1. Introduction
The monkeypox virus (MPXV) has been reported to cause human monkeypox (HMPX) zoonotic infection since early 1970s [
1,
2]. The disease has been endemic in Central and Western Africa since then, with a few outbreaks that were reported in the US and the UK [
3]. These outbreaks with limited spread were linked to imported animals from the endemic regions or travel history to these regions [
4,
5]. However, the latest 2022 HMPX multi-country outbreak has a different scenario, with more than 31,000 cases in 82 previously non-endemic countries and territories, in addition to 375 HMPX reported in seven endemic countries as of 11 August 2022 [
6]. The rapid rate of disease spread and the need for a collaborative and well-coordinated response necessitated the declaration of the 2022 HMPX outbreak as a public health emergency of international concern [
7,
8].
The transmission of the MPXV occurs directly through close contact and indirectly via fomites [
9,
10,
11,
12,
13]. Among the peculiarities of the ongoing HMPX outbreak is the observation of transmission clusters among men who have sex with men (MSM, including gays and bisexual men) [
12,
14,
15,
16,
17]. This suggests that sexual transmission could be an effective mode of virus spread [
18,
19,
20].
Clinically, HMPX is primarily a cutaneous disease with lymphadenopathy similar to the first infectious disease to be eradicated from humans; namely, smallpox [
2,
21]. The incubation period ranges between 5 and 21 days, followed by flu-like symptoms and the development of skin rash [
21]. This skin eruption evolves through the following stages: macules, papules, pustules, vesicles, and scabs [
22]. During the current HMPX outbreak, genital lesions have been frequently reported, with possibility of asymptomatic infection [
16,
22,
23]. Hospital admission could be indicated considering the reporting of HMPX complications that include: super-infection by bacteria, dehydration, and respiratory distress, among others [
12,
24,
25]. The case–fatality ratio has been reported up to 11%; however, only twelve mortalities have been linked to the disease amid the ongoing 2022 HMPX outbreak [
2,
3,
6,
10].
Antivirals are available for treatment, and prevention relies on vaccination [
10,
21,
26,
27]. In addition, the preventive efforts can benefit from the central role of healthcare workers (HCWs) through active surveillance and refined diagnosis and management, which can help in disease control [
28]. Therefore, the assessment of HCWs’ knowledge and their current confidence levels to diagnose and manage HMPX can be helpful in guiding the response plans needed for the control and mitigation efforts [
29].
The few previous and recent studies among HCWs, university students, and the general population that evaluated HMPX knowledge revealed defects in HMPX knowledge regarding the different aspects of the disease besides low levels of confidence to diagnose and manage the cases [
30,
31,
32,
33,
34]. These findings can be understandable due to the previous lack of attention to the disease outside the endemic regions, lack of educational material about the topic in health schools’ curricula, and courses besides the lack of clinical training [
31,
32,
33,
34,
35]. Further research is needed, particularly among health professionals based on their central role in outbreak response, and due to the rapid dissemination of the HMPX outbreak [
36].
Recently, the frequent emergence of infectious diseases was accompanied by infodemics characterized by viral dissemination of misinformation, social media panic, and bizarre conspiracy ideas that could spread faster than the disease, itself [
37,
38]. The belief in conspiracies was conspicuous during the recent Ebola outbreaks and the coronavirus disease 2019 (COVID-19) pandemic [
39,
40,
41,
42]. Thus, the almost immediate circulation of conspiracies surrounding the 2022 HMPX outbreak could be considered an expected phenomenon [
43,
44,
45]. Although the general embrace of conspiracy ideas could appear harmless, its potential harmful impact has been reported, particularly in the context of health-seeking behavior manifested in vaccination hesitancy and distrust in science and health institutions [
42]. Therefore, the assessment of conspiracy belief pervasiveness, especially among HCWs, appears essential, considering their role in curtailing the negative influence of these harmful beliefs [
46].
Kuwait is an Arab Middle Eastern high-income country with a population of more than 4,200,000 people. Although HMPX has not been reported in the country so far, the rapid increase of cases worldwide, besides the reporting of HMPX in other Arab countries (United Arab Emirates, Qatar, Lebanon, and Morocco) necessitates vigilant preparedness and response plans [
47]. Considering the primary role of health professionals in responding to the ongoing HMPX outbreak [
7,
29,
48], we aimed to assess the current knowledge of HCWs in Kuwait about the disease. In addition, the study goals included the evaluation of the current levels of confidence to diagnose and manage HMPX. Finally, we aimed to evaluate the attitude of HCWs in Kuwait towards conspiracies that are related to virus emergence and the subsequent measures aimed at controlling emerging viral diseases.
4. Discussion
The current study revealed the presence of knowledge gaps among HCWs in Kuwait regarding the HMPX infection. This result was found despite ubiquitous media coverage tackling the topic, as well as the rapid and timely delivery of published literature addressing almost every single aspect of the disease [
9,
12,
14,
15,
17,
19,
21,
22,
53]. Therefore, the design of efficient and well-organized response plans requires contemplation of HCWs’ knowledge and confidence levels to face the potential threats of this re-emerging infection [
54]. The frontline position of HCWs requires proper guidance that would help in patient care, in control efforts, and to address the possible issues of burnout and mental health problems frequently encountered among HCWs in outbreak situations [
55,
56]. Our study results were in agreement with past and recent studies that found defects in knowledge regarding HMPX among the general practitioners in Indonesia, physicians in Italy, and HCWs as well as university students in Jordan [
31,
33,
34,
51]. Expectedly, the level of monkeypox knowledge was higher in this study compared to those reported in the general public in Saudi Arabia and in the Kurdistan region of Iraq [
30,
57].
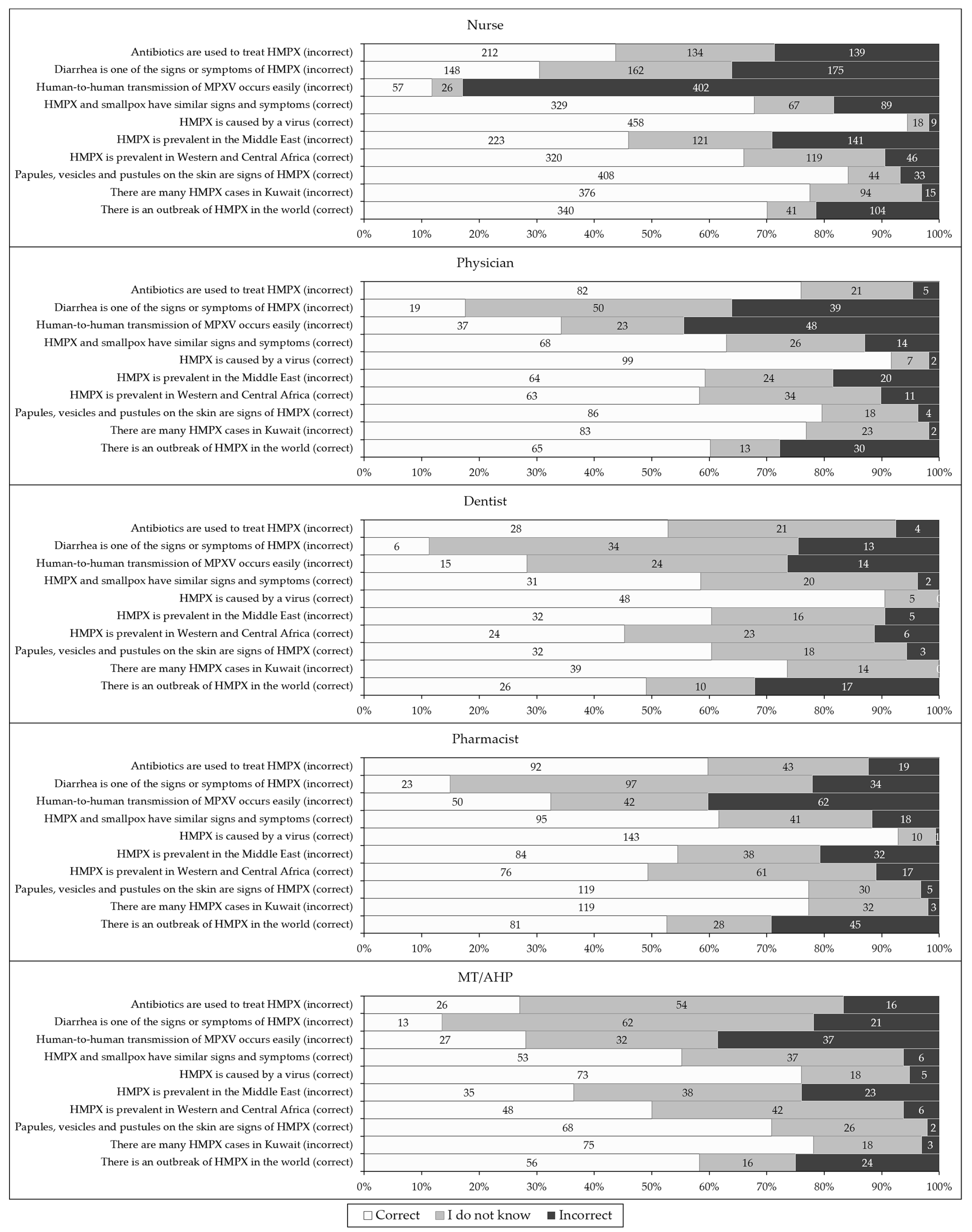
In this study, gaps in HMPX knowledge were most conspicuous for non-cutaneous manifestations of HMPX, besides the conditions of human-to-human transmission. For the item “human-to-human transmission of monkeypox occurs easily,” less than 40% of the participants responded correctly across the five occupational categories. Similar results were also noticed in the recent studies that used the same knowledge item [
34,
51]. The relevance of this result is related to the importance of implementing proper control and mitigation measures without exaggeration [
58]. Human-to-human transmission of MPXV has been reported prior to the 2022 outbreak, and became evident currently; nevertheless, it should be noted that transmission requires close contact and does not occur as readily as infections caused by respiratory viruses (e.g. SARS-CoV-2) [
58,
59]. Therefore, the emphasis on providing accurate information about the disease among HCWs cannot be overlooked. Subsequently, this approach among HCWs can help to guide the general public and to provide recommendations for patients, considering their important role amid this outbreak, which should be driven by the accurate knowledge needed to be alert but not panicked [
58].
It is also necessary to highlight the importance of providing accurate knowledge and training regarding the clinical presentation and treatment of the disease among HCWs. In this study, a considerable proportion of the participants (31.5%), incorrectly identified diarrhea as a symptom of HMPX. The high index of suspicion is necessary for timely diagnosis of HMPX, with subsequent implementation of control measures including contact tracing and isolation. However, the lack of accurate knowledge regarding the plethora of HMPX clinical manifestations could lead to a waste of valuable resources by the ordering of unnecessary diagnostic tests and the promotion of uneasiness for the patients [
60]. An additional important result was the finding that 20.4% of the participants incorrectly identified antibiotics as a treatment for HMPX. This is of particular interest in the Middle East region, where antimicrobial resistance was reported at alarmingly high levels, and the prescription of antibiotics due to lack of knowledge, without being clinically indicated, can aggravate this problem [
61,
62,
63].
Despite the general unsatisfactory level of HMPX knowledge observed across different occupational categories in this study, physicians displayed a higher level of knowledge about the disease. This result was in agreement with the findings of a recent study among HCWs in Jordan [
51]. The lower level of HMPX knowledge among non-physicians suggests that more efforts are needed to educate and train HCWs in these occupational categories, with a special focus on nurses, considering their central and direct role in patient care and response in outbreak situations [
64].
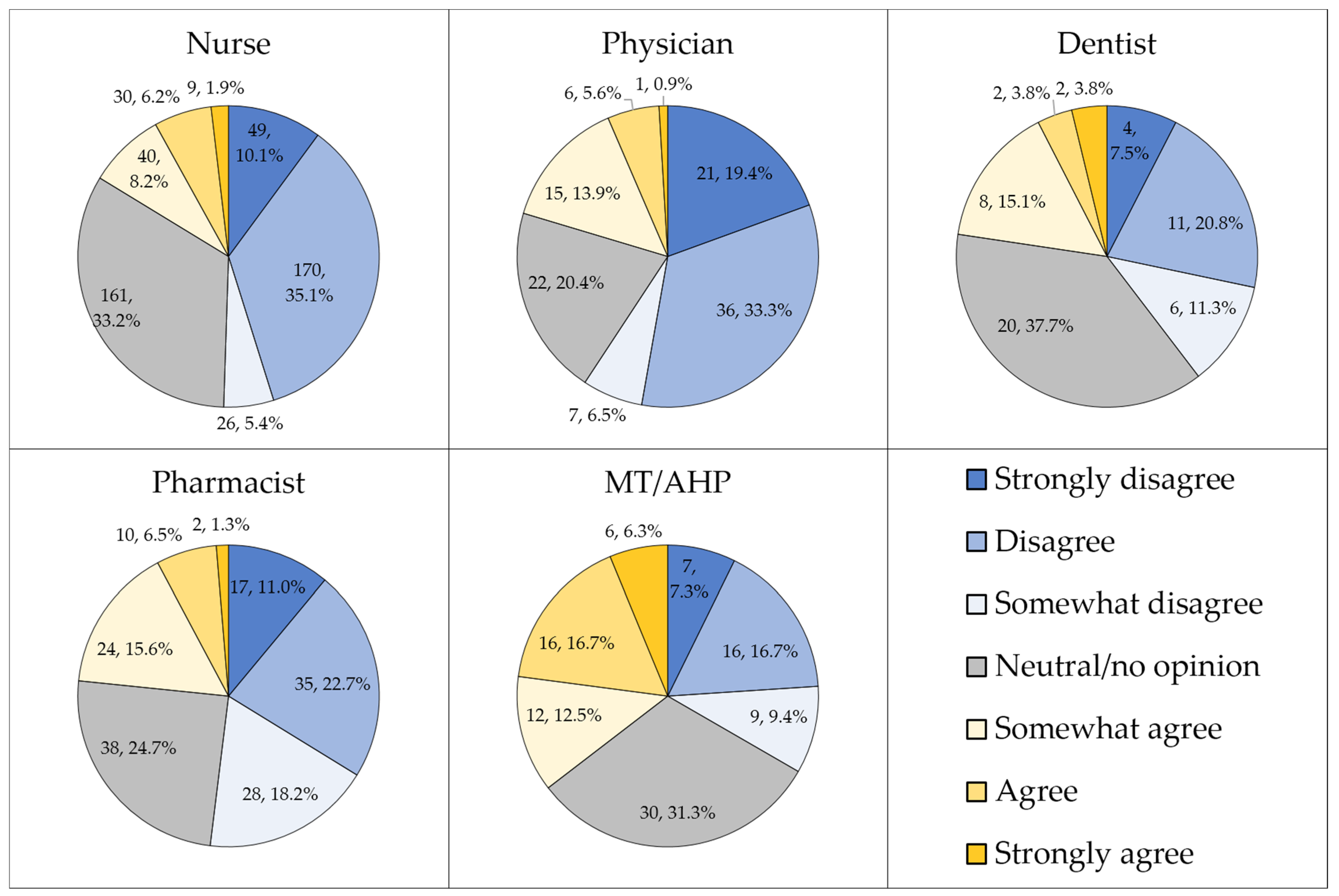
In contrast to the pattern of variability in HMPX knowledge per occupation noted in this study, nurses displayed higher self-reported confidence levels to diagnose and manage the disease. This result also contrasts with the findings of the study among HCWs in Jordan, where physicians reported higher confidence levels in association with higher HMPX knowledge, as well [
51]. The higher confidence levels among nurses compared to physicians in this study might be ascribed to the large proportion of non-native nurses in Kuwait [
65]. Previous studies showed that international experience among nurses is linked with acquisition of new clinical skills and awareness, which could explain such higher confidence levels among nurses [
66,
67]. The difference between nurses and physicians in this study was less conspicuous for the confidence in diagnostic tests, while generally low levels of confidence were reported among physicians to clinically diagnose and manage HMPX cases based on their current level of knowledge and skills. Thus, focusing on the improvement of physicians’ clinical skills through urgent training workshops and national conferences, as well as on providing clear guidelines for diagnosis and management, are a few suggested intervention measures that could help improve the low levels of confidence observed in this study [
32].
An interesting result in this study was the finding that 20.4% of the participants inaccurately believed that HMPX is exclusive to male homosexuals. It was also interesting to note that the belief in this false notion was independently correlated with lower HMPX knowledge and occupation (with higher prevalence of this inaccurate belief among MT/AHP compared to physicians, nurses, and pharmacists). Furthermore, the association between the agreement or neutrality towards the idea of HMPX exclusive occurrence among male homosexuals and the endorsement of conspiracy beliefs regarding emerging virus infections was remarkable, which was also noted in the recent study among HCWs in Jordan [
51].
Despite the observation that a majority of HMPX cases amid the current 2022 outbreak involve MSM, the disease was also reported among females and children [
12,
14,
15,
68]. Therefore, the idea that HMPX is exclusive to male homosexuals is inaccurate, in spite of the importance of focusing on MSM as the most-at-risk group that should be prioritized for control and preventive efforts, including vaccination [
69]. In this study, the survey item that was used to assess knowledge and attitude was not intended to directly assess the attitude towards the MSM role in the outbreak; nevertheless, the results might provide initial clues regarding the view of HCWs towards this issue. Specifically, holding the notion that the current HMPX outbreak is exclusive among MSM can have negative consequences that might include overlooking cases among women and children, in addition to linking the disease with sexual behavior, which might lead to stigma among the infected patients with subsequent deleterious effects on health-seeking behavior [
70,
71,
72]. Thus, future studies are warranted to directly investigate the possible stigma and discrimination directed towards HMPX patients, which is an urgent issue to be addressed, since it can cause collateral psychologic, social, and health damage in addition to the direct impact of the disease [
73,
74]. Such studies are of particular importance in the majority of countries in the Middle East region as a result of the dominant social, cultural, political, and religious perspectives that oppose homosexuality in the name of religious and cultural integrity [
75,
76,
77]. There is a notable prevalence of stigmatizing attitude towards MSM and patients with sexually transmitted infections in the region [
78,
79,
80]. Subsequently, if MPXV is introduced into the most-at-risk group (i.e. MSM), this can result in an outbreak with exacerbated consequences. Such a worrying outcome could stem from the correlation of stigma with adverse health practices (e.g. unprotected sex, multiple sexual partners, and reduced access to health care services) [
81,
82,
83].
In this study, the embrace of conspiracy beliefs regarding emerging virus infections was independently associated with agreement or lack of opinion towards the role of male homosexuals in HMPX spread. The previous study that was conducted among health professionals in Jordan revealed the same correlation. This result can be interpreted as either false knowledge without further effect on the attitude towards the patients, or as an observation that needs further elaboration to examine its possible link to stigmatizing attitude. Thus, we recommend future studies to examine the effect of such a hypothetical link, considering the importance of this concerning subject. This urgent issue needs to be addressed, taking into account the intensive media focus on MSM’s role in the current outbreak, which can fuel stigma towards this most-at-risk, often highly marginalized group [
73].
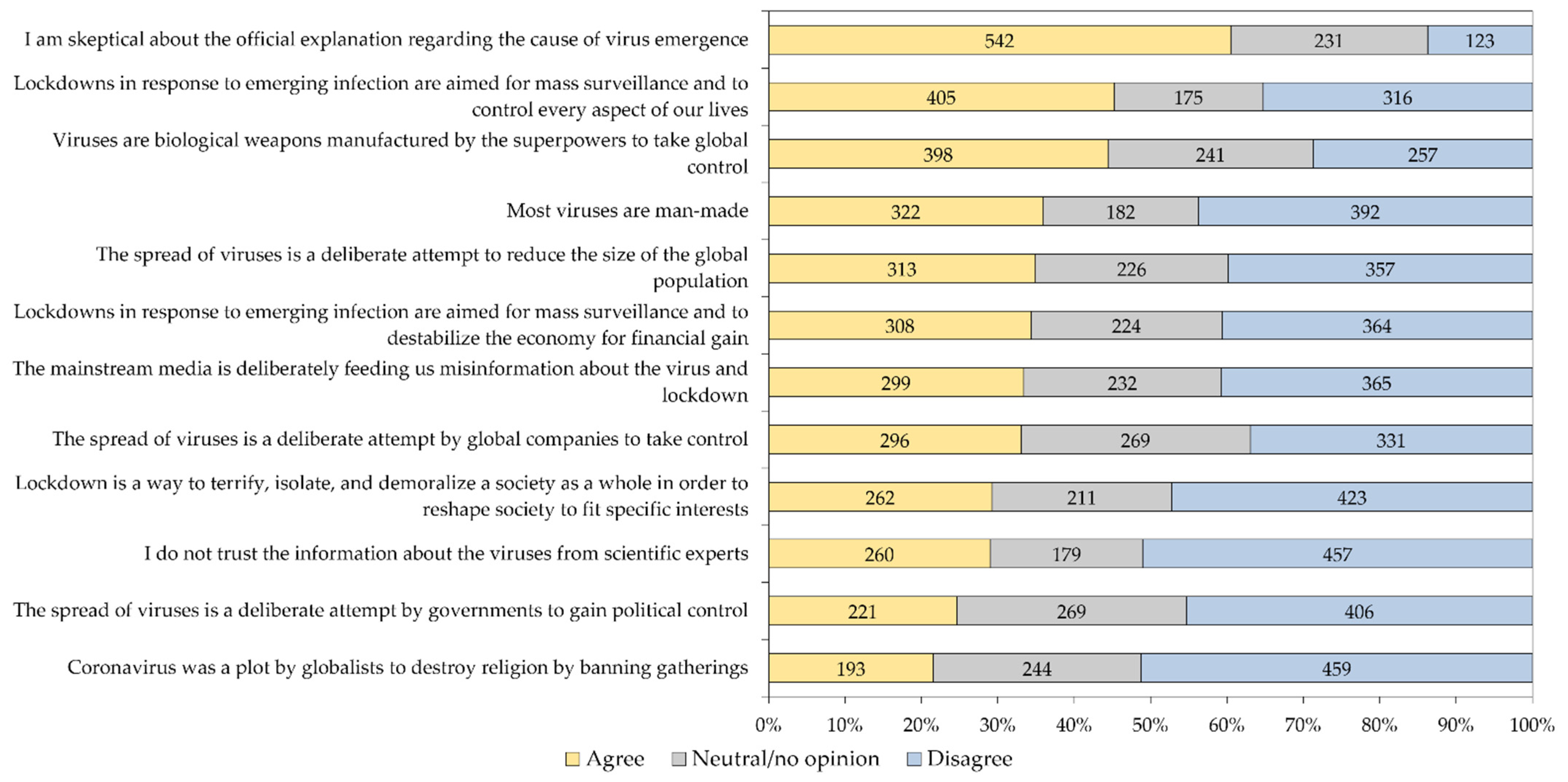
An important finding of the current study was the wide prevalence adoption of conspiratorial ideas about virus emergence and the subsequent intervention measures, which emerged as a recurrent pattern during the COVID-19 pandemic onwards, and particularly in the Middle East region [
34,
40,
51,
84]. Specifically, in this study, the skepticism to the official explanation of virus emergence was found at least to some extent among 60.5% of the study participants. In addition, the belief that “lockdowns in response to emerging infection are aimed for mass surveillance and to control every aspect of our lives” was found among 45.2% of the study sample, besides 44.4% who believed that “viruses are biological weapons manufactured by the superpowers to take global control.” The considerable proportion of individuals who held such beliefs was reported in the original comprehensive study by Freeman et al., with links to medical mistrust and lower levels of compliance to measures aimed to control the COVID-19 pandemic [
52].
In this study, and consistent with recent studies among university students and HCWs in Jordan [
34,
51], greater embrace of these conspiracies about emerging virus infection was associated with lower HMPX knowledge; however, it is important to emphasize that the directionality of this association and the cause–effect relationship cannot be inferred based on the cross sectional study design. Occupational category was also observed as an associated factor with higher embrace of conspiracies among nurses and MT/AHP. Higher embrace of conspiracies was also noted among females. The latter two results were also reported in the context of COVID-19 vaccine hesitancy and vaccine conspiracy beliefs among healthcare workers in Kuwait [
85].
It is important to highlight the recurring pattern of misinformation, and sometimes disinformation, that accompanies the reporting of infectious disease emergence [
86]. The viral spread of misinformation, amplified through social media, was described as an “infodemic” during the COVID-19 pandemic, and it became evident during the ongoing 2022 multi-country HMPX outbreak [
44,
45,
87,
88]. The relevance of this phenomenon in our study was reflected by the substantial percentage of the study participants who endorsed conspiratorial ideas regarding virus origin. The negative impact of such a phenomenon was investigated extensively during the COVID-19 pandemic, which included its association with negative psychologic, social, and health related consequences [
42,
89,
90]. Thus, the finding that a fraction of HCWs—a group that is considered knowledgeable regarding health-related topics—endorsed such ideas, was expected; nevertheless, the high prevalence of adoption of such conspiracies was surprising. One important issue in this context was reported by Alshahrani et al., with social media as the most frequent source of HMPX-related information among the general public in Saudi Arabia [
30]. The spread of health-related misinformation, including conspiracies, via social media channels was well known prior to the COVID-19 pandemic and the current HMPX outbreak, and a few suggested responses include the role of health organizations in providing corrective infographics, and partnership with social media platforms to allow immediate action through the promotion of the role of scientific experts in vigilant response [
91,
92].
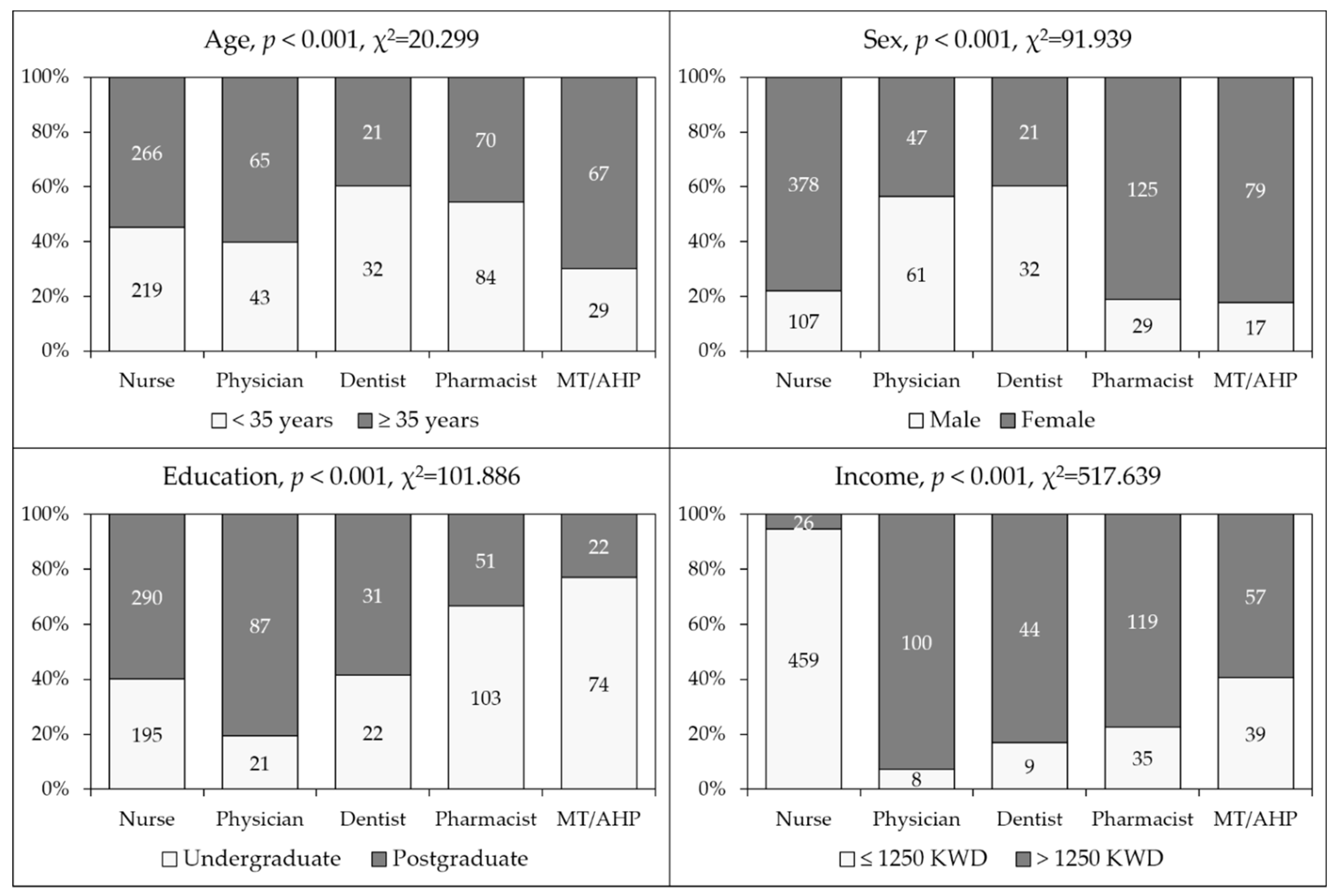
The study’s strength involved the inclusion of various HCW categories with a large sample size. However, the study was limited by the following caveats that must be considered in the interpretation of results, as follows: (1) Selection bias was inevitable, considering the snowball sampling approach; (2) Despite the large sample size, and the previous evidence that the number of nurses in Kuwait exceed the number of physicians, the dominance of nurses in the current study should be taken into account in the efforts to make generalizations [
49]; (3) the cross-sectional design precluded the assessment of causal associations; (4) the social desirability bias can be an important source of bias, particularly in relation to the items assessing conspiracies regarding emerging virus infections; (5) Future knowledge, attitude, and practice (KAP) HMPX studies can benefit from assessment of HMPX vaccination attitudes similar to the approach used by Riccò et al., and the low acceptance of HMPX vaccination in the region, as reported by Sirwan Ahmed et al. in Iraq, [
33,
57]; (6) The importance of assessment of the stigmatizing attitude towards patients, especially the high-risk MSM groups, should be considered in future research, as well; (7) The possibility of careless responses could not be excluded, particularly in relation to the absence of response time monitoring.









{kind=link}
{kind=link}
{kind=link}
{kind=link}