
Clinical Spectrum, Radiological Findings, and Outcomes of Severe Toxoplasmosis in Immunocompetent Hosts: A Systematic Review
 , , , ,
, , , ,
Abstract
:1. Background
2. Methods
2.1. Inclusion Criteria
2.2. Exclusion Criteria
2.3. Data Extraction
2.4. Analyses
3. Results
3.1. Primary Analysis (1985–2022)
3.2. Duration of Symptoms
3.3. Diagnostic Methods
3.4. Type of Infection
3.5. Risk Factors
3.6. Ascertainment of Immunocompetent Status
3.7. Toxoplasmic Manifestations
3.8. Clinical Findings
3.9. Laboratory Findings
3.10. Imaging Findings
3.10.1. Lung Imaging
3.10.2. CNS Imaging
3.10.3. Cardiac Imaging
3.11. Anti-Toxoplasma Therapy
3.12. Outcomes
3.13. Time to Resolution
3.14. Secondary Analysis (1941–1984)
4. Discussion
4.1. Clinical Suspicion of Toxoplasmic Pneumonia
4.2. Clinical Suspicion of Toxoplasmic Cardiac Involvement
4.3. Clinical Suspicion of Toxoplasmic CNS Involvement
4.4. Differential Diagnosis
4.5. Risk Factors for Severe Toxoplasmosis
4.6. Diagnostic Methods
4.7. Prior Reviews
5. Conclusions
Additional Information
Author Contributions
Funding
Institutional Review Board Statement
Data Availability Statement
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
| Section and Topic | Item # | Checklist Item | Location Where Item Is Reported |
|---|---|---|---|
| TITLE | |||
| Title | 1 | Identify the report as a systematic review. | Page 1 |
| ABSTRACT | |||
| Abstract | 2 | See the PRISMA 2020 for Abstracts checklist. | Page 1–2 |
| INTRODUCTION | |||
| Rationale | 3 | Describe the rationale for the review in the context of existing knowledge. | Page 2–3 |
| Objectives | 4 | Provide an explicit statement of the objective(s) or question(s) the review addresses. | Page 2–3 |
| METHODS | |||
| Eligibility criteria | 5 | Specify the inclusion and exclusion criteria for the review and how studies were grouped for the syntheses. | Page 4–5 |
| Information sources | 6 | Specify all databases, registers, websites, organisations, reference lists and other sources searched or consulted to identify studies. Specify the date when each source was last searched or consulted. | Page 3 |
| Search strategy | 7 | Present the full search strategies for all databases, registers and websites, including any filters and limits used. | Page 4 (Appendix A, Page 18) |
| Selection process | 8 | Specify the methods used to decide whether a study met the inclusion criteria of the review, including how many reviewers screened each record and each report retrieved, whether they worked independently, and if applicable, details of automation tools used in the process. | Page 3 |
| Data collection process | 9 | Specify the methods used to collect data from reports, including how many reviewers collected data from each report, whether they worked independently, any processes for obtaining or confirming data from study investigators, and if applicable, details of automation tools used in the process. | Page 5 |
| Data items | 10a | List and define all outcomes for which data were sought. Specify whether all results that were compatible with each outcome domain in each study were sought (e.g., for all measures, time points, analyses), and if not, the methods used to decide which results to collect. | Page 5 |
| 10b | List and define all other variables for which data were sought (e.g., participant and intervention characteristics, funding sources). Describe any assumptions made about any missing or unclear information. | Page 5 | |
| Study risk of bias assessment | 11 | Specify the methods used to assess risk of bias in the included studies, including details of the tool(s) used, how many reviewers assessed each study and whether they worked independently, and if applicable, details of automation tools used in the process. | N/A |
| Effect measures | 12 | Specify for each outcome the effect measure(s) (e.g., risk ratio, mean difference) used in the synthesis or presentation of results. | N/A |
| Synthesis methods | 13a | Describe the processes used to decide which studies were eligible for each synthesis (e.g., tabulating the study intervention characteristics and comparing against the planned groups for each synthesis (item #5)). | N/A |
| 13b | Describe any methods required to prepare the data for presentation or synthesis, such as handling of missing summary statistics, or data conversions. | N/A | |
| 13c | Describe any methods used to tabulate or visually display results of individual studies and syntheses. | N/A | |
| 13d | Describe any methods used to synthesize results and provide a rationale for the choice(s). If meta-analysis was performed, describe the model(s), method(s) to identify the presence and extent of statistical heterogeneity, and software package(s) used. | N/A | |
| 13e | Describe any methods used to explore possible causes of heterogeneity among study results (e.g., subgroup analysis, meta-regression). | N/A | |
| 13f | Describe any sensitivity analyses conducted to assess robustness of the synthesized results. | N/A | |
| Reporting bias assessment | 14 | Describe any methods used to assess risk of bias due to missing results in a synthesis (arising from reporting biases). | N/A |
| Certainty assessment | 15 | Describe any methods used to assess certainty (or confidence) in the body of evidence for an outcome. | N/A |
| RESULTS | |||
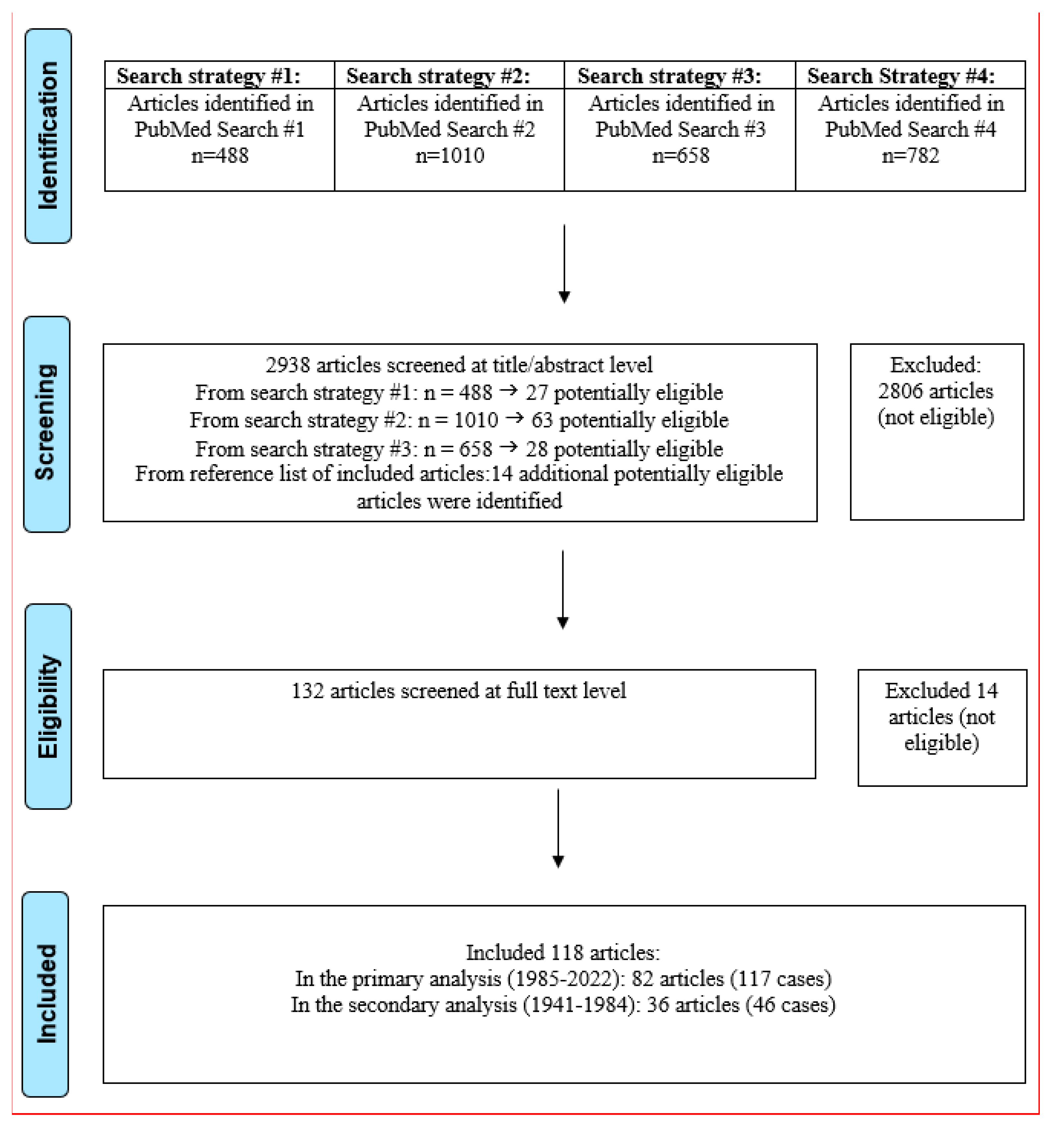
| Study selection | 16a | Describe the results of the search and selection process, from the number of records identified in the search to the number of studies included in the review, ideally using a flow diagram. | Page 3 |
| 16b | Cite studies that might appear to meet the inclusion criteria, but which were excluded, and explain why they were excluded. | N/A | |
| Study characteristics | 17 | Cite each included study and present its characteristics. | Appendix B, page 21–25, Appendix C-Table A10, page 54–55 |
| Risk of bias in studies | 18 | Present assessments of risk of bias for each included study. | N/A |
| Results of individual studies | 19 | For all outcomes, present, for each study: (a) summary statistics for each group (where appropriate) and (b) an effect estimate and its precision (e.g., confidence/credible interval), ideally using structured tables or plots. | N/A |
| Results of syntheses | 20a | For each synthesis, briefly summarize the characteristics and risk of bias among contributing studies. | N/A |
| 20b | Present results of all statistical syntheses conducted. If meta-analysis was done, present for each the summary estimate and its precision (e.g., confidence/credible interval) and measures of statistical heterogeneity. If comparing groups, describe the direction of the effect. | N/A | |
| 20c | Present results of all investigations of possible causes of heterogeneity among study results. | N/A | |
| 20d | Present results of all sensitivity analyses conducted to assess the robustness of the synthesized results. | N/A | |
| Reporting biases | 21 | Present assessments of risk of bias due to missing results (arising from reporting biases) for each synthesis assessed. | N/A |
| Certainty of evidence | 22 | Present assessments of certainty (or confidence) in the body of evidence for each outcome assessed. | N/A |
| DISCUSSION | |||
| Discussion | 23a | Provide a general interpretation of the results in the context of other evidence. | Page 14–15 |
| 23b | Discuss any limitations of the evidence included in the review. | Page 17 | |
| 23c | Discuss any limitations of the review processes used. | Page 17 | |
| 23d | Discuss implications of the results for practice, policy, and future research. | Page 17 | |
| OTHER INFORMATION | |||
| Registration and protocol | 24a | Provide registration information for the review, including register name and registration number, or state that the review was not registered. | N/A |
| 24b | Indicate where the review protocol can be accessed, or state that a protocol was not prepared. | N/A | |
| 24c | Describe and explain any amendments to information provided at registration or in the protocol. | N/A | |
| Support | 25 | Describe sources of financial or non-financial support for the review, and the role of the funders or sponsors in the review. | Page 17 |
| Competing interests | 26 | Declare any competing interests of review authors. | Page 18 |
| Availability of data, code and other materials | 27 | Report which of the following are publicly available and where they can be found: template data collection forms; data extracted from included studies; data used for all analyses; analytic code; any other materials used in the review. | Page 18 |
Appendix B
| 1. Abhilash KP, Roshine MK, Vandana K, Varghese GM. A probable case of acquired toxoplasmosis presenting as pyrexia of unknown origin in an immunocompetent individual. Int J Infect Dis. 2013 Nov;17(11):e1067-8. doi: 10.1016/j.ijid.2013.03.024. Epub 2013 May 28. PMID: 23726282. |
| 2. Aksoy A, Tanir G, Ozkan M, Oguz M, Yildiz YT. Acute disseminated encephalomyelitis associated with acute Toxoplasma gondii Infection. Pediatr Neurol. 2013 Mar;48(3):236-9. doi: 10.1016/j.pediatrneurol.2012.11.004. PMID: 23419476. |
| 3. Akturk HK, Sotello D, Ameri A, Abuzaid AS, Rivas AM, Vashisht P. Toxoplasma Infection in an Immunocompetent Host: Possible Risk of Living with Multiple Cats. Cureus. 2017 Mar 19;9(3):e1103. doi: 10.7759/cureus.1103. PMID: 28435763; PMCID: PMC5398893. |
| 4. Alapatt JP, Kutty RK, Jose B, Gopi P. A case of cerebral toxoplasmosis in a pregnant non-immunocompromised patient. Neurol Neurochir Pol. 2009 Jul-Aug;43(4):391-5. PMID: 19742399. |
| 5. Azarpira, Negar; Torabineghad, Simin; Rad, Hanieh; Taghipour, Musa Ventriculitis: A Case of Cerebral Toxoplasmosis in Immunocompetent Child. Neurosurgery Quarterly: August 2014 - Volume 24 - Issue 3 - p 159-160 doi: 10.1097/WNQ.0b013e31828cc5e1 |
| 6. Basit KA, Nasir S, Vohra E, Shazlee MK. Toxoplasmosis in an Immunocompetent Patient. Pak J Med Sci. 2018 Nov-Dec;34(6):1579-1581. doi: 10.12669/pjms.346.15016. PMID: 30559827; PMCID: PMC6290221. |
| 7. Beltrame A, Venturini S, Crichiutti G, Meroni V, Buonfrate D, Bassetti M. Recurrent seizures during acute acquired toxoplasmosis in an immunocompetent traveller returning from Africa. Infection. 2016 Apr;44(2):259-62. doi: 10.1007/s15010-015-0821-7. Epub 2015 Jul 14. PMID: 26168861. |
| 8. Bhattarai, Kumud, Anjali Bisht, Bhawesh Thapa and Ananta Bhakta Uprety. Toxoplasma gondii Pneumonia in an Immunocompetent Host: A Case Report. JNMA: Journal of the Nepal Medical Association 59 (2021): 84 - 87. |
| 9. Bossi P, Paris L, Caumes E, Katlama C, Danis M, Bricaire F. Severe acute disseminated toxoplasmosis acquired by an immunocompetent patient in French Guiana. Scand J Infect Dis. 2002;34(4):311-4. doi: 10.1080/00365540110080124. PMID: 12064700. |
| 10. Bossi, Philippe & Caumes, Eric & Paris, Luc & Darde, Marie Laure & Bricaire, Francois. (1999). Toxoplasma gondii-Associated Guillain-Barre’ Syndrome in an Immunocompetent Patient. Journal of clinical microbiology. 36. 3724-5. 10.1128/JCM.36.12.3724-3725.1998. |
| 11. Bousquet A, Bigaillon C, Dumitrescu N, Larréché S, Godreuil C, Mestiri R, Le Caruyer N, Mérens A, Andriamanantena D. Acute myocarditis in an immunocompetent young man: Don’t forget Toxoplasma gondii. Int J Cardiol. 2016 Jul 1;214:358-9. doi: 10.1016/j.ijcard.2016.03.155. Epub 2016 Apr 1. PMID: 27085128. |
| 12. Cai X, Zhou H, Xie Y, Yu D, Wang Z, Ren H. Anti-N-methyl-D-aspartate receptor encephalitis associated with acute Toxoplasma gondii infection: A case report. Medicine (Baltimore). 2018 Feb;97(7):e9924. doi: 10.1097/MD.0000000000009924. PMID: 29443773; PMCID: PMC5839864. |
| 13. Calore EE, Minkovski R, Khoury Z, Seguro AC, Perez Calore NM, Cavaliere MJ. Skeletal muscle pathology in 2 siblings infected with Toxoplasma gondii. J Rheumatol. 2000 Jun;27(6):1556-9. PMID: 10852291. |
| 14. Candolfi E, de Blay F, Rey D, Christmann D, Treisser A, Pauli G, Kien T. A parasitologically proven case of Toxoplasma pneumonia in an immunocompetent pregnant woman. J Infect. 1993 Jan;26(1):79-81. doi: 10.1016/0163-4453(93)96968-v. PMID: 8454890. |
| 15. Chandenier J, Jarry G, Nassif D, Douadi Y, Paris L, Thulliez P, Bourges-Petit E, Raccurt C. Congestive heart failure and myocarditis after seroconversion for toxoplasmosis in two immunocompetent patients. Eur J Clin Microbiol Infect Dis. 2000 May;19(5):375-9. doi: 10.1007/s100960050498. PMID: 10898141. |
| 16. Chang HJ, Hong CT, Hu CJ, Chan L. Central nervous system toxoplasmosis in an immunocompetent individual. Kaohsiung J Med Sci. 2019 Apr;35(4):248-249. doi: 10.1002/kjm2.12036. Epub 2019 Mar 19. PMID: 30887680. |
| 17. Chiappe Gonzalez AJ, Vargas Matos I, Massucco Revoredo V. Acute toxoplasmosis complicated with myopericarditis and possible encephalitis in an immunocompetent patient. IDCases. 2020 Apr 24;20:e00772. doi: 10.1016/j.idcr.2020.e00772. PMID: 32395428; PMCID: PMC7210424. |
| 18. Cortés AD, Aguirre N. Severe disseminated acute toxoplasmosis in an adult immunocompetent patient from the Colombian Pacific. Biomedica. 2018 Aug 1;38(0):19-23. doi: 10.7705/biomedica.v38i0.4087. PMID: 30184374. |
| 19. Cortés DA, Aguilar MC, Rios HA, Rodriguez FJ, Montes KV, Gómez-Marín JE,, de-la-Torre A. Severe acute multi-systemic failure with bilateral ocular toxoplasmosis in immunocompetent patients from urban settings in Colombia: Case reports. Am J Ophthalmol Case Rep. 2020 Mar 13;18:100661. doi: 10.1016/j.ajoc.2020.100661. PMID: 32195446; PMCID: PMC7078491. |
| 20. Cottrell AJ. Acquired toxoplasma encephalitis. Arch Dis Child. 1986 Jan;61(1):84-5. doi: 10.1136/adc.61.1.84. PMID: 3954425; PMCID: PMC1777557. |
| 21. Couvreur J, Thulliez P. Toxoplasmose acquise à localisation oculaire ou neurologique: 49 cas [Acquired toxoplasmosis of ocular or neurologic site: 49 cases]. Presse Med. 1996 Mar 16;25(9):438-42. French. PMID: 8685192. |
| 22. Darde’ ML, Villena I, Pinon JM, Beguinot I. Severe toxoplasmosis caused by a Toxoplasma gondii strain with a new isoenzyme type acquired in French Guyana. J Clin Microbiol. 1998 Jan;36(1):324. doi: 10.1128/JCM.36.1.324-324.1998. PMID: 9431981; PMCID: PMC124868. |
| 23. De Salvador-Guillouet F, Ajzenberg D, Chaillou-Opitz S, Saint-Paul MC, Dunais B, Dellamonica P, Marty P. Severe pneumonia during primary infection with an atypical strain of Toxoplasma gondii in an immunocompetent young man. J Infect. 2006 Aug;53(2):e47-50. doi: 10.1016/j.jinf.2005.10.026. Epub 2005 Dec 15. PMID: 16352339. |
| 24. Demar M, Ajzenberg D, Maubon D, Djossou F, Panchoe D, Punwasi W, Valery N, Peneau C, Daigre JL, Aznar C, Cottrelle B, Terzan L, Darde’ ML, Carme B. Fatal outbreak of human toxoplasmosis along the Maroni River: epidemiological, clinical, and parasitological aspects. Clin Infect Dis. 2007 Oct 1;45(7):e88-95. doi: 10.1086/521246. Epub 2007 Aug 27. PMID: 17806043. |
| 25. Demar M, Hommel D, Djossou F, Peneau C, Boukhari R, Louvel D, Bourbigot AM, Nasser V, Ajzenberg D, Darde ML, Carme B. Acute toxoplasmoses in immunocompetent patients hospitalized in an intensive care unit in French Guiana. Clin Microbiol Infect. 2012 Jul;18(7):E221-31. doi: 10.1111/j.1469-0691.2011.03648.x. Epub 2011 Sep 29. PMID: 21958195. |
| 26. Desguerre I, Pedespan JM, Buissonnie’re, Couvreur J, Ponsot G. [Acquired cerebral toxoplasmosis in an non-immunosuppressed child]. Arch Fr Pediatr. 1993 Apr;50(4):339-42. French. PMID: 8379823. |
| 27. de Souza Giassi K, Costa AN, Apanavicius A, Teixeira FB, Fernandes CJ, Helito AS, Kairalla RA. Tomographic findings of acute pulmonary toxoplasmosis in immunocompetent patients. BMC Pulm Med. 2014 Nov 25;14:185. doi: 10.1186/1471-2466-14-185. PMID: 25420956; PMCID: PMC4254211.28. Duffield JS, Jacob AJ, Miller HC. Recurrent, life-threatening atrioventricular dissociation associated with toxoplasma myocarditis. Heart. 1996 Nov;76(5):453-4. doi: 10.1136/hrt.76.5.453. PMID: 8944597; PMCID: PMC484583. |
| 29. Filipowicz A, Coca MN, Blair BM, Chang PY. Acute myocarditis with cardiogenic shock and multiple organ failure, followed by bilateral panuveitis masquerading as endogenous endophthalmitis, due to Toxoplasma gondii in an immunocompetent patient. Retin Cases Brief Rep. 2021 Sep 1;15(5):575-580. doi: 10.1097/ICB.0000000000000855. PMID: 30664080. |
| 30. Galli-Tsinopoulou A, Kyrgios I, Giannopoulou EZ, Gourgoulia S, Maggana I, Katechaki E, Chatzidimitriou D, Evangeliou AE. Acquired toxoplasmosis accompanied by facial nerve palsy in an immunocompetent 5-year-old child. J Child Neurol. 2010 Dec;25(12):1525-8. doi: 10.1177/0883073810370480. PMID: 21148450. |
| 31. Groh M, Faussart A, Villena I, Ajzenberg D, Carme B, Demar M, Joly V, Houze S, Simon S, Aubert D, Charlois-Ou C, Yeni P. Acute lung, heart, liver, and pancreatic involvements with hyponatremia and retinochoroiditis in a 33-year-old French Guianan patient. PLoS Negl Trop Dis. 2012;6(10):e1802. doi: 10.1371/journal.pntd.0001802. Epub 2012 Oct 25. PMID: 23145185; PMCID: PMC3493371. |
| 32. Gupta A, Raja A, Mahadevan A, Shankar SK. Toxoplasma granuloma of brainstem: a rare case. Neurol India. 2008 Apr-Jun;56(2):189-91. PMID: 18688147. |
| 33. Guerot E, Assayag P, Morgant C, Hess M, Valère PE. Manifestations pericardiques de la toxoplasmose [Pericardial manifestations of toxoplasmosis]. Arch Mal Coeur Vaiss. 1992 Jan;85(1):109-11. French. PMID: 1550430. |
| 34. Habek M, Ozretić D, Zarković K, Djaković V, Mubrin Z. Unusual cause of dementia in an immunocompetent host: toxoplasmic encephalitis. Neurol Sci. 2009 Feb;30(1):45-9. doi: 10.1007/s10072-008-0007-5. Epub 2009 Jan 16. PMID: 19148571. |
| 35. Harbada RK, Sorabjee JS, Surya N, Jadhav KA, Mirgh S. Cerebellar Toxoplasmosis in an Immunocompetent Patient with G6PD Deficiency. J Assoc Physicians India. 2016 Aug;64(8):79-82. PMID: 27762116. |
| 36. Henao-Martinez AF, Franco-Paredes C, Palestine AG, Mon-toya JG. Symptomatic acute toxoplasmosis in returning travelers. Open Forum Infect Dis 2018;5:ofy058. |
| 37. Hoti YU, Aziz A, Ishaque K, Abbas S, Ud Din TS. Intra-cranial Toxoplasmosis in an Immunocompetent Female. J Coll Physicians Surg Pak. 2016 Jun;26(6 Suppl):S39-41. PMID: 27376217. |
| 38. IñíguezC, Jericó I, Pascual LF, Cuesta J, Morales F. Síndrome de Miller-Fisher asociado a infección por toxoplasma [Miller-Fisher syndrome associated with toxoplasmosis]. Neurologia. 1997 Apr;12(4):172-4. Spanish. PMID: 9235026. |
| 39. Jimenez-Caballero PE, Serviá M, Marsal-Alonso C. Encefalomielitis aguda diseminada por toxoplasmosis en un paciente de edad avanzada [Acute disseminated encephalomyelitis due to toxoplasmosis in an elderly patient]. Rev Neurol. 2010 Apr 1;50(7):445-7. Spanish. PMID: 20387217. |
| 40. Kanno A, Suzuki Y, Minami M, Ogawa K, Oishi M, Kamei S. A healthy, 81-year-old woman with toxoplasmic encephalitis. Geriatr Gerontol Int. 2012 Oct;12(4):759-61. doi: 10.1111/j.1447-0594.2012.00863.x. PMID: 22998383. |
| 41. Kaushik RM, Mahajan SK, Sharma A, Kaushik R, Kukreti R. Toxoplasmic meningoencephalitis in an immunocompetent host. Trans R Soc Trop Med Hyg. 2005 Nov;99(11):874-8. doi: 10.1016/j.trstmh.2005.06.017. PMID: 16111730. |
| 42. Leal FE, Cavazzana CL, de Andrade HF Jr, Galisteo A Jr, de Mendonça JS, Kallas EG. Toxoplasma gondii pneumonia in immunocompetent subjects: case report and review. Clin Infect Dis. 2007 Mar 15;44(6):e62-6. doi: 10.1086/511871. Epub 2007 Feb 8. PMID: 17304443. |
| 43. Leroy J, Houzé S, Dardé ML, Yéra H, Rossi B, Delhaes L, Gabriel F, Loubet P, Deleplancque AS, Senneville E, Ajana F, Sendid B, Malvy D. Severe toxoplasmosis imported from tropical Africa in immunocompetent patients: A case series. Travel Med Infect Dis. 2020 May-Jun;35:101509. doi: 10.1016/j.tmaid.2019.101509. Epub 2019 Nov 9. PMID: 31712179. |
| 44. Lescop J, Brinquin L, Schill H, Soulié D, Sarrazin JL, Cordoliani YS. Encéphalite toxoplasmique diffuse chez un sujet non immunodéprimé [Diffuse toxoplasmic encephalitis in a non-immunosuppressed patient]. J Radiol. 1995 Jan;76(1):21-4. French. PMID: 7861364. |
| 45. Lesenne M, Asseman P, Fortier B, de Groote P, Bauchart JJ, Millaire A, Haftel Y, Thery C. Myocardite aiguë à toxoplasme simulant un infarctus. A propos d’un cas [Acute myocarditis caused by toxoplasmosis simulating infarction. Apropos of a case] Arch Mal Coeur Vaiss. 1996 Jul;89(7):923-5. French. PMID: 8869256. |
| 46. Li ZH, Guo FY, Wang ZQ, Cui J. Intracranial inflammatory granuloma caused by toxoplasmosis. Pathog Glob Health. 2014 Jul;108(5):255-9. doi: 10.1179/2047773214Y.0000000147. PMID: 25175876; PMCID: PMC4153827. |
| 47. Lima KDF, Queiroz ALG, Teixeira HS, Bonsi VM, Inada BSY, Lancellotti CLP, Ba êta AM. An atypical case of neurotoxoplasmosis in immunocompetent patient. Radiol Case Rep. 2021 May 1;16(7):1766-1769. doi: 10.1016/j.radcr.2021.04.013. PMID: 34007399; PMCID: PMC8111245. |
| 48. Luis Eduardo Pino, Jorge Enrique Salinas, Myriam Consuelo López, Descripcion de un brote epidemico de toxoplasmosis aguda en pacientes inmunocompetentes miembros de las fuerzas militares de Colombia durante operaciones de selva, Infectio, Volume 13, Issue 2, 2009, Pages 83-91, ISSN 0123-9392, https://doi.org/10.1016/S0123-9392(09)70729-5. |
| 49. Lyngberg KK, Vennervald BJ, Bygbjerg IC, Hansen TM, Thomsen OO: Toxoplasma pericarditis mimicking systemic lupus erythrematous: Diagnostic and treatment difficulties in one patient. Ann Med 1992; 24: 337-340 |
| 50. Lévêque MF, Chiffré D, Galtier C, Albaba S, Ravel C, Lachaud L, Iemmi A, Flori P, Sterkers Y. Molecular diagnosis of toxoplasmosis at the onset of symptomatic primary infection: A straightforward alternative to serological examinations. Int J Infect Dis. 2019 Feb;79:131-133. doi: 10.1016/j.ijid.2018.11.368. Epub 2018 Dec 4. PMID: 30529368. |
| 51. Manwani N, Ravikumar K, Viswanathan V, Rao SM, Mahadevan A. Acquired Toxoplasmosis Presenting with a Brainstem Granuloma in an Immunocompetent Adolescent. Indian Pediatr. 2016 Feb;53(2):159-61. doi: 10.1007/s13312-016-0813-4. PMID: 26897153. |
| 52. Mariani M, Pagani M, Inserra C, De Servi S. Complete atrioventricular block associated with toxoplasma myocarditis. Europace. 2006 Mar;8(3):221-3. doi: 10.1093/europace/euj046. Epub 2006 Feb 13. PMID: 16627444. |
| 53. Martinot M, Greigert V, Farnarier C, Darde ML, Piperoglou C, Mohseni-Zadeh M, Tarabeux J, Guffroy A, Villard O, Vely F. Spinal cord toxoplasmosis in a young immunocompetent patient. Infection. 2020 Apr;48(2):299-302. doi: 10.1007/s15010-019-01380-9. Epub 2019 Dec 9. PMID: 31820319. |
| 54. McCabe, Remington Rev Infect Dis 1987 (Ref 20) Clinical Spectrum of 107 cases of toxoplasmic lymphadenopathy |
| 55. Michel O. Thorax 1986 (ref 18) Acute pulmonary toxoplasmosis with alveolitis of T suppressor lymphocyte type (dci got pdf) |
| 56. Micheli R, Perini A, Duse M. Hemidystonia secondary to acquired toxoplasmosis in a non-immunodeficient patient. Eur J Pediatr. 1994 Oct;153(10):731-3. doi: 10.1007/BF01954489. PMID: 7813530. |
| 57. Montoya JG, Jordan R, Lingamneni S, Berry GJ, Remington JS. Toxoplasmic myocarditis and polymyositis in patients with acute acquired toxoplasmosis diagnosed during life. Clin Infect Dis. 1997 Apr;24(4):676-83. doi: 10.1093/clind/24.4.676. PMID: 9145743. |
| 58. Mustafa K, Hillyard J, Nowak E, Slowikowski J, Okogbue I, Garner D. Toxoplasma myocarditis: An atypical case in an immunocompetent patient. IDCases. 2021 Sep 8;26:e01273. doi: 10.1016/j.idcr.2021.e01273. PMID: 34584844; PMCID: PMC8450265. |
| 59. Nelwan EJ, Shakinah S, Clarissa G, Hosea FN, Herdanto DY, Pandelaki J. Rare cardiac complication of toxoplasmosis in immunocompetent host. IDCases. 2022 Jun 15;29:e01533. doi: 10.1016/j.idcr.2022.e01533. PMID: 35756700; PMCID: PMC9218370. |
| 60. Neves Ede S, Kropf A, Bueno WF, Bonna IC, Curi AL, Amendoeira MR, Fernandes Filho O. Disseminated toxoplasmosis: an atypical presentation in an immunocompetent patient. Trop Doct. 2011 Jan;41(1):59-60. doi: 10.1258/td.2010.100228. Epub 2010 Nov 9. PMID: 21062937. |
| 61. Nunura J, Va’squez T, Endo S, Salazar D, Rodriguez A, Pereyra S, Solis H. Disseminated toxoplasmosis in an immunocompetent patient from Peruvian Amazon. Rev Inst Med Trop Sao Paulo. 2010 Mar-Apr;52(2):107-10. doi: 10.1590/s0036-46652010000200008. PMID: 20464132. |
| 62. Oseroff A. Toxoplasmosis associated with nephrotic syndrome in an adult. South Med J. 1988 Jan;81(1):95-6. doi: 10.1097/00007611-198801000-00022. PMID: 3336807. |
| 63. Paruthikunnan S, Shankar B, Kadavigere R, Prabhu M, Narayanan R, Jain H. An unusual case of disseminated toxoplasmosis in a previously healthy pregnant patient: radiographic, CT, and MRI findings. Jpn J Radiol. 2014 Nov;32(11):664-9. doi: 10.1007/s11604-014-0352-7. Epub 2014 Aug 24. PMID: 25151528. |
| 64. Paspalaki PK, Mihailidou EP, Bitsori M, Tsagkaraki D, Mantzouranis E. Polyomyositis and myocarditis associated with acquired toxoplasmosis in an immunocompetent girl. BMC Musculoskelet Disord 2001;2:8. |
| 65. Pena HFJ, Ferreira MN, Gennari SM, de Andrade HF Jr, Meireles LR, Galisteo AJ Jr. Toxoplasma gondii isolated from a Brazilian patient with rare pulmonary toxoplasmosis has a novel genotype and is closely related to Amazonian isolates. Parasitol Res. 2021 Mar;120(3):1109-1113. doi: 10.1007/s00436-020-07008-4. Epub 2021 Jan 9. PMID: 33420622. |
| 66. Pustorino G, Ferlazzo E, Carpentieri MS, Cianci V, Gasparini S, Campello M, Milardi GL, Gangemi A, Aguglia U. Cerebral toxoplasmosis diagnosed by brain tissue PCR analysis in an immunocompetent patient. Neurol Clin Pract. 2017 Oct;7(5):436-438. doi: 10.1212/CPJ.0000000000000364. PMID: 29620083; PMCID: PMC5874466. |
| 67. Rafiqul Islam et al.Toxoplasmosis Presenting As P.U.O.- A Case ReportBang. Med. J. 1989; 18 (1), 30-32; file:///C:/Users/dcontop/Downloads/ToxoplasmosisPresentingAsPUO-ACaseReport-1.p |
| 68. Ramachandran R, Radhan P, Anand R, Subramanian I, Santosham R, Sai V. CNS toxoplasmosis in an immunocompetent individual. Radiol Case Rep. 2015 Dec 7;9(1):e00031. doi: 10.2484/rcr.v9i1.908. PMID: 27141248; PMCID: PMC4838758. |
| 69. Roubille F, Roubille C, Lattuca B, Gervasoni R, Vernhet-Kovacsik H, Leclercq F. Recent Toxoplasmosis Infection With Acute Myopericarditis and Persistent Troponin Elevation in an Immunocompetent Patient. Cardiol Res. 2012 Aug;3(4):189-191. doi: 10.4021/cr200w. Epub 2012 Jul 20. PMID: 28348686; PMCID: PMC5358212. |
| 70. Rösch D, Handrick W, Lietz R, Blatz R, König E. Erworbene Toxoplasmose mit zerebraler Beteiligung und nachfolgender Hörstörung [Acquired toxoplasmosis with cerebral involvement and subsequent hearing loss]. Klin Padiatr. 1998 May-Jun;210(3):125-7. German. doi: 10.1055/s-2008-1043863. PMID: 9629546.71. Rostoff, P.; Mroczek-Czernecka, D.; Piwowarska, W.; Gackowski, A.; Konduracka, E.; Trzos, M.; Pasowicz, M. Elevated CA-125 level in acute heart failure due to Toxoplasma gondii perimyocarditis. Int. J. Cardiol. 2008, 130, e114–e116. |
| 72. Sano J, Saitoh H, Kobayashi Y, Ikeda M, Kodani E, Takayama M, Kishida H, Takano T, Yano A. [Toxoplasma pericarditis without immunosuppressant disorder detected by polymerase chain reaction of pericardial fluid: a case report]. J Cardiol. 2000 Jan;35(1):47-54. Japanese. PMID: 10654250. |
| 73. Shimoni Z, Reichman N, Raz R, Flatau E. Pulmonary infiltrate in acute toxoplasmosis. Isr J Med Sci. 1989 Jan;25(1):46-7. PMID: 2925360. |
| 74. Silva LA, Vieira RS, Serafini LN, Carlotti CG Jr, Figueiredo JF. Toxoplasmose do sistema nervoso central em paciente sem evideªncia de imunossupressao: relato de caso [Toxoplasmosis of the central nervous system in a patient without immunosupression: case report]. Rev Soc Bras Med Trop. 2001 Sep-Oct;34(5):487-90. Portuguese. doi: 10.1590/s0037-86822001000500014. PMID: 11600917. |
| 75. Simanaityte D, Le Gouellec N, Ajana F, Baclet N, Poissy J, Laiskonis A, Mickiene A, Senneville E, Yazdanpanah Y, Legout L. Primo-infection toxoplasmique avec atteinte pulmonaire chez un immunocompétent [Primary pulmonary toxoplasmosis in an immunocompetent patient]. Med Mal Infect. 2010 Dec;40(12):713-5. French. doi: 10.1016/j.medmal.2010.03.013. Epub 2010 Apr 21. PMID: 20413237. |
| 76. Singhal KK, Kumar K, Mathew JL, Mewara A, Vaidya PC, Sodhi KS, Singh M. Active toxoplasmosis presenting with polymyositis and pleural effusion in a child. J Paediatr Child Health. 2021 Dec;57(12):1995-1997. doi: 10.1111/jpc.15390. Epub 2021 Feb 11. PMID: 33571377. |
| 77. Sobanski V, Ajzenberg D, Delhaes L, Bautin N, Just N. Severe toxoplasmosis in immunocompetent hosts: be aware of atypical strains. Am J Respir Crit Care Med. 2013 May 15;187(10):1143-5. doi: 10.1164/rccm.201209-1635LE. PMID: 23675724. |
| 78. Sugane K, Takamoto M, Nakayama K, Tada T, Yuasa T, Kurokawa K. Diagnosis of Toxoplasma meningoencephalitis in a non-AIDS patient using PCR. J Infect. 2001 Feb;42(2):159-60. doi: 10.1053/jinf.2000.0768. PMID: 11531325. |
| 79. Sánchez T, Soriano MJ, Almarza JL, CámaraM, Paricio P. Diagnóstico de toxoplasmosis cerebral en un paciente inmunocompetente [Diagnosis of cerebral toxoplasmosis in an immunocompetent patient]. Enferm Infecc Microbiol Clin. 2000 Jan;18(1):46-8. Spanish. PMID: 10721565. |
| 80. Undseth O, Gerlyng P, Goplen AK, Holter ES, von der Lippe E, Dunlop O. Primary toxoplasmosis with critical illness and multi-organ failure in an immunocompetent young man. Scand J Infect Dis. 2014 Jan;46(1):58-62. doi: 10.3109/00365548.2013.813065. Epub 2013 Aug 1. PMID: 23902584. |
| 81. Vastava PB, Pradhan S, Jha S, Prasad KN, Kumar S, Gupta RK. MRI features of toxoplasma encephalitis in the immunocompetent host: a report of two cases. Neuroradiology. 2002 Oct;44(10):834-8. doi: 10.1007/s00234-002-0852-5. Epub 2002 Aug 24. PMID: 12389133. |
| 82. Yang Y, Zuo W, Hu J, Esch GW, Zuo Y. Hemophagocytic syndrome as uncommon presentation of disseminated toxoplasmosis in an immunocompetent adult from Chinese Kunming. Am J Trop Med Hyg. 2013 Jun;88(6):1209-11. doi: 10.4269/ajtmh.12-0556. Epub 2013 Mar 18. PMID: 23509123; PMCID: PMC3752825. |
Appendix C
| Authors’ Countries | N | Percent |
|---|---|---|
| Bangladesh | 1 | 0.9 |
| Belgium | 1 | 0.9 |
| Brazil | 8 | 6.8 |
| China | 3 | 2.6 |
| Colombia | 12 | 10.3 |
| Croatia | 1 | 0.9 |
| Denmark | 1 | 0.9 |
| France | 30 | 25.6 |
| French Guiana | 13 | 11.1 |
| Germany | 1 | 0.9 |
| Greece | 2 | 1.7 |
| India | 10 | 8.6 |
| Indonesia | 1 | 0.9 |
| Iran | 1 | 0.9 |
| Israel | 1 | 0.9 |
| Italy | 5 | 4.3 |
| Japan | 3 | 2.6 |
| Nepal | 1 | 0.9 |
| Norway | 1 | 0.9 |
| Oman | 1 | 0.9 |
| Pakistan | 2 | 1.7 |
| Peru | 2 | 1.7 |
| Poland | 1 | 0.9 |
| Spain | 3 | 2.6 |
| Taiwan | 1 | 0.9 |
| Turkey | 1 | 0.9 |
| UK | 2 | 1.7 |
| USA | 8 | 6.8 |
| Total | 117 | 100 |
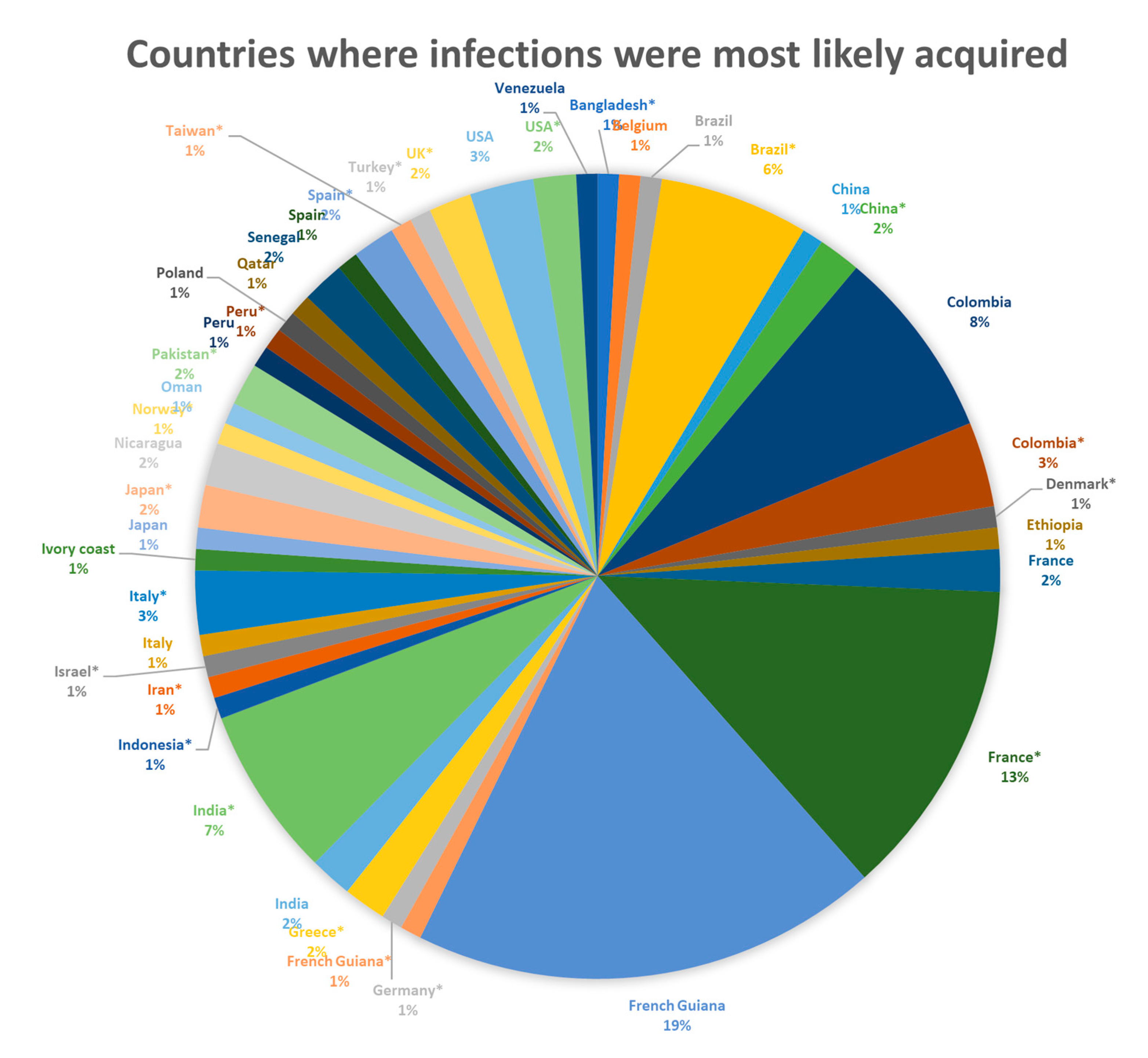
| Countries of Infections (Imputed Countries for Those Not Reported Shown with *) | N | Percent |
|---|---|---|
| Bangladesh * | 1 | 0.85 |
| Belgium | 1 | 0.85 |
| Brazil | 1 | 0.85 |
| Brazil * | 7 | 5.98 |
| China | 1 | 0.85 |
| China * | 2 | 1.71 |
| Colombia Colombia * | 8 4 | 6.80 3.42 |
| Croatia | 1 | 0.85 |
| Denmark * | 1 | 0.85 |
| Ethiopia | 1 | 0.85 |
| France | 2 | 1.71 |
| France * | 15 | 12.82 |
| French Guiana | 22 | 18.80 |
| French Guiana * | 1 | 0.85 |
| Germany * | 1 | 0.85 |
| Greece* | 2 | 1.71 |
| India | 2 | 1.71 |
| India * | 8 | 6.84 |
| Indonesia * | 1 | 0.85 |
| Iran * | 1 | 0.85 |
| Israel * | 1 | 0.85 |
| Italy | 1 | 0.85 |
| Italy * | 3 | 2.56 |
| Ivory coast | 1 | 0.85 |
| Japan | 1 | 0.85 |
| Japan * | 2 | 1.71 |
| Nicaragua | 2 | 1.71 |
| Norway * | 1 | 0.85 |
| Oman | 1 | 0.85 |
| Pakistan * | 2 | 1.71 |
| Peru | 1 | 0.85 |
| Peru * | 1 | 0.85 |
| Poland | 1 | 0.85 |
| Qatar | 1 | 0.85 |
| Senegal | 2 | 1.71 |
| Spain | 1 | 0.85 |
| Spain * | 2 | 1.71 |
| Taiwan * | 1 | 0.85 |
| Turkey * | 1 | 0.85 |
| UK * | 2 | 1.71 |
| USA | 3 | 2.56 |
| USA * | 2 | 1.71 |
| Venezuela | 1 | 0.85 |
| Total | 117 | 100.00 |
| Reported genotyping | 23/117 (20%) | |
| Atypical more virulent strain non-type II strains | 22/23 (96%) | No type II virulent strain, African I strain, Africa or recombinant I/III Argentinian strain, Atypical strain GUY-2004-ABE, GUY-204-ANG, GUY-2004-TER, New and unknown zymodeme 12 highly virulent, identical with reference strain AF146527, virulent ROP18 allele, Zymodeme 6 virulent strain |
| Type II strain | 1/23 (4%) | |
| Reported that no genotyping was done | 15/117 (13%) | |
| Not reported genotyping information | 79/117 (68%) |
| Toxoplasmosis Lung Imaging Findings | N |
|---|---|
| 31 1 |
| 1 |
| 1 |
| 1 |
| 1 |
| 1 |
| 1 |
| 1 |
| 1 |
| 1 |
| 1 |
| 1 |
| 1 |
| 1 |
| 1 |
| 1 |
| 1 |
| 1 |
| 1 |
| 1 |
| 1 |
| 1 |
| 1 |
| 1 |
| 1 |
| 1 |
| 1 |
| 1 |
| 1 |
| 1 |
| 1 |
| 1 |
| 1 |
| 1 |
| 1 |
| 1 |
| 1 |
| 1 |
| 1 |
| 1 |
| 1 |
| 1 |
| 15 |
| 64 |
| Total | 117 |
| CNS Imaging Findings | N |
|---|---|
CNS toxoplasmosis cases
| 41 1 |
| 1 |
| 1 |
| 1 |
| 1 |
| 1 |
| 1 |
| 1 |
| 1 |
| 1 |
| 1 |
| 1 |
| 1 |
| 1 |
| 1 |
| 1 |
| 1 |
| 1 |
| 1 |
| 1 |
| 1 |
| 1 |
| 1 |
| 1 |
| 1 |
| 1 |
| 1 |
| 1 |
| 1 |
| 1 |
| 1 |
| 1 |
| 1 |
| 1 |
| 1 |
| 1 |
| 1 |
| 1 |
| 1 |
| 1 |
| 1 |
| 1 |
| 18 |
| 58 |
| Total | 117 |
| Cardiac Cases (ECHO, Cardiac MRI, EKG) | N |
|---|---|
Cardiac toxoplasmosis
| 34 1 |
| 1 |
| 1 |
| 1 |
| 1 |
| 1 |
| 1 |
| 1 |
| 1 |
| 1 |
| 1 |
| 2 |
| 1 |
| 1 |
| 1 |
| 1 |
| 1 |
| 1 |
| 1 |
| 1 |
| 1 |
| 1 |
| 1 |
| 1 |
| 1 |
| 1 |
| 1 |
| 1 |
| 1 |
| 3 |
| 1 |
| 1 |
| 1 |
| 1 |
| 7 |
| 76 |
| Total | 117 |
| Treatments | N | Percent |
|---|---|---|
| Azithromycin | 2 | 1.71 |
| Azithromycin + Clindamycin | 1 | 0.85 |
| Clindamycin | 1 | 0.85 |
| Erythromycin and then Pyrimethamine + Sulfadiazine | 1 | 0.85 |
| Erythromycin initially, then after diagnosis Pyrimethamine + Sulfadiazine, initially, then spiramycin | 1 | 0.85 |
| Fansidar + Spiramycin (initially), then Pyrimethamine + Sulfadiazine, then fansidar maintenance | 1 | 0.85 |
| No anti-Toxoplasma treatment | 14 | 11.97 |
| Not reported | 5 | 4.27 |
| Not reported (TMP/SMX given later for the ocular findings (intravitreal clindamycin + dexamethasone (DXM])) | 2 | 1.71 |
| Pyrimethamin + Sulfadiazine +DXM (initially), then Pyrimethamine + Clindamycin | 1 | 0.85 |
| Pyrimethamine + Clindamycin | 3 | 2.56 |
| Pyrimethamine + Spiramycin | 1 | 0.85 |
| Pyrimethamine + clindamycin | 1 | 0.85 |
| Pyrimethamine +Sulfadiazine + Spiramycin | 1 | 0.85 |
| Pyrimethamine + Sulfadiazine | 52 | 44.44 |
| Pyrimethamine + Sulfadiazine + clindamycin | 1 | 0.85 |
| Pyrimethamine + Sulfadiazine + Spiramycin | 1 | 0.85 |
| Spiramycin | 4 | 3.42 |
| Spiramycin (initially) and then Pyrimethamine + Sulfadiazine | 1 | 0.85 |
| Spiramycin (initially), and then Pyrimethamine + Sulfadiazine | 1 | 0.85 |
| Spiramycin (initially), then Pyrimethamine + Sulfadiazine | 1 | 0.85 |
| TMP/SMX | 11 | 9.40 |
| TMP/SMX (initially) and then Pyrimethamine | 1 | 0.85 |
| TMP/SMX (initially), then Azithromycin + Clindamycin | 1 | 0.85 |
| TMP/SMX (initially), then Pyrimethamine + Sulfadiazine | 1 | 0.85 |
| TMP/SMX (initially), then Pyrimethamine + Sulfadiazine | 1 | 0.85 |
| TMP/SMX (initially), then clindamycin | 1 | 0.85 |
| Unspecified treatment | 1 | 0.85 |
| Unspecified anti-Toxoplasma treatment | 4 | 3.42 |
| Total | 117 | 100.00 |
| Author | Vignettes of Severe Toxoplasmosis Cases |
|---|---|
| Nelwan 2022 | Acute toxoplasmic myocarditis in a 28-yr-old male who presented w fever x8 wks and chest pain x1 wk PTA; cardiac MRI showing Late Gadolinium Enhancement (LGE) areas consistent with myocardial necrosis but w normal LV systolic function; elevated cardiac enzymes (hs-Troponin, CK-MB and proBNP), transaminitis, lymphopenia, hyponatremia//Patient responded initially to steroid treatment but relapsed again within 2 wks from the first hospital admission//This led to the diagnosis of Acute Toxoplasmosis (Acute Primary Infection) and initiation of anti- Toxoplasma treatment with Pyrimethamine + Clindamycin x 8 weeks//clinically improved after 4 wks of anti- Toxoplasma treatment, also w normalization of laboratory values// |
| Bhattarai 2021 | B/L interstitial pneumonia w respiratory distress in a 35-yr-old male with associated LADP and transaminitis (w fever, cough, respiratory distress, hypoxia requiring ICU admission; w subsequently development of b/l inguinal not tender LADP, hepatomegaly and lab values indicating transaminitis; hyperbilirubinemia//W Chest imaging findings suggestive of atypical pneumonia w CXR w b/l pulmonary infiltrates and Chest CT indicating b/l GGO with minimal b/l pleural effusions//With clinical and radiographic response to anti-Toxoplasma treatment (radiographic resolution of CXR findings at 4 wks f/up) |
| Filipowics 2021 | Cardiogenic shock 2/2 acute myocarditis w multiple organ failure in a 59-yr-old female, with need for ICU admission, w CHF with ECHO showing global hypokinesia w EF 45% initially dropping to 10% by HD2; w cardiac index 1.0 in cardiac catheterization; w elevated cardiac biomarkers, transaminitis, and leukocytosis//Initially managed w steroids for presumed infectious myocarditis w CHF//Cardiogenic shock with multiorgan failure and ICU admission, ECHO with global hypokinesia (EF 10%), elevated cardiac enzymes. The toxoplasmosis diagnosis was made >1 mo after onset of cardiac symptoms, when he developed ocular inflammation; at which time cardiac findings had resolved without specific anti-Toxoplasma treatment//Diagnosed with Toxoplasmosis based on acute serology at the time of ocular inflammation evaluation, despite prior negative myocardial biopsy histopathology for Toxoplasma and negative aqueous and vitreous fluid Toxoplasma PCR//Started anti- Toxoplasma treatment and steroids at the time of ocular inflammation presentation with resolution of chorioretinitis//Treated with TMP/SMX for 6 weeks and got daily suppressive treatment for 1 year) (Additional info: Underwent Myocardial biopsy. Diagnosed as viral myocarditis. //CSF evaluation due to initially associated altered mental status showed high protein (CSF protein 61)//D/C home after 1 mo of first hospitalization with several nosocomial infections//DOI 1 mo: developed floaters, decreased visual acuity and severe vitritis and b/l endophthalmitis. Failed antifungal treatment. Improved with vitrectomy in Left eye. Vitreous aspirate Toxoplasma PCR negative. //Toxoplasma serology suggestive of API with positive Toxoplasma IgG/IgM and avidity testing//Review of previous myocardial biopsy was negative for Toxoplasma cysts//Aqueous humor fluid was Toxoplasma PCR negative//Had vitrectomy also in R eye with improved vision, BUT after surgery developed chorioretinitis in Left eye consistent with ocular toxoplasmosis. //Started anti- Toxoplasma treatment and steroids with resolution of chorioretinitis//treated with TMP/SMX for 6 weeks and got daily suppressive treatment for 1 year)/////(also nosocomial pseudomonas pneumonia, clostridium difficile colitis, AKI requiring hemodialysis)//Required prolonged hospitalization x 1 mo (w several nosocomial infections) and was d/c in a long term care facility; where he developed decreased visual acuity and floaters b/l 2 mo after onset of cardiac symptoms w new onset of b/l panuveitis/chorioritenitis; at which time the diagnosis of Toxoplasmosis was made based on positive Toxoplasma serology for API (with elevated Toxoplasma IgG and IgM titers; avidity was done but results not given)/////The study did NOT clearly report when the cardiac symptoms had resolved; but probably the cardiogenic shock had resolved before the initiation of anti- Toxoplasma treatment //(Despite negative reexamination of prior cardiac Bx, NOT showing T.gondii cysts and despite negative aqueous and vitreous fluid T.gondii PCR)//with complete resolution of chorioretinitis within 1 wk of anti-Toxoplasma treatment with TMP/SMX+ Steroids, w no recurrence of ocular or systemic symptoms |
| Lima 2021 | Encephalitis with Right hemiparesis (but without altered level of consciousness) in a 60-yr-old male presenting with a 2 ds hx of HA and R sided weakness (R hemiparesis); with CSF mild pleocytosis (CSF WBC 15 cells/mm3), predominantly lymphomononuclear and brain MRI showing a peripheral enhancing lesion with central diffusion restriction and perivascular enhancing lesion with restricted diffusion with vasogenic edema and leptomeningeal enhancement in the white matter//w brain biopsy, revealing diffuse encephalitis with necrotic brain parenchyma and predominantly acute inflammation, AND T.gondii cysts with bradyzoites seen in the brain parenchyma//Anti- Toxoplasma treatment initiated with P/S x 6 weeks with complete clinical improvement of neurologic symptoms and MRI findings with regression of the brain lesion with no pathologic contrast enhancement |
| Mustafa 2021 | Acute myocarditis with heart failure in a 2-yr-old male, presenting with recurrent acute chest pain over 1 week period (w the first 2 episodes having self-resolved), w EKG with subtle lateral ST segment elevation//with elevation of cardiac enzymes (peak troponin 12.8 ng/mL; unl < 0.3), mild transaminitis (AST 108 and ALT 91)//with Cardiac MRI: consistent with an acute phase of biventricular myocarditis and heart failure (LVEF 45% and RVEF 41%) (despite normal ECHO), with associated edema and late gadolinium enhancement (LGE) //with elevated Troponin: 8.51 ng/mL with peak of 12.8//With resolution of cardiac symptoms after 18 ds of anti- Toxoplasma treatment with Pyrimethamine + Sulfadiazine |
| Sinhal 2021 | Polymyositis and b/l pleural effusion; in a 12-yr-old-male, who presented w fever, cough, HA, malaise and weight loss x 4 months PTA, with B/L pleural effusion on lung exam; who was initially diagnosed with extrapulmonary TB//with pleural fluid showing 6427 cells/mm3 with monocytic predominance (69%)//w subsequent development of swelling over left lower chest and lower back; with peripheral eosinophilia //with contrast chest CT showing b/l pleural effusion and heterogeneous left posterior muscle and paraspinal edema//With a diagnosis of acute Toxoplasma infection affecting the muscles and lungs made based on elevated Toxoplasma IgM antibodies on two occasions, two-fold rise in Toxoplasma IgG antibodies//Child clinically responded to anti- Toxoplasma treatment (given x 7 weeks)//At 3 wks f/up there was resolution of fever, weight gain and resolution of left lower chest swelling and at 7 wks f/up there was resolution of pleural effusions and normalization of eosinophilia |
| Chiappe Gonzalez 2020 | Toxoplasmic myopericarditis and possible encephalitis, in a 34-yr-old male who presented w 7 ds Hx of progressive HA, photophobia, fever, weakness, myalgias, arthralgias, maculopapular rash, generalized LADP, hepatomegaly//with normal Brain MRI and CSF examination//w elevated troponin and CK-MB, transaminitis, ESR and beta 2 microglobulin//w cardiac MRI confirming asymptomatic myocarditis with subpericardial LGE and mild pericardial effusion with normal ventricular function//With positive Toxoplasma IgG and Toxoplasma IgM (and increasing Toxoplasma IgM in the f/up)//with positive Toxoplasma PCR from the LN biopsy//w clinical, Laboratory and cardiac MRI improvement in response to anti-Toxoplasma treatment (TMP/SMX x 4 weeks initially and then Azithromycin + Clindamcyin X another 2 wks due to TMP/SMX induced neutropenia)//With no relapse of symptoms after >12 mo of f/up |
| Cortes 2020 | Multiorgan failure, with pneumonia/Respiratory failure requiring ICU admission (also myopericarditis, nephritis, FUO, ocular toxoplasmosis, splenomegaly and LADP); in a 44 Y M from Colombia without travel to Amazonian regions, who required prolonged hospitalizations x 32 ds //who presented w FUO, profuse sweating, HA, generalized malaise; weight loss, diarrhea////W persistence of systemic symptoms but w resolution of respiratory failure and without any need for IMV at that point-after the first 10 ds, even PRIOR to initiation of anti- Toxoplasma treatment ///who had complete improvement of systemic condition only after initiation of anti- Toxoplasma treatment with TMP/SMX///W identification of positive Toxoplasma IgG and IgM after the development of ocular findings; and also positive Toxoplasma PCR from the vitreous fluid |
| Cortes 2020 | Pneumonia with respiratory failure requiring ICU admission (also myopathy, ocular Toxoplasmosis, LADP mediastinal and intraabdominal);in a 67-yr-old male from Bogota without previous travel to Amazonian regions////in whom the diagnosis of Toxoplasmosis was made after the development of ocular findings 2 months after initial presentation of respiratory failure (apparently with resolution of respiratory failure prior to initiation of anti- Toxoplasma treatment)//Details for the response to anti- Toxoplasma treatment with TMP/SMX were not provided (except for the response of the ocular findings but not the systemic findings)//The ocular findings (decreased of visual acuity) led to the Toxoplasma diagnosis; with positive Toxoplasma PCR in vitreous fluid ///Serotyping of T.gondii identified an non Type II stain |
| Leroy 2020 | Pneumonia and pleural effusion//in a 23-yr-old immunocompetent male (HIV negative) of French nationality who had recently visited Ivory Coast and had Hx of eating Raw meat, who presented with fever and malaise, LADP, hepatosplenomegaly, myalgias, chest pain and developed pneumonia with dyspnea; with elevated inflammatory markers, mild transaminitis, high CPK//with Chest/Abdomen CT showing micronodular infiltrates in both lungs, multiple LN mesenteric and retroperitoneal//w PET scan showing diffuse pulmonary infiltrates intensely metabolic; hypermetabolic splenomegaly and LADP//With Serologic diagnosis of Toxoplasmosis 13 ds after onset of symptoms //with seroconversion from initially negative Toxoplasma IgG and IgM to positive Toxoplasma IgG and IgM, and Low avidity; and positive also Toxoplasma PCR in blood/BAL and bone marrow//T.gondii genotype Africa 1//Patient treated with P/S x 6 wks and had complete clinical cure without sequelae |
| Leroy 2020 | Post Infectious Acute Cerebellar ataxia (Static cerebellar syndrome), Rhombencephalitis (CN IV, VI & IX)//in a 34-yr-old immunocompetent male (HIV negative) of Lebanese nationality; who had recently visited Senegal, w H x of eating raw meat and unwashed fruits and vegetables//who presented with fever, malaise, diplopia, headaches, motor deficits and static cerebellar syndrome/ Rhombencephalitis (CN IV, VI &IX), myalgias//w transaminitis and mild CPK elevation//Normal Brain MRI// diagnosed with Toxoplasmosis within 10 ds from onset of symptoms //with seroconversion from negative Toxoplasma IgG to positive Toxoplasma IgG, Toxoplasma IgM and low avidity (Blood/CSF Toxoplasma PCR were negative)//Patient did NOT receive anti-Toxoplasma treatment; Pt received ONLY Steroids x 6 wks (for Post infectious neurologic presentation)//Patient had complete clinical cure after steroid treatment |
| Leroy 2020 | Polymyositis complicated by motor deficit of all four limbs, leptomeningitis//in a 33-yr-old immunocompetent male of French nationality, who had recently visited Senegal and Hx of eating raw meat and unwashed fruits//who presented with fever, malaise, decreased visual acuity, headaches, myalgias, dyspnea//w significant transaminitis (AST/ALT 2268/1619 IU/L; unl <40) and significantly elevated CPK (77,000 IU/L; unl < 190)//w Brain MRI showing leptomeningitis//w Serologic diagnosis of Toxoplasmosis made ~1 month after onset of symptoms with positive Toxoplasma IgG, Toxoplasma IgM, Toxoplasma IgA and low avidity//Positive Toxoplasma PCR from muscle biopsy and aqueous humour//With serotyping of T.gondii strain Africa or Recombinant I/III//With Muscle Biopsy showing granulomatous inflammation and myocyte necrosis with bradyzoites positive also with immunostaining for Toxoplasma //Patient treated with P/S x 6 weeks and due to the chorioretinitis got also TMP/SMX x 1 year///Patient had complete clinical cure of systemic symptoms; except for the persistence of decrease in visual acuity, despite treatment |
| Martinot 2020 | CNS- Brown-Sequard syndrome //in a 31-yr-old patient with spinal cord toxoplasmosis//Spinal MRI showed a 12-mm intramedullary C3–C4 cervical tumor on the left that had ring enhancement after a gadolinium injection, with normal Brain Imaging at the same time/////who had complete regression of all neurologic deficits after few weeks of pyrimethamine/sulfadiazine, and who after secondary prophylaxis x1 year had f/up MRI showing sequellar intramedullary image without contrast enhancement) |
| Chang 2019 | CNS toxoplasmosis with Rapid progressive cognitive decline within 1 month//in a 64-yr-old immunocompetent man //who presented with fever and mental status changes, wide-base gait and right -side deviation//Brain MRI showed lesion in Let internal capsule and thalamus////Spinal tap showed elevated opening pressure; CSF protein was elevated (50 mg/dl) without CSF pleocytosis //Positive Toxoplasma IgG in blood and CSF (no results for Toxoplasma IgM in serum were given)////Started on TMP/SMX, but his condition deteriorated; until he was switched to Pyrimethamine; with regression also of brain MRI lesions on f/up MRI //(patient had regularly fed with cats for years) |
| Leveque 2019 | Myopericarditis//in a 23-yr-old immunocompetent man from France, presented with a 2 ds Hx of intense chest pain typical of pericarditis//ECHO and EKG were normal but troponin was elevated (31.3 ng/l; unl < 14) and CRP was elevated too//Toxoplasma serology was negative, but Toxoplasma PCR in blood was positive//Cardiac symptoms self-resolved with anti-inflammatory medications after 3 ds; WITHOUT anti- Toxoplasma treatment//Cardiac MRI at f/up showed evidence of myocarditis //(Blood Toxoplasma PCR became negative after 2 wks of anti- Toxoplasma treatment and Toxoplasma IgG and IgM became positive (confirming recent seroconversion) |
| Basit, Nasir et al. 2018 | CNS Toxoplasmosis infection ///20-yr-old immunocompetent male (HIV negative) from Pakistan, with 3 wks Hx of fever and Unilateral weakness, with gradual development of ALOC, neck stiffness, hypertonia, weakness in R upper and lower libs; CSF without pleocytosis or elevated protein//Brain MRI with multiple ring enhancing lesions in white and grey matter, with surrounding vasogenic edema on FLAIR images//Had high positive Toxoplasma IgG and IgM//Started treatment with TMP/SMX + Steroids//F/up MRI 2 wks later showed decrease in size of brain lesions and of the surrounding edema/// |
| Cai 2018 | NMDA encephalitis///in a 9-yr-old immunocompetent who presented with seizures, headaches and vomiting CSF and Brain MRI initially normal and self-recovered without any treatment //1 weeks later development of unexplained personality and behavior changes, recurrence of seizures and fever//Repeated CSF with lymphocytic pleocytosis and positive anti-NMDAR antibody. //Had positive Toxoplasma IgM and IgG.//Diagnosed with anti-NMDA encephalitis associated with acute acquired toxoplasma gondii infection//Treated with 10 days azithromycin with substantial recovery from clinical symptoms (immunotherapy was been refused)//F/up 2 mo later patient completely asymptomatic |
| Cortes 2018 | Disseminated disease, with rapid neurologic deterioration and multiorgan failure that led to death in a 72-yr-old immunocompetent patient from Chocó, Colombia; who presented with a 12-day hx of fever, headache//with Brain CT showing hydrocephalus and fronto-parietal periventricular hypodensities //with histopathologic findings at autopsy showing tissue cysts morphologically suggestive of being bradyzoites of Toxoplasma gondii; confirmed by immunohistochemistry in heart, brain, and striated muscle. |
| Henao-Martinez, Montoya 2018 | Myocarditis (and mild transaminitis and bilateral retinitis)//in a 29-yr-old immunocompetent woman (HIV negative) from the US (after a trip to Nicaragua x 10 ds; ate undercooked meat during the trip)//presented with acute onset of fever, retroorbital headache, myalgias and rash//LADP also developed 12 ds later//, with transaminitis, anemia and lymphocytosis//Continued fevers, malaise and had new onset of blurry vision within 1 mo into her illness// Toxoplasma IgG and IgM were high positive; Toxoplasma IgA and IgE high positive//Troponin was mildly elevated (0.26; unl < 0.05 ng/mL)//Started TMP/SMX; and switched to Clindamycin (without Pyrimethamine) due to severe nausea with TMP/SMX //Got anti- Toxoplasma treatment for 8 wks and symptoms gradually resolved (including resolution of retinal findings), & troponin normalization (for ocular findings also received intravitreal clindamycin) |
| Henao-Martinez, Montoya 2018 | Myocarditis and Transaminitis//in a 30-yr-old immunocompetent male from the US (after a family trip to Nicaragua x 10ds, having eaten undercooked meat during the trip)//presented with fatigue, myalgias and bilateral conjunctivitis; transaminitis//Had high positive Toxoplasma IgG, High positive Toxoplasma IgM and igA and low avidity//mildly elevated troponin (0.1 ng/mL; unl < 0.05)//Due to persistence of symptoms got TMP/SMX x 2 weeks and his symptoms resolved completely//(Per authors conclusion: Acute toxoplasmosis remains an important diagnostic consideration among travelers with acute illness//Acute toxoplasmosis in immunocompetent patients with evidence of end organ injury is an indication for anti- Toxoplasma treatment)// |
| Akturk, Sotello et al. 2017 | Toxoplasmic encephalitis with multiple bilateral ring enhancing brain lesions in an immunocompetent 32-yr-old male with increasing agitation and confusion, personality changes and Hx of recurrent headaches with onset of HA few months PTA//Brain CT showing multifocal white matter lesions.//with Brain MRI showing extensive bilateral cortical and subcortical concentric ring-enhancing white matter lesions throughout both cerebral hemispheres; with lesions were more prominent in left parietal and frontal lobes//Treatment with steroids for presumed multiple sclerosis caused worsening of symptoms and increase in size of the brain MRI lesions//Subsequently, brain biopsy confirmed T.gondii infections by histopathology and PCR and treatment with Pyrimethamine/Sulfadiazine decreased the size of the brain lesions dramatically (case of severe Toxoplasmosis due to inappropriate administration of high dose steroids for mis-diagnosis for multiple Sclerosis- At the time of Toxoplasma serology the serologic profile was non-acute; however given the clinical presentation few months earlier, the Toxoplasma serology results at the time of testing are not inconsistent with an acute infection -few months earlier-at the time of clinical presentation) |
| Pustorino 2017 | Cerebral Toxoplasmosis //in a 30-yr-old immunocompetent man (HIV negative) from Italy with a 5 yr hx of monthly frontal headache, with worsening intensity and frequency over the last 1 month, with associated episodes of sudden falls without loss of consciousness, followed by unjustified crying//30 yr old immunocompetent man with Hx of after eating poorly cooked pork meat ///Brain CT showing multiple calcifications involving the basal ganglia and semioval centers//Brain MRI T2 weighted images showing multiple cystic lesions surrounded by brain edema, non enhancing after contrast///EEG showing mild slowing over left temporal region//no follow up for 20 mo, but due to daily severe headaches and secondary generalized seizures was readmitted wth Brain CT and MRI showing marked size increase of cystic lesions with ring enhancement and diffuse perilesional edema with midline shift//S/P emergency surgical removal of 2 large brain cysts, histopathologically showing several bradyzoites and positive T.gondii DNA PCR//with initiation of anti-Toxoplasma treatment with pyrimethamine/sulfadiazine + Dexamthasonze (later changed to pyrimethamine/clindamycin due to rash with sulfadiazine) (not more clinical details given)//A 20 mo f/up there was resolution of Headaches and persistence of sporadic partial motor seizures and f/up brain MRI showing mild decease in size of cystic lesions with reduction of perilesional edema and contrast enhancement |
| Beltrame, Venturini et al. 2016 | Seizures secondary to toxoplasmosis////15-yr-old immunocompetent boy, with LADP and recurrent seizures, after vacation to Ethiopia, with EEG showing sporadic single spike or sharp-wave paroxysms//with T.gondii serology consistent with acute primary infection//Brain MRI was normal//with normalization of the EEG after 4 weeks of anti- Toxoplasma treatment with P/S/FA//with recurrence of seizures 5 months later, with reappearance of fatigue and cervical LADP//with negative repeat brain MRI///with elevated CSF protein level (250 mg/dl; with the rest of the CSF analysis normal//with negative CSF Toxoplasma PCR at which time a diagnosis of epilepsy was made and seizures were controlled with valproic acid (this case represented the first reported case of seizures during acute primary toxoplasmosis in immunocompetent patient) |
| Bousquet 2016 | Acute myocarditis/ in a 20 yr old immunocompetent military man in Begin, with 2 ds Hx of headaches, myalgias and malaise (afebrile)//EKG with incomplete RBBB, very elevated Troponin and CPK; (suspected Acute MI but coronary angiography was normal)//Cardiac MRI: areas of myocardial edema//Toxoplasma serology showed seroconversion (initially positive Toxoplasma IgM, negative Ig and 2 wks later, positive Toxoplasma IgG and IgM)// treated with TMP/SMX x ~2 weeks//Patient fully recovered (in response to treatment) with no complications (except for significant asthenia × 3 month) (He was considered unfit for the operational field) |
| Harbada 2016 | Toxoplasma cerebritis and encephalitis///23-yr-old immunocompetent male residing in Oman with a 2 wks Hx of weakness, incoordination of R upper and lower extremities, 5 ds Hx of throbbing headache, and visual blurring//Brain MRI T2 weighted images showing ill-defined hyperintense lesion in Right cerebellar hemisphere with perilesional edema, extending along the right foramen of Luschka///Post Contrast T1 images showing heterogeneous post-contrast enhancements with peripheral enhancing ring ///Underwent surgical excision due to concern for malignant space occupying lesions///histopathology showed necrosis, hemorrhage, perivascular infiltrates, T.gondii cysts and evidence of cerebritis and encephalitis///treated with Clindamycin + Azithromycin due to G6PD deficiency//post surgery neurologic status deteriorated and Brain MRI showing increase in perilesional edema and inflammation involving the brain stem (Steroid doses were increased//Patient clinically deteriorated despite anti- Toxoplasma treatment and died the 10th postsurgical day due to spreading Toxoplasma cerebritis and encephalitis) |
| Hoti 2016 | Toxoplasmic encephalitis //in a 45-yr-old immunocompetent HIV negative woman from Pakistan, with headaches and vomiting x 2 months; with confusion, behavioral problems, weakness in R upper limb//Brain CT showing a hypodense lesion in left Frontoparietal region; with Brain MRI T1 images showing a hypodense lesion in left parietal area; contrast enhancing in T1 contrast images; and T2 hyperintense//S/P total surgical excision of the mass due to concern for neoplasm; with Brain histopathology showing inflammatory features of toxoplasmosis in cerebral cortex and grey matter, with bradyzoite encased within cysts; Positive Toxoplasma IgG and IgM//Post surgery her Right upper limb weakness grossly improved and speech and higher motor functions remained intact//Was treated with TMP/SMX x 14 ds and 6 months post OP her condition was stable//No immunosuppression concern at 1 year of f/up. |
| Manwani 2016 | CNS toxoplasmosis//in a 14-yr-old immunocompetent boy (HIV negative × 2) from India with a 10 ds Hx of difficulty closing R eye, deviation of angle of the mouth on the left, nasal regurgitation of feeds and unsteady wide-based gait; central R facial nerve palsy, with involvement also of the IX and X cranial nerves//Brain MRI showing a hypodense lesion in the pons extending into the medulla, with heterogeneous enhancement with contrast, with vague ring enhancement dorsally, with initially concern for Tuberculoma//Due to progressive increasing difficulty in swallowing, absent gag reflex and R hemiparesis, underwent surgical excision of the brain mass that showed zones of necrosis, thrombosed vessels and aggregate large histiocytes with a single T.gondii bradyzoite with positive Toxoplasma immunostaining//Positive Toxoplasma IgM//Despite initiation of TMP/SMX there was NO neurologic improvement within 1 week of treatment; w subsequent development brain stem dysfunction and eventually cardiac arrest and death 2 weeks after anti- Toxoplasma treatment initiation. |
| Azarpira 2014 | ABSTRACT: Cerebral toxoplasmosis is the most important opportunistic infection in patients with acquired immunodeficiency syndrome. However, it is a rare finding in immunocompetent persons. The patient was a 14 yr-old boy who presented with headache and vertigo. Toxoplasma serology revealed raised IgG antibody level. No primary or secondary immune deficiency was found. Radiologic examination revealed ventriculitis. Microscopically, the lesion consisted of reactive gliosis and calcification. After antitoxoplasma treatment, the patient condition improved. Brain toxoplasmosis usually presented as periventricular/basal ganglial lesions. We report a case of a child patient with an atypical pattern of toxoplasma encephalitis, presenting with ventriculitis. |
| Li 2014 | CNS toxoplasmosis//in a 33-yr-old immunocompetent male from China with 9 month Hx of dysphagia and numbness of left limb x 1 mo; with decreased sensation in R upper and lower extremities, expressive aphasia, positive Babinski on the R, papilledema, //Brain CT showing an isodense lesion with surrounding edema//Brain MRI showing a space occupying lesion, isointense in T1 and Hypointense in T2 and adjacent cerebral edema//Post contrast MRI showing mushroom-shaped lesions with irregular enhanced rim //Serum and CSF Toxoplasma IgG were positive//Underwent total mass removal and his preoperative neurologic symptoms improved//Histopathology of the excised brain mass showed parasite within a pseudocyst structure; with positive Toxoplasma immunostaining//Was treated with Azithromycin (initially IV and then PO × 4 weeks) with dramatic clinical and radiologic improvement; with no recurrence in f/up MRI 2.5 yrs post OP) |
| Paruthikunnan 2014 | Disseminated toxoplasmosis with pulmonary and CNS involvement//in a 28-yr-old immunocompetent (HIV negative) pregnant woman from India, with intermittent fever and cough × 1 month; with elevated inflammatory markers, Eosinophilia (18%)//Patient had an abortion at the time of high fever//CXR showed multiple ill-defined nodular opacities in both lungs and patchy areas of consolidation in R upper and mid zones//Chest CT showing an area of consolidation the RUL and multiple nodules with GGO haloes around them-There was no pleural effusion and no significantly enlarged mediastinal LN//Due to high suspicion for TB initially; patient was treated with anti-TB therapy///Subsequently patient became drowsy with deteriorating level of consciousness//Brain MRI showed an irregular ring enhancing lesion in the R globus pallidus and R internal capsule; Hypointense on T1 and Hyperintense in T2 images/ with ADC (apparent Diffusion coefficient) images showing that the lesion has a peripheral rim of restricted diffusion with a central area of facilitated diffusion//Postcontrast coronal T1-weighted images on admission show the same lesion enhancing peripherally and another enhancing nodular lesion in the right superior frontal gyrus //Excisional biopsy of a Cervical LN showed T. gondii Trophozoites on histopathology//Strongly Positive Toxoplasma IgG and IgM//Started on anti- Toxoplasma treatment with P/S and Clindamycin and her clinical condition improved significantly in response to therapy//F/up CXR after 1 mo of anti- Toxoplasma therapy showed resolution of lung opacities//Examination of placenta and abortus showed the presence of placental and congenital toxoplasmosis in the fetus///F/up Chest CT 4.5 mo later also showed resolution of consolidation and nodules with bronchiectatic changes seen in the segment previously affected by consolidation//Repeat Brain MRI after 5 months also showed near complete resolution of the brain lesion, with some gliotic changes in the R basal ganglia |
| Ramachandran 2014 | CNS toxoplasmosis//in a 42-yr-old immunocompetent male (HIV negative) from India, with Headache and neck pain x 1 week; weight loss X 1 month, but NO fever; with elevated inflammatory markers//with Brain MRI showing multiple large bilateral lesions that appeared hypotense in T1 images and hyperintense in T2/FLAIR sequences//with intense homogeneous enhancement post contrast administration//Patient’s symptoms worsened over the next 3 ds //Repeat head CT showed multiple homogeneous enhancing hyperdense lesions with surrounding peri-legional edema in both cerebral hemispheres concerning for CNS lymphoma///Brain MRI the same day showed new lesions in the left Thalamus and globus pallidus with restricted diffusion on DWI images with los signal in ADC images suggestive of true restriction//MR spectroscopy showed elevated Lipid lactate peak///In view of the multiplicity of brain lesion and the onset of newer lesions within a span of one week, the possibility of CNS Toxoplasmosis was raised//CSF Toxoplasma IgG and IgM were Highly positive//Patient left against medical advice and subsequently died due to respiratory failure/// |
| Undseth 2014 | Multi-organ failure; pneumonitis, myocarditis, hepatitis, and meningoencephalitis//in a 39-yr-old immunocompetent man (HIV negative multiple times) from Norway, with Disseminated Toxoplasmosis with mutliorgan involvement with pneumonia, myocarditis, hepatitis, meningoencephalitis//who presented with Headache, High Fever and Diarrhea, generalized LADP//CSF with slight pleocytosis (11 cells/mm3)//During a LN excision procedure became respiratory and circulatory unstable and transferred to a regional hospital with Hypoxia (needing 70% FiO2), w high fevers//Required Inotropes and subsequently also mechanical Ventilation x 11 ds total/ Corticosteroids were added initially to his antimicrobial regimen//Had elevated inflammatory markers (CRP = 186 mg/dl; unl < 10.0) thrombocytopenia, Very elevated CPK and LDH, transaminitis and elevated γGT, Very elevated Ferritin (27,220 μg/l) and elevated Troponin; Low CD4 (133 cells/μL) and CD8 cells///Initial Brain MRI was normal but second MRI showed meningeal enhancement without intracerebral pathology//Patient was consistently confused and disoriented for a long period////Toxoplasma serology with high positive Toxoplasma IgM and Toxoplasma IgG and low avidity & positive Toxoplasma blood PCR & positive CSF Toxoplasma PCR//All biopsies (3 LN and Bone marrow biopsies (were positive for Toxoplasma cysts by microscopy; with the first POSITIVE results for Toxoplasmosis became available on HD #8//Haemophagocytosis was described//Was started on IV TMP/SMX //Once toxoplasmosis diagnosis was made on d#8 and anti-Toxoplasma treatment was started, clinical improvement was seen a few ds later///By D#22 he was overall more stable, LADP had decreased in size; but continued to have high fevers for another 16 ds & had persistent tachycardia with elevated troponin//On d#72 was transferred to a rehabilitation unit//After 1 year he was fully rehabilitated and back to full time work///Shortly after this developed visual disturbances and diagnosed with Toxoplasma chorioretinitis and anti-Toxoplasma treatment was resumed//The patient’s PLTs normalized after 3 wks of TMP/SMX//The patient had high Ferritin in serum and erythrophagocytosis in LN biopsy; however ferritin levels fell from 27, 220 to 1549 μg/L after 5 ds of TMP/SMX and also LDH decreased from 2663 to 657 IU/L)//RISK factors: had recently travelled across the Greenland glacier under quite challenging conditions and possibly consumed undercooked food//Primary infection was treated x7 wks and did NOT receive secondary prophylaxis; However was placed on long term secondary prophylaxis after the ocular toxoplasmosis reactivation 1 year later/// |
| De Souza Giassi 2014 | Acute Respiratory failure in a 36-yr-old male (w Hx of type 2 DM) secondary to acute toxoplasmosis with extensive lung involvement; who presented w 2 wks febrile illness, headache and progressive dyspnea few ds prior to admission; w crackles in lung exam, hypoxia to 82–86%; splenomegaly and in Lab values: lymphocytosis, transaminitis and elevated inflammatory markers//Chest CT w diffuse GGO, peribroncho-vascular and septal thickening and nodules, and small pleural effusions//Patient responded to anti-Toxoplasma treatment with complete resolution of clinical symptoms without subsequent relapse///Complete resolution also of Chest CT findings after 3 mo of reatment |
| De Souza Giassi 2014 | Acute Respiratory failure in a 56-yr-old female (w Hx of type 2 DM) secondary to acute toxoplasmosis with extensive lung involvement//who presented w 2 wks febrile illness, headache and progressive dyspnea few ds prior to admission; w crackles in lung exam, hypoxia to 82–86%; splenomegaly and in Lab values: lymphocytosis, transaminitis//Chest CT w diffuse GG and peribrochovascular and septal thickening AND mediastinal paratracheal LN enlargement//Patient responded to anti-Toxoplasma treatment with complete resolution of clinical symptoms without subsequent relapse |
| De Souza Giassi 2014 | Acute Respiratory failure in a 38-yr-old-female secondary to acute toxoplasmosis with extensive lung involvement who presented w 2 wks febrile illness, dyspnea and cough; w crackles in lung exam, hypoxia to 82–86%; splenomegaly and in Lab values: lymphocytosis, transaminitis//Chest CT w diffuse GGO, peribroncho-vascular and septal thickening and atelectasis and small pleural effusions//Patient responded to anti-Toxoplasma treatment with complete resolution of clinical symptoms without subsequent relapse/// |
| Abhilash, Roshine 2013 | High grade intermittent fever of 6 months duration, generalized arthralgia, significant weight loss, cervical and axillary LADP, splenomegaly (4 cm below the left costal margin.)/////in a 32-yr-old immunocompetent HIV negative woman///with LN biopsy showing reactive follicular hyperplasia//Bone Marrow biopsy showing multiple oval cysts suggestive of T.gondii //Toxoplasma IgM strongly positive and Toxoplasma IgG positive//Patient responded to pyrimethamine and clindamycin treatment x 2 wks with resolution of fevers and regression of LADP and splenomegaly at the 3 months f/up |
| Aksoy, Tanir 2013 | Diagnosis of acute disseminated encephalomyelitis (ADEM) in a 10-yr-old immunocompetent boy (HIV negative x2) with difficulty walking and urinary and stool incontinence//with normal inflammatory markers, diagnosed with ADEM in the context of recent acute primary Toxoplasmosis infection (with case presenting as the pure myelitis form of ADEM, with imaging findings nevertheless in both brain and spinal cord-but without encephalopathy////with CSF analysis showing pleocytosis, lymphocytosis (210 lymphs/mm3); mildly elevated CSF protein (54 mg/dl)///FLAIR MRI showing high intensity lesions in the periventricular white matter, corona radiata, semiovale center and left parietal lobe; no mass effect and no contrast enhancement//All brain lesions were hyperintense in DWI and ADC(apparent diffusion coefficient) images AND Spinal MRI showing diffuse abnormal signal intensity C4-T6 level with no enhancement (imaging findings consistent with ADEM)///Boy was treated with steroids (high dose for first 5 ds) and on d3 of steroid there was significant reduction in the neurologic findings and on d7 there was complete resolution//The positive serologic results for Toxoplasmosis became available 2 wks after admission (after the improvement of symptoms on steroids only) and was treated with P/S x 4 wks (Patient had a 4-fold rise in Toxoplasma IgG titers over a 3 wk interval, with positive Toxoplasma IgM and low IgG avidity, indicating recent API//F/up MRI 6 mo later showed disappearance of the initial lesions AND child without neurologic findings |
| Sobanski 2013 | Pulmonary toxoplasmosis, severe retinochoroiditis//in a 47-yr-old immunocompetent (HIV negative) man (case from France); who presented with high fever, dyspnea and flu like symptoms (no duration of symptoms PTA was given); night sweats, N/V, rash and generalized LADP//Hypoxia (92% O2 Sats)//CXR diffuse interstitial infiltrates; Transaminitis; high LDH, lymphocytosis//Toxoplasma serology with seroconversion: initially Toxoplasma IgM positive, Toxoplasma IgG negative and 2 mo later Toxoplasma IgG positive (and IgM negative at that time)//Chest CT at that stage showed mediastinal LADP WITHOUT parenchymal infiltrates//BAL: positive Toxoplasma DNA PCR// treatment initiated with Spiramycin X 3 weeks (HD #12) and clinically improved within 3 ds (with defervescence)////Relapse of clinical status 1 mo later with recurrence of fevers, night sweats and weight loss AND decreased Visual acuity//PET scan (2 mo after symptoms onset) showed increased LN uptakes AND Inguinal LN biopsy (2 mo after symptoms onset) was positive for Toxoplasma DNA PCR (indicating ineffectiveness of Spiramycin treatment)//At that time treated with Pyrimethamine + Clindamycin x 6 weeks with clinical response except for only partial recovery of eyesight///Genotype showed Atypical genotype (Risk: consumption of raw horse meat from Brazil and Canada |
| Yang 2013 | Multi-organ failure, Respiratory failure, HLH, disseminated toxoplasmosis//in a 41-yr-old immunocompetent (HIV negative) male from China; who presented with a 4 d Hx of fever, malaise, dry cough, confusion//Along with high fever, HSM, cytopenias, hyperferritinemia, hypofibrinogenemia, hypertriglyceridemia suggestive of Hemophagocytic syndrome (leukopenia (WBC 2290/ μL) and Thrombocytopenia (PLT = 9.000/μL), transaminitis, elevated LDH, very high Ferritin (23,800μg/L) and high TG; //CXR with interstitial and alveolar infiltrates//HSM//(Risk factors: forest policeman/ hunter, drinking stream water)//Clinical condition rapidly worsened with respiratory failure and need for IMV on HD 3; MOF developed on HD 8 and patient died//diagnosis of Toxoplasmosis made postmortem with Bone Marrow Bx showing large amount of T.gondii tachyzoites and Cysts and positive Toxoplasma PCR// |
| Demar 2012 | 22-yr-old male from French Guiana, admitted in ICU for B/L interstitial pneumonia, no IMV, hypoxia, Chest CT with Bilateral interstitial pneumonia, Cardiomegaly, pericarditis///ABSTRACT: A newly described form of toxoplasmosis, ‘Amazonian toxoplasmosis’ (AT), has been reported since 2002 in French Guiana. It is characterized by severe cases and atypical strains linked to a neotropical forest-based cycle. We report on the cases of AT that required intensive care management. We performed a prospective observational study on hospitalized adults in the Intensive Care Unit (ICU) from 2002 to 2008. Clinical and laboratory data, microbiological findings and outcomes were recorded. Data, including the ICU simplified acute physiology score and the pneumonia severity index, were calculated. Epidemiological risk factors for AT were assessed through questionnaires. Eleven non-immunodeficient patients were admitted to the ICU in Cayenne for life-threatening pneumonia associated with disseminated toxoplasmosis. |
| Demar 2012 | 41-yr-old male from French Guiana, admitted in ICU, for hypoxia, B/L interstitial pneumonia//ABSTRACT: A newly described form of toxoplasmosis, ‘Amazonian toxoplasmosis’ (AT), has been reported since 2002 in French Guiana. It is characterized by severe cases and atypical strains linked to a neotropical forest-basedcycle. We report on the cases of AT that required intensive care management. We performed a prospective observational study on hospitalized adults in the Intensive Care Unit (ICU) from 2002 to 2008. Clinical and laboratory data, microbiological findings and outcomes were recorded. Data, including the ICU simplified acute physiology score and the pneumonia severity index, were calculated. Epidemiological risk factors for AT were assessed through questionnaires. Eleven non-immunodeficient patients were admitted to the ICU inCayenne for life-threatening pneumonia associated with disseminated toxoplasmosis. |
| Demar 2012 | 36-yr-old male from French Guiana, admitted to ICU, needed IMV for hypoxia, B/L interstitial pneumonia//ABSTRACT: A newly described form of toxoplasmosis, ‘Amazonian toxoplasmosis’ (AT), has been reported since 2002 in French Guiana. It is characterized by severe cases and atypical strains linked to a neotropical forest-based cycle. We report on the cases of AT that required intensive care management. We performed a prospective observational study on hospitalized adults in the Intensive Care Unit (ICU) from 2002 to 2008. Clinical and laboratory data, microbiological findings and outcomes were recorded. Data, including the ICU simplified acute physiology score and the pneumonia severity index, were calculated. Epidemiological risk factors for AT were assessed through questionnaires. Eleven non-immunodeficient patients were admitted to the ICU in Cayenne for life-threatening pneumonia associated with disseminated toxoplasmosis. |
| Demar 2012 | 39-yr-old male from French Guiana, admitted to ICU, needed IMV for hypoxia, B/L interstitial pneumonia //ABSTRACT: A newly described form of toxoplasmosis, ‘Amazonian toxoplasmosis’ (AT), has been reported since 2002 in French Guiana. It is characterized by severe cases and atypical strains linked to a neotropical forest-based cycle. We report on the cases of AT that required intensive care management. We performed a prospective observational study on hospitalized adults in the Intensive Care Unit (ICU) from 2002 to 2008. Clinical and laboratory data, microbiological findings and outcomeswere recorded. Data, including the ICU simplified acute physiology score and the pneumonia severity index, were calculated. Epidemiological risk factors for AT were assessed through questionnaires. Eleven non-immunodeficient patients were admitted to the ICU in Cayenne for life-threatening pneumonia associated with disseminated toxoplasmosis. |
| Demar 2012 | 19-yr-old male from French Guiana, admitted to ICU, needed IMV, for hypoxia, pneumonia “white lung”, meningismus//ABSTRACT: A newly described form of toxoplasmosis, ‘Amazonian toxoplasmosis’ (AT), has been reported since 2002 in French Guiana. It is characterized by severe cases and atypical strains linked to a neotropical forest-based cycle. We report on the cases of AT that required intensive care management. We performed a prospective observational study on hospitalized adults in the Intensive Care Unit (ICU) from 2002 to 2008. Clinical and laboratory data, microbiological findings and outcomes were recorded. Data, including the ICU simplified acute physiology score and the pneumonia severity index, were calculated. Epidemiological risk factors for AT were assessed through questionnaires. Eleven non-immunodeficient patients were admitted to the ICU in Cayenne for life-threatening pneumonia associated with disseminated toxoplasmosis. |
| Demar 2012 | 30-yr-old male from French Guiana, admitted to ICU, needed IMV for hypoxia, B/L interstitial pneumonia; had cardiac arrhythmia//ABSTRACT: A newly described form of toxoplasmosis, ‘Amazonian toxoplasmosis’ (AT), has been reported since 2002 in French Guiana. It is characterized by severe cases and atypical strains linked to a neotropical forest-based cycle. We report on the cases of AT that required intensive care management. We performed a prospective observational study on hospitalized adults in the Intensive Care Unit (ICU) from 2002 to 2008. Clinical and laboratory data, microbiological findings and outcomes were recorded. Data, including the ICU simplified acute physiology score and the pneumonia severity index, were calculated. Epidemiological risk factors for AT were assessed through questionnaires. Eleven non-immunodeficient patients were admitted to the ICU in Cayenne for life-threatening pneumonia associated with disseminated toxoplasmosis. |
| Demar 2012 | 38-yr-old male from French Guiana, admitted to ICU, needed IMV for B/L interstitial pneumonia//ABSTRACT: A newly described form of toxoplasmosis, ‘Amazonian toxoplasmosis’ (AT), has been reported since 2002 in French Guiana. It is characterized by severe cases and atypical strains linked to a neotropical forest-based cycle. We report on the cases of AT that required intensive care management. We performed a prospective observational study on hospitalized adults in the Intensive Care Unit (ICU) from 2002 to 2008. Clinical and laboratory data, microbiological findings and outcomes were recorded. Data, including the ICU simplified acute physiology score and the pneumonia severity index, were calculated. Epidemiological risk factors for AT were assessed through questionnaires. Eleven non-immunodeficient patients were admitted to the ICU inCayenne for life-threatening pneumonia associated with disseminated toxoplasmosis. |
| Demar 2012 | 28-yr-old female from French Guiana, admitted to ICU, with B/L interstitial infiltrated, had myopericarditis, cardiomegaly, low EF 26%, Hypokinesia/ABSTRACT: A newly described form of toxoplasmosis, ‘Amazonian toxoplasmosis’ (AT), has been reported since 2002 in French Guiana. It is characterized by severe cases and atypical strains linked to a neotropical forest-based cycle. We report on the cases of AT that required intensive care management. We performed a prospective observational study on hospitalized adults in the Intensive Care Unit (ICU) from 2002 to 2008. Clinical and laboratory data, microbiological findings and outcomes were recorded. Data, including the ICU simplified acute physiology score and the pneumonia severity index, were calculated. Epidemiological risk factors for AT were assessed through questionnaires. Eleven non-immunodeficient patients were admitted to the ICU in Cayenne for life-threatening pneumonia associated with disseminated toxoplasmosis. |
| Demar 2012 | 22-yr-old female from French Guiana, admitted to ICU, needed IMV for hypoxia, B/L interstitial pneumonia, had pericarditis//ABSTRACT: A newly described form of toxoplasmosis, ‘Amazonian toxoplasmosis’ (AT), has been reported since 2002 in French Guiana. It is characterized by severe cases and atypical strains linked to a neotropical forest-based cycle. We report on the cases of AT that required intensive care management. We performed a prospective observational study on hospitalized adults in the Intensive Care Unit (ICU) from 2002 to 2008. Clinical and laboratory data, microbiological findings and outcomes were recorded. Data, including the ICU simplified acute physiology score and the pneumonia severity index, were calculated. Epidemiological risk factors for AT were assessed through questionnaires. Eleven non-immunodeficient patients were admitted to the ICU in Cayenne for life-threatening pneumonia associated with disseminated toxoplasmosis. |
| Demar 2012 | 24-yr-old male from French Guiana, admitted to the ICU for hypoxia and B/L interstitial pneumonia; had meningismus//ABSTRACT: A newly described form of toxoplasmosis, ‘Amazonian toxoplasmosis’ (AT), has been reported since 2002 in French Guiana. It is characterized by severe cases and atypical strains linked to a neotropical forest-based cycle. We report on the cases of AT that required intensive care management. We performed a prospective observational study on hospitalized adults in the Intensive Care Unit (ICU) from 2002 to 2008. Clinical and laboratory data, microbiological findings and outcomes were recorded. Data, including the ICU simplified acute physiology score and the pneumonia severity index, were calculated. Epidemiological risk factors for AT were assessed through questionnaires. Eleven non-immunodeficient patients were admitted to the ICU in Cayenne for life-threatening pneumonia associated with disseminated toxoplasmosis. |
| Demar 2012 | 11-yr-old male from French Guiana, admitted to ICU, needed IMV for hypoxia, B/L interstitial pneumonia, had cardiomegaly, pericarditis, low EFABSTRACT: A newly described form of toxoplasmosis, ‘Amazonian toxoplasmosis’ (AT), has been reported since 2002 in French Guiana. It is characterized by severe cases and atypical strains linked to a neotropical forest-based cycle. We report on the cases of AT that required intensive care management. We performed a prospective observational study on hospitalized adults in the Intensive Care Unit (ICU) from 2002 to 2008. Clinical and laboratory data, microbiological findings and outcomes were recorded. Data, including the ICU simplified acute physiology score and the pneumonia severity index, were calculated. Epidemiological risk factors for AT were assessed through questionnaires. Eleven non-immunodeficient patients were admitted to the ICU in Cayenne for life-threatening pneumonia associated with disseminated toxoplasmosis. |
| Groh 2012 | Pneumonia, Congestive heart failure (CHF) (along with transaminitis, pancreatitis, hyponatremia and chorioretinitis) //in an immunocompetent (HIV negative) Chinese man living in French Guiana who presented with a 3 wk Hx of fever, dyspnea and confusion, weight loss//CXR with alveolar infiltrates //Had Tachycardia and findings of CHF, lung crackles in R lung, LADP and chorioretinitis and corneal ulcer//Had elevated cardiac markers, (Troponin and BNP), high LDH, Hyponatremia (Na nadir: 125; likely due to pneumonia associated SIADH), mild transaminitis & pancreatitis (high lipase) //High positive Toxoplasma IgG and IgM, low avidity and positive blood Toxoplasma PCR, positive mice subinoculation//Genotype analysis with 15 microsatellite markers showed Atypical T.gondii strain //ECHO showed low LVEF (35%) with global hypokinesia//Also w chorioretinitis in L eye suggestive of Toxoplasmosis (Risk: consumption of semi-raw Tapir 3 wks before onset of symptoms; Toxoplasma PCR was positive also from the frozen Maipour meat)//Patient responded to treatment with Pyrimethamin + Sulfadiazine (later sulfadiazine changed to clindamycin due to hepatotoxicity); anti-Toxoplasma treatment given x 6 weeks// |
| Kanno 2012 | Toxoplasmic encephalitis//in a 81-yr-old immunocompetent woman from Japan with Right lower limb discomfort, who subsequently developed memory disturbances)//with Brain MRI FLAIR images showing a high signal lesion in Left parietal region///with f/up MRI showing enlargement of original lesion and development of new lesion contralaterally (along with Left lower limb Dyskinesia, myoclonus, involuntary limb movements incoherent speech; low CD4 cells 286/μL, HIV negative), normal CSF analysis; High Toxoplasma IgG Antibodies, negative Toxoplasma IgM and negative CSF T.gondii PCR)//with repeat brain MRI due to worsening level of consciousness showing Bilateral temporal and frontal lesions with T2 target signs (on T2 weighted image a three-layered structure with low signal, high signal, and low signal)//(Due to suspicion of Toxoplasma encephalitis Pyrimethamine + Sulfadiazine was started with gradual improvement in patient’s level of consciousness, disappearance of involuntary limb movements AND ultimately disappearance of brain MRI lesions //((T2 target sign (core is iso-signal or low signal, the exterior is a high signal and the outermost side is iso-signal or iso-signal); an abscess core with an iso-signal or low signal compared with normal white matter of diffusion weighted imaging and the core with high signal on ADC mapping: are distinct imaging findings of toxoplasmic encephalitis) |
| Roubille 2012 | Myopericarditis w mild pericardial effusion in a 24-yr-old male, who presented with acute chest pain and SOB (with mild pericardial effusion developing after onset of fever), with elevated inflammatory markers, elevated troponin (peak Troponin 17.4 μg/L; unl <0.05)//with cardiac MRI showing LGE (late gadolinium enhancement) and mild pericardial effusion consistent with the diagnosis of myocarditis//Patient’s symptoms had resolved prior to the Toxoplasmosis diagnosis and without anti-Toxoplasma treatment; although 4 wks from presentation patient still had elevated troponin (0.4μg/L) (of note patient refused initiation of anti- Toxoplasma treatment at that time) |
| Neves 2011 | Disseminated toxoplasmosis//in a 41-yr-old immunocompetent man (HIV negative) from Brazil, presented with a 2 ds Hx of high fever, myalgias, severe headache and nausea; with transaminitis; with his condition rapidly deteriorating with development of dyspnea, cough, intense headache with meningeal signs, nausea and vomiting; cervical LADP during the 2nd week of illness; CXR showed B/L alveolar infiltrates//CSF analysis showed pleocytosis (35 cells/mm3) with lymphocytosis (85% lymphocytes)///Had positive Toxoplasma IgG and IgM with low avidity//Treated with Clindamycin + Pyrimethamine; with rapid clinical improvement; resolution of CXR findings; normalization of CSF findings and resolution of transaminitis//Remained asymptomatic at the 22 mo f/up |
| Galli Tsiropoulou 2010 | The authors report a 5-yr-old boy who presented with cervical lymphadenopathy because of acquired toxoplasmosis accompanied with unilateral facial nerve paralysis. Toxoplasma gondii DNA detection in blood by polymerase chain reaction, as well as elevated specific immunoglobulin M antibodies against it, established the diagnosis. Characteristic brain lesions on magnetic resonance imaging were absent and ophthalmologic examination revealed no inflammatory lesions in the retina and choroid. Treatment with pyrimethamine, sulfadiazine, and folic acid resulted in a complete recovery after 2 months of therapy |
| Jimenez-Caballero 2010 | Case of ADEM in a 76-yr-old immunocompetent male (HIV negative) from Spain; who presented with a 7 ds Hx of fever, malaise, inability to walk, and drowsiness//ALOC, Stupor, nystagmus, dysarthria, R dysmetria, ataxia, global hypereflexia//Toxoplasma IgG and IgM were positive //CSF analysis showed hypoglycorrhachia (CSF Gl = 50/serum 93 mg/dl) and elevated CSF protein, but without CSF pleocytosis///Brain MRI showed multiple Hyperintense T2 lesions//FLAIR images showed pseudonodules with vascular distribution//Given presumed diagnosis of ADEM after acute Toxoplasma infection, patient was initiated on Steroids;(5 ds with a 15 ds tapering with good clinical response and progressively there was recovery in the LOC, hemiparesis, ataxia and dysarthria///At 3 mo f/up he was asymptomatic and brain MRI at 6 mo F/up showed resolution of the brain lesions (at that time there was significant rise in Toxoplasma IgG and IgM had become negative) |
| Nunura 2010 | Pneumonia, retinochoroiditis, hepatitis, synovitis and myositis//in a 37-yr-old immunocompetent male (HIV negative) marine on a military operation by the Peruvian Amazon x prior 4 mo///who presented with R hip pain and limping; subsequently on HD 5 developed Fever, Dyspnea, tachypnea, rales in the left hemithorax and decreased Visual acuity//Also had leukocytosis, transaminitis, CXR with diffuse interstitial infiltrates////Chest CT with multiple nodular cavities and pleural effusions//Eye findings suggestive of Toxoplasma chorioretinitis//On HD15 results of Toxoplasma serology showed positive Toxoplasma IgG, IgM, a thick blood smear was positive for tachyzoites//Initially was started on Clarithromycin + TMP/SMX+ Clindamycin +CTX (but on HD5 was changed to Vanco + Imipenem and his fever/cough and dyspnea persisted//After the Toxoplasma serology results had become available was started on Pyrimethamine + Sulfadoxine (Clindamycin + TMP/SMX were discontinued) and patient defervested on the 2nd d of this treatment //R hip MRI showed avascular necrosis and mild synovial effusion and R hip muscle biopsy showed T. gondii bradyzoites//Patient 1 year later had only achieved partial recovery from his chorioretinitis and hip disability//Risk factors: Cooked for the brigade, brigade frequently hunted mammals//drank stream water and ate undercooked meat and had 3 cats) |
| Pergola 2010 | Acute pericarditis and myocarditis//in a 32-yr-old immunocompetent man (HIV negative) living in France who presented with 2 wk Hx of severe chest pain worsening with deep breathing, fever, arthralgia, malaise, LADP//Had elevated cardiac enzymes (troponin, CPK), high LDH, elevated inflammatory markers//ECHO with moderate pericardial effusion, hyperechoic pericardium slightly detached in the back side// Toxoplasma IgM was positive; with further increase in Toxoplasma IgM titers within the next 10 ds (Toxoplasma IgG still negative at that time; but became Toxoplasma IgG positive 10 weeks after D/C)//Patient’s condition clinically improved and patient was discharged on HD12, with resolution of ECHO findings (resolution of pericardial effusion) ///Patient received treatment with Spiramycin x 1 month; in addition to anti-inflammatory medications// |
| Simanaityte 2010 | Toxoplasmic pneumonia with small left pleural effusion.//in a 29-yr-old immunocompetent man (HIV negative) (most likely from France); who presented with a 4 ds Hx of malaise, high fevers, night sweats//subsequently developed headache without meningeal signs; weight loss, generalized LADP; Hypoxia (92% O2 Sats); elevated inflammatory markers, high LDH, //Chest CT showed left lobar pneumonia with small pleural effusion//Given the mononucleosis like syndrome presentation and the LADP Toxoplasma serology was sent; with positive Toxoplasma IgG and IgM and low avidity//Patient initially received Roxithromycin, and defervested after 4 ds; and subsequently changed to Spiramycin (x 3 weeks total)//2 weeks after D/C patient remaining afebrile, although malaise persisted// |
| Alapatt 2009 | Cerebral toxoplasmosis in a 40-yr-old immunocompetent pregnant woman (HIV negative) from India who presented with a 4 mo Hx of behavioral changes and generalized seizures (during the 5th mo of pregnancy); 3 mo Hx of headaches, left sided weakness and spastic hemiparesis diplopia; with subsequent development of unsteady gait; urine and stool incontinence; confusion and dysphasia; Upper motor neuron palsy of the facial nerve; increased DTRs and positive Babinski on the Right side.//Brain MRI revealed large Hyperintense lesion in the R basal ganglia, periventricular grey matter, left frontal and parietal midbrain and pons; with hydrocephalus AND mass effect; with bulging of the mass on the R wall of the 3d ventricle (initially concerning for glioblastoma)//Underwent brain mass biopsy and ventriculostomy with improvement of the level of consciousness//Delivered vaginally///Histopathology revealed inflammatory pathology, most likely toxoplasmosis/ Serum Toxoplasma IgG and IgM were positive//Started P/S x 6 weeks//Repeat Head CT showed marked decrease in the size of the lesion//Continued anti-Toxoplasma treatment x 6 months and remained clinically well without headache, or confusion; Her Left hemiparesis had not fully recovered and remained on anticonvulsants/// |
| Habek 2009 | Toxoplasmic encephalitis, rapidly progressing dementia///69 yr old immunocompetent HIV negative male from Croatia, with a 2 mo hx of rapidly progressive cognitive decline with poor speech, dyslexia, dysgraphia, constructional apraxia, verbal and visual memory deficits, positive Babinski and left side and gait apraxia//Brain MRI T2 images showed Hyperintense lesions in both thalami and putamina and head of caudate nucleus without diffusion restriction on DWI sequences (T2 shine through) ///CSF showed elevated protein (1.08 g/L) without pleocytosis and elevated CRP//Clinical course complicated by gram negative sepsis and patient died, with toxoplasmic encephalitis revealed at the autopsy///Brain autopsy showed confluent small and soft partially hemorrhagic lesions in basal ganglia with few cysts containing T.gondii bradyzoites (per authors conclusion: Toxoplasmic encephalitis should be considered in the differential diagnosis as a rare cause of rapidly progressive dementia in immunocompetent patients. Moreover, in the presence of multiple hyperintense lesions on T2 and hypointense lesions on T1 images without diffusion restriction, toxoplasmosis should also be considered even in the absence of CSF pleocytosis, particularly so though in the presence of elevated CSF protein) |
| Pino Salinas 2009 | 23-yr-old male from Colombia Armed Forces, admitted to ICU with Respiratory failure, NYHAIII, myalgias, arthralgias, HA, LADP////ABSTRACT: Toxoplasmosis is a common opportunistic infection in patients infected with HIV/AIDS while in immunocompetent patients this infection causes symptoms only in 10% to 20% of the cases, generally with a benign and autoresolutive course. In the last decade some severe cases with visceral involvement has been reported in immunocompetent patients, though they were isolated or recovered during years. //We present the first Colombian report of an epidemic outbreak caused by Toxoplasma gondii in military personnel deployed to rural areas located at La Macarena, Meta, Colombia. All 18 cases were confirmed by IgG indirect immunofluorescence (IFI) with titers higher than 1:1024 (normal range: 1:16). Their main symptoms were fever, adenopathies and pulmonary and gastrointestinal compromise. One patient developed severe myocardial compromise. All the patients recovered after treatment with pyrimethamine/sulfadoxine and clindamycin for 3 weeks. A possible hypothesis for this out- break was the consumption of contaminated water with oocysts, and probably the severity of the compromise could be elicited by a “wild” strain of the parasite as it is reported in the literature. Unfortunately, it was impossible to isolate and identify the specific strain. |
| Pino Salinas 2009 | 31-yr-old male from Colombia Armed forces, who presented with dyspnea NYHA III, HA, myalgias, sweating, LADP//ABSTRACT: Toxoplasmosis is a common opportunistic infection in patients infected with HIV/AIDS while in immunocompetent patients this infection causes symptoms only in 10% to 20% of the cases, generally with a benign and autoresolutive course. In the last decade some severe cases with visceral involvement has been reported in immunocompetent patients, though they were isolated or recovered during years. //We present the first Colombian report of an epidemic outbreak caused by Toxoplasma gondii in military personnel deployed to rural areas located at La Macarena, Meta, Colombia. All 18 cases were confirmed by IgG indirect immunofluorescence (IFI) with titers higher than 1:1024 (normal range: 1:16). Their main symptoms were fever, adenopathies and pulmonary and gastrointestinal compromise. One patient developed severe myocardial compromise. All the patients recovered after treatment with pyrimethamine/sulfadoxine and clindamycin for 3 weeks. A possible hypothesis for this out- break was the consumption of contaminated water with oocysts, and probably the severity of the compromise could be elicited by a “wild” strain of the parasite as it is reported in the literature. Unfortunately, it was impossible to isolate and identify the specific strain. |
| Pino Salinas 2009 | 24-yr-old male from Colombia Armed Forces, admitted to ICU with respiratory failure, cough, dyspnea NYHA IV, HA, malaise, LADO///ABSTRACT: Toxoplasmosis is a common opportunistic infection in patients infected with HIV/AIDS while in immunocompetent patients this infection causes symptoms only in 10% to 20% of the cases, generally with a benign and autoresolutive course. In the last decade some severe cases with visceral involvement has been reported in immunocompetent patients, though they were isolated or recovered during years. //We present the first Colombian report of an epidemic outbreak caused by Toxoplasma gondii in military personnel deployed to rural areas located at La Macarena, Meta, Colombia. All 18 cases were confirmed by IgG indirect immunofluorescence (IFI) with titers higher than 1:1024 (normal range: 1:16). Their main symptoms were fever, adenopathies and pulmonary and gastrointestinal compromise. One patient developed severe myocardial compromise. All the patients recovered after treatment with pyrimethamine/sulfadoxine and clindamycin for 3 weeks. A possible hypothesis for this out- break was the consumption of contaminated water with oocysts, and probably the severity of the compromise could be elicited by a “wild” strain of the parasite as it is reported in the literature. Unfortunately, it was impossible to isolate and identify the specific strain. |
| Pino Salinas 2009 | 21-yr-old male from Colombia Armed Forces, who presented w cough/dyspnea, NYHAII, HA, malaise, LADP///ABSTRACT: Toxoplasmosis is a common opportunistic infection in patients infected with HIV/AIDS while in immunocompetent patients this infection causes symptoms only in 10% to 20% of the cases, generally with a benign and autoresolutive course. In the last decade some severe cases with visceral involvement has been reported in immunocompetent patients, though they were isolated or recovered during years. //We present the first Colombian report of an epidemic outbreak caused by Toxoplasma gondii in military personnel deployed to rural areas located at La Macarena, Meta, Colombia. All 18 cases were confirmed by IgG indirect immunofluorescence (IFI) with titers higher than 1:1024 (normal range: 1:16). Their main symptoms were fever, adenopathies and pulmonary and gastrointestinal compromise. One patient developed severe myocardial compromise. All the patients recovered after treatment with pyrimethamine/sulfadoxine and clindamycin for 3 weeks. A possible hypothesis for this out- break was the consumption of contaminated water with oocysts, and probably the severity of the compromise could be elicited by a “wild” strain of the parasite as it is reported in the literature. Unfortunately, it was impossible to isolate and identify the specific strain. |
| Pino Salinas 2009 | 31-yr-old male from Colombia Armed Forces who presented w cough/dyspnea, NYHA III, LADP, HA, myalgia and a 21-yr old with cough/dyspnea, NYHA II, HA, malaise ///ABSTRACT: Toxoplasmosis is a common opportunistic infection in patients infected with HIV/AIDS while in immunocompetent patients this infection causes symptoms only in 10% to 20% of the cases, generally with a benign and autoresolutive course. In the last decade some severe cases with visceral involvement has been reported in immunocompetent patients, though they were isolated or recovered during years. //We present the first Colombian report of an epidemic outbreak caused by Toxoplasma gondii in military personnel deployed to rural areas located at La Macarena, Meta, Colombia. All 18 cases were confirmed by IgG indirect immunofluorescence (IFI) with titers higher than 1:1024 (normal range: 1:16). Their main symptoms were fever, adenopathies and pulmonary and gastrointestinal compromise. One patient developed severe myocardial compromise. All the patients recovered after treatment with pyrimethamine/sulfadoxine and clindamycin for 3 weeks. A possible hypothesis for this out- break was the consumption of contaminated water with oocysts, and probably the severity of the compromise could be elicited by a “wild” strain of the parasite as it is reported in the literature. Unfortunately, it was impossible to isolate and identify the specific strain. |
| Gupta 2008 | Toxoplasma granuloma of the brainstem in a 27-yr-old immunocompetent male (HIV negative) from India with sudden onset of headache, left sided weakness and vomiting; with a similar prior episode 1 mo earlier that had self-resolved//Had anisocoria, crossed hemiplegia with left hemiparesis and Righ V, VII, Xi, and X cranial nerves involvement//Brain MRI showed on T1 images a hypotense pontine lesion with extension to midbrain; with heterogeneous contrast enhancement and vague ring enhancement//brain biopsy (due to concern for neoplasm) showed an inflammatory lesion (with dense microglia reaction mixed with foamy histiocytes; focal areas of active necrosis; with foci of spotty calcifications along the edge of the necrotic zone, along with few ruptured but calcified Toxoplasma cysts characteristic of Toxoplasmosis (Toxoplasma granuloma of the brainstem) (Risk factors: Prior Hx of owing a cat)//(Serial Toxoplasma IgG and IgM were within normal range)//Based on the histopathologic findings was started on P/S x4 wks //At 6 mo f/up had complete recovery with no residual neurologic deficits; with repeat brain MRI showing complete resolution of brain lesion//At 2 yrs f/up remained asymptomatic |
| Rostoff et al. 2008 | Myopericarditis with acute heart failure (NYHA IV), large pericardial effusion and B/L pleural effusions in a 67 y F, who presented w severe dyspnea at rest, left pleuritic chest pain, high fever, generalized LADP (w a PMH of suspected myocarditis 3 mo PTA with LVEF 35% but w normal troponin)//w CXR showing B/L pleural effusions and cardiomegaly//w ECHO showing LV systolic dysfunction with LVEF 33% and large pericardial effusion//w Chest CT confirming the presence of pericardial and pleural effusions//w markedly elevated inflammatory markers (CPR 232 mg/dl; ESR 100 mm/h); with slightly high Troponin (0.10–1.12 ng/dl)//With significant clinical improvement of cardiac symptoms after 3 wks of Spiramycin treatment (Spiramycin was used because of sulfa allergy); with normalization of inflammatory markers; resolution of CXR and ECHO findings with increase in LVEF to 50%//Patient was discharged after 7 wks of treatment with no further evidence of Heart Failure///Also with elevated serum CA-125 during acute presentation and normal CA-125 at 1 year follow up |
| Demar 2007 | The hospitalized patients, who did not have any immunodeficiencies, presented with an infectious disease with multivisceral involvement. Serological examination confirmed acute toxoplasmosis. One adult died, and a neonate and a fetus with congenital toxoplasmosis also died. During the investigation, 4 additional acute cases of toxoplasmosis were diagnosed among the 33 villagers. Only 3 inhabitants had serological evidence of previous T. gondii infection. In total, we reported 11 cases of toxoplasmosis: 8 multivisceral cases in immunocompetent adults, resulting in 1 death; 2 cases of lethal congenital toxoplasmosis in a neonate and a fetus; and 1 symptomatic case in a child. Molecular analysis demonstrated that identical isolates of only 1 atypical strain were responsible for at least 5 of the 11 cases of toxoplasmosis in the outbreak. No epidemiological sources could be linked to this severe community-wide outbreak of toxoplasmosis. |
| Leal 2007 | 41-yr-old immunocompetent male (HIV negative) from Brazil w 8 ds of fever, myalgias, HA; this occurred 20 ds after eating semiraw beef 20 ds earlier,//Progressed to Respiratory failure w B/L interstitial infiltrates///Toxoplasma IgM+, Positive Toxoplasma PCR from CSF, nl CSF count/ positive mice subinoculation/ w marked clinical radiographic and laboratory improvement after 4 ds of anti- Toxoplasma treatment Pyrimethamine/Sulfadiazine/ Steroids (after treatment CD4 increased from 435 to 921 /mm3)//ABSTRACT: Pulmonary toxoplasmosis is rare in immunocompetent subjects. Here, we describe a 41-year-old previously healthy male patient who presented to the emergency department of a hospital with a life-threatening case of pneumonia due to Toxoplasma gondii infection, which responded to specific therapy. Clinical and image-based findings overlap with those for atypical pneumonias, and toxoplasmosis should be considered in the differential diagnosis—especially if immunoglobulin M–specific antibodies are detected. |
| Mariani 2006 | ABSTRACT: We report a case of toxoplasma myocarditis in a young healthy man.///Patient had 2 Toxoplasmosis manifestations: myocardial involvement with complete AV block and cerebral lesions. This patient is the second AV block case related to toxoplasma infection described in the literature. |
| De Salvador 2005 | ABSTRACT: We report a case of severe acute primary pulmonary toxoplasmosis in an immunocompetent young man living in Nice (Southern France). The Toxoplasma DNA extracted from the broncho-alveolar lavage fluid allowed a genetic characterization of the responsible strain which displayed an atypical genotype of Toxoplasma gondii. This unusual genetic composition of the parasite may have influenced, among other factors, the severity of the disease.///The 11-yr-old sister of the patient also developed Acute toxoplasmosis with fever and LADP, but without pulmonary findings//Thus for the severity of the presentation the atypical implicated T.gondii genotype might not be solely responsible. //A massive parasite load in the 19-yr-old pt might have overwhelmed the immune response and led to a severe toxoplasmosis. //In such cluster cases differences in inoculum size are more likely explained by ingestion of oocysts rather than ingestions of cysts in infected meat |
| Kaushik 2005 | Meningoencephalitis//in a 28-yr-old immunocompetent F from India (HIV negative x2) with 2 mo Hx of low grade fever, Headache and vomiting; with worsening headache and deterioration of level of consciousness, confusion, irritability, neck rigidity and hepatomegaly//Spinal tap showed elevated opening pressure; Pleocytosis (495 cells/mm3); elevated CSF protein 210 mg/dl(unl < 50 mg/dl) and low CSF glucose (24 mg/dl)//Head CT showed multiple ring lesions with hypointensive centre and moderate hydrocephalus, with meningeal enhancement ///T2 weighted images showed moderate dilatation of the lateral, third and fourth ventricles with periventricular hyperintensity, and multiple widely scattered ring lesions with a hypointense centre and a peripheral hyperintense rim in both the cerebral hemispheres including the thalamus and basal ganglia. Lesions were also visualized in the pons, middle cerebellar peduncles and both the cerebellar hemispheres. The majority of these lesions was associated with perifocal edema//Patient was initially started on anti-TB therapy+ steroids for suspected TB meningoencephalitis with multiple tuberculomas)///After 10 ds Brain MRI T1 images showed isointense to Hyperintense exudate in the supra-cellar cistern///Repeat CSF analysis showed decrease in pleocytosis (from 495 to 250 cells/mm3; probably due to the Steroid treatment); increase in CSF protein (From 210 to 440 mg/dl) and increase in CSF glucose (From 24 to 60 mg/dl); probably due to steroids//Failure to respond to anti-TB treatment led to the suspicion of Toxoplasmosis///Toxoplasma IgG was high positive (1294 IU.ml; cutoff < 15 IU/mL) and positive Toxoplasma IgM (1.48; cutoff <1.1 AI)//Patient was started on TMP/SMX x 6 weeks; with rapid initiation of clinical improvement within 3 ds of TMP/SMX; with gradual disappearance of fever and headache over 2–3 weeks///Repeat spinal tap after 3 weeks of anti- Toxoplasma treatment showed normalization of opening pressure and CSF cell country//Repeat brain MRI after 6 wks showed regression in size of all lesions; Some of these lesions appeared as foci of hypointense signals on the T2 weighted images, which accentuated on the T2 images, consistent with calcification. ///(Absence of LADP make this presentation rare) |
| Bossi 2002 | Disseminated toxoplasmosis,//30-yr-old immunocompetent (HIV negative) man from French Guiana, who presented with a 3 wk Hx of fever, cough, rash, myalgia, myositis, diffuse LADP, HA, confusion (Risk eating undercooked boar meat); with with b/l interstitial infiltrates and b/l pleural and pericardial effusions, HSM, transaminitis and pancreatitis//Chest CT bilateral interstitial infiltrates with b/l pleural and pericardial effusions//Once ABX switched to Spiramycin, his respiratory symptoms and pericarditis improved within 5 ds//CD4 = 332// Toxoplasma IgG and IgM highly positive titers//Muscle Biopsy showed T.gondii cysts and tachyzoites// treated with Pyrimethamine + Sulfadiazine (x 6 wks) and condition improved; defervested within 5 ds and muscle symptoms resolved within 15 ds//F/up 1 year later was asymptomatic. |
| Vastava 2002 | Toxoplasma encephalitis//in a 22-yr-old immunocompetent man (HIV negative) from India, who presented with fever, HA, left sided weakness and gradual LOC (loss of consciousness), with Left hemiparesis//CSF with mild pleocytosis and high protein (112 mg/dl)//High Toxoplasma IgG in blood and CSF//Brain MRI: w large hemorrhagic lesion in R parietal region with perifocal edema and mass effect//Multiple lesions with High T2 signal, with multiple nodular and linear enhancing lesions//Started Pyrimethamine + Sulfadiazine w marked clinical improvement within 2 weeks; f/up MRI 4 wks later showed regression of the lesions//6 mo f/up MRI with almost complete regression of the lesions// |
| Vastava 2002 | Toxoplasma encephalitis//in a 35-yr-old immunocompetent man (HIV negative) from India, with a 15 ds Hx of ALOC; who presented with severe throbbing headache, sudden onset of vomiting and low grade fever//Brain MRI showed multiple high T2 signal lesions in both hemispheres, with linear radiation and nodular contrast enhancement //Started empirically Pyrimethamine + Sulfadiazine, with marked clinical improvement within 1 week//f/up MRI after 2 weeks showed regression of the lesions and 6 mo f/up MRI showed only small residual lesions with no contrast enhancement |
| Paspalaki 2001 | Polymyositis and myocarditis (severe proximal muscle weakness, elevated muscle enzymes, positive EMG consistent with subacute inflammatory myopathy; ECHO: dilation of Left ventricle w poor contractility suggestive of myocardial involvement)//////(13-yr-old immunocompetent girl with 3 wk hx of high fevers, malaise, mild proximal muscle weakness, weight loos, and vomiting; transaminitis, and a round 2 cm non cystic liver lesion by abdominal US and CT//initially presumed to have bacterial liver abscess; with rapid neurologic deterioration with dysphagia, inability to walk and raise arms, further weight loss, fine tremor of hands, maculopapular rash on palms and soles; with EMG consistent with subacute inflammatory myopathy//with ECHO showing left ventricle dilation with poor contractility///With rising and eventually very high Toxoplasma IgG titers (up to 1:109,350 4 weeks later prior to any Tx/steroids) and positive Toxoplasma IgM)//Had favorable response to steroids only treatment; with resolution of fever within 2 wks; and improvement of clinical and laboratory findings; with resolution of rash on palms and resolved within 3 months//Authors’ presumed diagnosis with Toxoplasmic acute myositis and myocarditis; the liver lesion might also be attributed to Toxoplasmosis//The improvement with prednisolone along was suggestive of immunologic disturbances contributing to the development of inflammatory myositis//With patient remaining completely asymptomatic at the 4 yr f/up) |
| Silva 2001 | 46-yr-old immunocompetent woman (HIV negative) from Brazil; presented with fainting and decreased visual acuity x 8 ds, and inability to perform usual tasks as housewife (with hx of partial seizures due to intracranial calcifications secondary to neruocysticercosis)//with Paresis of Left upper limb; Head CT showed hypodense lesion with vasogenic edema in the R occipital lobe, with heterogeneous contrast uptake around the lesion//MRI revealed an occipital lobe mass measuring 3.5 × 2.9 × 3 cm with perilesional edema and areas of high signal on T1 and T2//Underwent neurosurgical exploration due to concern for CNS neoplasm; and complete surgical excision of two nodular lesions with a yellowish-brown appearance with areas of central necrosis and cavitation; revealing chronic inflammation surrounding the necrotic material; with pseudocysts filled with bradyzoites seen in immunostaining for T.gondii//Toxoplasma IgG was positive but negative Toxoplasma IgM// diagnosis of Brain abscess due to Toxoplasmosis was made ///it was not possible to define whether there was a RLI triggered by an unidentified immunosuppressive factor, or an API with negative IgM in the serum// treatment with P/S was initiated with progressive improvement of initial neurological s/s//At f/up 6 months after diagnosis (without any treatment) reported only hypoesthesia in the feet and NO evidence of immunosuppression 1 year after diagnosis |
| Sugane 2001 | Meningoencephalitis (preceding headache x 2 wks ( associated with high fever and urinary retention)//subsequently facial numbness, gait disturbances progressing to extreme unsteadiness, delirium, positive Kernig’s sign ABSTRACT: We report herein a rare case of Toxoplasma gondii meningoencephalitis in a non-AIDS patient. Although T. gondii itself was not detected in nucleated cells in peripheral blood and cerebrospinal fluid under the microscope, the polymerase chain reaction method effectively detected the B1 gene of T. gondii in the cells. A serological examination showed increased levels of the IgG but not the IgM antibody to T. gondii, suggesting reactivation of the infection in the brain. |
| Chandenier 2000 | Acute myocarditis with rapid onset of CHF (congestive heart failure) shortly after acute infection//in a 21-yr-old immunocompetent woman (HIV negative) living in France, who was admitted in the Cardiac ICU with chest pain with deep inspirations, fever and dyspnea.//ECHO showed global hypokinesia with SF 17% (nl range 30–35%) and EF 36% (nl range 60%) but no pericardial effusion; High CPK, LDH, transaminitis, elevated inflammatory markers//Serial Toxoplasma serology was positive for Toxoplasma IgG, IgM and IgA, confirming recent seroconversion (rising Toxoplasma IgG titers))///CHF and myocardial contractility self-normalized within 8 ds, NO anti- Toxoplasma treatment was given; (in HD12 suffered bilateral Pulmonary Emboli and recovered ONLY with anti-coagulation treatment) |
| Chandenier 2000 | Cardiac dysfunction, dyspnea, pulmonary edema, transaminitis//in a 9-yr-old immunocompetent girl (HIV negative) living in France, who presented with Acute Pulmonary Edema, Dyspnea and Tachycardia, with 1 wk prior having had fever and dyspnea for which treated with Amoxicillin (fever subsided by dyspnea worsened)//CXR showed Pulmonary edema and cardiomegaly //ECHO showed systolic Left ventricular dysfunction with akinetic basal and median septum and hypokinesia of other ventricular walls//SF 10% (nl 30–35%) and EF 35% (nl 60%)//Cardiac enzymes were normal (CPK, LDH, troponin and Myoglobin), transaminitis//Her clinical condition improved on symptomatic treatment //Toxoplasma serology showed positive Toxoplasma IgG, IgM and IgA, Blood Toxoplasma PCR was negative, but Toxoplasma IgG avidity and Agglutination test implied an infection acquired 6–12 mo prior to testing//(Risk factor: contact with kittens 3 mo prior) //Pyrimethamine + Sulfadiazine given later (x 4 wks) led to improvement in cardiac function//(at 6 mo f/up the cardiac function was completely normal) |
| Sanchez 2000 | Toxoplasmic encephalitis //in a 61-yr-old immunocompetent male from Recurrent seizures within an 8 mo period (2 episodes 8 mo prior and 1 current episode); multiple nodular brain calcifications along the convexity, paracortical regions and brain base; otherwise normal CSF analysis (normal cells, protein and glucose), +Toxoplasma IgG, +IgM, +IgA but high avidity at the time of the 3d seizure episode.///Seizures resolved -with not recurrence over subsequent 6 months-without specific anti- Toxoplasma treatment. |
| Sano 2000 | ABSTRACT: There have been several case reports, a total of 22 up to the present, of toxoplasma pericarditis. Out of them, in only a few cases the diagnosis was properly made with a proof of the microscopic presence of Toxoplasma gondii. This is the first report of toxoplasma pericarditis in which the presence of Toxoplasma gondii was detected by polymerase chain reaction of pericardial effusion. In addition, the previous reports will be reviewed, and compared to this present case. A 29 yr-old woman, without immunosuppressant disorder, suffering from fever and orthopnea was admitted to our hospital. Blood chemistry findings indicated mild liver dysfunction and inflammation. Chest radiography showed cardiac enlargement. Electrocardiography showed sinus tachycardia and ST elevation. Echocardiography revealed a massive pericardial effusion. Pericardiocentesis demonstrated 638 mL of bloody fluid. Cytologic study of the fluid was class II for malignancy, and polymerase chain reaction to tuberculosis was negative. However, a high titer of the anti- toxoplasma antibody of 1: 20,480 (passive hemagglutination) indicated pericarditis caused by Toxoplasma gondii. Subsequently, Toxoplasma gondii was identified in the pericardial effusion by polymerase chain reaction. Clinical symptoms improved after pericardiocentesis, but 2 months later pericarditis recurred. Treatment was started with 800 mg acetylspiramycin daily but failed to improve the symptoms. Because of the development of pleuritis, treatment was changed to sulfadoxine 1000 mg/pyrimethamine 50 mg. After the treatment with them, her symptoms improved. Only 22 cases of toxoplasma pericarditis have been reported worldwide and 15 of those cases were without immunosuppressant disorder. The usual symptoms at the onset of pericarditis without immunosuppressant disorder are fever, dyspnea and chest pain. Seven patients developed cardiac tamponade. Pericardiocentesis was performed in 8 cases and the pericardial fluid was hemorrhagic in 6. Pericardial thickening was detected in 5 cases. The diagnosis of toxoplasma infection is very difficult, because asymptomatic infection of Toxoplasma gondii is very common. Pericarditis is a disease difficult to confirm the etiology. Detection of Toxoplasma gondii in pericardial effusion by the polymerase chain reaction is very useful for its diagnosis. |
| Calore 2000 | ABSTRACT: Skeletal muscle can be the site of inflammatory diseases that lead to muscle weakness, pain, and increased myogenic serum enzymes. Most of these inflammatory myopathies are idiopathic. In some cases, inflammatory myopathies are due to infectious agents. We describe the pathological aspects of muscle biopsies of 2 Brazilian siblings who acquired toxoplasmosis at the same time and in similar conditions. One developed a tetraplegia that was confirmed to be due to inflammatory myositis due to toxoplasma. The other developed myocarditis, with heart failure, without skeletal muscle weakness. In both cases many toxoplasma organisms were observed in the muscle biopsies, but in case 1 only was there an inflammatory myopathy with myofiber necrosis; the inflammatory cells were predominantly macrophages with some CD4+ cells and rare CD20+ cells. In case 1, expression of CD54 was observed in many inflammatory cells as well in endothelial cells, but only in endothelial cells in case 2. After treatment with clindamycin and corticosteroids both cases had only partial improvement, case 1 with a residual muscle weakness and case 2 with residual cardiac insufficiency (requiring digoxin). These cases show that the presence of the parasite in myofibers is not enough to induce an inflammatory myositis with muscle cell necrosis. This suggests that immunological disturbances may contribute to the development of inflammatory myositis due to toxoplasma. |
| Bossi 1998 | ABSTRACT: Cases of severe toxoplasmosis have been reported involving immunocompetent patients living in French Guyana, where oocysts are found in river water and wild animals (2). A poor host adaptation to the uncommon highly virulent tropical strains of T. gondii can explain these unusual clinical presentations. In our case, Guillain-Barre’ syndrome was observed in an immunocompetent patient during a disseminated infection with a new strain of T. gondii. This strain was highly virulent, as confirmed by the rapid death of the mice (within 3 days). Moreover, this strain was not altered by a 10-day treatment with spiramycin (which is ineffective in toxoplasmosis with central nervous system symptoms), and parasitemia remained after this therapy. The combination of Guillain-Barre´ syndrome, massive alteration of the patient’s condition, and skin, pulmonary, liver, pancreatic, and ocular involvement is unique for toxoplasmosis. Only the standard treatment for toxoplasmosis was effective, whereas spiramycin and intravenous IGs were ineffective.//His symptoms started 2 mo PTA= 15 ds after eating undercooked meat of warthog and doe during a 3 ds tour in the tropical forest of French Guyana (fever, HA, maculopapular rash, dry cough, diarrhea//1 mo later admitted with high fever 15 Kg weight loss) |
| Darde 1998 | 35-yr-old immunocompetent (HIV negative) military man, presented with malaise, fever, chills, myalgias, HD, B/ conjunctivitis, maculopapular rash and leukopenia after a 4 mo stay in deep forest of French Guyana, HD13 developed LADP, transaminitis, HD15 diarrhea and rales in both lungs//Numerous T.gondii trophozoites detected in BAL//Mice subinoculation positive, High Positive Toxoplasma IgG, IgM IgA, IgE//transiently low CD4 count = 344/μL//During same period 4 other military personnel returning from French Guyan became sick; ABSTRACT: Disseminated toxoplasmosis with lung involvement is rare in immunocompetent patients. We describe a case with unusual epidemiological aspects associated with a new strain genotype. The unusually severe manifestations in the case we describe could be explained by poor host adaptation to this uncommon parasite strain. |
| Rosch 1998 | Encephalitis, abnormal EEG, hearing loss//in a 9-yr-old immunocompetent boy from Germany who presented with 1week Hx of low-grade fever, headache and clinical signs of encephalitis and unilateral deafness; Anti-Toxoplasma treatment with P/S lead to the rapid disappearance of most of the signs and symptoms except for the deafness that persisted (Article in German, only English Abstract) |
| Iniguez 1997 | Miller-Fisher syndrome (ataxia, ophthalmoplegia and areflexia) / in a 30 Yr old immunocompetent patient who presented with Miller-Fisher syndrome with central and peripheral neural involvement, and diplopia with acute Toxoplasmosis |
| Montoya 1997 | Acute toxoplasmosis with skeletal muscle and myocardial involvement and CHF, S/P cardiac arrest and Seizures//ABSTRACT: We report the first case of biopsy-proven toxoplasmic myocarditis and polymyositis simultaneously occurring in the same individual that was diagnosed during life. Results of her toxoplasmic serology were consistent with acute toxoplasmosis. She subsequently developed visual symptoms consistent with toxoplasmic chorioretinitis. She had a positive clinical response to therapeutic agents specific against Toxoplasma gondii. Her toxoplasmic serological profile established the diagnosis of acute toxoplasmosis////(1 mo PTA fever and URI symptoms, 2 wks PTA flu vaccination; subsequently developed myalgias, HA, LADP, exertional dyspnea, orthopnea//admitted with acute onset of CHF (EF 30%; hypokinesia, mitral regurgitation, Myocardial Bx: showed myocarditis of unknown etiology)//Initially treated with steroids for presumed viral myocarditis and her symptoms gradually resolved///During steroid tapering developed proximal muscle weakness and Muscle Biopsy showed multiple T. gondii cysts (ECHO at that time EF 60%) Started treatment with Pyrimethamine/Sulfadiazine and Prednisone was reinstituted//////2 mo later developed progressive dyspnea and signs of CHF////Followed by Progressive sinus bradycardia and complete Heart Block associated with seizures and respiratory failure, Hypoxia//required inotropes, CSF was normal, CXR worsening CHF (at that time transferred to Stanford); had hyponatremia, transaminitis, CXR showed B/L interstitial and mild alveolar airspace changes in the RLL and Left retrocardiac region with small b/l effusions (at that time blood PC and mice sub-inocculation were negative)/////subsequently developed visual symptoms consistent with toxo chorioretinitis//She responded to anti-Toxoplasma treatment (Pyrimethamine + Sulfadiazine + Steroids initially, then Pyrimethamine + Clindamycin + Steroids)///12 ds prior to onset of Symptoms had eaten raw beef and raw lamb, Had symptoms of myalgia/HA/LADP for 13 ds PTA |
| Couvreur 1996 | ABSTRACT: Objectives: Over a period of 13 years (1982–1995), 49 cases of acquired toxoplasmosis complicated with ocular and/or neurologic or meningeal involvement were observed in our toxoplasmosis laboratory. This series includes 43 cases of isolated ocular lesions, 3 cases of meningoencephalitis (associated with retinochoroiditis in 1 case), 1 case of meningitis with uveitis, 1 case of polyradiculoneuritis and 1 case of facial nerve palsy.Methods: The patients were aged 1 to 62 years. None had either spontaneous or iatrogenic immunodeficiency. There were two steps in the diagnosis. First congenital infection was eliminated on one or several of the following criteria: any possibility of maternal infection during pregnancy ruled out in 26 cases, evidence of recent acquired infection (i.e., clinical and/or serological evidence of recent acquired toxoplasmosis in 17 cases, retinochoroiditis in non-twin siblings in 3 cases). The second step was to confirm the diagnosis of toxoplasma infection. Apart from serological evidence of recent infection, confirmation included specific local antibody synthesis in the aqueous humor of the eye and/or in cerebro-spinal fluid or ocular lesions characteristic of toxoplasmosis and absence of other etiology.Results: Ocular lesions were unilateral in 43 cases among 45. A mean follow-up of 37.9 months revealed relapses in 14 among 36 patients (39%). As routine serological examination for toxoplasmosis is compulsory in France since 1978, it was possible to document retrospectively the immune status of the mothers of many of the patients of the present series during pregnancy and to rule out congenital toxoplasmosis in a number of cases. This might explain the discrepancy between the relatively large number of cases in the present series and the fact that complicated acquired toxoplasmosis has been considered hitherto as relatively rare in immunocompetent patients.Conclusion: Based on the epidemiology of ocular toxoplasmosis and the data obtained here, it is suggested that the acquired pattern of ocular toxoplasmosis might be more frequent than estimated up to now. |
| Duffield 1996 | Toxoplasmic myocarditis resulting in recurrent symptomatic AV dissociation in a 25-yr-old immunocompetent patient (HIV Not performed, but was well at 1 yr f/up) presented initially w 10 ds Hx of Fever, Myalgias, lethargy that self-resolved//then 1 wk later acute unwell with hypotension, dizziness, chest tightness, EG showed AV dissociation, normal cardiac enzymes//1 mo later also LADP//Excision of LN showed Toxoplasmosis//Had new episode of Collapse again with AV dissociation, and profound hypotension, ECHO showed impaired LVF, hypotension//Responded to Dual chamber pacing///Positive Toxoplasma IgG Dye test and positive Toxoplasma IgM///After the 3d recurrence of AV block started Pyrimethamine + Spiramycin and a permanent dual chamber pacemaker was implanted//ABSTRACT: “We believe this case is unique in that Toxoplasma gondii myocarditis resulted in recurrent, symptomatic AV dissociation with interference. During each attack an identical pattern of AV dissociation was present. Resolution of hypotension and symptoms followed AV sequential pacing. The patient was not bradycardic and LV dysfunction occurred only once. Thus, AV dissociation caused hypotension. This pattern suggests that the patient was experiencing a condition similar to pacemaker syndrome, which occurs in some patients with a ventricular demand pacemaker. The severity of the condition is variable, ranging from flushing to hypotensive collapse, and is not always reproducible. There is often a delay of hours or days in the development of symptoms. The condition is thought to be mediated by several mechanisms including the activation of atrial stretch receptors during AV dissociation, causing an inappropriate reduction in peripheral resistance, and retrograde VA conduction. The latter does not occur during AV dissociation with interference. However, VA conduction is not a prerequisite for development of pacemaker syndrome”. |
| Lesenne 1996 | ABSTRACT: Acute myocarditis due to toxoplasmosis infection has been previously reported, usually in patients suffering from immuno-depression. Cardiac involvement by toxoplasmosis is rare in subjects with a normal immunological status. The authors report the case of a 16-yr-old immunocompetent (HIV negative) patient without immuno-depression with acute myocarditis caused by toxoplasmosis simulating myocardial infarction. //Patient’s symptomatology rapidly resolved//Patient had a favorable outcome without complications from the Toxoplasmic myocarditis//Toxoplasmic myocarditis in IC patients has a good prognosis//////(Acute onset of symptoms of chest pain, fever, EKG ST changes, initial diagnosis of myocarditis mimicking acute MI, had LADP, and splenomegaly, elevated CPK and MB fraction//Toxoplasma serology initially Toxoplasma IgG, IgM and IgA negative with f/up serology showing seroconversion (positive IgG, high positive IgM and IgA) Treated with Spiramycin and f/up ECHO 2 mo later was normal (also the previously abnormal scintigraphy scan was subsequently normalized) |
| Lescop 1995 | Diffuse toxoplasmic encephalitis with rapidly fatal outcome (within HD #6); Brain CT and MRI showing non-specific finding of brain swelling (Figiure 1) and cortical infarcts due to vasculitis; Spine-echo pTw: flatening of the grooves and the periencephalic cisterns; Spine-echo pT1: small haemorrhagic zone in the R parietal cortex, Spin Echo pT1: minimal enhancement after gadolinium injection (Figiure 2) |
| Micheli 1994 | ABSTRACT: We discuss the unusual presentation of acquired toxoplasmosis in a girl with severe and transient hemidystonia as a unique symptom. Serum titers of anti-toxoplasma antibodies increased whereas no specific antibody response in the CSF was observed. While symptomatic drugs were inefficacious, specific anti-toxoplasmosis therapy led to complete and permanent recovery within 2 months. ///1 d of fever 4 wks PTA for repetitive contractures of right thumb, with progressive worsening of involuntary movement and within subsequent 20 ds unable to handle objects or write//Toxo IgG serology showed significant rise in titers (CSF toxo IgG was negative)//The neurologic symptoms progressively worsened with athetoid like movements and Ballistic like hyperkinesia on the R//Eye exam, abd Brain CT and Brain MRI were all normal///treatment with symptomatic drugs (benzodiazepines etc) was not effective//When specific anti-Toxoplasma treatment with Pyrimethamine + Spiramycin+ Sulphonamides was instituted, the clinical condition progressively improved and within 2 mo the girl completely recovered; while the EEG normalized in 8 mo (of note earlier EEG showed posterior pseudoperiodic synchronous sharp waves during eye closure, 2 later EEG showed no paroxysmal activity excluding epilepsy) (the absence of CSF Toxoplasma antibodies supports the hypothesis of focal vasculitis) |
| Candolfi 1993 | Pulmonary Toxoplasmosis (Pneumonia)//in a 33-yr-old immunocompetent (HIV negative) pregnant woman from Cambodia; with a 7 d Hx of dyspnea, fever, dry cough, CXR with reticulondular opacities B/L//BAL showed T.gondii by immunoperoxidase staining//Toxoplasma IgG and IgM initially negative, but had seroconversion 2 wks later with positive Toxoplasma IgG and IgM//Was treated initially with Spiramycin (before the BAL results) and symptoms improved within 1 week; subsequently given Pyrimethamine/Sulfadiazine x 5 wks (until delivery)//Initially had low CD4 count (CD4: 250) which normalized after anti- Toxoplasma treatment |
| Desguerre 1993 | Acute respiratory distress with interstitial pneumonia, myocarditis and pericardial effusion and subsequently also meningoencephalitis //in a 2 yr old immunocompetent child (HIV negative) living in Guyana, who presented with respiratory distress, fever; pericardial fluid was drained//Subsequently within 1 mo developed also spastic quadriparesis and chorioretinitis; with emotional liability and limited expressive language; nystagmus//Toxoplasma IgG and IgM positive///Treated with Fansidar + Spiramycin but without response///Elevated CSF protein (100mg/dl) without pleocytosis initially, but subsequently developed pleocytosis (CSF WBC 47/mm3,high CSF protein (80 mg/dl) and positive CSF Toxoplasma IgG and Toxoplasma IgM (this, along with the presentation with acute pneumonia and myocarditis, argues against a case of congenital Toxoplasmosis and favored the diagnosis of acquired toxoplasmosis)//Brain CT: w numerous calcifications and Hypodense areas//Brain MRI with high T2 signal in periventricular white matter, internal capsule, and “centres semi-ovales”//Treated with 6 weeks of P/S (Fansidar) with stabilization of the diseases and then placed in maintenance treatment with weekly Fansidar x 2 years//At 2 years f/up: has persistent asymetric tetraparesis and had 2 seizures and the previously noted MRI white matter increased signals in the periventricular area and internal capsule had persisted but had decreased in intensity |
| Guerot 1992 | Pericarditis//in a 20 yr-old immunocompetent man living in France (HIV negative) who presented with fever and LADP, Toxoplasma IgG and IgM were positive///treated with Spiramycin x 8 ds with resolution of fever, that subsequently relapses with onset of new chest pain suggestive of pericarditis, w characteristic EKG findings and cardiomegaly on CXR //ECHO showed a large pericardial effusion without cardiac tamponade///Cardiac symptoms persisted with anti-inflammatory treatment x 10 ds and then Pyrimethamine/Sulfadiazine was given, with rapid resolution of clinical symptoms and pericardial fluid///At 3 months of f/up patient remained well |
| Lyngberg 1992 | Severe exudative pericarditis w cardiac tamponade in a F patient with SLE like musculoskeletal symptoms for the 8 preceding months; with relapsing pericarditis despite 2 anti-Toxoplasma treatment courses with Pyrimethamine/Sulfadiazine (x 3 wks and 7 wks respectively)//61-yr-old immunocompetent woman (HIV negative) from Denmark who presented with SLE like symptoms (synovitis R knee, bursitis, finger stiffness and generalized malaise, myalgias, and weight loss (not responding to 8 months treatment with NSAIDS and Sulfasalazine)///Toxoplasmosis reactivation was suspected based on high Toxoplasma IgG, Toxoplasma IgM Negative// treatment with pyrimethamine/Sulfadiazine given x 3 wks//1 wk after the end of the anti- Toxoplasma treatment there was relapse with worsening clinical symptoms, dyspnea, pericarditis symptoms (patient refused further treatment) and pericarditis progressed to cardiac tamponade; Cardiomegaly in CXR and pericarditis EKG findings//ECHO showed severe exudative pericarditis with normal myocardium//Pericardial fluid was Toxoplasma POSITIVE (Mice sub-inoculation with pericardial fluid was positive and mice died from Toxoplasmosis)///Pericardiocentesis showed marked leukocytosis// treated with Pyrimethamine/Sulfadiazine + Prednisone (after the cardiac tamponade had already occurred) x 7 weeks and cardiac symptoms gradual resolved////2 months after the 7 wks anti-Toxoplasma treatment there was another relapse of Symptoms that was treated again with anti-Toxoplasma treatment x 4 wks of P/S and clinical condition improved again with resolution of the SLE like symptoms and decrease in the ANA//Patient remained well at 9 months follow up. (diagnosis in patients with Rheumatic mimicking disease may be delayed, and false positive Toxoplasma IgG and IgM results in patients with ANA antibodies have been described. Patients with SLE should be screened for Toxoplasmosis) |
| Shimoni 1989 | Pneumonitis with pulmonary infiltrate in right upper lobe//in a 51-yr-old immunocompetent man (HIV negative) living in Israel with inactive RA + (treated only with indomethacin, without any steroids or immunosuppressive medications), who presented with a 2 wk Hx of generalized LADP and RUL pneumonia, not responding to Amoxicillin//Toxoplasma Dye test positive and Toxoplasma IgM positive//His general condition otherwise was excellent//Was D/C home on TMP/SMX and at 2 mo f/up was clinically asymptomatic, with resolution of CXR findings//At 1 yr f/up patient continued to remain healthy |
| Rafiqul Islam 1989 | FUO (low grade Fever 100–1011) and malaise x 5 months and lymphadenopathy///(in a 17-yr-old immunocompetent male from Bangladesh//with 5 months of FUO, malaise and generalized LADP, thrombocytopenia //Strongly positive Latex Agglutination test for Toxoplasmosis (no known risk factors for toxoplasmosis)//LN biopsy suggestive of toxoplasmic lymphadenitis//With Response to anti-Toxoplasma treatment (P/S x4 wks) with resolution of fever and disappearance of LADP)//(not known risk factors for toxoplasmosis reported) |
| Oseroff 1988 | Fever, polymyositis, myocarditis, hepatitis, nephrotic syndrome and transaminitis//in a 48-yr-old woman with high fever (that lasted x 6 weeks), dyspnea, generalized myalgias, muscle weakness, N/V/D and pitting edema in extremities; with leukocytosis (WBC = 35K); eosinophilia (548--> 1500/mm3), transaminitis, Elevated CPK, with high MB fraction, elevated LDH and elevated inflammatory markers (ESR = 70 mmHg)///Subsequently developed non cardiogenic pulmonary edema (with large proteinuria) requiring IMV//Fever persisted x 6 weeks; Chest CT and Gallium scan were normal////Toxoplasma serology showed rising Toxoplasma IgG titers over a 3 month period//By the time the Toxoplasmosis diagnosis was made, patient was already clinically improving with just supportive care and NO anti-Toxoplasma treatment //No anti-Toxoplasma treatment was given//At 2 mo after D/C clinically asymptomatic |
| McCabe, Remington 1987 | Transient R lung pneumonia with pleural effusion at the onset of the illness; with persistence of fever, LAPD and HSM for 7 months///in a 32 yr-old woman, missionary in the jungles of Venezuela, who presented with fevers, chills, malaise, myalgias, headaches and anorexia not responding to malaria treatment ///generalized LADP and HSM present//Transient R pneumonia with pleural effusion detected///ON HD45 subinocculation to mice of LN biopsy tissue was positive for Toxoplasmosis //Toxoplasma serology consistent with acute acquired Toxoplasmosis infection with high positive IgG and IgM //5 family members were also Toxoplasma positive |
| Cottrell 1986 | Encephalitis//in a 4-yr-old immunocompetent boy, living in England, with a 3 week Hx of recurrent generalized seizures, increasing in frequency and ataxia, tremor, dysarthria//Brain CT and CSF were normal; EEG showed seizure activity/ Toxoplasma IgG was positive and “subsequently” Toxoplasma IgM also became positive//Before the Toxoplasmosis results were available, child was started on Steroids and Phenobarbital with dramatic decrease in seizures and ataxia within 3 ds////At steroid tapering there was recurrence of seizures and ataxia and had continuous myoclonic jerks and was drowsy///Once Toxoplasma results became available started on Pyrimethamine/Sulfadimidine (x6 mo) with improvement within the first 2 wks of anti- Toxoplasma treatment, and then rapidly returned to normal; although some myoclonic seizures persisted until clonazepam was added///After d/c of anti- Toxoplasma treatment after 6 mo he remained well, and EEG showed improvement although some R sided predominance remained//// |
| Michel 1986 | Acute pulmonary toxoplasmosis//in a 21-yr-old immunocompetent Portuguese man living in Belgium, who presented w high fever, shivers, dry cough, myalgia, arthralgia and rash (duration not given); cervical LADP, b/l lung crackles, hepatomegaly//CXR: b/l interstitial infiltrates//Hypoxia (PaO2 52 mmHg); elevated LDH and CPK//PFTS with mild restrictive patterns//BAL with excess lymphocytes///Patient responded to treatment with Erythromycin and after 10 ds of treatment with resolution of fever and hypoxia and normalization of CXR.//With rising and highly positive Toxoplasma IgG and IgM serology (with Toxoplasma IgG from 1:1000 to 1:4000 and Toxoplasma IgM from 1/320 to 1/12(x 3 mo)//after 3 mo of anti- Toxoplasma treatment there was normalization of the initially low OKT4 counts and initially high OKT8 counts (before treatment OKT4: 357 & OKT8: 2589 58%; after treatment OKT4: 765 & OKT8 1135 cells/mL 43%) |
| N (%) | |
|---|---|
| Articles | 36 |
| Cases | 46 |
| Top countries of cases (imputed when not reported by the country of authors) | |
| USA | 16 (28%) |
| Ireland | 6 (13%) |
| France | 4 (13%) |
| Switzerland | 3 (7%) |
| N of cases per article | |
| 22 | 1/36 (3%) |
| 11 | 1/36 (3%) |
| 6 | 2/36 (6%) |
| 3 | 1/36 (3%) |
| 2 | 8/36 (22%) |
| 1 | 23/36 (64%) |
| Age | |
| Adult | 28 (61%) |
| Pediatric | 13 (28%) |
| Not reported | 5 (11%) |
| Manifestations | |
| Pulmonary | 8/46 (17%) |
| CNS | 12/46 (26%) |
| Cardiac | 16/46 (35%) |
| Disseminated | 6/46 (13%) |
| Prolonged duration (myositis, renal, other) > 3 months | 4/46 (9%) |
| 1. Adams EM, Hafez GR, Carnes M, Wiesner JK, Graziano FM. The development of polymyositis in a patient with toxoplasmosis: clinical and pathologic findings and review of literature. Clin Exp Rheumatol. 1984 Jul-Sep;2(3):205-8. PMID: 6529871. |
| 2. Amato Neto V. Caso fatal de pneumonia intersticial toxoplasmótica [A fatal case of interstitial pneumonia due to toxoplasmosis]. Rev Inst Med Trop Sao Paulo. 1969 Sep-Oct;11(5):377-81. Spanish. PMID: 5356133. |
| 3. Armstrong C, Macmurray FG. Toxoplasmosis found by recovery of toxoplasma gondii from excised maxillary gland. J Am Med Assoc. 1953 Mar 28;151(13):1103-4. doi: 10.1001/jama.1953.02940130049009a. PMID: 13034439. |
| 4. Arribada A, Escobar E. Cardiomyopathies produced by Toxoplasma gondii. Am Heart J. 1968 Sep;76(3):329-39. doi: 10.1016/0002-8703(68)90227-5. PMID: 4951330. |
| 5. Bach MC, Armstrong RM. Acute toxoplasmic encephalitis in a normal adult. Arch Neurol. 1983 Sep;40(9):596-7. doi: 10.1001/archneur.1983.04050080096025. PMID: 6604513. |
| 6. Collart F, Glupzinski Y, Cogan E, Schmerber J: Acute pericarditis of toxoplasmic origin. J Infect 1983; 7: 82-83 |
| 7. Cunningham T: Pancreatitis in acute toxoplasmosis. Am J Clin Pathol 1982; 78: 403-405 |
| 8. Doffoel M, Coumaros D, Levy P, Jacques C, Saada K, Laidoudi A, Bockel R, Himy-Dahan R, Kien T. Neurotoxoplasmose. A propos d’un cas de méningo-encéphalite acquise [Neurotoxoplasmosis. Description of a case of an acquired meningo-encephalitis (author’s transl)]. Sem Hop. 1980 Apr 18-25;56(15-16):788-90. French. PMID: 6246619. |
| 9. Espersen E. Toxoplasmosis; a survey and a case of acquired pulmonary toxoplasmosis. Acta Tuberc Scand. 1957;34(3-4):163-72. PMID: 13520397. |
| 10. Guignard JP, Torrado A. Interstital nephritis and toxoplasmosis in a 10-year-old child. J Pediatr. 1974 Sep;85(3):381-2. doi: 10.1016/s0022-3476(74)80123-x. PMID: 4610420. |
| 11. Guimares FN: Toxoplasmose humana: meningoencefalomielite toxoplasmica: ocorrencia em adulto e em recemnascido. Mem Inst Oswaldo Cruz 1943; 38: 257-320 (in Portugese) |
| 12. Hafstrom T. Toxoplasmic encephalopathy: a form of meningo-encephalomyelitis in adult toxoplasmosis. Acta Psychiatr Scand. 1959;34(3):311-21. doi: 10.1111/j.1600-0447.1959.tb07581.x. PMID: 14398759. |
| 13. Hakkila J, Frick HM, Halonen PI: Pericarditis and myocarditis caused by toxoplasma: Report of a case and review of the literature. Am Heart J 1958; 55: 758 - 766 |
| 14. Israel J, Baufine-Ducrocq H: Les Pericardites aigues d’origine toxoplasmique. Coeur Med Interne 1969; 8: 47-54 (in French) |
| 15. Jones TC, Kean BH, Kimball AC: Pericarditis associated with toxoplasmosis. Ann Intern Med 1965: 62:786-790 |
| 16. Kass EH, Andrus SB, Adams RD, Turner FC, Feldman HA. Toxoplasmosis in the human adult. AMA Arch Intern Med. 1952 May;89(5):759-82. doi: 10.1001/archinte.1952.00240050073006. PMID: 14914215. |
| 17. Leak D, Meghji M: Toxoplasmic infection in cardiac disease. Am J Cardiol 1979; 43: 841-849 |
| 18. Ludlam GB, Beattie CP, Pulmonary Toxoplasmosis? Lancet. 1963 Nov 30;2(7318):1136-8. doi: 10.1016/s0140-6736(63)90789-x. PMID: 14072910. |
| 19. Mary AS, Hamilton M. Ventricular tachycardia in a patient with toxoplasmosis. Br Heart J. 1973 Mar;35(3):349-52. doi: 10.1136/hrt.35.3.349. PMID: 4692665; PMCID: PMC458615. |
| 20. Mirada A, Rubies-Prat J, Cerda E, Foz M: Pericarditis associated to acquired toxoplasmosis in a child. Cardiology 1976; 61: 303-306 |
| 21. Mishra DN, Gupta RC, Atal PR, Shukla SP. Toxoplasmosis in an adult presenting as paraparesis (a case report). J Assoc Physicians India. 1975 Nov;23(11):779-81. PMID: 1223077. |
| 22. Nagaratnam N, Stephen SJ: Chronic constrictive pericarditis associated with toxoplasmosis. Br Heart J 1973; 35: 868-870 |
| 23. Niutta R, Fatigante R. Miliare polmonare da toxoplasma gondii in adulto [Pulmonary miliaria caused by Toxoplasma gondii in an adult]. Minerva Med. 1978 Sep 1;69(40):2717-22. Italian. PMID: 714266. |
| 24. Alam M, Duvernoy WFC, Quinn EL, Fisher EJ. Congestive cardiomyopathy as an end stage of Toxoplasma myocarditis. Henry Ford Hospital Medical Journal 1975: Vol. 23: No. 3, 141-144. Available at: https://scholarlycommons.henryford.com/hfhmedjournal/vol23/iss3/6. |
| 25. Pinkerton, H., and Henderson, R.G. Adult toxoplasmosis; previously unrecognized disease entity simulating typhug-spotted fever group F. Am. M. Ass., 1941, 116, 807-814 |
| 26. Prado S, Pacheco V, Noemi I, Eimbcke F, Zilleruelo R, Vicuna D, Vera S, Saieh M, Jaeger H, Gomez O, Arretz C: Toxoplasma pericarditis and myocarditis. Rev Chil Pediatr 1978: 49: 179-185 (in Spanish with Eng abstr) |
| 27. Sabin AB: Toxoplasmic encephalitis in children. JAMA 116:801-807, 1941. |
| 28. Sacks JJ, Delgado DG, Lobel HO, Parker RL. Toxoplasmosis infection associated with eating undercooked venison. Am J Epidemiol. 1983 Dec;118(6):832-8. doi: 10.1093/oxfordjournals.aje.a113701. PMID: 6650484. |
| 29. Sante LR. Roentgen manifestations of adult toxoplasmosis. AmericanJournal of Roentgenology and Radium Therapy 1942;47:825-9. |
| 30. Sexton RCJr, Eyles DE, Dillman RE. Adult toxoplasmosis. Am J Med. 1953 Mar;14(3):366-77. doi: 10.1016/0002-9343(53)90047-3. PMID: 13030493. |
| 31. Stagno S, Dykes AC, Amos CS, Head RA, Juranek DD, Walls K. An outbreak of toxoplasmosis linked to cats. Pediatrics. 1980 Apr;65(4):706-12. PMID: 7189277. |
| 32. Townsend JJ, Wolinsky JS, Baringer JR, Johnson PC. Acquired toxoplasmosis. A neglected cause of treatable nervous system disease. Arch Neurol. 1975 May;32(5):335-43. doi: 10.1001/archneur.1975.00490470079012. PMID: 1094993. |
| 33. Vischer TL, Bernheim C, Engelbrecht E. Two cases of hepatitis due to Toxoplasma gondii. Lancet. 1967 Oct 28;2(7522):919-21. doi: 10.1016/s0140-6736(67)90235-8. PMID: 4167857. |
| 34. Walter J, Schwartz J, Bloch R, Schaub S: Existe-t-il une pericardite toxoplasmique? Presse Med 1964; 72: 3047-3048 (in French) |
| 35. Wilkinson EE. The radiologic aspects of toxoplasmosis. J Am Med Womens Assoc (1972). 1973 Feb;28(2):76-80. PMID: 4347594. |
References
- Pappas, G.; Roussos, N.; Falagas, M.E. Toxoplasmosis snapshots: Global status of Toxoplasma gondii seroprevalence and implications for pregnancy and congenital toxoplasmosis. Int. J. Parasitol. 2009, 39, 1385–1394. [Google Scholar] [CrossRef]
- Torgerson, P.R.; Mastroiacovo, P. The global burden of congenital toxoplasmosis: A systematic review. Bull. World Health Organ. 2013, 91, 501–508. [Google Scholar] [CrossRef]
- Undseth, O.; Gerlyng, P.; Goplen, A.K.; Holter, E.S.; von der Lippe, E.; Dunlop, O. Primary toxoplasmosis with critical illness and multi-organ failure in an immunocompetent young man. Scand. J. Infect. Dis. 2014, 46, 58–62. [Google Scholar] [CrossRef]
- Contopoulos-Ioannidis, D.G.; Cho, S.M.M.; Bertaina, A.M.; Leung, A.N.; Fischbein, N.; Lanzman, B.; Schwenk, H.T.M.; Montoya, J.G. Toxoplasmosis Among 38 751 Hematopoietic Stem-cell Transplant Recipients: A Systematic Review of Disease Prevalence and a Compilation of Imaging and Autopsy Findings. Transplantation 2021, 105, e375–e386. [Google Scholar] [CrossRef]
- Schwenk, H.T.; Khan, A.; Kohlman, K.; Bertaina, A.; Cho, S.; Montoya, J.G.; Contopoulos-Ioannidis, D.G. Toxoplasmosis in Pediatric Hematopoietic Stem Cell Transplantation Patients. Transpl. Cell. Ther. 2021, 27, 292–300. [Google Scholar] [CrossRef] [PubMed]
- Peleg, A.Y.; Husain, S.; Kwak, E.J.; Silveira, F.P.; Ndirangu, M.; Tran, J.; Shutt, K.; Shapiro, R.; Thai, N.; Abu-Elmagd, K.; et al. Opportunistic infections in 547 organ transplant recipients receiving alemtuzumab, a humanized monoclonal CD-52 antibody. Clin. Infect. Dis. 2007, 44, 204–212. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nardone, R.; Zuccoli, G.; Brigo, F.; Trinka, E.; Golaszewski, S. Cerebral toxoplasmosis following adalimumab treatment in rheumatoid arthritis. Rheumatology 2014, 53, 284. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Young, J.D.; McGwire, B.S. Infliximab and reactivation of cerebral toxoplasmosis. N. Engl. J. Med. 2005, 353, 1530–1531, Discussion-1. [Google Scholar]
- Maldonado, Y.A.; Read, J.S.; Committee On Infectious, D. Diagnosis, Treatment, and Prevention of Congenital Toxoplasmosis in the United States. Pediatrics 2017, 139, e20163860. [Google Scholar] [CrossRef] [Green Version]
- Demar, M.P.; Ajzenberg, D.; Maubon, D.; Djossou, F.; Panchoe, D.; Punwasi, W.; Valery, N.; Peneau, C.; Daigre, J.; Aznar, C.; et al. Fatal outbreak of human toxoplasmosis along the Maroni River: Epidemiological, clinical, and parasitological aspects. Clin. Infect. Dis. 2007, 45, e88–e95. [Google Scholar] [CrossRef] [Green Version]
- Demar, M.; Hommel, D.; Djossou, F.; Peneau, C.; Boukhari, R.; Louvel, D.; Bourbigot, A.-M.; Nasser, V.; Ajzenberg, D.; Darde, M.-L.; et al. Acute toxoplasmoses in immunocompetent patients hospitalized in an intensive care unit in French Guiana. Clin. Microbiol. Infect. 2012, 18, E221–E231. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bossi, P.; Paris, L.; Caumes, E.; Katlama, C.; Danis, M.; Bricaire, F. Severe acute disseminated toxoplasmosis acquired by an immunocompetent patient in French Guiana. Scand. J. Infect. Dis. 2002, 34, 311–314. [Google Scholar] [CrossRef]
- Sacks, J.J.; Delgado, D.G.; Lobel, H.O.; Parker, R.L. Toxoplasmosis infection associated with eating undercooked venison. Am. J. Epidemiol. 1983, 118, 832–838. [Google Scholar] [CrossRef] [PubMed]
- Schumacher, A.C.; Elbadawi, L.I.; DeSalvo, T.; Straily, A.; Ajzenberg, D.; Letzer, D.; Moldenhauer, E.; Handly, T.L.; Hill, D.; Dardé, M.-L.; et al. Toxoplasmosis Outbreak Associated With Toxoplasma gondii-Contaminated Venison-High Attack Rate, Unusual Clinical Presentation, and Atypical Genotype. Clin. Infect. Dis. 2021, 72, 1557–1565. [Google Scholar] [CrossRef] [PubMed]
- Bowie, W.R.; King, A.S.; Werker, D.H.; Isaac-Renton, J.L.; Bell, A.; Eng, S.B.; Marion, S.A. Outbreak of toxoplasmosis associated with municipal drinking water. The BC Toxoplasma Investigation Team. Lancet 1997, 350, 173–177. [Google Scholar] [CrossRef] [PubMed]
- Pomeroy, C.; Filice, G.A. Pulmonary toxoplasmosis: A review. Clin. Infect. Dis. 1992, 14, 863–870. [Google Scholar] [CrossRef] [PubMed]
- Leal, F.E.; Cavazzana, C.L.; de Andrade, H.F., Jr.; Galisteo, A., Jr.; de Mendonca, J.S.; Kallas, E.G. Toxoplasma gondii pneumonia in immunocompetent subjects: Case report and review. Clin. Infect. Dis. 2007, 44, e62–e66. [Google Scholar] [CrossRef] [Green Version]
- Graham, A.K.; Fong, C.; Naqvi, A.; Lu, J.Q. Toxoplasmosis of the central nervous system: Manifestations vary with immune responses. J. Neurol. Sci. 2021, 420, 117223. [Google Scholar] [CrossRef]
- Zhou, Z.; Lopez, H.I.A.O.; Perez, G.E.; Burgos, L.M.; Farina, J.M.; Saldarriaga, C.; Lopez-Santi, R.; Cotella, J.I.; Pérez, A.L.S.; Baranchuk, A. Toxoplasmosis and the Heart. Curr. Probl. Cardiol. 2021, 46, 100741. [Google Scholar] [CrossRef]
- Gallo, R.C.; Sarin, P.S.; Gelmann, E.P.; Robert-Guroff, M.; Richardson, E.; Kalyanaraman, V.S.; Mann, D.; Sidhu, G.D.; Stahl, R.E.; Zolla-Pazner, S.; et al. Isolation of human T-cell leukemia virus in acquired immune deficiency syndrome (AIDS). Science 1983, 220, 865–867. [Google Scholar] [CrossRef]
- Barre-Sinoussi, F.; Chermann, J.C.; Rey, F.; Nugeyre, M.T.; Chamaret, S.; Gruest, J.; Dauguet, C.; Axler-Blin, C.; Vezinet-Brun, F.; Rouzioux, C.; et al. Isolation of a T-lymphotropic retrovirus from a patient at risk for acquired immune deficiency syndrome (AIDS). Science 1983, 220, 868–871. [Google Scholar] [CrossRef] [Green Version]
- A Timeline of AIDS". aids.gov. U.S. Department of Health & Human Services. aids.gov staff. Available online: https://en.wikipedia.org/wiki/Timeline_of_HIV/AIDS#Pre-1980s (accessed on 26 February 2023).
- Holland, G.N. Ocular toxoplasmosis: A global reassessment. Part I: Epidemiology and course of disease. Am. J. Ophthalmol. 2003, 136, 973–988. [Google Scholar] [CrossRef] [PubMed]
- Holland, G.N. Ocular toxoplasmosis: A global reassessment. Part II: Disease manifestations and management. Am. J. Ophthalmol. 2004, 137, 1–17. [Google Scholar] [CrossRef]
- Strang, A.G.; Ferrari, R.G.; Rosário, D.K.D.; Nishi, L.; Evangelista, F.F.; Santana, P.L.; de Souza, A.H.; Mantelo, F.M.; Guilherme, A.L.F. The congenital toxoplasmosis burden in Brazil: Systematic review and meta-analysis. Acta Trop. 2020, 211, 105608. [Google Scholar] [CrossRef]
- Smit, G.S.A.; Padalko, E.; Van Acker, J.; Hens, N.; Dorny, P.; Speybroeck, N.; Devleesschauwer, B. Public Health Impact of Congenital Toxoplasmosis and Cytomegalovirus Infection in Belgium, 2013: A Systematic Review and Data Synthesis. Clin. Infect. Dis. 2017, 65, 661–668. [Google Scholar] [CrossRef] [Green Version]
- Garweg, J.G.; Kieffer, F.; Mandelbrot, L.; Peyron, F.; Wallon, M. Long-Term Outcomes in Children with Congenital Toxoplasmosis-A Systematic Review. Pathogens 2022, 11, 1187. [Google Scholar] [CrossRef] [PubMed]
- Filipowicz, A.; Coca, M.N.; Blair, B.M.; Chang, P.Y. Acute Myocarditis with Cardiogenic Shock and Multiple Organ Failure, Followed by Bilateral Panuveitis Masquerading as Endogenous Endophthalmitis, Due to Toxoplasma Gondii in an Immunocompetent Patient. Retin. Cases Brief Rep. 2021, 15, 575–580. [Google Scholar] [CrossRef] [PubMed]
- Mustafa, K.; Hillyard, J.; Nowak, E.; Slowikowski, J.; Okogbue, I.; Garner, D. Toxoplasma myocarditis: An atypical case in an immunocompetent patient. IDCases 2021, 26, e01273. [Google Scholar] [CrossRef] [PubMed]
- Montoya, J.G.; Jordan, R.; Lingamneni, S.; Berry, G.J.; Remington, J.S. Toxoplasmic myocarditis and polymyositis in patients with acute acquired toxoplasmosis diagnosed during life. Clin. Infect. Dis. 1997, 24, 676–683. [Google Scholar] [CrossRef] [Green Version]
- Oseroff, A. Toxoplasmosis associated with nephrotic syndrome in an adult. South Med. J. 1988, 81, 95–96. [Google Scholar] [CrossRef]
- Akturk, H.K.; Sotello, D.; Ameri, A.; Abuzaid, A.S.; Rivas, A.M.; Vashisht, P. Toxoplasma Infection in an Immunocompetent Host: Possible Risk of Living with Multiple Cats. Cureus 2017, 9, e1103. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Martinot, M.; Greigert, V.; Farnarier, C.; Dardé, M.L.; Piperoglou, C.; Mohseni-Zadeh, M.; Tarabeux, J.; Guffroy, A.; Villard, O.; Vely, F. Spinal cord toxoplasmosis in a young immunocompetent patient. Infection 2020, 48, 299–302. [Google Scholar] [CrossRef]
- Groh, M.; Faussart, A.; Villena, I.; Ajzenberg, D.; Carme, B.; Demar, M.; Joly, V.; Houze, S.; Simon, S.; Aubert, D.; et al. Acute lung, heart, liver, and pancreatic involvements with hyponatremia and retinochoroiditis in a 33-year-old French Guianan patient. PLoS Negl. Trop. Dis. 2012, 6, e1802. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yang, Y.; Zuo, W.; Hu, J.; Esch, G.W.; Zuo, Y. Hemophagocytic syndrome as uncommon presentation of disseminated toxoplasmosis in an immunocompetent adult from Chinese Kunming. Am. J. Trop. Med. Hyg. 2013, 88, 1209–1211. [Google Scholar] [CrossRef] [Green Version]
- Luis, E.; Pino, J.E.S.; López, M.C. Descripción de un brote epidémico de toxoplasmosis aguda en pacientes inmunocompetentes miembros de las fuerzas militares de Colombia durante operaciones de selva. Infectio 2009, 13, 83–91, ISSN 0123-9392. [Google Scholar]
- Bossi, P.; Caumes, E.; Paris, L.; Darde, M.L.; Bricaire, F. Toxoplasma gondii-associated Guillain-Barre syndrome in an immunocompetent patient. J. Clin. Microbiol. 1998, 36, 3724–3725. [Google Scholar] [CrossRef] [Green Version]
- Darde, M.L.; Villena, I.; Pinon, J.M.; Beguinot, I. Severe toxoplasmosis caused by a Toxoplasma gondii strain with a new isoenzyme type acquired in French Guyana. J. Clin. Microbiol. 1998, 36, 324. [Google Scholar] [CrossRef] [Green Version]
- Lescop, J.; Brinquin, L.; Schill, H.; Soulie, D.; Sarrazin, J.L.; Cordoliani, Y.S. [Diffuse toxoplasmic encephalitis in a non-immunosuppressed patient]. J. Radiol. 1995, 76, 21–24. [Google Scholar] [PubMed]
- Desguerre, I.; Pedespan, J.M.; Buissonniere, R.; Couvreur, J.; Ponsot, G. [Acquired cerebral toxoplasmosis in an non-immunosuppressed child]. Arch. Fr. Pediatr. 1993, 50, 339–342. [Google Scholar]
- Bousquet, A.; Bigaillon, C.; Dumitrescu, N.; Larréché, S.; Godreuil, C.; Mestiri, R.; Le Caruyer, N.; Mérens, A.; Andriamanantena, D. Acute myocarditis in an immunocompetent young man: Don’t forget Toxoplasma gondii. Int. J. Cardiol. 2016, 214, 358–359. [Google Scholar] [CrossRef]
- Nunura, J.; Vásquez, T.; Endo, S.; Salazar, D.; Rodriguez, A.; Pereyra, S.; Solis, H. Disseminated toxoplasmosis in an immunocompetent patient from Peruvian Amazon. Rev. Inst. Med. Trop. Sao Paulo 2010, 52, 107–110. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- McCabe, R.E.; Brooks, R.G.; Dorfman, R.F.; Remington, J.S. Clinical spectrum in 107 cases of toxoplasmic lymphadenopathy. Rev. Infect. Dis. 1987, 9, 754–774. [Google Scholar] [CrossRef] [PubMed]
- Henao-Martinez, A.F.; Franco-Paredes, C.; Palestine, A.G.; Montoya, J.G. Symptomatic Acute Toxoplasmosis in Returning Travelers. Open Forum. Infect. Dis. 2018, 5, ofy058. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Briand, P.Y.; Gangneux, J.P.; Favaretto, G.; Ly-Sunnaram, B.; Godard, M.; Robert-Gangneux, F.; Fest, T. [Hemophagocytic syndrome and toxoplasmic primo-infection]. Ann. Biol. Clin. 2008, 66, 199–205. [Google Scholar]
- Barbosa, C.J.D.G.; Molina, R.J.; De Souza, M.B.; Silva, A.C.A.; Micheletti, A.R.; Dos Reis, M.A.; Teixeira, V.D.P.A.; Silva-Vergara, M.L. Disseminated toxoplasmosis presenting as sepsis in two AIDS patients. Rev. Inst. Med. Trop. Sao Paulo 2007, 49, 113–116. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nelwan, E.J.; Shakinah, S.; Clarissa, G.; Hosea, F.N.; Herdanto, D.Y.; Pandelaki, J. Rare cardiac complication of toxoplasmosis in immunocompetent host. IDCases 2022, 29, e01533. [Google Scholar] [CrossRef] [PubMed]
- Chiappe Gonzalez, A.J.; Vargas Matos, I.; Massucco Revoredo, V. Acute toxoplasmosis complicated with myopericarditis and possible encephalitis in an immunocompetent patient. IDCases 2020, 20, e00772. [Google Scholar] [CrossRef]
- Candolfi, E.; de Blay, F.; Rey, D.; Christmann, D.; Treisser, A.; Pauli, G.; Kien, T. A parasitologically proven case of Toxoplasma pneumonia in an immunocompetent pregnant woman. J. Infect. 1993, 26, 79–81. [Google Scholar] [CrossRef]
- de Souza Giassi, K.; Costa, A.N.; Apanavicius, A.; Teixeira, F.B.; Fernandes, C.J.C.; Helito, A.S.; Kairalla, R.A. Tomographic findings of acute pulmonary toxoplasmosis in immunocompetent patients. BMC Pulm. Med. 2014, 14, 185. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Singhal, K.K.; Kumar, K.; Mathew, J.L.; Mewara, A.; Vaidya, P.C.; Sodhi, K.S.; Singh, M. Active toxoplasmosis presenting with polymyositis and pleural effusion in a child. J. Paediatr. Child Health 2021, 57, 1995–1997. [Google Scholar] [CrossRef]
- Michel, O.; Sergysels, R. Acute pulmonary toxoplasmosis with alveolitis of T suppressor lymphocyte type. Thorax 1986, 41, 972–973. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rostoff, P.; Mroczek-Czernecka, D.; Piwowarska, W.; Gackowski, A.; Konduracka, E.; Trzos, M.; Pasowicz, M. Elevated CA-125 level in acute heart failure due to Toxoplasma gondii perimyocarditis. Int. J. Cardiol. 2008, 130, e114–e116. [Google Scholar] [CrossRef] [PubMed]
- Cortes, A.D.; Aguirre, N. Severe disseminated acute toxoplasmosis in an adult immunocompetent patient from the Colombian Pacific. Biomedica 2018, 38, 19–23. [Google Scholar]
- De Salvador-Guillouet, F.; Ajzenberg, D.; Chaillou-Opitz, S.; Saint-Paul, M.-C.; Dunais, B.; Dellamonica, P.; Marty, P. Severe pneumonia during primary infection with an atypical strain of Toxoplasma gondii in an immunocompetent young man. J. Infect. 2006, 53, e47–e50. [Google Scholar] [CrossRef]
- Luft, B.J.; Kansas, G.; Engleman, E.G.; Remington, J.S. Functional and quantitative alterations in T lymphocyte subpopulations in acute toxoplasmosis. J. Infect. Dis. 1984, 150, 761–767. [Google Scholar] [CrossRef]
- Ramachandran, R.; Radhan, P.; Anand, R.; Subramanian, I.; Santosham, R.; Sai, V. CNS toxoplasmosis in an immunocompetent individual. Radiol. Case Rep. 2014, 9, e00031. [Google Scholar] [CrossRef] [Green Version]
- Lima, K.D.F.; de Queiroz, A.L.G.; Teixeira, H.S.; Bonsi, V.M.; Inada, B.S.Y.; Lancellotti, C.L.P.; Baêta, A.M. An atypical case of neurotoxoplasmosis in immunocompetent patient. Radiol. Case Rep. 2021, 16, 1766–1769. [Google Scholar] [CrossRef]
- Harbada, R.K.; Sorabjee, J.S.; Surya, N.; Jadhav, K.A.; Mirgh, S. Cerebellar Toxoplasmosis in an Immunocompetent Patient with G6PD Deficiency. J. Assoc. Physicians India 2016, 64, 79–82. [Google Scholar] [PubMed]
- Manwani, N.; Ravikumar, K.; Viswanathan, V.; Rao, S.M.; Mahadevan, A. Acquired Toxoplasmosis Presenting with a Brainstem Granuloma in an Immunocompetent Adolescent. Indian Pediatr. 2016, 53, 159–161. [Google Scholar] [CrossRef] [PubMed]
- Habek, M.; Ozretic, D.; Zarkovic, K.; Djakovic, V.; Mubrin, Z. Unusual cause of dementia in an immunocompetent host: Toxoplasmic encephalitis. Neurol. Sci. 2009, 30, 45–49. [Google Scholar] [CrossRef] [PubMed]
- Habek, M.; Ozretić, D.; Žarković, K.; Djaković, V.; Mubrin, Z. Severe acute multi-systemic failure with bilateral ocular toxoplasmosis in immunocompetent patients from urban settings in Colombia: Case reports. Am. J. Ophthalmol. Case Rep. 2020, 18, 100661. [Google Scholar]
- Roubille, F.; Roubille, C.; Lattuca, B.; Gervasoni, R.; Vernhet-Kovacsik, H.; Leclercq, F. Recent Toxoplasmosis Infection With Acute Myopericarditis and Persistent Troponin Elevation in an Immunocompetent Patient. Cardiol. Res. 2012, 3, 189–191. [Google Scholar] [CrossRef] [Green Version]
- Lévêque, M.F.; Chiffré, D.; Galtier, C.; Albaba, S.; Ravel, C.; Lachaud, L.; Iemmi, A.; Flori, P.; Sterkers, Y. Molecular diagnosis of toxoplasmosis at the onset of symptomatic primary infection: A straightforward alternative to serological examinations. Int. J. Infect. Dis. 2019, 79, 113–131. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chandenier, J.; Jarry, G.; Nassif, D.; Douadi, Y.; Paris, L.; Thulliez, P.; Bourges-Petit, E.; Raccurt, C. Congestive heart failure and myocarditis after seroconversion for toxoplasmosis in two immunocompetent patients. Eur. J. Clin. Microbiol. Infect. Dis. 2000, 19, 375–379. [Google Scholar] [CrossRef] [PubMed]
- Lévêque, M.F.; Albaba, S.; Arrada, N.; Avignon, M.; Sasso, M.; Fillaux, J.; Lachaud, L. Diagnosis of Congenital Toxoplasmosis: No Benefit of IgA Antibody Detection by Platelia ELISA in a Tricentric Evaluation. J. Clin. Microbiol. 2022, 60, e0011622. [Google Scholar] [CrossRef]
- Jimenez-Caballero, P.E.; Servia, M.; Marsal-Alonso, C. [Acute disseminated encephalomyelitis due to toxoplasmosis in an elderly patient]. Rev. Neurol. 2010, 50, 445–447. [Google Scholar]
- Paspalaki, P.K.; Mihailidou, E.P.; Bitsori, M.; Tsagkaraki, D.; Mantzouranis, E. Polyomyositis and myocarditis associated with acquired toxoplasmosis in an immunocompetent girl. BMC Musculoskelet. Disord. 2001, 2, 8. [Google Scholar] [CrossRef] [Green Version]
- Iniguez, C.; Jerico, I.; Pascual, L.F.; Cuesta, J.; Morales, F. [Miller-Fisher syndrome associated with toxoplasmosis]. Neurologia 1997, 12, 172–174. [Google Scholar]
- Sanchez, T.; Soriano, M.J.; Almarza, J.L.; Camara, M.; Paricio, P. [Diagnosis of cerebral toxoplasmosis in an immunocompetent patient]. Enferm. Infecc. Microbiol. Clin. 2000, 18, 46–48. [Google Scholar]
- Rutenberg, D.Z.Y.; Montoya, J.; Contopoulos-Ioannidis, D.; Elshereye, A.; Sinnott, J.; Kim, K.; Ava, M.; Strosberg, C. Severe toxoplasmosis pneumonia requiring intubation in an immunocompetent patient after consumption of deer meat in the southern United States. In Proceedings of the Abstract number 00173 33rd European Congress of Clinical Microbiology and Infectious Diseases—ECCMID 2023, Copenhagen, Denmark, 15–18 April 2023. [Google Scholar]
- Henry, L.; Beverley, J.K.; Johnson, S.G.; Whittaker, G.E. Experimental toxoplasmic myocarditis in rabbits. J. Pathol. 1970, 101, 141–149. [Google Scholar] [CrossRef] [PubMed]
- Bach, M.C.; Armstrong, R.M. Acute toxoplasmic encephalitis in a normal adult. Arch. Neurol. 1983, 40, 596–597. [Google Scholar] [CrossRef]
- Bannoura, S.; El Hajj, R.; Khalifeh, I.; El Hajj, H. Acute disseminated encephalomyelitis and reactivation of cerebral toxoplasmosis in a child: Case report. IDCases 2018, 13, e00434. [Google Scholar] [CrossRef]
- Azarpira, N.T.S.; Rad, H.; Taghipour, M. Ventriculitis: A Case of Cerebral Toxoplasmosis in Immunocompetent Child. Neurosurg. Q. 2014, 24, 159–160. [Google Scholar] [CrossRef]
- Galli-Tsinopoulou, A.; Kyrgios, I.; Giannopoulou, E.Z.; Gourgoulia, S.; Maggana, I.; Katechaki, E.; Chatzidimitriou, D.; Evangeliou, A.E. Acquired toxoplasmosis accompanied by facial nerve palsy in an immunocompetent 5-year-old child. J. Child Neurol. 2010, 25, 1525–1528. [Google Scholar] [CrossRef]
- Couvreur, J.; Thulliez, P. [Acquired toxoplasmosis of ocular or neurologic site: 49 cases]. Presse Med. 1996, 25, 438–442. [Google Scholar] [PubMed]
- Kaushik, R.M.; Mahajan, S.K.; Sharma, A.; Kaushik, R.; Kukreti, R. Toxoplasmic meningoencephalitis in an immunocompetent host. Trans. R. Soc. Trop. Med. Hyg. 2005, 99, 874–878. [Google Scholar] [CrossRef] [PubMed]
- Carme, B.; Demar, M.; Ajzenberg, D.; Darde, M.L. Severe acquired toxoplasmosis caused by wild cycle of Toxoplasma gondii, French Guiana. Emerg. Infect. Dis. 2009, 15, 656–658. [Google Scholar] [CrossRef]
- Darde, M.L. Toxoplasma gondii, “new” genotypes and virulence. Parasite 2008, 15, 366–371. [Google Scholar] [CrossRef] [Green Version]
- Maubon, D.; Ajzenberg, D.; Brenier-Pinchart, M.P.; Darde, M.L.; Pelloux, H. What are the respective host and parasite contributions to toxoplasmosis? Trends Parasitol. 2008, 24, 299–303. [Google Scholar] [CrossRef] [PubMed]
- Sullivan, W.J., Jr.; Jeffers, V. Mechanisms of Toxoplasma gondii persistence and latency. FEMS Microbiol. Rev. 2012, 36, 717–733. [Google Scholar] [CrossRef] [Green Version]
- Blaizot, R.; Nabet, C.; Laghoe, L.; Faivre, B.; Escotte-Binet, S.; Djossou, F.; Mosnier, E.; Henaff, F.; Blanchet, D.; Mercier, A.; et al. Outbreak of Amazonian Toxoplasmosis: A One Health Investigation in a Remote Amerindian Community. Front. Cell. Infect. Microbiol. 2020, 10, 401. [Google Scholar] [CrossRef] [PubMed]
- Blaizot, R.; Nabet, C.; Blanchet, D.; Martin, E.; Mercier, A.; Dardé, M.L.; Elenga, N.; Demar, M. Pediatric Amazonian Toxoplasmosis Caused by Atypical Strains in French Guiana, 2002–2017. Pediatr. Infect. Dis. J. 2019, 38, e39–e42. [Google Scholar] [CrossRef] [PubMed]
- Sobanski, V.; Ajzenberg, D.; Delhaes, L.; Bautin, N.; Just, N. Severe toxoplasmosis in immunocompetent hosts: Be aware of atypical strains. Am. J. Respir. Crit. Care Med. 2013, 187, 1143–1145. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Boyer, K.M.; Holfels, E.; Roizen, N.; Swisher, C.; Mack, D.; Remington, J.; Withers, S.; Meier, P.; McLeod, R.; Toxoplasmosis Study Group. Risk factors for Toxoplasma gondii infection in mothers of infants with congenital toxoplasmosis: Implications for prenatal management and screening. Am. J. Obstet. Gynecol. 2005, 192, 564–571. [Google Scholar] [CrossRef] [PubMed]
- Boyer, K.; Hill, D.; Mui, E.; Wroblewski, K.; Karrison, T.; Dubey, J.P.; Sautter, M.; Noble, A.G.; Withers, S.; Swisher, C.; et al. Unrecognized ingestion of Toxoplasma gondii oocysts leads to congenital toxoplasmosis and causes epidemics in North America. Clin. Infect. Dis. 2011, 53, 1081–1089. [Google Scholar] [CrossRef] [Green Version]


| N (or N/Total; %) | |
|---|---|
| Articles | 82 |
| N of severe toxoplasmosis cases | 117 |
| Ages | |
| Adults | 98/117 (84%) |
| Pediatric | 19/117 (16%) |
| Top 5/33 countries (where infection most likely acquired) * | |
| French Guiana | 23/117 (20%) |
| France | 17/117 (15%) |
| Colombia | 12/117 (9%) |
| India | 10/117 (9%) |
| Brazil | 8/117 (7%) |
| Duration of symptoms prior to admission (among those reporting) | N cases/Total reporting this information (%) |
| All | |
| <3 weeks (acute) | 62/83 (75%) |
| <3 months (acute or subacute) | 77/83 (93%) |
| Pulmonary | |
| <3 weeks (acute) | 25/31 (81%) |
| <3 months (acute or subacute) | 30/31 (97%) |
| CNS | |
| <3 weeks (acute) | 21/32 (66%) |
| <3 months (acute or subacute) | 29/32 (91%) |
| Cardiac | |
| <3 weeks (acute) | 20/23 (87%) |
| <3 months (acute or subacute) | 23/23 (100%) |
| Disseminated | |
| <3 weeks (acute) | 11/13 (85%) |
| <3 months (acute or subacute) | 13/13 (100%) |
| Diagnostic methods | |
| Serology | 111/117 (95%) |
| Molecular | 22/117 (19%) |
| Histopathologic | 24/117 (21%) |
| More than one diagnostic method | 98/117 (84%) |
| Based on response to anti-Toxoplasma therapy | 88/110 (80%) (unclear for 7) |
| Type of infection (cases) | |
| Acute Primary Toxoplasmosis | 98/117 (84%) |
| Unclear | 19/117 (16%) |
| Type of implicated T. gondii strains genotyped in (strains) | |
| Non-type II atypical strains | 22/23 (96%) |
| Type II strain | 1/23 (4%) |
| No genotyping/Not reporting genotyping data | 94/117 (80%) |
| Reporting risk factor | 60/117 (51%) |
| Risk factors | |
| Eating raw or undercooked meat or eating game meat | 28/60 (47%) |
| Living in high prevalence area (e.g., French Guiana) | 23/60 (38%) |
| Drinking untreated water | 22/60 (37%) |
| Contact with cats | 14/60 (23%) |
| Travel to high prevalence area (Central/South America/Amazonian region) | 8/60 (13%) |
| Contact with soil (gardening) | 2/60 (3%) |
| Multiple risk factors | 19/60 (32%) |
| Not reported risk factors | 57/117 (49%) |
| Outbreaks of severe toxoplasmosis cases (among those reporting risk factors) | |
| Military personnel outbreak | 13/60 (22%) |
| Family outbreak (e.g., outbreak during a humanitarian mission in Venezuela, or in family in the US returning from international Travel) | 2/60 (3%) |
| Clinical Manifestations of Severe Toxoplasmosis | N Cases/Total Applicable Cases (%) |
|---|---|
| Pulmonary a | 51/117 (44%) |
| Pneumonia | 48/51 (94%) |
| Respiratory failure | 24/51 (47%) |
| CNS a | 46/117 (39%) |
| Encephalitis | 25/46 (54%) |
| Meningitis | 6/46 (13%) |
| Focal Neurologic findings | 11/46 (24%) |
| Cranial nerve palsies | 8/46 (17%) |
| Guillain Barre syndrome | 3/46 (7%) |
| Spinal lesion | 1/46 (2%) |
| Cardiac a | 36/117 (31%) |
| Myocarditis | 27/36 (75%) |
| Pericarditis | 18/36 (50%) |
| Heart failure | 7/36 (19%) |
| Arrhythmia | 8/36 (22%) |
| Disseminated disease b | 28/117 (24%) |
| FUO > 3 months c | 2/117 (2%) |
| More than one organ system involved | 31/117 (27%) |
| Severity of Illness (among those reporting) | |
| Critical Illness | 44/90 (49%) |
| ICU admission | 29/54 (54%) |
| Fatal Outcome | 9/110 (8%) |
| Outcomes (among those reporting) | |
| Improvement/resolution (at last follow up) | 88/110 (80%) |
| Resolution without or before anti-Toxoplasma treatment | 13/110 (12%) |
| Fatal outcome | 9/110 (8%) |
| Time to resolution (among those reporting) | |
| Resolution <4 weeks from treatment | 23/36 (64%) |
| N Cases/Total Applicable Cases Reporting This Information (%) | |
|---|---|
| Lung Imaging Findings a (reported in 75% (38/51) of pulmonary cases) | |
| Diffuse bilateral infiltrates (ground glass opacities, interstitial/alveolar infiltrates) | 31/38 (82%) |
| Nodular lesions/opacities | 5/38 (13%) |
| Focal localized consolidations | 6/38 (16%) |
| Pleural effusions | 18/38 (47%) |
| Mediastinal LADP | 4/38 (11%) |
| CNS Imaging Findings a (reported in 41/46 CNS cases) | |
| By appearance | |
| Abscess like/mass-like focal lesions | 21/41 (51%) |
| Diffuse encephalitis | 7/41 (17%) |
| Meningitis | 4/41 (10%) |
| Meningoencephalitis | 2/41 (5%) |
| By location | |
| Focal supratentorial lesions | 28/41 (68%) |
| Focal infratentorial lesions | 3/41 (7%) |
| Spinal lesions | 2/41 (5%) |
| Cardiac Imaging Findings a (reported in 34/36 cardiac cases) | |
| Myocarditis | 23/34 (68%) |
| Pericarditis | 16/34 (47%) |
| Myopericarditis | 11/34 (34%) |
| Low cardiac function/heart failure | 13/34 (45%) |
| Cardiac rhythm abnormalities | 10/34 (29%) |
| Imaging Findings | |
|---|---|
| Lung imaging findings * | Diffuse ground glass opacities (GGO) Pulmonary interstitial infiltrates (unilateral or bilateral)/interstitial syndrome /interstitial pneumonia Reticular/alveolar infiltrates Peribroncho-vascular thickening Septal thickening Pulmonary nodules/nodular opacities (multiple, unilateral or bilateral) Nodular cavities Focal areas of consolidation (unilateral) Atelectasis Paratracheal/mediastinal lymphadenopathy Pleural effusions (large or small, bilateral or unilateral) Diffuse pulmonary infiltrates and/or mediastinal lymphadenopathy intensely metabolically active in PET scan. |
| CNS imaging findings £ | Multifocal white matter and/or grey matter lesions T2 hyperintense lesions/T1 hypointense lesions (unifocal or multifocal), in the frontoparietal, temporal, periventricular region, basal ganglia, pons or corticomedullary junction € FLAIR high signal lesions Ring-enhancing lesions (single or multiple, unilateral or bilateral) Peripherally enhancing lesions (with or without central diffusion restriction in DWI sequences) Open ring-enhancing lesions Mass-like lesions/abscess-like lesions/ granuloma-like lesions/ tuberculoma-like lesions Micro-abscess like lesions (with perilesional edema) Mushroom-shaped lesions (with irregular rim enhancement) Perivascular enhancing lesions with vasogenic edema and adjacent hemorrhagic focus Midline shift ADEM-like lesions Cerebellar lesions/ rhombencephalitis Hydrocephalus/ Ventriculitis Leptomeningeal enhancement Brain calcifications Intraspinal/intramedullary ring enhancing lesion Normal brain MRI (e.g., case of NMDA encephalitis associated with acute toxoplasmosis) |
| Cardiac imaging findings ± | Myocarditis picture with late gadolinium enhancement; subepicardial enhancement and/or myocardial necrosis in cardiac MRI Pericarditis findings with hyperechoic pericardium/ pericardial effusions (small or large, with or without cardiac tamponade) in cardiac MRI Cardiomegaly Cardiac function with poor contractility; hypokinesia of ventricular walls; low ejection fraction, heart failure EKG with AV block, AV dissociation, bundle branch block; tachyarrhythmia, ventricular fibrillation |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Layton, J.; Theiopoulou, D.-C.; Rutenberg, D.; Elshereye, A.; Zhang, Y.; Sinnott, J.; Kim, K.; Montoya, J.G.; Contopoulos-Ioannidis, D.G. Clinical Spectrum, Radiological Findings, and Outcomes of Severe Toxoplasmosis in Immunocompetent Hosts: A Systematic Review. Pathogens 2023, 12, 543. https://doi.org/10.3390/pathogens12040543
Layton J, Theiopoulou D-C, Rutenberg D, Elshereye A, Zhang Y, Sinnott J, Kim K, Montoya JG, Contopoulos-Ioannidis DG. Clinical Spectrum, Radiological Findings, and Outcomes of Severe Toxoplasmosis in Immunocompetent Hosts: A Systematic Review. Pathogens. 2023; 12(4):543. https://doi.org/10.3390/pathogens12040543
Chicago/Turabian StyleLayton, John, Danai-Christina Theiopoulou, David Rutenberg, Amro Elshereye, Yumeng Zhang, John Sinnott, Kami Kim, Jose G. Montoya, and Despina G. Contopoulos-Ioannidis. 2023. "Clinical Spectrum, Radiological Findings, and Outcomes of Severe Toxoplasmosis in Immunocompetent Hosts: A Systematic Review" Pathogens 12, no. 4: 543. https://doi.org/10.3390/pathogens12040543