
Case Series of Primaquine-Induced Haemolytic Events in Controlled Trials with G6PD Screening
 , ,
, ,
Abstract
:1. Introduction
2. Case Series
2.1. Case 1
2.2. Case 2
2.3. Case 3
2.4. Case 4
2.5. Case 5
3. Discussion
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A. Primaquine Dosing Table

{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Body Weight (kg) | mg/tab | Tablet Given/Day | Actual Dose (mg/kgBW) | Total Dose (mg/kgBW) |
|---|---|---|---|---|
| 11.5–12.4 | 15 | 0.75 | 0.94 | 6.56 |
| 12.5–13.4 | 15 | 0.75 | 0.87 | 6.06 |
| 13.5–14.4 | 15 | 1 | 1.07 | 7.50 |
| 14.5–15.4 | 15 | 1 | 1.00 | 7.00 |
| 15.5–16.4 | 15 | 1 | 0.94 | 6.56 |
| 16.5–17.4 | 15 | 1 | 0.88 | 6.18 |
| 17.5–18.4 | 15 | 1.25 | 1.04 | 7.29 |
| 18.5–19.4 | 15 | 1.25 | 0.99 | 6.91 |
| 19.5–20.4 | 15 | 1.25 | 0.94 | 6.56 |
| 20.5–21.4 | 15 | 1.25 | 0.89 | 6.25 |
| 21.5–22.4 | 15 | 1.5 | 1.02 | 7.16 |
| 22.5–23.4 | 15 | 1.5 | 0.98 | 6.85 |
| 23.5–24.4 | 15 | 1.5 | 0.94 | 6.56 |
| 24.5–25.4 | 15 | 1.5 | 0.90 | 6.30 |
| 25.5–26.4 | 15 | 1.75 | 1.01 | 7.07 |
| 26.5–27.4 | 15 | 1.75 | 0.97 | 6.81 |
| 27.5–28.4 | 15 | 1.75 | 0.94 | 6.56 |
| 28.5–29.4 | 15 | 1.75 | 0.91 | 6.34 |
| 29.5–30.4 | 15 | 2 | 1.00 | 7.00 |
| 30.5–31.4 | 15 | 2 | 0.97 | 6.77 |
| 31.5–32.4 | 15 | 2 | 0.94 | 6.56 |
| 32.5–33.4 | 15 | 2.25 | 1.02 | 7.16 |
| 33.5–34.4 | 15 | 2.25 | 0.99 | 6.95 |
| 34.5–35.4 | 15 | 2.25 | 0.96 | 6.75 |
| 35.5–36.4 | 15 | 2.25 | 0.94 | 6.56 |
| 36.5–37.4 | 15 | 2.5 | 1.01 | 7.09 |
| Weight | 10–19.9 kg | 20–29.9 kg | 30–39.9 kg | 40–49.9 | ≥50 kg |
|---|---|---|---|---|---|
| Number of tablets per daily dose | ½ tablet | ¾ tablet | 1 tablet | 1 ½ tablets | 2 tablets |
| Primaquine per daily dose (mg) | 3.75 | 5.625 | 7.5 | 11.25 | 15 |
| Primaquine mg/kg daily dose range | 0.19–0.375 | 0.19–0.281 | 0.19–0.25 | 0.23–0.28 | ≤0.3 |
| Weight Band | Weight/kg | PQ7 | PQ14 | ||
|---|---|---|---|---|---|
| 1 mg/kg/Day | mg/kg | 0.5 mg/kg/Day | mg/kg | ||
| A | 5 to 22 | see suspension dosing chart | see suspension dosing chart | ||
| A | 23–34 | 30 | 0.88–1.3 | 15 | 0.44–0.65 |
| B | 35–45 | 45 | 1–1.29 | 22.25 | 0.5–0.64 |
| C | ≥46 | 60 | <1.33 | 30 | ≤0.67 |
| Weight | mL/Day | 7 Day Primaquine Regimen (PQ7) Two 15 mg Tablet Dissolved in 5 mL Syrup (1 mL = 6 mg) | 14 Day Primaquine Regimen (PQ14) One 15 mg Tablet Dissolved in 5 mL Syrup (1 mL = 3 mg) | ||||||
|---|---|---|---|---|---|---|---|---|---|
| Daily Dose in mg/Day | Daily Dose in mg/kg/Day | Total Dose in mg/kg | Total Dose in mg | Daily Dose in mg/Day | Daily Dose in mg/kg/Day | Total Dose in mg/kg | Total Dose in mg | ||
| 5 | 0.8 | 4.8 | 0.96 | 6.72 | 33.6 | 2.4 | 0.48 | 6.72 | 33.6 |
| 6 | 1 | 6 | 1 | 7 | 42 | 3 | 0.5 | 7 | 42 |
| 7 | 1.2 | 7.2 | 1.03 | 7.2 | 50.4 | 3.6 | 0.51 | 7.2 | 50.4 |
| 8 | 1.3 | 7.8 | 0.98 | 6.83 | 54.6 | 3.9 | 0.49 | 6.83 | 54.6 |
| 9 | 1.5 | 9 | 1 | 7 | 63 | 4.5 | 0.5 | 7 | 63 |
| 10 | 1.7 | 10.2 | 1.02 | 7.14 | 71.4 | 5.1 | 0.51 | 7.14 | 71.4 |
| 11 | 1.8 | 10.8 | 0.98 | 6.87 | 75.6 | 5.4 | 0.49 | 6.87 | 75.6 |
| 12 | 2 | 12 | 1 | 7 | 84 | 6 | 0.5 | 7 | 84 |
| 13 | 2.2 | 13.2 | 1.02 | 7.11 | 92.4 | 6.6 | 0.51 | 7.11 | 92.4 |
| 14 | 2.3 | 13.8 | 0.99 | 6.9 | 96.6 | 6.9 | 0.49 | 6.9 | 96.6 |
| 15 | 2.5 | 15 | 1 | 7 | 105 | 7.5 | 0.5 | 7 | 105 |
| 16 | 2.5 | 15 | 0.94 | 6.56 | 105 | 7.5 | 0.47 | 6.56 | 105 |
| 17 | 3 | 18 | 1.06 | 7.41 | 126 | 9 | 0.53 | 7.4 | 126 |
| 18 | 3 | 18 | 1 | 7 | 126 | 9 | 0.5 | 7 | 126 |
| 19 | 3 | 18 | 0.95 | 6.63 | 126 | 9 | 0.47 | 6.63 | 126 |
| 20 | 3 | 18 | 0.9 | 6.3 | 126 | 9 | 0.45 | 6.3 | 126 |
| 21 | 3.5 | 21 | 1 | 7 | 147 | 10.5 | 0.5 | 7 | 147 |
| 22 | 3.5 | 21 | 0.95 | 6.68 | 147 | 10.5 | 0.48 | 6.68 | 147 |
Appendix B. Clinical Progression and Laboratory Parameters from the Start of Primaquine Administration to the Onset of Acute Haemolytic Anaemia
| Treatment Day | Day 1 | Day 2 | Day 3 | Day 4 | Day 5 |
|---|---|---|---|---|---|
| Date | 2 March 2022 | 3 March 2022 | 4 March 2022 | 5 March 2022 | 6 March 2022 |
| Symptoms | None | None | None | Abdominal pain and nausea relieved after meal and antacid | Fever, headache, and abdominal pain |
| General condition | Good | Good | Good | Good | Slightly weaker, outdoor activity is impaired |
| MetHb | 0.4 (during enrolment) | − | − | − | 4.9 |
| Temperature (°C) | − | − | − | − | 36.7 |
| Heart rate (beats/min) | 82 | 101 | 92 | 95 | 116 |
| Respiratory rate (breaths/min) | 18 | 19 | 24 | 21 | 20 |
| Primaquine exposure (mg/kg) | 1.1 | 0.9 | 0.9 | 0.9 | Stopped |
| Hb (g/dL) | 12.0 (during enrolment) | 12.1 | 10.6 | 10.8 | 8.3 |
| Hillmen | 2 | 2 | 3 | 4 | 5 |
| Urine dipstick | Blood trace, urobilinogen 0.2 E.U./dL | No blood, urobilinogen 0.2 E.U./dL | No blood, urobilinogen 1.0 E.U./dL | Blood trace, urobilinogen 1.0 E.U./dL | Blood trace, urobilinogen 2.0 E.U./dL |
| Treatment Day | Day 1 | Day 2 | Day 3 | Day 4 |
|---|---|---|---|---|
| Date | 2 November 2017 | 3 November 2017 | 4 November 2017 | 5 November 2017 |
| Symptoms | None | Fatigue | Fatigue | Fatigue |
| General condition | Good | Good | Good | Pale, jaundice |
| metHb (%) | 0.0 | 8.3 | 11.6 | 15.8 |
| Temperature (°C) | 37.2 | 36.6 | 37.3 | 37.7 |
| Heart rate (beats/min) | 53 | 58 | 63 | 75 |
| Respiratory rate (breaths/min) | 22 | 20 | 24 | 20 |
| Primaquine exposure (mg/kg) | 0.28 | 0.28 | 0.28 | Stopped |
| Hb (g/dL) | 10.1 | 9.3 | 9.1 | 7.9 |
| Hillmen | − | − | − | 5 |
| Urine dipstick | − | − | − | Urobilinogen 8.0 E.U./dL |
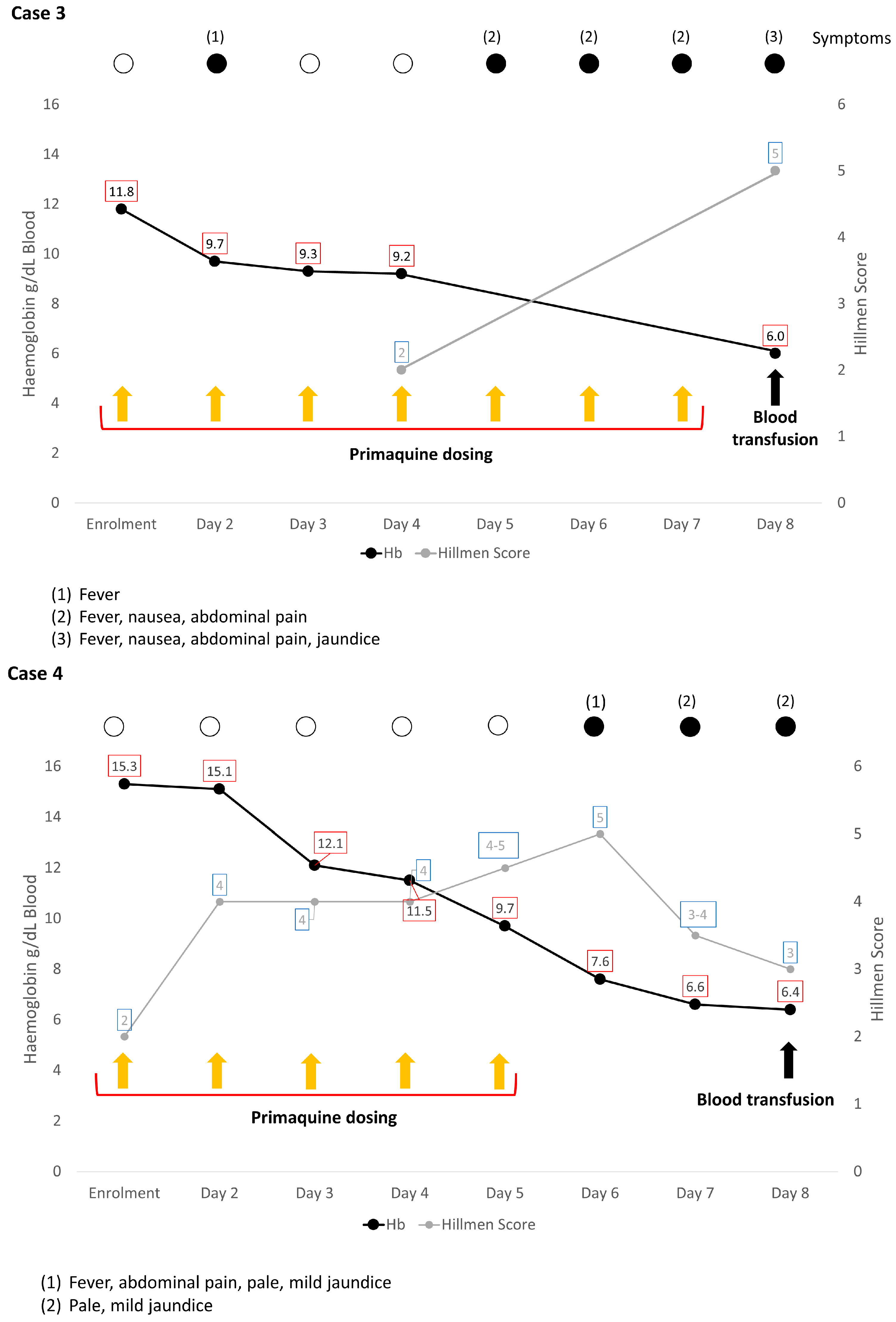
| Treatment Day | Day 1 | Day 2 | Day 3 | Day 4 | Day 5 | Day 6 | Day 7 | Day 8 |
|---|---|---|---|---|---|---|---|---|
| Date | 19 December 2017 | 20 December 2017 | 21 December 2017 | 22 December 2017 | 23 December 2017 | 24 December 2017 | 25 December 2017 | 26 December 2017 |
| Symptoms | None | Fever | None | None | − | − | − | Fever, nausea over 3 days |
| General condition | Good | Good | Good | Good | − | − | − | Pale, jaundice, right upper quadrant abdominal pain |
| metHb (%) | 0.4 | 0.5 | 0.1 | 2.5 | − | − | − | 1.7 |
| Temperature (°C) | 36.9 | 37.2 | 36.7 | 37.1 | − | − | − | 37.8 |
| Heart rate (beats/min) | 84 | 80 | 75 | 78 | − | − | − | 102 |
| Respiratory rate (breaths/min) | 25 | 22 | 24 | 26 | − | − | − | 22 |
| Primaquine exposure (mg/kg) | 0.27 | 0.27 | 0.27 | 0.27 | 0.27 | 0.27 | 0.27 | Stopped |
| Hb (g/dL) | 11.8 | 9.7 | 9.3 | 9.2 | − | − | − | 6.0 |
| Hillmen | − | − | − | 2 | − | − | − | 5 |
| Urine dipstick | − | − | − | Urobilinogen 0.2 E.U./dL (3.2 µmol/L) | − | − | − | Urobilinogen 8 E.U./dL (131 µmol/L) |
| Treatment Day | Day 1 | Day 2 | Day 3 | Day 4 | Day 5 | Day 6 |
|---|---|---|---|---|---|---|
| Date | 16 November 2014 | 17 November 2014 | 18 November 2014 | 19 November 2014 | 20 November 2014 | 21 November 2014 |
| Symptoms | None | None | None | None | None | Abdominal pain |
| General condition | Good | Good | Good | Good | Good | Pale, mild jaundice |
| MetHb | − | − | − | − | − | − |
| Heart rate (beats/min) | 108 | 81 | 82 | 82 | 90 | 96 |
| Respiratory rate (breaths/min) | 32 | 30 | 26 | 24 | 24 | 26 |
| Primaquine exposure (mg/kg) | 1.0 | 1.0 | 1.0 | 1.0 | 1.0 | Stopped |
| Hb (g/dL) | 15.3 | 15.1 | 12.1 | 11.5 | 9.7 | 7.6 |
| Hillmen | 2 | 4 | 4 | 4 | 4–5 | 5 |
| Urine dipstick | − | − | − | − | − | − |
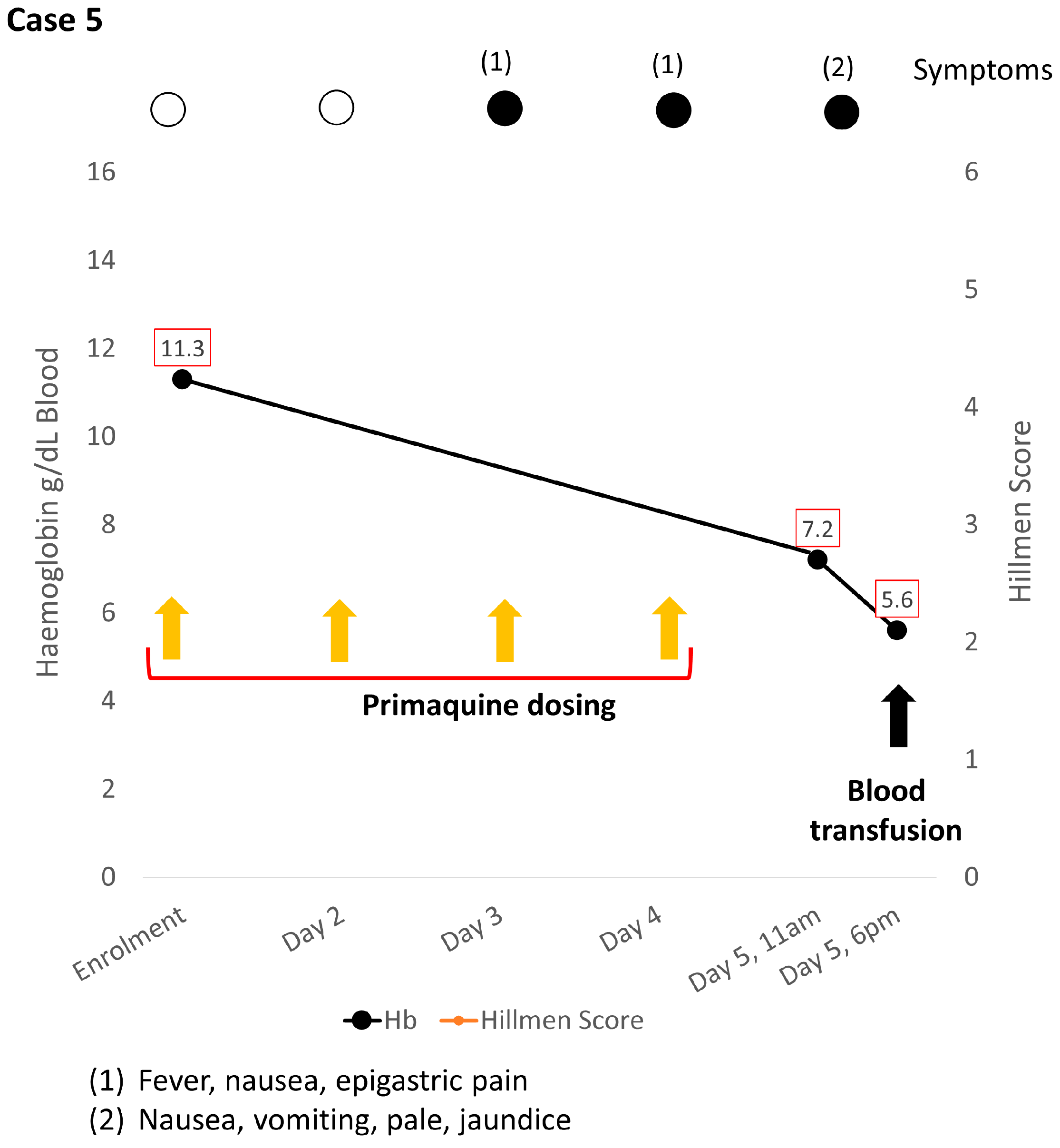
| Treatment Day | Day 1 | Day 2 | Day 3 | Day 4 | Day 5 |
|---|---|---|---|---|---|
| Date | 19 October 2012 | 20 October 2012 | 21 October 2012 | 22 October 2012 | 23 October 2012 |
| Symptoms | None | None | Nausea, fever | Nausea, vomiting, fever | Nausea, vomiting |
| General condition | Good | Good | Epigastric pain | Epigastric pain | Pale, jaundice |
| Temperature (°C) | − | − | − | 36.4 | 36.8 |
| metHb | − | − | − | − | − |
| Heart rate (beats/min) | − | − | − | − | 129 |
| Respiratory rate (breaths/min) | − | − | − | − | 20 |
| Primaquine (mg/kg) | 0.65 | 0.65 | 0.65 | 0.65 | Stopped |
| Hb (g/dL) | 11.3 | − | − | − | 7.2 |
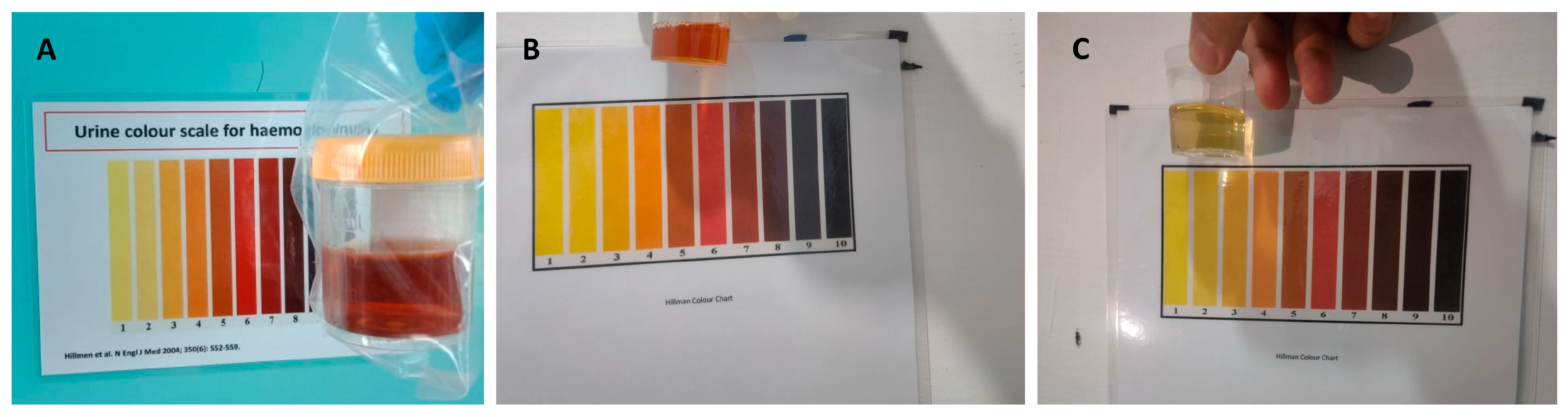
| Urine colour * | − | − | − | − | Dark |
| Urine dipstick | − | − | − | − | − |
Appendix C. Laboratory Finding Upon Admission to Referral Hospital
| Parameter (Unit) | Case 1 | Case 2 * | Case 3 | Case 4 | Case 5 | Reference ** |
|---|---|---|---|---|---|---|
| Hematology | ||||||
| Haemoglobin (g/dL) | 4.7 | − | 6.7 | 7.1 | 5.6 | 10.8–15.6 |
| Hematocrit (%) | 15.0 | − | − | 21.0 | 19.4 | 33–45 |
| Reticulocyte (%) | 6.26 | − | − | − | − | 0.2–2.5 |
| Platelet (/µL) | 353,000 | − | 355,000 | − | 244,000 | 181,000–521,000 |
| Leucocyte (/µL) | 19,090 | − | 8500 | − | 23,600 | 4500–13,500 |
| Neutrophil count (/µL) | 11,660 | − | − | − | − | 2400–7300 |
| SGPT/AST (U/L) | 12 | − | − | 43 | 45 | 0–55 |
| SGOT/ALT (U/L) | 23 | − | − | 29 | 14 | 5–34 |
| Urea (mg/dL) | 26 | − | − | − | 66 | 19–44 |
| Creatinine (mg/dL) | 0.91 | − | − | 0.89 | 0.58 | 0.7–1.3 |
| Procalcitonin (mg/mL) | 0.71 | − | − | − | − | <0.1 |
| Ferritin (ng/mL) | 600 | − | − | − | − | 15–150 |
| Fe/iron (µg/dL) | 217 | − | − | − | − | 65–175 |
| TIBC (µg/dL) | 242 | − | − | − | − | 112–346 |
| Direct coombs test | Negative | − | − | Negative | − | Negative |
| Indirect coombs test | Negative | − | − | Negative | − | Negative |
| Total bilirubin (mg/dL) | 2.4 | − | − | 0.91 | 8.8 | 0.2–1.2 |
| Direct bilirubin (mg/dL) | 0.7 | − | − | 0.24 | 0.7 | <0.5 |
Appendix D. G6PD Genotyping Methods
G6PD Genotyping Methods in Case 1
Appendix E. Ethical Approval Information
Appendix E.1. Case 1
Appendix E.2. Case 2 & 3
Appendix E.3. Case 4
Appendix E.4. Case 5
References
- World Health Organization. World Malaria Report 2022; World Health Organization: Geneva, Switzerland, 2022. [Google Scholar]
- Angrisano, F.; Robinson, L.J. Plasmodium vivax—How hidden reservoirs hinder global malaria elimination. Parasitol. Int. 2022, 87, 102526. [Google Scholar] [CrossRef]
- Stadler, E.; Cromer, D.; Mehra, S.; Adekunle, A.I.; Flegg, J.A.; Anstey, N.M.; Watson, J.A.; Chu, C.S.; Mueller, I.; Robinson, L.J.; et al. Population heterogeneity in Plasmodium vivax relapse risk. PLoS Neglected Trop. Dis. 2022, 16, e0010990. [Google Scholar] [CrossRef]
- World Health Organization. WHO Guidelines for Malaria, 3 June 2022; World Health Organization: Geneva, Switzerland, 2022. [Google Scholar]
- Anjum, M.U.; Naveed, A.K.; Mahmood, S.N.; Naveed, O.K. Single dose tafenoquine for preventing relapse in people with Plasmodium vivax malaria—An updated meta-analysis. Travel Med. Infect. Dis. 2020, 36, 101576. [Google Scholar] [CrossRef]
- Beutler, E.; Duparc, S. Glucose-6-phosphate dehydrogenase deficiency and antimalarial drug development. Am. J. Trop. Med. Hyg. 2007, 77, 779–789. [Google Scholar] [CrossRef] [PubMed]
- Howes, R.E.; Piel, F.B.; Patil, A.P.; Nyangiri, O.A.; Gething, P.W.; Dewi, M.; Hogg, M.M.; Battle, K.E.; Padilla, C.D.; Baird, J.K.; et al. G6PD deficiency prevalence and estimates of affected populations in malaria endemic countries: A geostatistical model-based map. PLoS Med. 2012, 9, e1001339. [Google Scholar] [CrossRef] [PubMed]
- Pasaribu, A.P.; Chokejindachai, W.; Sirivichayakul, C.; Tanomsing, N.; Chavez, I.; Tjitra, E.; Pasaribu, S.; Imwong, M.; White, N.J.; Dondorp, A.M. A randomized comparison of dihydroartemisinin-piperaquine and artesunate-amodiaquine combined with primaquine for radical treatment of vivax malaria in Sumatera, Indonesia. J. Infect. Dis. 2013, 208, 1906–1913. [Google Scholar] [CrossRef] [PubMed]
- Satyagraha, A.W.; Sadhewa, A.; Baramuli, V.; Elvira, R.; Ridenour, C.; Elyazar, I.; Noviyanti, R.; Coutrier, F.N.; Harahap, A.R.; Baird, J.K. G6PD deficiency at Sumba in Eastern Indonesia is prevalent, diverse and severe: Implications for primaquine therapy against relapsing Vivax malaria. PLoS Negl. Trop. Dis. 2015, 9, e0003602. [Google Scholar] [CrossRef]
- Bancone, G.; Menard, D.; Khim, N.; Kim, S.; Canier, L.; Nguong, C.; Phommasone, K.; Mayxay, M.; Dittrich, S.; Vongsouvath, M.; et al. Molecular characterization and mapping of glucose-6-phosphate dehydrogenase (G6PD) mutations in the Greater Mekong Subregion. Malar. J. 2019, 18, 20. [Google Scholar] [CrossRef]
- Kuwahata, M.; Wijesinghe, R.; Ho, M.F.; Pelecanos, A.; Bobogare, A.; Landry, L.; Bugora, H.; Vallely, A.; McCarthy, J. Population screening for glucose-6-phosphate dehydrogenase deficiencies in Isabel Province, Solomon Islands, using a modified enzyme assay on filter paper dried bloodspots. Malar. J. 2010, 9, 223. [Google Scholar] [CrossRef]
- Satyagraha, A.W.; Sadhewa, A.; Elvira, R.; Elyazar, I.; Feriandika, D.; Antonjaya, U.; Oyong, D.; Subekti, D.; Rozi, I.E.; Domingo, G.J.; et al. Assessment of point-of-care diagnostics for G6PD deficiency in malaria endemic rural eastern Indonesia. PLoS Negl. Trop. Dis. 2016, 10, e0004457. [Google Scholar] [CrossRef]
- Pal, S.; Bansil, P.; Bancone, G.; Hrutkay, S.; Kahn, M.; Gornsawun, G.; Penpitchaporn, P.; Chu, C.S.; Nosten, F.; Domingo, G.J. Evaluation of a novel quantitative test for glucose-6-phosphate dehydrogenase deficiency: Bringing quantitative testing for glucose-6-phosphate dehydrogenase deficiency closer to the patient. Am. J. Trop. Med. Hyg. 2019, 100, 213–221. [Google Scholar] [CrossRef] [PubMed]
- Commons, R.J.; Simpson, J.A.; Watson, J.; White, N.J.; Price, R.N. Estimating the proportion of Plasmodium vivax recurrences caused by relapse: A systematic review and meta-analysis. Am. J. Trop. Med. Hyg. 2020, 103, 1094–1099. [Google Scholar] [CrossRef] [PubMed]
- Charnaud, S.; Munro, J.E.; Semenec, L.; Mazhari, R.; Brewster, J.; Bourke, C.; Ruybal-Pesántez, S.; James, R.; Lautu-Gumal, D.; Karunajeewa, H.; et al. PacBio long-read amplicon sequencing enables scalable high-resolution population allele typing of the complex CYP2D6 locus. Commun. Biol. 2022, 5, 168. [Google Scholar] [CrossRef] [PubMed]
- WHO Global Malaria Programme; Malaria Policy Advisory Group. Meeting Report of the Technical Consultation to Review the Classification of Glucose-6-Phosphate Dehydrogenase (G6PD); WHO: Geneva, Switzerland, 2022. [Google Scholar]
- Taylor, W.R.J.; Thriemer, K.; von Seidlein, L.; Yuentrakul, P.; Assawariyathipat, T.; Assefa, A.; Auburn, S.; Chand, K.; Chau, N.H.; Cheah, P.Y.; et al. Short-course primaquine for the radical cure of Plasmodium vivax malaria: A multicentre, randomised, placebo-controlled non-inferiority trial. Lancet 2019, 394, 929–938. [Google Scholar] [CrossRef] [PubMed]
- Syafruddin, D.; Bangs, M.J.; Sidik, D.; Elyazar, I.; Asih, P.B.; Chan, K.; Nurleila, S.; Nixon, C.; Hendarto, J.; Wahid, I.; et al. Impact of a spatial repellent on malaria incidence in two villages in Sumba, Indonesia. Am. J. Trop. Med. Hyg. 2014, 91, 1079–1087. [Google Scholar] [CrossRef]
- Kim, S.; Nguon, C.; Guillard, B.; Duong, S.; Chy, S.; Sum, S.; Nhem, S.; Bouchier, C.; Tichit, M.; Christophel, E.; et al. Performance of the CareStart™ G6PD deficiency screening test, a point-of-care diagnostic for primaquine therapy screening. PLoS ONE 2011, 6, e28357. [Google Scholar] [CrossRef]
- Zobrist, S.; Brito, M.; Garbin, E.; Monteiro, W.M.; Clementino Freitas, S.; Macedo, M.; Soares Moura, A.; Advani, N.; Kahn, M.; Pal, S.; et al. Evaluation of a point-of-care diagnostic to identify glucose-6-phosphate dehydrogenase deficiency in Brazil. PLoS Negl. Trop. Dis. 2021, 15, e0009649. [Google Scholar] [CrossRef]
- Tinley, K.E.; Loughlin, A.M.; Jepson, A.; Barnett, E.D. Evaluation of a rapid qualitative enzyme chromatographic test for glucose-6-phosphate dehydrogenase deficiency. Am. J. Trop. Med. Hyg. 2010, 82, 210–214. [Google Scholar] [CrossRef]
- Thielemans, L.; Gornsawun, G.; Hanboonkunupakarn, B.; Paw, M.K.; Porn, P.; Moo, P.K.; van Overmeire, B.; Proux, S.; Nosten, F.; McGready, R.; et al. Diagnostic performances of the fluorescent spot test for G6PD deficiency in newborns along the Thailand-Myanmar border: A cohort study. Wellcome Open Res. 2018, 3, 1. [Google Scholar] [CrossRef]
- Sadhewa, A.; Cassidy-Seyoum, S.; Acharya, S.; Devine, A.; Price, R.N.; Mwaura, M.; Thriemer, K.; Ley, B. A review of the current status of G6PD deficiency testing to guide radical cure treatment for vivax malaria. Pathogens 2023, 12, 650. [Google Scholar] [CrossRef]
- Commons, R.J.; Simpson, J.A.; Thriemer, K.; Chu, C.S.; Douglas, N.M.; Abreha, T.; Alemu, S.G.; Añez, A.; Anstey, N.M.; Aseffa, A.; et al. The haematological consequences of Plasmodium vivax malaria after chloroquine treatment with and without primaquine: A WorldWide Antimalarial Resistance Network systematic review and individual patient data meta-analysis. BMC Med. 2019, 17, 151. [Google Scholar] [CrossRef] [PubMed]
- Alving, A.S.; Johnson, C.F.; Tarlov, A.R.; Brewer, G.J.; Kellermeyer, R.W.; Carson, P.E. Mitigation of the haemolytic effect of primaquine and enhancement of its action against exoerythrocytic forms of the Chesson strain of Piasmodium vivax by intermittent regimens of drug administration: A preliminary report. Bull. World Health Organ. 1960, 22, 621–631. [Google Scholar] [PubMed]
- Chu, C.S.; Phyo, A.P.; Turner, C.; Win, H.H.; Poe, N.P.; Yotyingaphiram, W.; Thinraow, S.; Wilairisak, P.; Raksapraidee, R.; Carrara, V.I.; et al. Chloroquine versus dihydroartemisinin-piperaquine with standard high-dose primaquine given either for 7 days or 14 days in Plasmodium vivax malaria. Clin. Infect. Dis. 2019, 68, 1311–1319. [Google Scholar] [CrossRef] [PubMed]
- Salvidio, E.; Pannacciulli, I.; Tizianello, A.; Ajmar, F. Nature of hemolytic crises and the fate of G6PD deficient, drug-damaged erythrocytes in Sardinians. N. Engl. J. Med. 1967, 276, 1339–1344. [Google Scholar] [CrossRef] [PubMed]
- Taylor, W.R.J.; Kim, S.; Kheng, S.; Muth, S.; Tor, P.; Christophel, E.; Mukaka, M.; Kerleguer, A.; Luzzatto, L.; Baird, J.K.; et al. Dynamics of G6PD activity in patients receiving weekly primaquine for therapy of Plasmodium vivax malaria. PLoS Negl. Trop. Dis. 2021, 15, e0009690. [Google Scholar] [CrossRef] [PubMed]
- Chu, C.S.; Bancone, G.; Soe, N.L.; Carrara, V.I.; Gornsawun, G.; Nosten, F. The impact of using primaquine without prior G6PD testing: A case series describing the obstacles to the medical management of haemolysis. Wellcome Open Res. 2019, 4, 25. [Google Scholar] [CrossRef]
- Douglas, N.M.; Piera, K.A.; Rumaseb, A.; Ley, B.; Anstey, N.M.; Price, R.N. Primaquine-induced severe hemolysis in the absence of concomitant malaria: Effects on G6PD activity and renal function. Am. J. Trop. Med. Hyg. 2023, 108, 76–80. [Google Scholar] [CrossRef]
- Kheng, S.; Muth, S.; Taylor, W.R.; Tops, N.; Kosal, K.; Sothea, K.; Souy, P.; Kim, S.; Char, C.M.; Vanna, C.; et al. Tolerability and safety of weekly primaquine against relapse of Plasmodium vivax in Cambodians with glucose-6-phosphate dehydrogenase deficiency. BMC Med. 2015, 13, 203. [Google Scholar] [CrossRef]
- Brueckner, R.P.; Lasseter, K.C.; Lin, E.T.; Schuster, B.G. First-time-in-humans safety and pharmacokinetics of WR 238605, a new antimalarial. Am. J. Trop. Med. Hyg. 1998, 58, 645–649. [Google Scholar] [CrossRef]
- Baird, K. Origins and implications of neglect of G6PD deficiency and primaquine toxicity in Plasmodium vivax malaria. Pathog. Glob. Health 2015, 109, 93–106. [Google Scholar] [CrossRef]
- Bancone, G.; Chu, C.S. G6PD variants and haemolytic sensitivity to primaquine and other drugs. Front. Pharmacol. 2021, 12, 638885. [Google Scholar] [CrossRef]
- Pannacciulli, I.; Tizianello, A.; Ajmar, F.; Salvidio, E. The course of experimentally induced hemolytic anemia in a primaquine-sensitive Caucasian. A case study. Blood 1965, 25, 92–95. [Google Scholar] [CrossRef] [PubMed]
- Burgoine, K.L.; Bancone, G.; Nosten, F. The reality of using primaquine. Malar. J. 2010, 9, 376. [Google Scholar] [CrossRef] [PubMed]
- Meloni, T.; Forteleoni, G.; Dore, A.; Cutillo, S. Favism and hemolytic anemia in glucose-6-phosphate dehydrogenase-deficient subjects in North Sardinia. Acta Haematol. 1983, 70, 83–90. [Google Scholar] [CrossRef] [PubMed]




Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kosasih, A.; James, R.; Chau, N.H.; Karman, M.M.; Panggalo, L.V.; Wini, L.; Thanh, N.V.; Obadia, T.; Satyagraha, A.W.; Asih, P.B.S.; et al. Case Series of Primaquine-Induced Haemolytic Events in Controlled Trials with G6PD Screening. Pathogens 2023, 12, 1176. https://doi.org/10.3390/pathogens12091176
Kosasih A, James R, Chau NH, Karman MM, Panggalo LV, Wini L, Thanh NV, Obadia T, Satyagraha AW, Asih PBS, et al. Case Series of Primaquine-Induced Haemolytic Events in Controlled Trials with G6PD Screening. Pathogens. 2023; 12(9):1176. https://doi.org/10.3390/pathogens12091176
Chicago/Turabian StyleKosasih, Ayleen, Robert James, Nguyen Hoang Chau, Michelle M. Karman, Lydia Visita Panggalo, Lyndes Wini, Ngo Viet Thanh, Thomas Obadia, Ari Winasti Satyagraha, Puji Budi Setia Asih, and et al. 2023. "Case Series of Primaquine-Induced Haemolytic Events in Controlled Trials with G6PD Screening" Pathogens 12, no. 9: 1176. https://doi.org/10.3390/pathogens12091176