
Markers of Inflammation, Tissue Damage, and Fibrosis in Individuals Diagnosed with Human Immunodeficiency Virus and Pneumonia: A Cohort Study
 , , , , and
, , , , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Setting
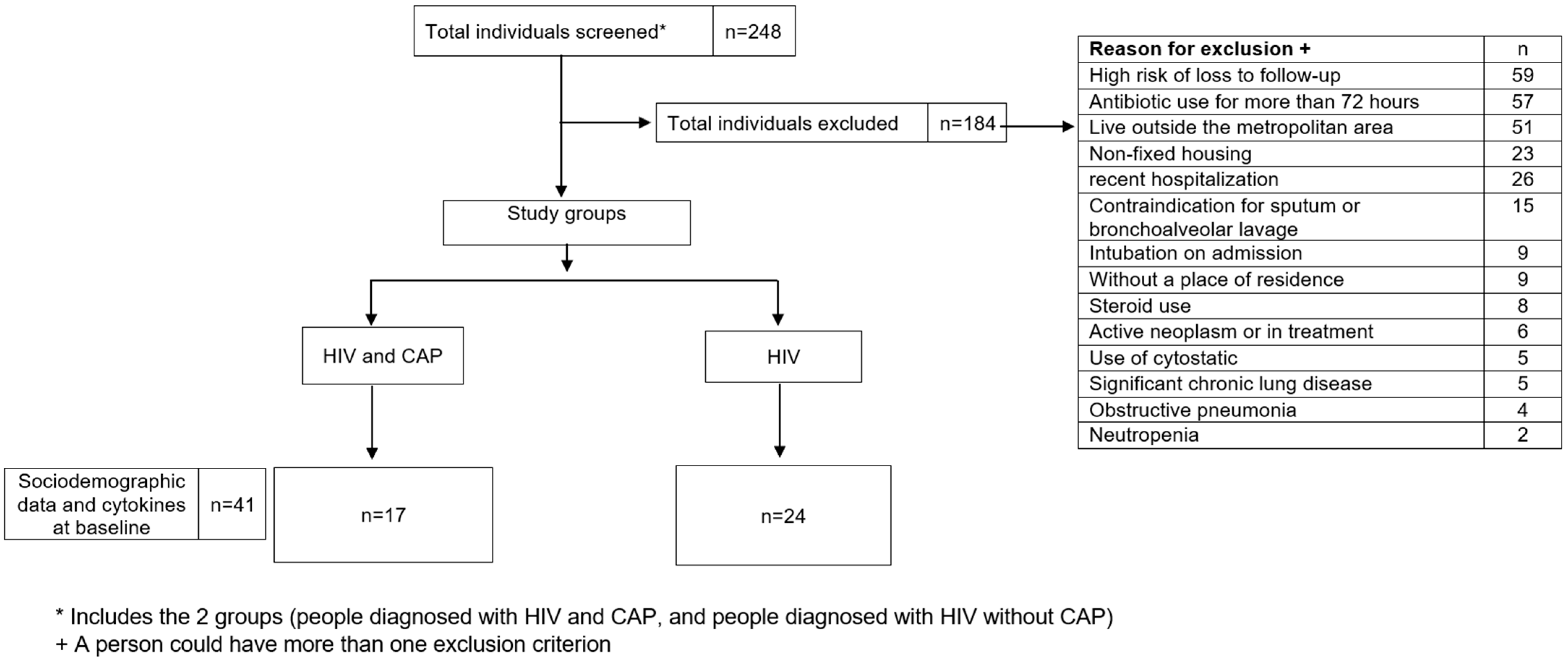
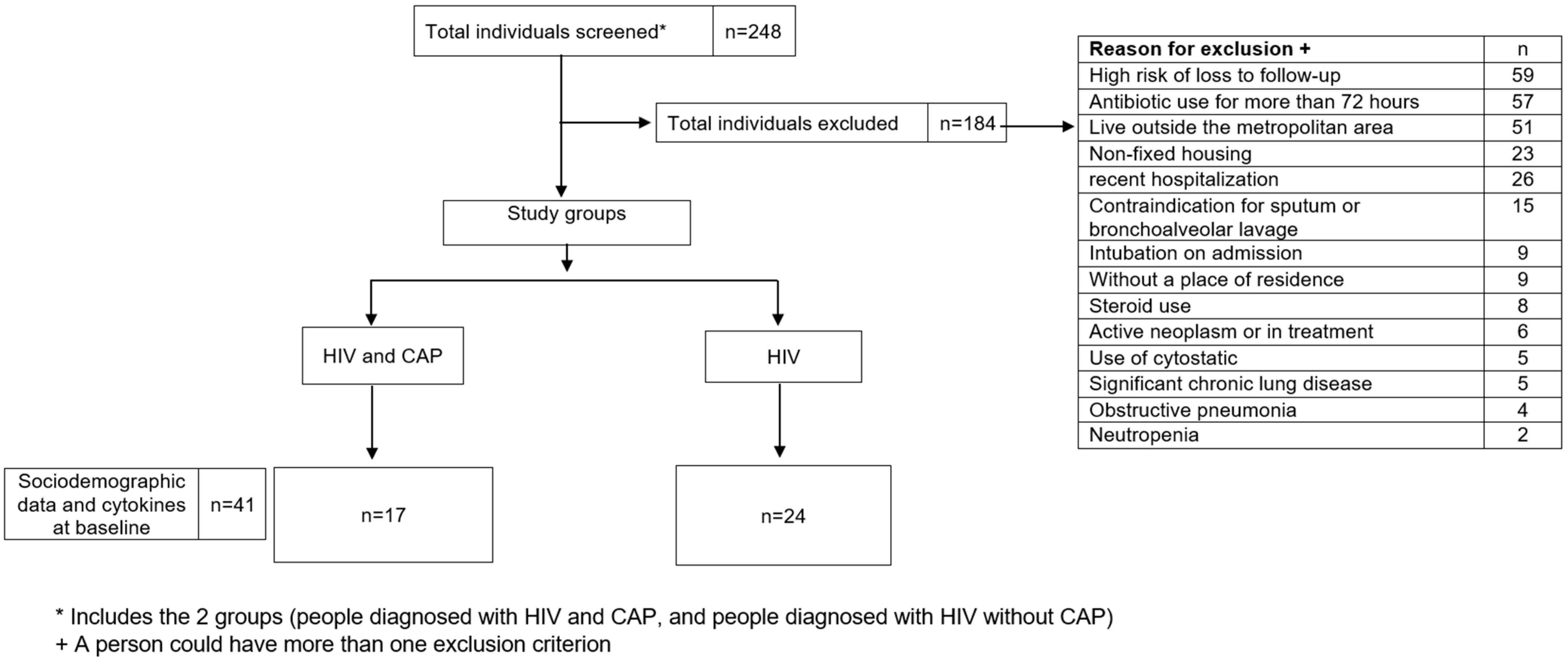
2.2. Participants
2.3. Eligibility Criteria
2.3.1. Inclusion Criteria
2.3.2. Exclusion Criteria
2.4. Definitions
2.4.1. Community-Acquired Pneumonia (CAP)
2.4.2. Human Immunodeficiency Virus (HIV) Infection
2.4.3. Pulmonary Dysfunction (Outcome)
2.4.4. FEF25 (Forced Expiratory Flow at 25% of the Forced Vital Capacity)
2.4.5. FEF25-75 (Forced Expiratory Flow between 25% and 75% of the Forced Vital Capacity)
2.4.6. FEV1 (Forced Expiratory Volume in 1 s)
2.5. Procedures
2.5.1. Admission
2.5.2. Blood Sample Collection
2.5.3. Spirometry
2.5.4. Data Collection
2.5.5. Cytokines and Chemokines Selection and Detection
2.6. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- WHO. Infección Por el VIH. Available online: https://www.who.int/es/news-room/fact-sheets/detail/hiv-aids (accessed on 13 March 2023).
- WHO. HIV. Available online: https://www.who.int/data/gho/data/themes/hiv-aids (accessed on 6 March 2023).
- KFF. The Global HIV/AIDS Epidemic. Available online: https://www.kff.org/global-health-policy/fact-sheet/the-global-hiv-aids-epidemic/ (accessed on 27 July 2023).
- Cuenta de Alto Costo (CAC). Día Mundial de Respuesta al VIH 2023; Cuenta de Alto Costo (CAC): Bogotá, Colombia, 2023; Available online: http://cuentadealtocosto.org/vih/dia-mundial-de-respuesta-al-vih-2023/ (accessed on 27 July 2023).
- UNAIDS Global HIV & AIDS Statistics—Fact Sheet. Available online: https://www.unaids.org/en/resources/fact-sheet (accessed on 13 March 2023).
- Cribbs, S.K.; Uppal, K.; Li, S.; Jones, D.P.; Huang, L.; Tipton, L.; Fitch, A.; Greenblatt, R.M.; Kingsley, L.; Guidot, D.M.; et al. Correlation of the Lung Microbiota with Metabolic Profiles in Bronchoalveolar Lavage Fluid in HIV Infection. Microbiome 2016, 4, 3. [Google Scholar] [CrossRef]
- Opportunistic Infections|Living with HIV|HIV Basics|HIV/AIDS|CDC. Available online: https://www.cdc.gov/hiv/basics/livingwithhiv/opportunisticinfections.html (accessed on 13 March 2023).
- Brune, K.A.; Ferreira, F.; Mandke, P.; Chau, E.; Aggarwal, N.R.; D’Alessio, F.R.; Lambert, A.A.; Kirk, G.; Blankson, J.; Drummond, M.B.; et al. HIV Impairs Lung Epithelial Integrity and Enters the Epithelium to Promote Chronic Lung Inflammation. PLoS ONE 2016, 11, e0149679. [Google Scholar] [CrossRef]
- Kristoffersen, U.S.; Lebech, A.-M.; Mortensen, J.; Gerstoft, J.; Gutte, H.; Kjaer, A. Changes in Lung Function of HIV-Infected Patients: A 4·5-Year Follow-up Study. Clin. Physiol. Funct. Imaging 2012, 32, 288–295. [Google Scholar] [CrossRef]
- Crothers, K.; Thompson, B.W.; Burkhardt, K.; Morris, A.; Flores, S.C.; Diaz, P.T.; Chaisson, R.E.; Kirk, G.D.; Rom, W.N.; Huang, L. HIV-Associated Lung Infections and Complications in the Era of Combination Antiretroviral Therapy. Proc. Am. Thorac. Soc. 2011, 8, 275–281. [Google Scholar] [CrossRef] [PubMed]
- Rendon, A.; Rendon-Ramirez, E.J.; Rosas-Taraco, A.G. Relevant Cytokines in the Management of Community-Acquired Pneumonia. Curr. Infect. Dis. Rep. 2016, 18, 10. [Google Scholar] [CrossRef]
- Fernandez-Botran, R.; Uriarte, S.M.; Arnold, F.W.; Rodriguez-Hernandez, L.; Rane, M.J.; Peyrani, P.; Wiemken, T.; Kelley, R.; Uppatla, S.; Cavallazzi, R.; et al. Contrasting Inflammatory Responses in Severe and Non-Severe Community-Acquired Pneumonia. Inflammation 2014, 37, 1158–1166. [Google Scholar] [CrossRef]
- Ravimohan, S.; Kornfeld, H.; Weissman, D.; Bisson, G.P. Tuberculosis and Lung Damage: From Epidemiology to Pathophysiology. Eur. Respir. Rev. 2018, 27, 170077. [Google Scholar] [CrossRef]
- Ngcobo, S.; Molatlhegi, R.P.; Osman, F.; Ngcapu, S.; Samsunder, N.; Garrett, N.J.; Abdool Karim, S.S.; Abdool Karim, Q.; McKinnon, L.R.; Sivro, A. Pre-Infection Plasma Cytokines and Chemokines as Predictors of HIV Disease Progression. Sci. Rep. 2022, 12, 2437. [Google Scholar] [CrossRef]
- American Psychiatric Association (Ed.) Guía de Consulta de los Criterios Diagnósticos del DSM-5; American Psychiatric Publishing: Arlington, VA, USA, 2014; ISBN 978-0-89042-551-0. [Google Scholar]
- Vogelmeier, C.F.; Criner, G.J.; Martinez, F.J.; Anzueto, A.; Barnes, P.J.; Bourbeau, J.; Celli, B.R.; Chen, R.; Decramer, M.; Fabbri, L.M.; et al. Global Strategy for the Diagnosis, Management, and Prevention of Chronic Obstructive Lung Disease 2017 Report: GOLD Executive Summary. Eur. Respir. J. 2017, 49, 557–582. [Google Scholar] [CrossRef]
- Vestbo, J.; Hurd, S.S.; Agustí, A.G.; Jones, P.W.; Vogelmeier, C.; Anzueto, A.; Barnes, P.J.; Fabbri, L.M.; Martinez, F.J.; Nishimura, M.; et al. Global Strategy for the Diagnosis, Management, and Prevention of Chronic Obstructive Pulmonary Disease. Am. J. Respir. Crit. Care Med. 2013, 187, 347–365. [Google Scholar] [CrossRef]
- Miller, M.R.; Hankinson, J.; Brusasco, V.; Burgos, F.; Casaburi, R.; Coates, A.; Crapo, R.; Enright, P.; van der Grinten, C.P.M.; Gustafsson, P.; et al. Standardisation of Spirometry. Eur. Respir. J. 2005, 26, 319–338. [Google Scholar] [CrossRef] [PubMed]
- David, S.; Edwards, C.W. Forced Expiratory Volume. In StatPearls; StatPearls Publishing: Treasure Island, FL, USA, 2022. [Google Scholar]
- Quanjer, P.H.; Tammeling, G.J.; Cotes, J.E.; Pedersen, O.F.; Peslin, R.; Yernault, J.-C. Lung Volumes and Forced Ventilatory Flows. Eur. Respir. J. 1993, 6, 5–40. [Google Scholar] [CrossRef]
- Hoesterey, D.; Das, N.; Janssens, W.; Buhr, R.G.; Martinez, F.J.; Cooper, C.B.; Tashkin, D.P.; Barjaktarevic, I. Spirometric Indices of Early Airflow Impairment in Individuals at Risk of Developing COPD: Spirometry beyond FEV1/FVC. Respir. Med. 2019, 156, 58–68. [Google Scholar] [CrossRef]
- Katz, S.; Arish, N.; Rokach, A.; Zaltzman, Y.; Marcus, E.-L. The Effect of Body Position on Pulmonary Function: A Systematic Review. BMC Pulm. Med. 2018, 18, 159. [Google Scholar] [CrossRef]
- Head, B.M.; Mao, R.; Keynan, Y.; Rueda, Z.V. Inflammatory mediators and lung abnormalities in HIV: A systematic review. PLoS ONE 2019, 14, e0226347. [Google Scholar] [CrossRef]
- Mao, R.; Trajtman, A.; Head, B.; Rodríguez Sabogal, I.A.; Cabrera, R.; Marín, D.; López, L.; Rodiño, J.; Aguilar, Y.; Herrera Díaz, M.; et al. Inflammatory Cell Differentiation and Chemotaxis and Extracellular Tissue Repair Markers Are Correlated with Pulmonary Dysfunction in HIV Infected Individuals Presenting with Community-Acquired Pneumonia. J. Interferon Cytokine Res. 2020, 40, 106–115. [Google Scholar] [CrossRef]
- Klatt, N.R.; Chomont, N.; Douek, D.C.; Deeks, S.G. Immune Activation and HIV Persistence: Implications for Curative Approaches to HIV Infection. Immunol. Rev. 2013, 254, 326–342. [Google Scholar] [CrossRef]
- Cribbs, S.K.; Crothers, K.; Morris, A. Pathogenesis of HIV-Related Lung Disease: Immunity, Infection, and Inflammation. Physiol. Rev. 2020, 100, 603–632. [Google Scholar] [CrossRef]
- Alexandrova, Y.; Costiniuk, C.T.; Jenabian, M.-A. Pulmonary Immune Dysregulation and Viral Persistence During HIV Infection. Front. Immunol. 2022, 12, 808722. [Google Scholar]
- Wiewel, M.A.; Huson, M.A.; van Vught, L.A.; Hoogendijk, A.J.; Klein Klouwenberg, P.M.C.; Horn, J.; Lutter, R.; Cremer, O.L.; Schultz, M.J.; Bonten, M.J.; et al. Impact of HIV Infection on the Presentation, Outcome and Host Response in Patients Admitted to the Intensive Care Unit with Sepsis; a Case Control Study. Crit. Care 2016, 20, 322. [Google Scholar] [CrossRef]
- Keynan, Y.; Rueda, Z.V.; Aguilar, Y.; Trajtman, A.; Vélez, L.A. Unique Cytokine and Chemokine Patterns in Bronchoalveolar Lavage Are Associated with Specific Causative Pathogen among HIV Infected Patients with Pneumonia, in Medellin, Colombia. Cytokine 2015, 73, 295–301. [Google Scholar] [CrossRef] [PubMed]
- Wang, R.J.; Moore, J.; Moisi, D.; Chang, E.G.; Byanyima, P.; Kaswabuli, S.; Musisi, E.; Sanyu, I.; Sessolo, A.; Lalitha, R.; et al. HIV Infection Is Associated with Elevated Biomarkers of Immune Activation in Ugandan Adults with Pneumonia. PLoS ONE 2019, 14, e0216680. [Google Scholar] [CrossRef] [PubMed]
- Tanaka, T.; Narazaki, M.; Kishimoto, T. IL-6 in Inflammation, Immunity, and Disease. Cold Spring Harb. Perspect. Biol. 2014, 6, a016295. [Google Scholar] [CrossRef] [PubMed]
- Scheller, J.; Chalaris, A.; Schmidt-Arras, D.; Rose-John, S. The Pro- and Anti-Inflammatory Properties of the Cytokine Interleukin-6. Biochim. Biophys. Acta 2011, 1813, 878–888. [Google Scholar] [CrossRef]
- Velazquez-Salinas, L.; Verdugo-Rodriguez, A.; Rodriguez, L.L.; Borca, M.V. The Role of Interleukin 6 During Viral Infections. Front. Microbiol. 2019, 10, 1057. [Google Scholar]
- Saylor, D.; Kumar, A.; Nakigozi, G.; Anok, A.; Batte, J.; Kisakye, A.; Mayanja, R.; Nakasujja, N.; Robertson, K.R.; Gray, R.H.; et al. Interleukin-6 Is Associated with Mortality and Neuropsychiatric Outcomes in Antiretroviral-Naïve Adults in Rakai, Uganda. J. Neurovirol. 2019, 25, 735–740. [Google Scholar] [CrossRef]
- Martínez, R.; Menéndez, R.; Reyes, S.; Polverino, E.; Cillóniz, C.; Martínez, A.; Esquinas, C.; Filella, X.; Ramírez, P.; Torres, A. Factors Associated with Inflammatory Cytokine Patterns in Community-Acquired Pneumonia. Eur. Respir. J. 2011, 37, 393–399. [Google Scholar] [CrossRef] [PubMed]
- Antunes, G.; Evans, S.A.; Lordan, J.L.; Frew, A.J. Systemic Cytokine Levels in Community-Acquired Pneumonia and Their Association with Disease Severity. Eur. Respir. J. 2002, 20, 990–995. [Google Scholar] [CrossRef]
- Dao, B.N.; Le, H.D.T.; Nguyen, K.X.; Viet, T.T.; Tran, C.T.; Luong, T.C.; Le, T.D.; Nguyen, S.T.; Vu, H.N.; Pham, N.T.K.; et al. Relationship between Serum TNF-α, IL-6, and IL-10 Levels and Disease Severity, and Changes in the Cytokines after Treatment in Patients with Bacterial Community-Acquired Pneumonia. Pneumon 2023, 36, 27. [Google Scholar] [CrossRef]
- Bernhard, S.; Hug, S.; Stratmann, A.E.P.; Erber, M.; Vidoni, L.; Knapp, C.L.; Thomaß, B.D.; Fauler, M.; Nilsson, B.; Nilsson Ekdahl, K.; et al. Interleukin 8 Elicits Rapid Physiological Changes in Neutrophils That Are Altered by Inflammatory Conditions. J. Innate Immun. 2021, 13, 225–241. [Google Scholar] [CrossRef]
- Taylor, G.H.; Williams, A.A.; Garzino-Demo, A. Highly Active Antiretroviral Therapy Reduces Pulmonary IL-8 in HIV-Positive Women Smokers. Pathog. Dis. 2016, 74, ftv115. [Google Scholar] [CrossRef] [PubMed]
- Iyer, S.S.; Cheng, G. Role of Interleukin 10 Transcriptional Regulation in Inflammation and Autoimmune Disease. Crit. Rev. Immunol. 2012, 32, 23–63. [Google Scholar]
- Steen, E.H.; Wang, X.; Balaji, S.; Butte, M.J.; Bollyky, P.L.; Keswani, S.G. The Role of the Anti-Inflammatory Cytokine Interleukin-10 in Tissue Fibrosis. Adv. Wound Care 2020, 9, 184–198. [Google Scholar] [CrossRef]
- Carlini, V.; Noonan, D.M.; Abdalalem, E.; Goletti, D.; Sansone, C.; Calabrone, L.; Albini, A. The Multifaceted Nature of IL-10: Regulation, Role in Immunological Homeostasis and Its Relevance to Cancer, COVID-19 and Post-COVID Conditions. Front. Immunol. 2023, 14, 1161067. [Google Scholar] [CrossRef] [PubMed]
- Rojas, J.M.; Avia, M.; Martín, V.; Sevilla, N. IL-10: A Multifunctional Cytokine in Viral Infections. J. Immunol. Res. 2017, 2017, 6104054. [Google Scholar] [CrossRef]
- Redford, P.S.; Murray, P.J.; O’Garra, A. The Role of IL-10 in Immune Regulation during M. Tuberculosis Infection. Mucosal Immunol. 2011, 4, 261–270. [Google Scholar] [CrossRef]
- Freeman, M.L.; Shive, C.L.; Nguyen, T.P.; Younes, S.-A.; Panigrahi, S.; Lederman, M.M. Cytokines and T-Cell Homeostasis in HIV Infection. J. Infect. Dis. 2016, 214, S51–S57. [Google Scholar] [CrossRef] [PubMed]
- Baidya, A.; Sangle, S.; Marbaniang, I.; Kulkarni, V.; Deshpande, P.; Nimkar, S.; Chavan, A.; Salvi, S.; Lokhande, R.; Kadam, D.; et al. Clinical and Immunological Markers of Pulmonary Impairment Among People with HIV in India. Open Forum Infect. Dis. 2022, 9, ofac233. [Google Scholar] [CrossRef]
- Tahtinen, S.; Tong, A.-J.; Himmels, P.; Oh, J.; Paler-Martinez, A.; Kim, L.; Wichner, S.; Oei, Y.; McCarron, M.J.; Freund, E.C.; et al. IL-1 and IL-1ra Are Key Regulators of the Inflammatory Response to RNA Vaccines. Nat. Immunol. 2022, 23, 532–542. [Google Scholar] [CrossRef]
- Nosik, M.; Ryzhov, K.; Rymanova, I.; Sobkin, A.; Kravtchenko, A.; Kuimova, U.; Pokrovsky, V.; Zverev, V.; Svitich, O. Dynamics of Plasmatic Levels of Pro- and Anti-Inflammatory Cytokines in HIV-Infected Individuals with M. Tuberculosis Co-Infection. Microorganisms 2021, 9, 2291. [Google Scholar] [CrossRef]
- Dinarello, C.A. Overview of the IL-1 Family in Innate Inflammation and Acquired Immunity. Immunol. Rev. 2018, 281, 8–27. [Google Scholar] [CrossRef]
- Jambo, K.C.; Tembo, D.L.; Kamng’ona, A.W.; Musicha, P.; Banda, D.H.; Kankwatira, A.M.; Malamba, R.D.; Allain, T.J.; Heyderman, R.S.; Russell, D.G.; et al. HIV-Associated Disruption of Lung Cytokine Networks Is Incompletely Restored in Asymptomatic HIV-Infected Malawian Adults on Antiretroviral Therapy. ERJ Open Res. 2017, 3, 00097-2017. [Google Scholar] [CrossRef]
- Ihim, S.A.; Abubakar, S.D.; Zian, Z.; Sasaki, T.; Saffarioun, M.; Maleknia, S.; Azizi, G. Interleukin-18 Cytokine in Immunity, Inflammation, and Autoimmunity: Biological Role in Induction, Regulation, and Treatment. Front. Immunol. 2022, 13, 919973. [Google Scholar] [CrossRef]
- Park, S.Y.; Hisham, Y.; Shin, H.M.; Yeom, S.C.; Kim, S. Interleukin-18 Binding Protein in Immune Regulation and Autoimmune Diseases. Biomedicines 2022, 10, 1750. [Google Scholar] [CrossRef]
- Shimizu, M.; Takei, S.; Mori, M.; Yachie, A. Pathogenic Roles and Diagnostic Utility of Interleukin-18 in Autoinflammatory Diseases. Front. Immunol. 2022, 13, 951535. [Google Scholar] [CrossRef]
- Bordon, J.; Aliberti, S.; Fernandez-Botran, R.; Uriarte, S.M.; Rane, M.J.; Duvvuri, P.; Peyrani, P.; Morlacchi, L.C.; Blasi, F.; Ramirez, J.A. Understanding the Roles of Cytokines and Neutrophil Activity and Neutrophil Apoptosis in the Protective versus Deleterious Inflammatory Response in Pneumonia. Int. J. Infect. Dis. IJID 2013, 17, e76–e83. [Google Scholar] [CrossRef]
- Lin, W.; Li, L.; Guo, P.; He, Y.; He, H.; Li, H.; Zhong, H.; Liu, C.; Du, P.; Cai, W.; et al. Early On-Treatment Plasma Interleukin-18 as a Promising Indicator for Long-Term Virological Response in Patients with HIV-1 Infection. Front. Med. 2023, 10, 1170208. [Google Scholar]
- Liu, M.; Guo, S.; Hibbert, J.M.; Jain, V.; Singh, N.; Wilson, N.O.; Stiles, J.K. CXCL10/IP-10 in Infectious Diseases Pathogenesis and Potential Therapeutic Implications. Cytokine Growth Factor Rev. 2011, 22, 121–130. [Google Scholar] [CrossRef]
- Samaras, C.; Kyriazopoulou, E.; Poulakou, G.; Reiner, E.; Kosmidou, M.; Karanika, I.; Petrakis, V.; Adamis, G.; Gatselis, N.K.; Fragkou, A.; et al. Interferon Gamma-Induced Protein 10 (IP-10) for the Early Prognosis of the Risk for Severe Respiratory Failure and Death in COVID-19 Pneumonia. Cytokine 2023, 162, 156111. [Google Scholar] [CrossRef]
- Deshmane, S.L.; Kremlev, S.; Amini, S.; Sawaya, B.E. Monocyte Chemoattractant Protein-1 (MCP-1): An Overview. J. Interferon Cytokine Res. 2009, 29, 313–326. [Google Scholar] [CrossRef] [PubMed]
- Singh, S.; Anshita, D.; Ravichandiran, V. MCP-1: Function, Regulation, and Involvement in Disease. Int. Immunopharmacol. 2021, 101, 107598. [Google Scholar] [CrossRef]
- Sui, Y.; Li, S.; Pinson, D.; Adany, I.; Li, Z.; Villinger, F.; Narayan, O.; Buch, S. Simian Human Immunodeficiency Virus-Associated Pneumonia Correlates with Increased Expression of MCP-1, CXCL10, and Viral RNA in the Lungs of Rhesus Macaques. Am. J. Pathol. 2005, 166, 355–365. [Google Scholar] [CrossRef]
- Chaisavaneeyakorn, S.; Moore, J.M.; Mirel, L.; Othoro, C.; Otieno, J.; Chaiyaroj, S.C.; Shi, Y.P.; Nahlen, B.L.; Lal, A.A.; Udhayakumar, V. Levels of Macrophage Inflammatory Protein 1α (MIP-1α) and MIP-1β in Intervillous Blood Plasma Samples from Women with Placental Malaria and Human Immunodeficiency Virus Infection. Clin. Diagn. Lab. Immunol. 2003, 10, 631–636. [Google Scholar] [CrossRef]
- Cocchi, F.; DeVico, A.L.; Yarchoan, R.; Redfield, R.; Cleghorn, F.; Blattner, W.A.; Garzino-Demo, A.; Colombini-Hatch, S.; Margolis, D.; Gallo, R.C. Higher Macrophage Inflammatory Protein (MIP)-1α and MIP-1β Levels from CD8+ T Cells Are Associated with Asymptomatic HIV-1 Infection. Proc. Natl. Acad. Sci. USA 2000, 97, 13812–13817. [Google Scholar] [CrossRef]
- Van de Wijer, L.; van der Heijden, W.A.; ter Horst, R.; Jaeger, M.; Trypsteen, W.; Rutsaert, S.; van Cranenbroek, B.; van Rijssen, E.; Joosten, I.; Joosten, L.; et al. The Architecture of Circulating Immune Cells Is Dysregulated in People Living with HIV on Long Term Antiretroviral Treatment and Relates with Markers of the HIV-1 Reservoir, Cytomegalovirus, and Microbial Translocation. Front. Immunol. 2021, 12, 661990. [Google Scholar] [CrossRef]
- Höft, M.A.; Burgers, W.A.; Riou, C. The Immune Response to SARS-CoV-2 in People with HIV. Cell. Mol. Immunol. 2023, 11, 1–13. [Google Scholar] [CrossRef]
- Sarkar, S.; Brown, T.T. CROI 2023: Metabolic and Other Complications of HIV Infection. Top. Antivir. Med. 2023, 31, 538–542. [Google Scholar]
- Gingo, M.R.; Nouraie, M.; Kessinger, C.J.; Greenblatt, R.M.; Huang, L.; Kleerup, E.C.; Kingsley, L.; McMahon, D.K.; Morris, A. Decreased Lung Function and All-Cause Mortality in HIV-Infected Individuals. Ann. Am. Thorac. Soc. 2018, 15, 192–199. [Google Scholar] [CrossRef]
- Varkila, M.R.J.; Vos, A.G.; Barth, R.E.; Tempelman, H.A.; Devillé, W.L.J.; Coutinho, R.A.; Grobbee, D.E.; Klipstein-Grobusch, K. The Association between HIV Infection and Pulmonary Function in a Rural African Population. PLoS ONE 2019, 14, e0210573. [Google Scholar] [CrossRef]
- North, C.M.; Allen, J.G.; Okello, S.; Sentongo, R.; Kakuhikire, B.; Ryan, E.T.; Tsai, A.C.; Christiani, D.C.; Siedner, M.J. HIV Infection, Pulmonary Tuberculosis and COPD in Rural Uganda: A Cross-Sectional Study. Lung 2018, 196, 49–57. [Google Scholar] [CrossRef]
- Morris, A.M.; Huang, L.; Bacchetti, P.; Turner, J.; Hopewell, P.C.; Wallace, J.M.; Kvale, P.A.; Rosen, M.J.; Glassroth, J.; Reichman, L.B.; et al. Permanent Declines in Pulmonary Function Following Pneumonia in Human Immunodeficiency Virus-Infected Persons. The Pulmonary Complications of HIV Infection Study Group. Am. J. Respir. Crit. Care Med. 2000, 162, 612–616. [Google Scholar] [CrossRef]
- Ronit, A.; Lundgren, J.; Afzal, S.; Benfield, T.; Roen, A.; Mocroft, A.; Gerstoft, J.; Nordestgaard, B.G.; Vestbo, J.; Nielsen, S.D.; et al. Airflow Limitation in People Living with HIV and Matched Uninfected Controls. Thorax 2018, 73, 431–438. [Google Scholar] [CrossRef]
- Popescu, I.; Drummond, M.B.; Gama, L.; Coon, T.; Merlo, C.A.; Wise, R.A.; Clements, J.E.; Kirk, G.D.; McDyer, J.F. Activation-Induced Cell Death Drives Profound Lung CD4(+) T-Cell Depletion in HIV-Associated Chronic Obstructive Pulmonary Disease. Am. J. Respir. Crit. Care Med. 2014, 190, 744–755. [Google Scholar] [CrossRef]
- Barratt, S.L.; Flower, V.A.; Pauling, J.D.; Millar, A.B. VEGF (Vascular Endothelial Growth Factor) and Fibrotic Lung Disease. Int. J. Mol. Sci. 2018, 19, 1269. [Google Scholar] [CrossRef]
- Thudium, R.F.; Arentoft, N.S.; Hoel, H.; Afzal, S.; von Stemann, J.H.; Forman, J.L.; Wilcke, J.T.; Benfield, T.; Trøseid, M.; Borges, Á.H.; et al. Elevated Levels of Interleukin-1β and Interleukin-10 Are Associated with Faster Lung Function Decline in People with Well-Treated Human Immunodeficiency Virus. J. Infect. Dis. 2023, 228, 1080–1088. [Google Scholar] [CrossRef]
- Kolb, M.; Margetts, P.J.; Anthony, D.C.; Pitossi, F.; Gauldie, J. Transient Expression of IL-1β Induces Acute Lung Injury and Chronic Repair Leading to Pulmonary Fibrosis. J. Clin. Invest. 2001, 107, 1529–1536. [Google Scholar] [CrossRef]
- Liu, B.; Totten, M.; Nematollahi, S.; Datta, K.; Memon, W.; Marimuthu, S.; Wolf, L.A.; Carroll, K.C.; Zhang, S.X. Development and Evaluation of a Fully Automated Molecular Assay Targeting the Mitochondrial Small Subunit rRNA Gene for the Detection of Pneumocystis Jirovecii in Bronchoalveolar Lavage Fluid Specimens. J. Mol. Diagn. JMD 2020, 22, 1482–1493. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Groups | ||||||
|---|---|---|---|---|---|---|
| Variable | HIV and CAP (n = 17) | HIV (n = 24) | p-Value | |||
| n | % | n | % | |||
| Sex | Female | 5 | 29.4 | 3 | 12.5 | 0.178 |
| Male | 12 | 70.6 | 21 | 87.5 | ||
| Age, years | <24.9 | 2 | 11.8 | 3 | 12.5 | 0.943 |
| 25–64 | 15 | 88.2 | 21 | 87.5 | ||
| BMI (kg/m2) | 18.5 | 10 | 62.5 | 1 | 8.3 | 0.001 * |
| 18.51–24.99 | 5 | 31.3 | 16 | 66.7 | ||
| >24 | 1 | 6.3 | 6 | 25.0 | ||
| Taken antibiotics in the last 3 months | 2/3 | 66.7 | 5/5 | 100.0 | 0.168 | |
| Inhaling drugs used in the last month | 1/17 | 5.9 | 2/24 | 8.3 | 0.767 | |
| Smoking drugs used in the last month | 2/17 | 11.8 | 5/24 | 20.8 | 0.447 | |
| Cigarettes used in the last month | 4 | 23.5 | 9 | 37.5 | 0.344 | |
| Liquor consumption in the last month | 6/17 | 35.3 | 13/24 | 54.2 | 0.233 | |
| Cigarettes/day | <5 | 15 | 88.2 | 17 | 70.8 | 0.319 |
| 6–15 | 2 | 11.8 | 5 | 20.8 | ||
| >16 | 0 | 0.0 | 2 | 8.3 | ||
| Diabetes | 1 | 5.9 | 1 | 4.2 | 0.802 | |
| Chronic renal injury | 0 | 0.0 | 2 | 8.3 | 0.222 | |
| Congestive cardiac failure | 0 | 0.0 | 2 | 8.3 | 0.222 | |
| Microbiological diagnosis | Bacteria | 5 | 33.3 | 0 | 0.0 | 0.0352 * |
| Mycobacterium tuberculosis | 7 | 46.7 | 3 | 12.5 | ||
| Mycosis | 3 | 20.0 | 1 | 25.0 | ||
| CD4 count < 200 (cells/µL) | 10/15 | 66.7 | 7/23 | 30.4 | 0.003 * | |
| Viral load > 100,000 (copies/µL) | 6/16 | 37.5 | 6/16 | 37.5 | 1.000 | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Peña-Valencia, K.; Riaño, W.; Herrera-Diaz, M.; López, L.; Marín, D.; Gonzalez, S.; Agudelo-García, O.; Rodríguez-Sabogal, I.A.; Vélez, L.; Rueda, Z.V.; et al. Markers of Inflammation, Tissue Damage, and Fibrosis in Individuals Diagnosed with Human Immunodeficiency Virus and Pneumonia: A Cohort Study. Pathogens 2024, 13, 84. https://doi.org/10.3390/pathogens13010084
Peña-Valencia K, Riaño W, Herrera-Diaz M, López L, Marín D, Gonzalez S, Agudelo-García O, Rodríguez-Sabogal IA, Vélez L, Rueda ZV, et al. Markers of Inflammation, Tissue Damage, and Fibrosis in Individuals Diagnosed with Human Immunodeficiency Virus and Pneumonia: A Cohort Study. Pathogens. 2024; 13(1):84. https://doi.org/10.3390/pathogens13010084
Chicago/Turabian StylePeña-Valencia, Katherine, Will Riaño, Mariana Herrera-Diaz, Lucelly López, Diana Marín, Sandra Gonzalez, Olga Agudelo-García, Iván Arturo Rodríguez-Sabogal, Lázaro Vélez, Zulma Vanessa Rueda, and et al. 2024. "Markers of Inflammation, Tissue Damage, and Fibrosis in Individuals Diagnosed with Human Immunodeficiency Virus and Pneumonia: A Cohort Study" Pathogens 13, no. 1: 84. https://doi.org/10.3390/pathogens13010084