
Fifty Years of the National Rabies Control Program in Brazil under the One Health Perspective
 , , , , and
, , , , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Area
2.2. Study Design
2.2.1. Part One—Describing the Five Decades
2.2.2. Part Two—Exploring Possible Drivers
2.3. Data Collection, Sources, and Definitions
2.4. Data Analysis
3. Results
3.1. Part 1
3.1.1. Period A, from 1973 to 1979—Establishing and Implementing the Program
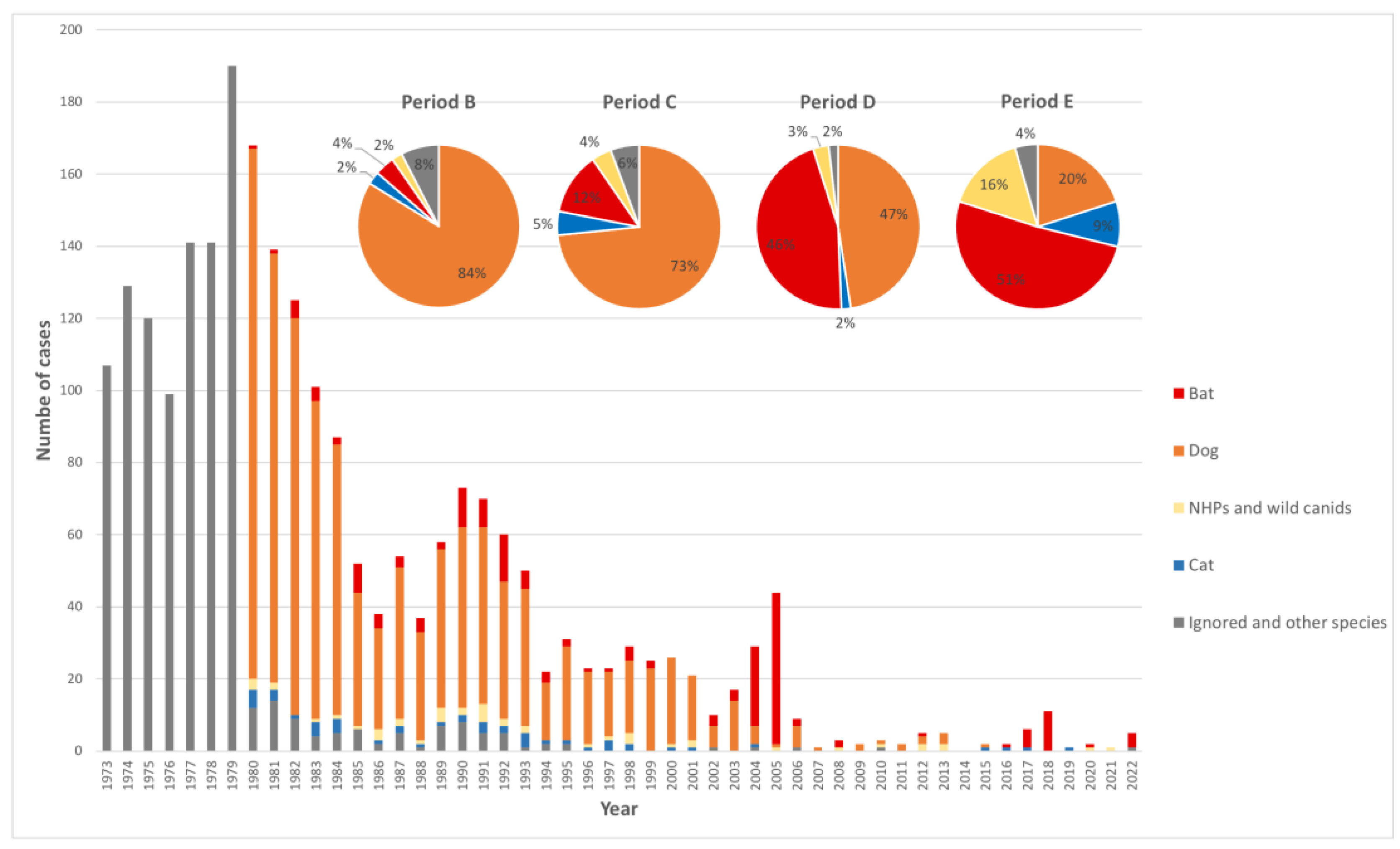
3.1.2. Period B, from 1980 to 1989—Reduction in Dog Transmissions
3.1.3. Period C, from 1990 to 1999—Increasing the Number of Human Cases Transmitted by Bats
3.1.4. Period D, from 2000 to 2010—The Shift between Cases Mediated by Virus in Dogs to Those Transmitted by Wild Animals
3.1.5. Period E, from 2010 to 2022—Almost Eliminating Human Cases Mediated by Dogs and Increasing the Wild Canid Cases
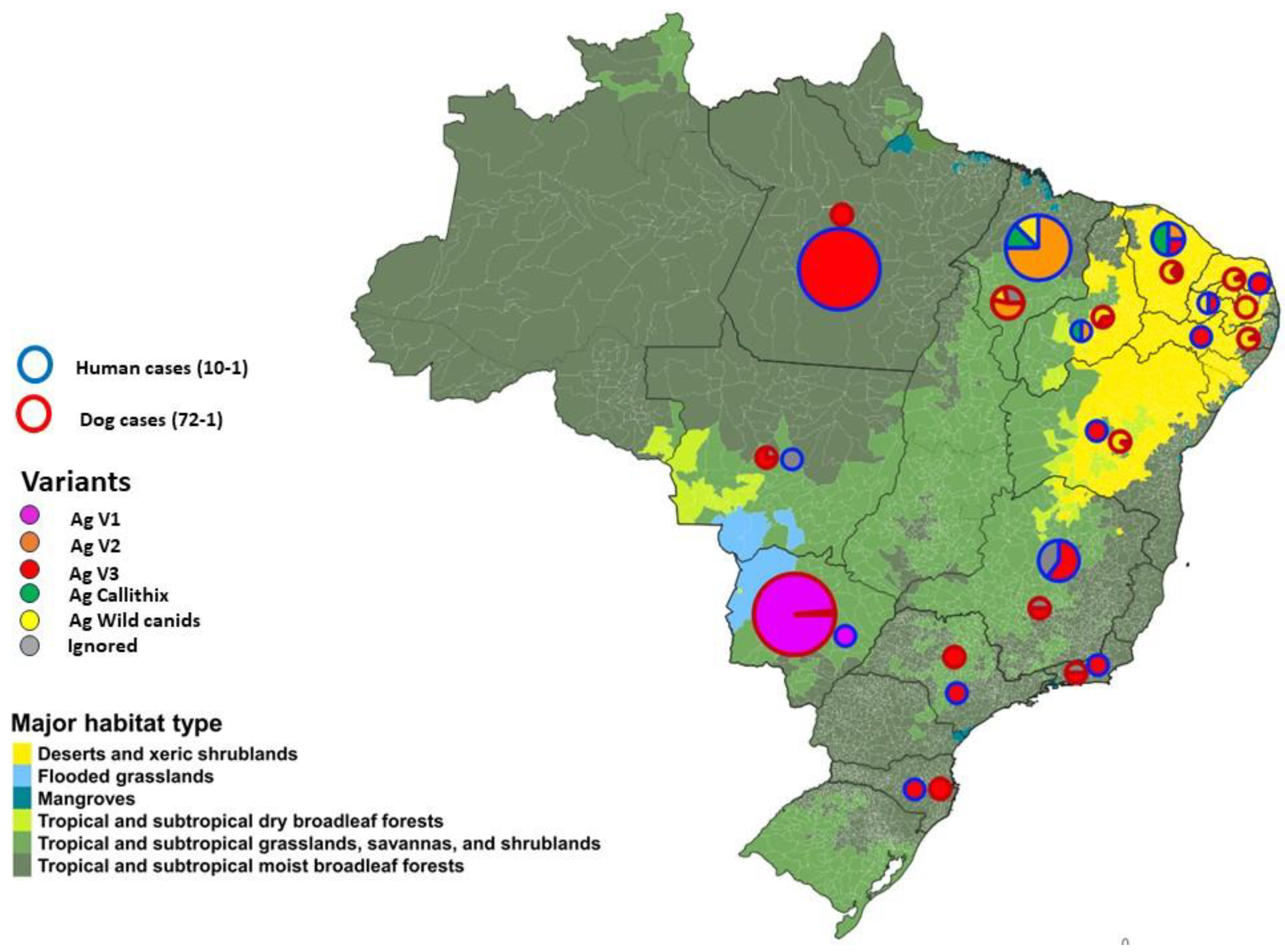
Rabies Virus Variants in Brazil
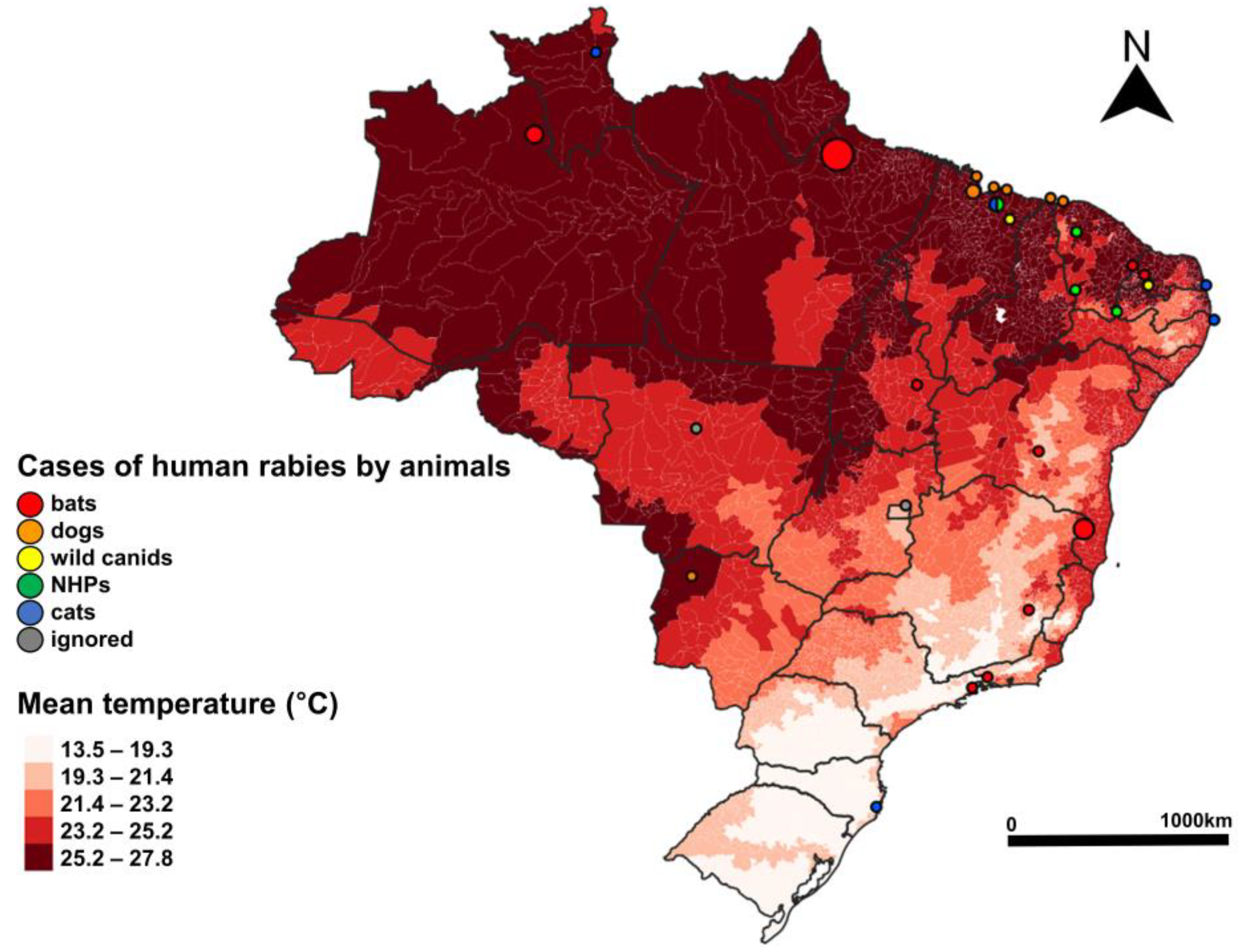
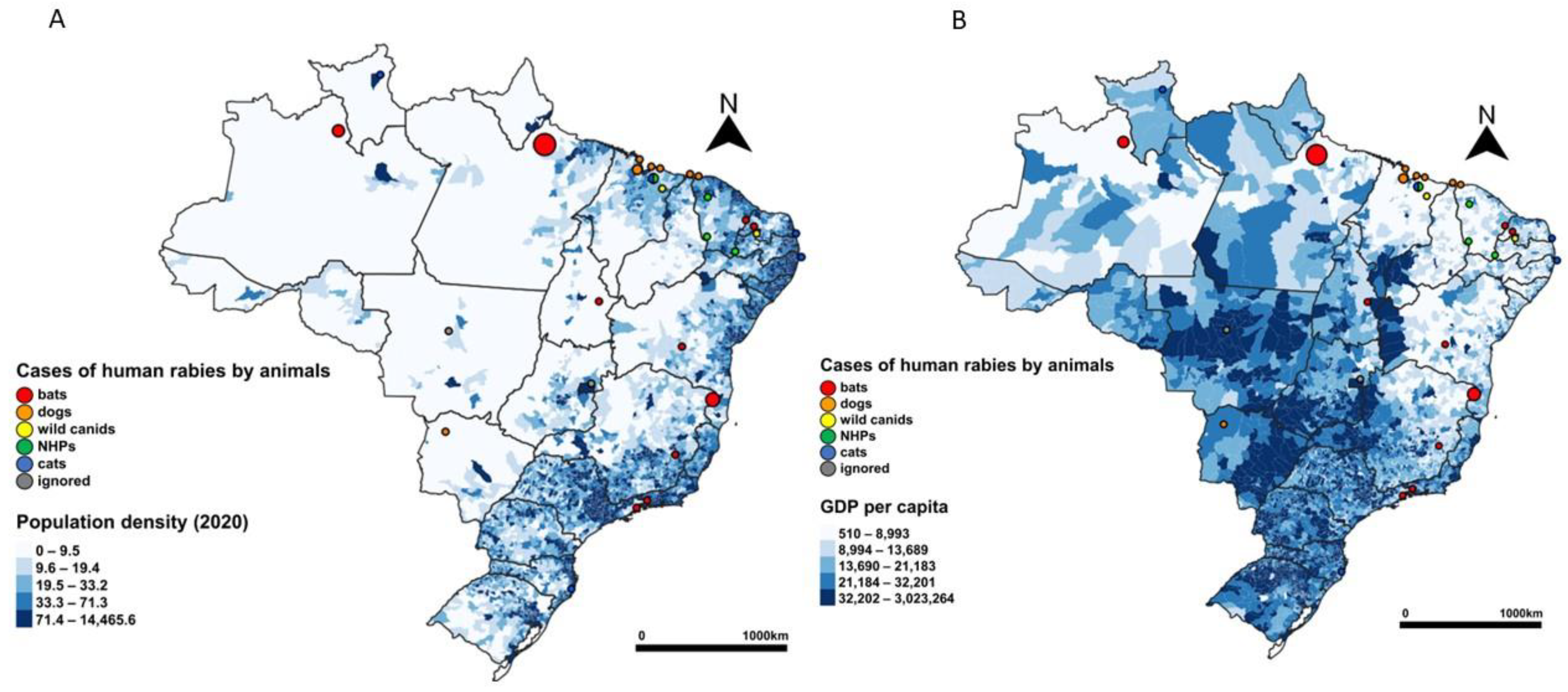
3.2. Part 2—Exploring Possible Drivers during Period D (2010 to 2022)
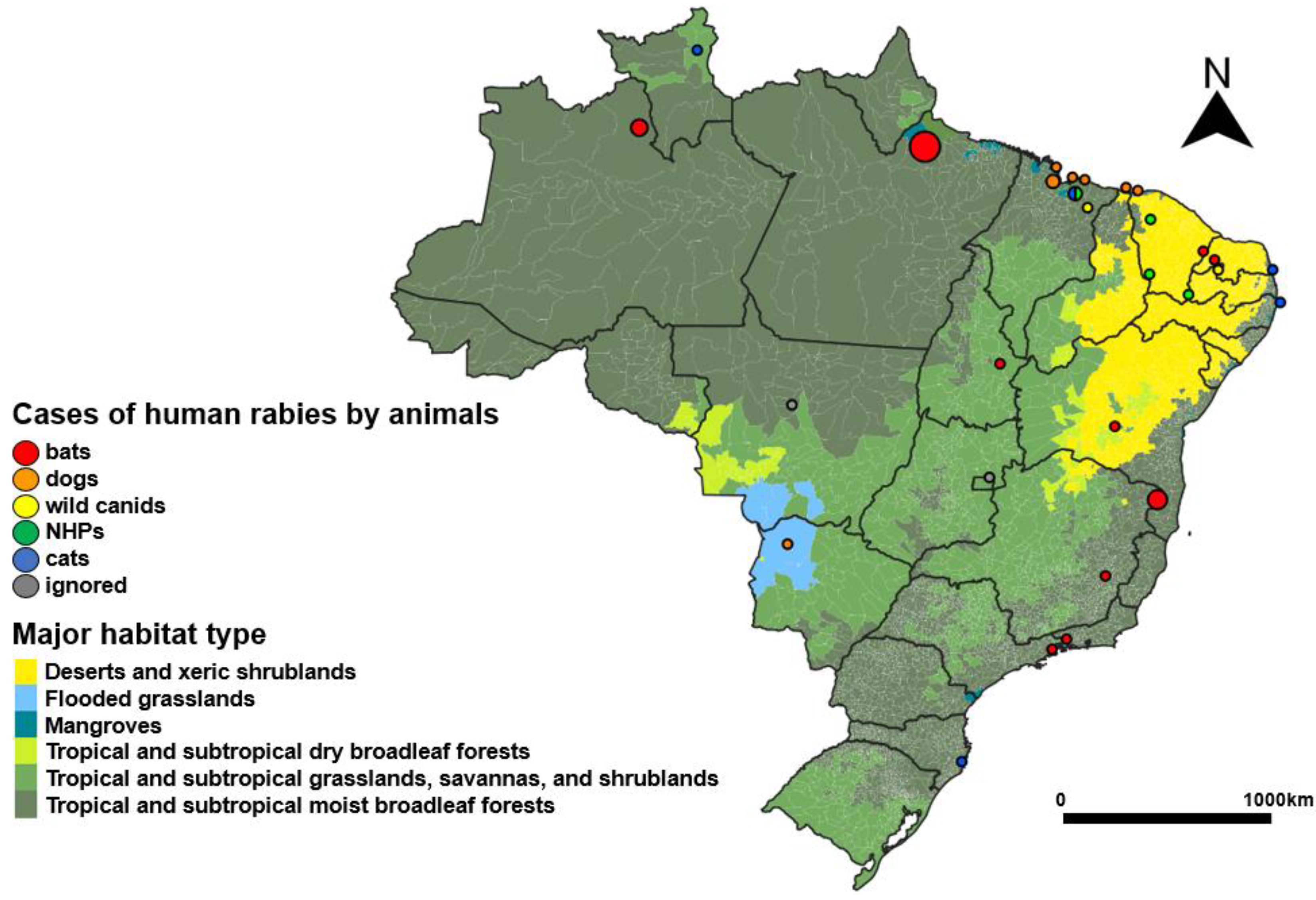
3.2.1. Describing the Human Cases in the Country over Selected Possible Drivers
3.2.2. Descriptive and Statistical Analysis of the Northeast Region
4. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Rupprechet, C.E.; Barrett, J.; Briggs, D.; Cliquet, F.; Fooks, A.R.; Lumlertdacha, B.; Meslin, F.X.; Müler, T.; Nel, L.H.; Schneider, C.; et al. Can rabies be eradicated? Dev. Biol. 2008, 131, 95–121. Available online: https://europepmc.org/article/med/18634470#impact (accessed on 8 July 2023).
- WHO. WHO Expert Consultation on Rabies, 3rd Report; WHO Technical Report Series, No. 1012; WHO: Geneva, Switzerland, 2018; Available online: https://www.who.int/publications/i/item/WHO-TRS-1012 (accessed on 4 August 2023).
- Hampson, K.; Coudeville, L.; Lembo, T.; Sambo, M.; Kieffer, A.; Attlan, M.; Barrat, J.; Blanton, J.D.; Briggs, D.J.; Cleaveland, S.; et al. Correction: Estimating the Global Burden of Endemic Canine Rabies. PLoS Negl. Trop. Dis. 2015, 9, e0003786. [Google Scholar] [CrossRef] [PubMed]
- Wunner, W.H.; Briggs, D.J. Rabies in the 21st Century. PLoS Negl. Trop. Dis. 2010, 4, e591. [Google Scholar] [CrossRef]
- WHO. Ending the Neglect to Attain the Sustainable Development Goals: A Road Map for Neglected Tropical Diseases 2021–2030; World Health Organization: Geneva, Switzerland, 2020; p. 196. Available online: https://www.who.int/publications/i/item/9789240010352 (accessed on 9 August 2023).
- Minghui, R.; Stone, M.; Semedo, M.H.; Nel, L. New global strategic plan to eliminate dog-mediated rabies by 2030. Lancet Glob. Health 2018, 6, e828–e829. Available online: https://pubmed.ncbi.nlm.nih.gov/29929890/ (accessed on 4 August 2023). [CrossRef] [PubMed]
- Freire de Carvalho, M.; Vigilato, M.A.N.; Pompei, J.A.; Rocha, F.; Vokaty, A.; Molina-Flores, B.; Cosivi, O.; Del Rio Vilas, V. Rabies in the Americas: 1998–2014. PLoS Negl. Trop. Dis. 2018, 12, e0006271. [Google Scholar] [CrossRef]
- Schneider, M.C.; Pereira, L.R.M. Substantial reductions in rabies, but still a lot to be done. Lancet Glob. Health 2017, 5, e957–e958. Available online: https://pubmed.ncbi.nlm.nih.gov/28911756/ (accessed on 10 September 2023). [CrossRef] [PubMed]
- Vigilato, M.A.; Clavijo, A.; Knobl, T.; Silva, H.M.; Cosivi, O.; Schneider, M.C.; Leanes, L.F.; Belotto, A.J.; Espinal, M.A. Progress towards eliminating canine rabies: Policies and perspectives from Latin America and the Caribbean. Philos. Trans. R. Soc. Lond. B Biol. Sci. 2013, 368, 20120143. Available online: https://pubmed.ncbi.nlm.nih.gov/23798691/ (accessed on 15 July 2023). [CrossRef]
- Clavijo, A.; Del Rio Vilas, V.J.; Mayen, F.L.; Yadon, Z.E.; Beloto, A.J.; Vigilato, M.A.; Schneider, M.C.; Cosivi, O. Gains and future road map for the elimination of dog-transmitted rabies in the Americas. Am. J. Trop. Med. Hyg. 2013, 89, 1040–1042. Available online: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3854880/ (accessed on 20 August 2023). [CrossRef]
- Schneider, M.C.; Aguilera, X.P.; Barbosa da Silva Junior, J.; Ault, S.K.; Najera, P.; Martinez, J.; Requejo, R.; Nicholls, R.S.; Yadon, Z.; Silva, J.C.; et al. Elimination of Neglected Diseases in Latin America and the Caribbean: A Mapping of Selected Diseases. PLoS Negl. Trop. Dis. 2011, 5, e964. [Google Scholar] [CrossRef]
- Schneider, M.C.; Belotto, A.; Adé, M.P.; Hendrickx, S.; Leanes, L.F.; Rodrigues, M.J.; Medina, G.; Correa, E. Current status of human rabies transmitted by dogs in Latin America. Cad. Saude Publica 2007, 23, 2049–2063. Available online: https://pubmed.ncbi.nlm.nih.gov/17700940/ (accessed on 20 August 2023). [CrossRef]
- Belotto, A.; Leanes, L.F.; Schneider, M.C.; Tamayo, H.; Correa, E. Overview of rabies in the Americas. Virus Res. 2005, 111, 5–12. Available online: https://pubmed.ncbi.nlm.nih.gov/15896398/ (accessed on 10 September 2023). [CrossRef]
- Schneider, M.C.; Belotto, A.; Adé, M.P.; Leanes, L.F.; Correa, E.; Tamoyo, H.; Medina, G.; Rodrigues, M.J. Epidemiologic situation of human rabies in Latin America in 2004. Epidemiol. Bull. 2005, 26, 2–4. [Google Scholar]
- Schneider, M.C.; Munoz-Zanzi, C.; Min, K.; Aldighieri, S. “One health” from concept to application in the global world. In Oxford Research Encyclopedia of Global Public Health; Oxford University Press: Oxford, UK, 2019; Available online: https://oxfordre.com/publichealth/display/10.1093/acrefore/9780190632366.001.0001/acrefore-9780190632366-e-29?rskey=2si5Zz&result=35 (accessed on 28 May 2023).
- Moraes, N.B.; Schneider, M.C.; Lima Junior, F.E.F.; Andrade Filho, G.V.; Costa, J.R.R.; Camargo, L.E.B.; Romijn, P.C. A Evolução da Saúde Pública Veterinária no Brasil: Do Controle da Raiva à Saúde Única; Revista Conselho Federal de Medicina Veterinária: Brasília, Brazil, 2020; Volume 85. Available online: https://www.cfmv.gov.br/wp-content/uploads/2020/09/revista85.pdf (accessed on 28 May 2023).
- PAHO Panaftosa. Organización Panamericana de la Salud. Sistema de Informação Regional Pará Vigilância Epidemiológica da Raiva.. Available online: https://sirvera.panaftosa.org.br/Site/Inicio/Index?idl=1 (accessed on 4 September 2023).
- King, L.J.; Anderson, L.R.; Blackmore, C.G.; Blackwell, M.J.; Lautner, E.A.; Marcus, L.C.; Meyer, T.E.; Monath, T.P.; Nave, J.E.; Ohle, J.; et al. Executive summary of the AVMA One Health Initiative Task Force report. J. Am. Vet. Med. Assoc. 2008, 233, 259–261. Available online: https://pubmed.ncbi.nlm.nih.gov/18627228/ (accessed on 17 September 2023). [CrossRef]
- Kaplan, B.; Kahn, L.H.; Monath, T.P. The brewing storm. Vet. Ital. 2009, 45, 9–18. Available online: https://www.izs.it/vet_italiana/2009/45_1/9.pdf (accessed on 17 September 2023).
- Rabinowitz, P.M.; Kock, R.; Kachani, M.; Kunkel, R.; Thomas, J.; Gilbert, J.; Wallace, R.; Blackmore, C.; Wong, D.; Karesh, W.; et al. Toward proof of concept of a One Health approach to disease prediction and control. Emerg. Infect. Dis. 2013, 19, e130265. Available online: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3840882/ (accessed on 17 September 2023). [CrossRef]
- One Health High-Level Expert Panel (OHHLEP); Adisasmito, W.B.; Almuhairi, S.; Behravesh, C.B.; Bilivogui, P.; Bukachi, S.A.; Casas, N.; Becerra, N.C.; Charron, D.F.; Chaudhary, A.; et al. One Health: A new definition for a sustainable and healthy future. PLoS Pathog. 2022, 18, e1010537. [Google Scholar] [CrossRef]
- FAO; OIE; WHO. Taking a Multisectoral, One Health Approach: A TripartiteGuide to Addreesing Zoonotic Diseases in Countries; World Health Organization (WHO), Food and Agriculture Organization of the United Nations (FAO) and World Organisation for Animal Health (OIE): Geneva, Switzerland, 2019; Available online: https://www.who.int/initiatives/tripartite-zoonosis-guide (accessed on 9 August 2023).
- FAO; UNEP; WHO; WOAH. One Health Joint Plan of Action (2022–2026). Working Together for the Health of Humans, Animals, Plants and the Environment; FAO; UNEP; WHO; World Organisation for Animal Health (WOAH) (founded as OIE): Rome, Italy, 2022; p. 86. Available online: https://www.fao.org/documents/card/en/c/cc2289en (accessed on 9 August 2023).
- Badrane, H.; Tordo, N. Host switching in Lyssavirus history from the Chiroptera to the Carnivora orders. J. Virol. 2001, 75, 8096–8104. Available online: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC115054/ (accessed on 12 June 2023). [CrossRef]
- Schneider, M.C. Rabia Humana Transmitida por Murciélago Hematófago en Brasil: Modelo de Transmisión y acciones de Control. Ph.D. Thesis, Instituto Nacional de Salud Pública, Cuernavaca, Mexico, 1996. [Google Scholar]
- Lord, R.D. Manual de Campanha Pará o Controle de Morcegos Vampiros e da Raiva; Bat Conservation International: Austin, TX, USA, 1998; p. 39. [Google Scholar]
- Morato, F. Raiva: Uma doença antiga, mas ainda atual. Rev. Educ. Contin. Med. Veterinária Zootec. CRMV-SP (Rev. MVZ). 2011, 9, 20–29. Available online: https://www.revistamvez-crmvsp.com.br/index.php/recmvz/article/view/173 (accessed on 4 June 2023). [CrossRef]
- Ministerio da Saude do Brasil. Guia de Vigilancia em Saude, 3rd ed.; Ministério da Saúde: Brasília, DF, Brazil, 2019; Volume único. Available online: https://bvsms.saude.gov.br/bvs/publicacoes/guia_vigilancia_saude_3ed.pdf (accessed on 5 June 2023).
- Batista-Morais, N.; Neilson-Rolim, B.; Matos- Chaves, H.H.; Matos-Chaves, H.H.; Brito-Neto, J.; Maria-da-Silva, L. Rabies in Tamarins (Callithrix jacchus) in the State of Ceará, Brazil, a Distinct Viral Variant? J. Microbes Their Vectors Causing Hum. Infect. 2000, 95, 609–610. Available online: https://memorias.ioc.fiocruz.br/article/2728/rabies-in-tamarins-callithrix-jacchus-in-the-state-of-cear%C3%A1-brazil-a-distinct-viral-variant (accessed on 4 June 2023).
- IBGE. Fundação Instituto Brasileiro de Estatística. In Estimativas da População.; 2021. Available online: https://www.ibge.gov.br/estatisticas/sociais/populacao/9103-estimativas-de-populacao.html?edicao=31451&t=custom-data-edicao (accessed on 20 February 2023).
- Castro, M.C.; Massuda, A.; Almeida, G.; Menezes-Filho, N.A.; Andrade, M.V.; de Souza Noronha, K.V.M.; Rocha, R.; Macinko, J.; Hone, T.; Tasca, R.; et al. Brazil’s unified health system: The first 30 years and prospects for the future. Lancet 2019, 394, 345–356. Available online: https://pubmed.ncbi.nlm.nih.gov/31303318/ (accessed on 16 July 2023). [CrossRef] [PubMed]
- Ministério da Saúde, Brasil. E-Gestor AB. In Sistemas da Atenção Primaria a Saude. Histórico de Coberturas. Available online: https://egestorab.saude.gov.br/paginas/acessoPublico/relatorios/relHistoricoCobertura.xhtml (accessed on 5 February 2023).
- SINAN. Sistema de Informação de Agravos de Notificação. Casos de Raiva Humana; Ministério da Saúde: Brasília, DF, Brazil. Available online: https://www.gov.br/saude/pt-br/assuntos/saude-de-a-a-z/r/raiva (accessed on 23 February 2023).
- Ministerio da Saude do Brasil. Secretaria de Vigilancia em Saude e Ambiente. Raiva. Available online: https://www.gov.br/saude/pt-br/centrais-de-conteudo/publicacoes/svsa/raiva (accessed on 5 February 2023).
- Schneider, M.C. Estudo de Avaliação Sobre Área de Risco Pará a Raiva no Brasil. Master’s Thesis, Fundação Oswaldo Cruz, Escola Nacional de Saúde Pública, Rio de Janeiro, Brazil, 1990. [Google Scholar]
- Min, K.-D.; Schneider, M.C.; Cho, S. Association between predator species richness and human hantavirus infection emergence in Brazil. One Health 2020, 11, 100196. [Google Scholar] [CrossRef]
- Hamrick, P.N.; Aldighieri, S.; Machado, G.; Leonel, D.G.; Vilca, L.M.; Uriona, S.; Schneider, M.C. Geographic patterns and environmental factors associated with human yellow fever presence in the Americas. PLoS Negl. Trop. Dis. 2017, 11, e0005897. [Google Scholar] [CrossRef] [PubMed]
- Schneider, M.C.; Min, K.-D.; Hamrick, P.N.; Montebello, L.R.; Ranieri, T.M.; Mardini, L.; Camara, V.M.; Luiz, R.R.; Liese, B.; Vuckovic, M.; et al. Overview of snakebite in Brazil: Possible drivers and a tool for risk mapping. PLoS Negl. Trop. Dis. 2021, 15, e0009044. [Google Scholar] [CrossRef]
- FAO. FAO-GeoNetwork-Geo-Spatial-WWF Global Ecoregions Map. Available online: http://www.fao.org/geonetwork/srv/en/resources.get?id=1009&fname=1009.zip&access=private (accessed on 10 December 2014).
- WWF Global. Major Habitat Types. Available online: http://wwf.panda.org/about_our_earth/ecoregions/about/habitat_types/ (accessed on 10 December 2014).
- United Nations Environment Programme (UNEP) 2014. Available online: http://ede.grid.unep.ch//mod_download/download_geospatial.php?selectedID=1814&newFile=download/wwf_ecoreg_tot_po_shp.zip (accessed on 10 December 2014).
- Fick, S.E.; Hijmans, R.J. Worldclim 2: New 1-km spatial resolution climate surfaces for global land areas. Int. J. Climatol. 2017, 37, 4302–4315. Available online: https://www.worldclim.org/ (accessed on 2 September 2023). [CrossRef]
- Hansen, M.C.; Potapov, P.V.; Moore, R.; Hancher, M.; Turubanova, S.A.; Tyukavina, A.; Thau, D.; Stehman, S.V.; Goetz, S.J.; Loveland, T.R.; et al. High-resolution global maps of 21st-century forest cover change. Science 2013, 342, 850–853. Available online: https://earthenginepartners.appspot.com/science-2013-global-forest (accessed on 2 September 2023). [CrossRef]
- IBGE. Fundação Instituto Brasileiro de Estatística. In Producto Interno Bruto dos Municipios.; 2021. Available online: https://www.ibge.gov.br/estatisticas/economicas/contas-nacionais/9088-produto-interno-bruto-dos-municipios.html?=&t=downloads (accessed on 10 February 2023).
- Schneider, M.C.; Almeida, G.A.; Souza, L.M.; Morares, N.B.; Diaz, R.C. Controle da raiva no Brasil de 1980 a 1990. Rev. Saúde Pública 1996, 30, 196–203. Available online: https://pesquisa.bvsalud.org/portal/resource/pt/lil-168606 (accessed on 8 July 2023). [CrossRef]
- OPS. Eliminación de la Rabia Humana Transmitida por Perros en América Latina; Organização Pan-Americana de Saúde: Washington, DC, USA, 2005; p. 71. Available online: https://iris.paho.org/handle/10665.2/37534 (accessed on 29 July 2023).
- Lopez, A.; Miranda, P.; Tejada, E.; Fishbein, D.B. Outbreak of human rabies in the Peruvian jungle. Lancet 1992, 15, 408–411. Available online: https://pubmed.ncbi.nlm.nih.gov/1346669/ (accessed on 29 July 2023). [CrossRef] [PubMed]
- Schneider, M.C.; Santos-Burgoa, C.; Aron, J.; Munoz, B.; Ruiz-Velazco, S.; Uieda, W. Potential force of infection of human rabies transmitted by vampire bats in the Amazonian region of Brazil. Am. J. Trop. Med. Hyg. 1996, 55, 680–684. Available online: https://pubmed.ncbi.nlm.nih.gov/9025698/ (accessed on 29 July 2023). [CrossRef] [PubMed]
- Schneider, M.C.; Aron, J.; Santos-Burgoa, C.; Uieda, W.; Ruiz-Velazco, S. Common vampire bat attacks on humans in a village of the Amazon region of Brazil. Cad. Saúde Pública 2001, 17, 1531–1536. Available online: https://www.scielo.br/j/csp/a/mytWjDdRCZjLpb8w4bKn8Sn/abstract/?lang=pt (accessed on 28 July 2023). [CrossRef] [PubMed]
- Schneider, M.C.; Romijn, P.C.; Uieda, W.; Tamayo, H.; da Silva, D.F.; Belotto, A.; da Silva, J.B.; Leanes, L.F. Rabies transmitted by vampire bats to humans: An emerging zoonotic disease in Latin America? Rev. Panam. Salud Publica 2009, 25, 260–269. Available online: https://pubmed.ncbi.nlm.nih.gov/19454154/ (accessed on 28 July 2023). [CrossRef]
- Favoretto, S.R.; de Mattos, C.C.; Morais, N.B.; Alves Araújo, F.A.; de Mattos, C.A. Rabies in marmosets (Callithrix jacchus), Ceará, Brazil. Emerg. Infect. Dis. 2001, 7, 1062–1065. Available online: https://pubmed.ncbi.nlm.nih.gov/11747745/ (accessed on 2 September 2023). [CrossRef] [PubMed]
- Kotait, I.; Oliveira, R.N.; Carrieri, M.L.; Castilho, J.G.; Macedo, C.I.; Pereira, P.M.C.; Boere, V.; Montebello, L.; Rupprecht, C.E. Non-human primates as a reservoir for rabies virus in Brazil. Zoonoses Public Health 2018, 66, 47–59. [Google Scholar] [CrossRef]
- Benavides, J.A.; Raghavan, R.K.; Boere, V.; Rocha, S.; Wada, M.Y.; Vargas, A.; Voietta, F.; Silva, I.d.O.e.; Leal, S.; de Castro, A.; et al. Spatio-temporal dynamics of rabies and habitat suitability of the common marmoset Callithrix jacchus in Brazil. PLoS Neglected Trop Dis. 2022, 16, e0010254. [Google Scholar] [CrossRef]
- De Sousa, L.L.F.; de Souza, T.L.; Tibo, L.H.S.; Moura, F.B.P.; Junior, F.A.S.; de Oliveira-Filho, E.F.; Ludwig-Begall, L.F.; Cabral-Miranda, G.; Andreata-Santos, R.; Janini, L.M.R.; et al. Rabies virus variants from bats closely related to variants found in marmosets (Callithrix jacchus), a neglected source of human rabies infection in Brazil. J. Med. Virol. 2023, 95, e29046. Available online: https://pubmed.ncbi.nlm.nih.gov/37605969/ (accessed on 27 September 2023). [CrossRef] [PubMed]
- Wada, M.Y.; Rocha, S.M.; Maia-Elkoury, A.N.S. Situação da Raiva no Brasil, 2000 a 2009. Epidemiol. Serv. Saúde 2011, 20, 509–518. Available online: http://scielo.iec.gov.br/pdf/ess/v20n4/v20n4a10.pdf (accessed on 27 September 2023). [CrossRef]
- PAHO-Pan American Health Organization. Resolution CD49.R9. In Elimination of Neglected Diseases and Other Poverty-Related Infections; Forty-Ninth Directing Council: Washington, DC, USA, 2009; Available online: https://iris.paho.org/handle/10665.2/33933 (accessed on 9 August 2023).
- Kessels, J.A.; Recuenco, S.; Navarro-Vela, A.M.; Deray, R.; Vigilato, M.; Ertl, H.; Durrheim, D.; Rees, H.; Nel, L.H.; Abela-Ridder, B.; et al. Pre-exposure rabies prophylaxis: A systematic review. Bull. World Health Organ. 2017, 95, 210–219C. Available online: https://pubmed.ncbi.nlm.nih.gov/28250534/ (accessed on 16 October 2023). [CrossRef]
- Queiroz, L.H.; Favoretto, S.R.; Cunha, E.M.S.; Campos, A.C.A.; Lopes, M.C.; Carvalho, C.; Iamamoto, K.; Araujo, D.B.; Venditti, L.L.; Ribeiro, E.S. Rabies in southeast Brazil: A change in the epidemiological pattern. Arch. Virol. 2012, 157, 93–105. [Google Scholar] [CrossRef]
- Rocha, S.M.; de Oliveira, S.V.; Heinemann, M.B.; Gonçalves, V.S. Epidemiological Profile of Wild Rabies in Brazil (2002–2012). Transbound. Emerg. Dis. 2017, 64, 624–633. Available online: https://pubmed.ncbi.nlm.nih.gov/26423323/ (accessed on 16 October 2023). [CrossRef] [PubMed]
- BRASIL. Raiva Transmitida por Cachorros do Mato (Cerdocyon thous): Casos Humanos e Conhecimento, Atitudes e Práticas no Nordeste do Brasil. 2021. Available online: https://www.gov.br/saude/pt-br (accessed on 10 February 2023).
- Carnieli, P., Jr.; Ruthner Batista, H.B.; de Novaes Oliveira, R.; Castilho, J.G.; Vieira, L.F. Phylogeographic dispersion and diversification of rabies virus lineages associated with dogs and crab-eating foxes (Cerdocyon thous) in Brazil. Arch. Virol. 2013, 158, 2307–2313. Available online: https://pubmed.ncbi.nlm.nih.gov/23749047/ (accessed on 25 August 2023). [CrossRef]
- Ministério da Saúde. Secretaria de Vigilancia em Saude (2021). Bolhetim Epiemiogico 48. Volume 52 | Dez; 2021. Available online: https://www.gov.br/saude/pt-br/centrais-de-conteudo/publicacoes/boletins/epidemiologicos/edicoes/2021 (accessed on 10 February 2023).
- Cordeiro, R.A.; Duarte, N.F.H.; Rolim, B.N.; Soares Junior, F.A.; Franco, I.C.F.; Ferrer, L.L.; Almeida, C.P.; Duarte, B.H.; Araujo, D.B.; Rocha, M.F.G.; et al. The Importance of Wild Canids in the Epidemiology of Rabies in Northeast Brazil: A Retrospective Study. Zoonoses Public Health 2016, 63, 486–493. [Google Scholar] [CrossRef]
- Favoretto, S.R.; de Mattos, C.C.; de Mattos, C.A.; Campos, A.C.; Sacramento, D.R.; Durigon, E.L. The emergence of wildlife species as a source of human rabies infection in Brazil. Epidemiol. Infect. 2013, 141, 1552–1561. Available online: https://pubmed.ncbi.nlm.nih.gov/23433340/ (accessed on 20 October 2023). [CrossRef]
- Malukiewicz, J.; Boere, V.; de Oliveira, M.A.B.; D’arc, M.; Ferreira, J.V.A.; French, J.; Housman, G.; de Souza, C.I.; Jerusalinsky, L.; de Melo, F.R.; et al. An Introduction to the Callithrix Genus and Overview of Recent Advances in Marmoset Research. ILAR J. 2020, 61, 110–138. [Google Scholar] [CrossRef]
- Estima, N.M.; Wada, M.Y.; Rocha, S.M.; Moraes, D.S.; Ohara, P.M.; Vargas, A.; Assis, D. Descrição das notificações de atendimento antirrábico humano Pará profilaxia pós-exposição no Brasil, 2014–2019. Epidemiol. Serv. Saúde 2022, 31, e2021627. Available online: https://www.scielo.br/j/ress/a/KLDgrQQtbvWThG6ZD8cp3NG/?lang=pt (accessed on 24 July 2023). [CrossRef]
- Ministério da Saúde. Secretaria de Vigilância em Saúde (2020). In Bolhetim Epiemiogico 16. Volume 51 | Abr.; 2020. Available online: https://www.gov.br/saude/pt-br/centrais-de-conteudo/publicacoes/boletins/epidemiologicos/edicoes/2020/ (accessed on 10 February 2023).
- de Souza, D.N.; Carnieli, P., Jr.; Macedo, C.I.; de Novaes Oliveira, R.; de Carvalho Ruthner Batista, H.B.; Rodrigues, A.C.; Pereira, P.M.C.; Achkar, S.M.; Vieira, L.F.P.; Kawai, J.G.C. Phylogenetic analysis of rabies virus isolated from canids in North and Northeast Brazil. Arch. Virol. 2017, 162, 71–77. Available online: https://pubmed.ncbi.nlm.nih.gov/27671776/ (accessed on 15 July 2023). [CrossRef]
- Poch, O.; Blumberg, B.M.; Bougueleret, L.; Tordo, N. Sequence comparison of five polymerases (L proteins) of unsegmented negative-strand RNA viruses: Theoretical assignment of functional domains. J. Gen. Virol. 1990, 71, 1153–1162. Available online: https://pubmed.ncbi.nlm.nih.gov/2161049/ (accessed on 15 July 2023). [CrossRef]
- Ito, M.; Arai, Y.T.; Itou, T.; Sakai, T.; Ito, F.H.; Takasaki, T.; Kurane, I. Genetic characterization and geographic distribution of rabies virus isolates in Brazil: Identification of two reservoirs, dogs and vampire bats. Virology 2001, 284, 214–222. Available online: https://pubmed.ncbi.nlm.nih.gov/11384221/ (accessed on 14 October 2023). [CrossRef]
- Wanderler, A.I.; Matter, H.C.; Kappeler, A.; Budde, A. The ecology of dogs and canine rabies: A selective review. Rev. Sci. Tech. (Int. Off. Epizoot.) 1993, 12, 51–71. Available online: https://doc.woah.org/dyn/portal/index.xhtml?page=alo&aloId=26281 (accessed on 14 October 2023). [CrossRef]
- Mattos, C.A.; Favi, M.; Yung, V.; Pavletic, C.; Mattos, C.C. Bat Rabies in Urban Centers in Chile. J. Wildl. Dis. 2000, 36, 231–240. Available online: https://meridian.allenpress.com/jwd/article/36/2/231/122628/BAT-RABIES-IN-URBAN-CENTERS-IN-CHILE (accessed on 16 October 2023). [CrossRef] [PubMed]
- Romijn, P.C.; van der Heide, R.; Cattaneo, C.A.; Silva, R.d.C.; van der Poel, W.H. Study of lyssaviruses of bat origin as a source of rabies for other animal species in the State of Rio De Janeiro, Brazil. Am. J. Trop. Med. Hyg. 2003, 69, 81–86. Available online: https://pubmed.ncbi.nlm.nih.gov/12932103/ (accessed on 22 September 2023). [CrossRef]
- Postic, B.; DeAngelis, C.; Breinig, M.K.; Monto, H.O. Effect of temperature on the induction of interferons by endotoxin and virus. J. Bacteriol. 1966, 91, 1277–1281. Available online: https://pubmed.ncbi.nlm.nih.gov/5929756/ (accessed on 23 September 2023). [CrossRef] [PubMed]
- Moriyama, M.; Ichinohe, T. High ambient temperature dampens adaptive immune responses to influenza A virus infection. Proc. Natl. Acad. Sci. USA 2019, 116, 3118–3125. [Google Scholar] [CrossRef]
- Carlson, C.J.; Albery, G.F.; Merow, C.; Trisos, C.H.; Zipfel, C.M.; Eskew, E.A.; Olival, K.J.; Ross, N.; Bansal, S. Climate change increases cross-species viral transmission risk. Nature 2022, 607, 555–562. [Google Scholar] [CrossRef]
- Olival, K.; Hosseini, P.; Zambrana-Torrelio, C.; Ross, N.; Bogich, T.L.; Daszak, P. Host and viral traits predict zoonotic spillover from mammals. Nature 2017, 546, 646–650. [Google Scholar] [CrossRef]
- Hoberg, E.P.; Brooks, D.R. Evolution in action: Climate change, biodiversity dynamics and emerging infectious disease. Philos. Trans. R. Soc. Lond. B Biol. Sci. 2015, 370, 20130553. Available online: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4342959/ (accessed on 18 August 2023). [CrossRef]
- Morales-Castilla, I.; Pappalardo, P.; Farrell, J.; Alonso Aguirre, A.; Huong, S.; Gehman, A.-L.M.; Dalla, T.; Gravel, D.; Jonathan Davies, R. Forecasting Parásite sharing under climate change. Philos. Trans. R. Soc. 2021, 376, 20200360. [Google Scholar] [CrossRef]
- Lee, D.N.; Papeş, M.; Van Den Bussche, R.A. Present and Potential Future Distribution of Common Vampire Bats in the Americas and the Associated Risk to Cattle. PLoS ONE 2012, 7, e42466. [Google Scholar] [CrossRef]
- Hayes, M.A.; Piaggio, A.J. Assessing the potential impacts of a changing climate on the distribution of a rabies virus vector. PLoS ONE 2018, 13, e0192887. [Google Scholar] [CrossRef]
- Carlson, C.J.; Zipfel, C.M.; Garnier, R.; Bansal, S. Global estimates of mammalian viral diversity accounting for host sharing. Nat. Ecol. Evol. 2019, 3, 1070–1075. Available online: https://pubmed.ncbi.nlm.nih.gov/31182813/ (accessed on 5 September 2023). [CrossRef]
- Giovanella, L.; Bousquat, A.; Schenkman, S.; Almeida, P.F.; Sardinha, L.M.; Vieira, M.L.F.P. Cobertura da Estratégia Saúde da Família no Brasil: O que nos mostram as Pesquisas Nacionais de Saúde 2013 e 2019. Ciênc. Saúde Coletiva 2023, 26, 2543–2556. Available online: https://www.scielo.br/j/csc/a/SMZVrPZRgHrCTx57H35Ttsz/?lang=pt# (accessed on 25 October 2023). [CrossRef]
- Bastos, V.; Mota, R.; Guimarães, M.; Richard, Y.; Lima, A.L.; Casseb, A.; Barata, G.C.; Andrade, J.; Casseb, L.M.N. Challenges of Rabies Surveillance in the Eastern Amazon: The Need of a One Health Approach to Predict Rabies Spillover. Front. Public Health 2021, 9, 624574. [Google Scholar] [CrossRef]
- da Silva, R.M.; Megid, J.; Hampson, K.; Campos, A.A.S.; Higashi, C.S.; Medeiros, F.S.; Pereira, A.S.; Benavides, J.A. Factors Limiting the Appropriate Use of Rabies Post-exposure Prophylaxis by Health Professionals in Brazil. Front. Vet. Sci. 2022, 9, 846994. Available online: https://pubmed.ncbi.nlm.nih.gov/35601400/ (accessed on 27 October 2023). [CrossRef] [PubMed]
- Souza, P.C.A.; Schneider, M.C.; Simões, M.; Fonseca, A.G.; Vilhena, M. A Concrete Example of the One Health Approach in the Brazilian Unified Health System. Front. Public Health 2021, 9, 618234. [Google Scholar] [CrossRef] [PubMed]
- Porta, M. A Dictionary of Epidemiology, 6th ed.; Oxford University Press: Oxford, UK, 2016; Available online: https://www.oxfordreference.com/display/10.1093/acref/9780199976720.001.0001/acref-9780199976720 (accessed on 17 September 2023).







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Region | Population | GDP per Capita | 1980–989 Period A | 1990–999 Period B | 2000–2009 Period C | 2010–2022 Period D | Total | Percent (%) | ||
|---|---|---|---|---|---|---|---|---|---|---|
| State | ||||||||||
| North | 18,672,591 | 25,608 | 132 | 86 | 61 | 15 | 294 | 19.71 | ||
| Acre | 894,470 | 18.420 | 0 | 16 | 03 | 0 | 19 | 3.42 | ||
| Amapá | 861,773 | 21.432 | 7 | 01 | 0 | 0 | 8 | 1.27 | ||
| Amazonas | 4,207,714 | 27.573 | 31 | 06 | 02 | 03 | 42 | 2.82 | ||
| Pará | 8,690,745 | 24.847 | 73 | 35 | 45 | 10 | 163 | 10.92 | ||
| Rondônia | 1,796,460 | 28.722 | 21 | 21 | 09 | 0 | 51 | 3.42 | ||
| Roraima | 631,181 | 25.388 | 0 | 0 | 0 | 01 | 1 | 0.07 | ||
| Tocantins | 1,590,248 | 27.448 | 0 | 07 | 02 | 01 | 10 | 0.67 | ||
| Northeast | 53,374,243 | 18,812 | 456 | 239 | 85 | 19 | 799 | 53.55 | ||
| Alagoas | 3,351,543 | 18.858 | 71 | 26 | 05 | 0 | 102 | 6.84 | ||
| Bahia | 14,930,634 | 20.449 | 82 | 55 | 09 | 01 | 147 | 9.85 | ||
| Ceará | 9,187,103 | 18.168 | 94 | 29 | 13 | 04 | 140 | 9.38 | ||
| Maranhão | 7,114,598 | 15.028 | 50 | 55 | 48 | 08 | 161 | 10.79 | ||
| Paráíba | 4,039,277 | 17.402 | 22 | 14 | 0 | 02 | 38 | 2.55 | ||
| Pernambuco | 9,616,621 | 20.101 | 78 | 40 | 04 | 01 | 123 | 8.24 | ||
| Piauí | 3,281,480 | 17.185 | 26 | 12 | 03 | 02 | 43 | 2.88 | ||
| Rio Grande do Norte | 3,534,165 | 20.342 | 26 | 02 | 00 | 01 | 29 | 1.94 | ||
| Sergipe | 2,318,822 | 19.583 | 7 | 06 | 03 | 0 | 16 | 1.07 | ||
| Southeast | 89,012,240 | 44,406 | 184 | 48 | 10 | 07 | 249 | 16.69 | ||
| Espírito Santo | 4,064,052 | 34.066 | 07 | 07 | 02 | 0 | 16 | 1.07 | ||
| Minas Gerais | 21,292,666 | 32.067 | 65 | 35 | 06 | 05 | 111 | 7.44 | ||
| Rio de Janeiro | 17,366,189 | 43.408 | 59 | 0 | 01 | 01 | 61 | 4.09 | ||
| São Paulo | 46,289,333 | 51.365 | 53 | 06 | 01 | 01 | 61 | 4.09 | ||
| South | 30,192,315 | 43,327 | 5 | 0 | 0 | 01 | 6 | 0.40 | ||
| Paráná | 11,516,840 | 42.367 | 1 | 0 | 0 | 0 | 1 | 0.07 | ||
| Rio Grande do Sul | 11,422,973 | 41.228 | 1 | 0 | 0 | 0 | 3 | 0.20 | ||
| Santa Catarina | 7,252,502 | 48.159 | 3 | 0 | 0 | 01 | 2 | 0.13 | ||
| Central-West | 16,504,303 | 47,942 | 96 | 38 | 07 | 03 | 144 | 9.65 | ||
| Federal District | 3,055,149 | 87.016 | 0 | 00 | 00 | 01 | 1 | 0.07 | ||
| Goiás | 7,113,540 | 31.507 | 81 | 25 | 03 | 0 | 109 | 7.31 | ||
| Mato Grosso | 3,526,220 | 50.663 | 9 | 11 | 04 | 01 | 25 | 1.68 | ||
| Mato Grosso do Sul | 2,809,394 | 43.649 | 6 | 02 | 0 | 01 | 9 | 0.60 | ||
| Total | 211,755,692 | 35.936 | 873 | 411 | 163 | 45 | 1492 | 100 | ||
| Groups of Indicators | Indicators |
|---|---|
| Epidemiological situation | Productive area: Where there is a known active transmission of the rabies virus to people and/or domestic animals within the past three years. Indicators: Cases of rabies in people and/or domestic animals. Silent area: Area in which the information system is considered unreliable; the recommendation is to send 0.2% of annual samples from the estimated canine population for laboratory diagnosis of rabies. Indicators: Number of canine samples sent. Vulnerability: Probability of the introduction of a case to an area where no cases have been occurring. Indicators: Number of cases of any kind in neighboring municipalities; number of imported canine cases; and presence of infected vampire bats in the area. Receptivity: Probability of the occurrence of new cases of rabies after virus introduction into an area. Indicators: Dog vaccination coverage; outbreak control; and observation of aggressive animals. |
| Control actions | Relationship between health units with treatment and population. Immunoglobulin application. Percentage of people treated in relation to those assisted. Percentage of treatment abandonment. Percentage of observed aggressive animals. Vaccination coverage. Outbreak control. Percentage of samples sent for diagnosis in relation to the canine population. Animal care centers. Existence of hematophagous bat control efforts. Existence of diagnostic laboratory. |
| Socioeconomic conditions | Proportional mortality. Migration. Population coverage of safe water. Income up to two minimum wage salaries. Illiteracy. |
| Risk Situation | Actions to Be Developed | |||
| Type I |
|
| ||
| Type II |
| Situation 1 With information system Situation 2 Without information system | To all
| Situation 1 Request from the health care services negative notification of people bitten by bats Situation 2 Active surveillance of people bitten by bats |
| Type III |
| Situation 1 With access to health care services Situation 2 Without access to health care services With suspicion of virus circulation | To all
| Situation 1 PEP of people bitten by bats Situation 2 PEP of people bitten by bats Pre-exposure vaccination for high-risk groups |
| Type IV |
| Situation 1 With access to health care services Situation 2 Without access to health care services With suspicion of virus circulation | To all
| Situation 1 PEP of people bitten by bats Situation 2 PEP of people bitten by bats Pre-exposure vaccination for high-risk groups |
| Region | Municipality (Population) | HR Bats | HR Dogs | HR Cats | HR NHP | HR Wild Canids | HR Ign | Variant | Zone | Major Habitat Type | Gini Index |
|---|---|---|---|---|---|---|---|---|---|---|---|
| State | |||||||||||
| North | 14 | 0 | 1 | 0 | 0 | 0 | |||||
| Amazonas | Barcelos (27,638) | 3 | 0 | 0 | 0 | 0 | 0 | AgV3 | R | TSMBF | 0.7367 |
| Pará | Melgaco (27,890) | 10 | 0 | 0 | 0 | 0 | 0 | AgV3 | R | TSMBF | 0.5537 |
| Roraima | Boa Vista (419,652) | 0 | 0 | 1 | 0 | 0 | 0 | AgV3 | U | TSGSS | 0.5936 |
| Tocantins | Ponte Alta do Tocantins (8116) | 1 | 0 | 0 | 0 | 0 | 0 | AgV3 | R | TSGSS | 0.6420 |
| Northeast | 3 | 8 | 2 | 4 | 2 | 0 | |||||
| Bahia | Parámirim (21,695) | 1 | 0 | 0 | 0 | 0 | 0 | AgV3 | R | TSMBF | 0.5134 |
| Ceará | Chaval (13,091) | 0 | 1 | 0 | 0 | 0 | 0 | AgV2 | R | DXS | 0.5062 |
| Ipu (42,058) | 0 | 0 | 0 | 1 | 0 | 0 | AgV Callithrix | R | DXS | 0.5648 | |
| Iracema (14,326) | 1 | 0 | 0 | 0 | 0 | 0 | AgV3 | R | DXS | 0.5562 | |
| Jati (8130) | 0 | 0 | 0 | 1 | 0 | 0 | AgV Callithrix | R | DXS | 0.4995 | |
| Maranhão | Chapadinha (80,195) | 0 | 0 | 0 | 0 | 1 | 0 | Wild canids | R | TSMBF | 0.6019 |
| Humberto de Campos (28,932) | 0 | 1 | 0 | 0 | 0 | 0 | AgV2 | U | TSMBF | 0.6312 | |
| Mirinzal (15,011) | 0 | 1 | 0 | 0 | 0 | 0 | AgV2 | U | TSMBF | 0.5160 | |
| Paco do Lumiar (123,747) | 0 | 1 | 0 | 0 | 0 | 0 | AgV2 | R | M | 0.5067 | |
| Sao Jose do Ribamar (179,028) | 0 | 2 | 0 | 0 | 0 | 0 | AgV2 | R/U | TSMBF | 0.5268 | |
| Sao Luis | 0 | 2 | 0 | 0 | 0 | 0 | AgV2 | U/U | TSMBF | 0.6266 | |
| Paráíba | Catole do Rocha (30,684) | 0 | 0 | 0 | 0 | 1 | 0 | Wild canids | R | DXS | 0.5046 |
| Jacarau (14,450) | 0 | 0 | 1 | 0 | 0 | 0 | AgV3 | R | DXS | 0.5499 | |
| Pernambuco | Recife (1,653,461) | 0 | 0 | 1 | 0 | 0 | 0 | AgV3 | U | M | 0.6894 |
| Piauí | Parnaiba (153,482) | 0 | 0 | 0 | 1 | 0 | 0 | AgV Callithrix | U | DXS | 0.5772 |
| Pio IX (18,459) | 0 | 0 | 0 | 1 | 0 | 0 | AgV Callithrix | R | DXS | 0.5749 | |
| Rio Grande do Norte | Frutuoso Gomes (4041) | 1 | 0 | 0 | 0 | 0 | 0 | AgV3 | R | DXS | 0.4768 |
| Southeast | 7 | 0 | 0 | 0 | 0 | 0 | |||||
| Minas Gerais | Bertopolis (4607) | 4 | 0 | 0 | 0 | 0 | 0 | (4)AgV3 | R | TSMBF | 0.5442 |
| Rio Casca (13,473) | 1 | 0 | 0 | 0 | 0 | 0 | AgV3 | R | TSMBF | 0.4741 | |
| Rio de Janeiro | Angra dos Reis (207,044) | 1 | 0 | 0 | 0 | 0 | 0 | AgV3 | R | M | 0.5293 |
| São Paulo | Ubatuba (91,824) | 1 | 0 | 0 | 0 | 0 | 0 | AgV3 | PU | TSMBF | 0.5971 |
| South | 0 | 0 | 1 | 0 | 0 | 0 | |||||
| Santa Catarina | Gravatal (11,577) | 0 | 0 | 1 | 0 | 0 | 0 | AgV3 | R | TSMBF | 0.3993 |
| Central-West | 0 | 1 | 0 | 0 | 0 | 2 | |||||
| Federal District | Brasilia (3,055,149) | 0 | 0 | 0 | 0 | 0 | 1 | AgV3 | U | TSGSS | 0.6370 |
| Mato Grosso | Tapurah (14,046) | 0 | 0 | 0 | 0 | 0 | 1 | AgV3 | R | TSMBF | 0.5586 |
| Mato Grosso do Sul | Corumbá (112,058) | 0 | 1 | 0 | 0 | 0 | 0 | AgV1 | U | FG | 0.5589 |
| Total | 24 | 9 | 4 | 4 | 2 | 2 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Schneider, M.C.; Min, K.-D.; Romijn, P.C.; De Morais, N.B.; Montebello, L.; Manrique Rocha, S.; Sciancalepore, S.; Hamrick, P.N.; Uieda, W.; Câmara, V.d.M.; et al. Fifty Years of the National Rabies Control Program in Brazil under the One Health Perspective. Pathogens 2023, 12, 1342. https://doi.org/10.3390/pathogens12111342
Schneider MC, Min K-D, Romijn PC, De Morais NB, Montebello L, Manrique Rocha S, Sciancalepore S, Hamrick PN, Uieda W, Câmara VdM, et al. Fifty Years of the National Rabies Control Program in Brazil under the One Health Perspective. Pathogens. 2023; 12(11):1342. https://doi.org/10.3390/pathogens12111342
Chicago/Turabian StyleSchneider, Maria Cristina, Kyung-Duk Min, Phyllis Catharina Romijn, Nelio Batista De Morais, Lucia Montebello, Silene Manrique Rocha, Sofia Sciancalepore, Patricia Najera Hamrick, Wilson Uieda, Volney de Magalhães Câmara, and et al. 2023. "Fifty Years of the National Rabies Control Program in Brazil under the One Health Perspective" Pathogens 12, no. 11: 1342. https://doi.org/10.3390/pathogens12111342