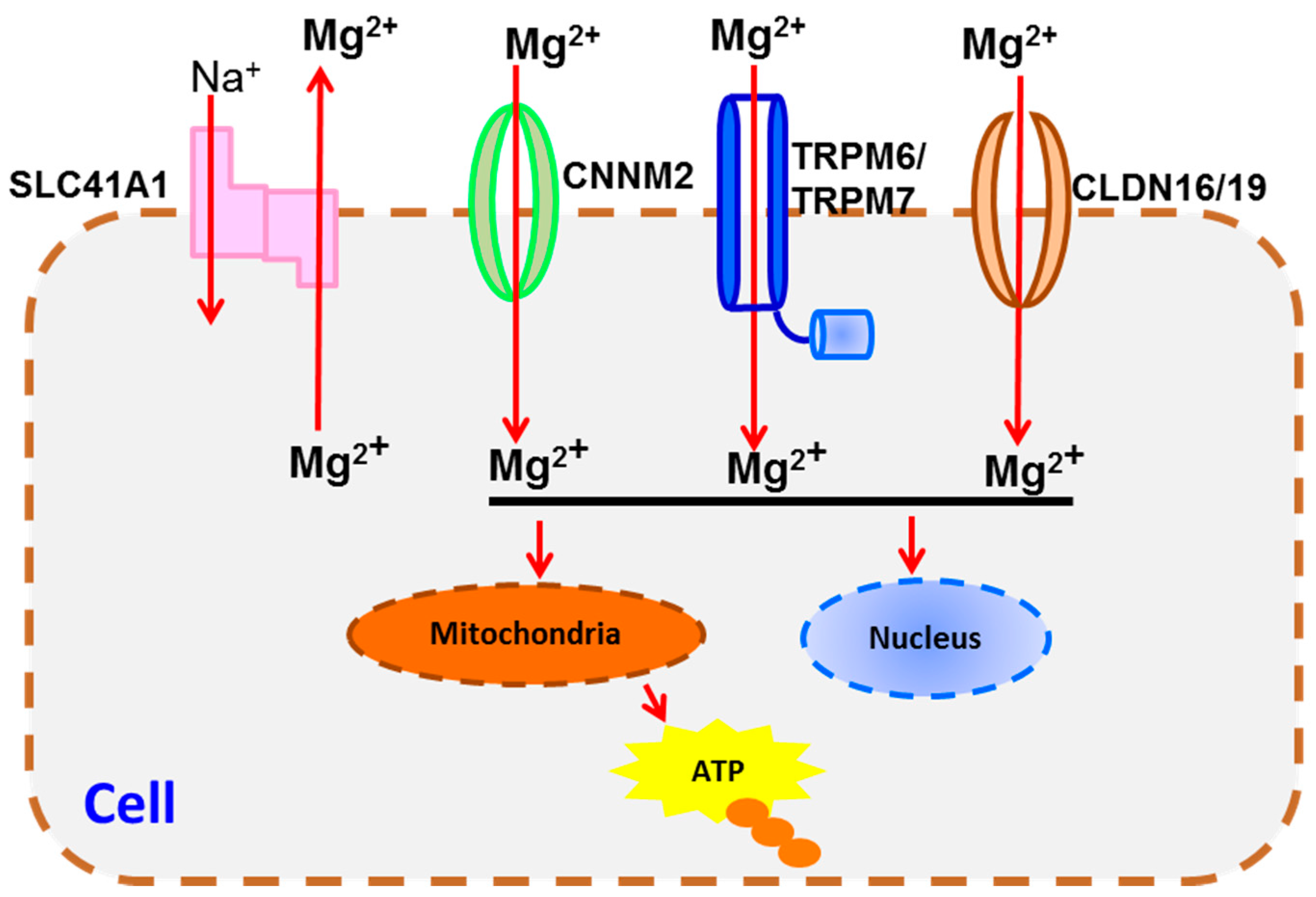
Figure 2.
Mg2+ interferes with calcium homeostasis and Ca-P layer deposition. Abbreviations: Pit, inorganic phosphate transporter; MGP, matrix Gla protein; BMP, bone morphogenetic protein; RUNX2, runt-related transcription factor 2.
Figure 2.
Mg2+ interferes with calcium homeostasis and Ca-P layer deposition. Abbreviations: Pit, inorganic phosphate transporter; MGP, matrix Gla protein; BMP, bone morphogenetic protein; RUNX2, runt-related transcription factor 2.

{kind=link}
{kind=link}
Table 1.
Molecular factors involved in or possibly related to the response to magnesium-based materials (MBM) implant corrosion products.
Table 1.
Molecular factors involved in or possibly related to the response to magnesium-based materials (MBM) implant corrosion products.
| Biological Responses | Mg2+ | Ca-P | H2 |
|---|---|---|---|
| Cell Adhesion | α5β1-, α3β1-, β1-integrins [44], Shc [46], FAK [44], vitronectin and fibronectin [47,49], SERPINE 1 [56] | ||
| Transportation Signaling | TRPM6/7 [67,81,82], SLC41A1 [68], CLDN16/19 [76], CNNM2 [69] | CaSR [90,91], BGP [84] | |
| Immune Response | IL-8, PDGF, TGF-β1, Angio1, βFGF, VEGF, ET-1, CXCR-1, HIF-1α [39]; HMOX1 [56], IL-1, TNFα, IL-6 [97]; IL-1 α and IL-1 β [100]; BSF-2 [100] | TNF-α, IL-6, IL-1β, CCL2 and IL-10, TNF-γ, IL-12, CAM-1 [103]; HMGB-1 [104]; PGE2 [105], NF-κB [106] | |
| Tissue Growth | collagen I extracellular matrix protein [44]; EGF, FGF, GM-CSF, TGF-β, VEGF, PDGF [110]; IKK-NF-κB [110,115]; α5α1 and α3α1 [114] | ||
© 2017 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
MDPI and ACS Style
Liu, L.; Wang, J.; Russell, T.; Sankar, J.; Yun, Y. The Biological Responses to Magnesium-Based Biodegradable Medical Devices. Metals 2017, 7, 514. https://doi.org/10.3390/met7110514
AMA Style
Liu L, Wang J, Russell T, Sankar J, Yun Y. The Biological Responses to Magnesium-Based Biodegradable Medical Devices. Metals. 2017; 7(11):514. https://doi.org/10.3390/met7110514
Chicago/Turabian StyleLiu, Lumei, Juan Wang, Teal Russell, Jagannathan Sankar, and Yeoheung Yun. 2017. "The Biological Responses to Magnesium-Based Biodegradable Medical Devices" Metals 7, no. 11: 514. https://doi.org/10.3390/met7110514
Note that from the first issue of 2016, this journal uses article numbers instead of page numbers. See further details here.