
Acute Hepatitis of Unknown Origin in Children: Analysis of 17 Cases Admitted to the Bambino Gesù Children’s Hospital in Rome
 , , , , , , ,
, , , , , , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Patients
2.2. Laboratory Testing
2.2.1. Nucleic Acid Amplification Tests (NAATs) and Antigen Test
2.2.2. Serologic Tests
2.3. Statistical Analysis
3. Results
3.1. Demographics and Clinical Characteristics
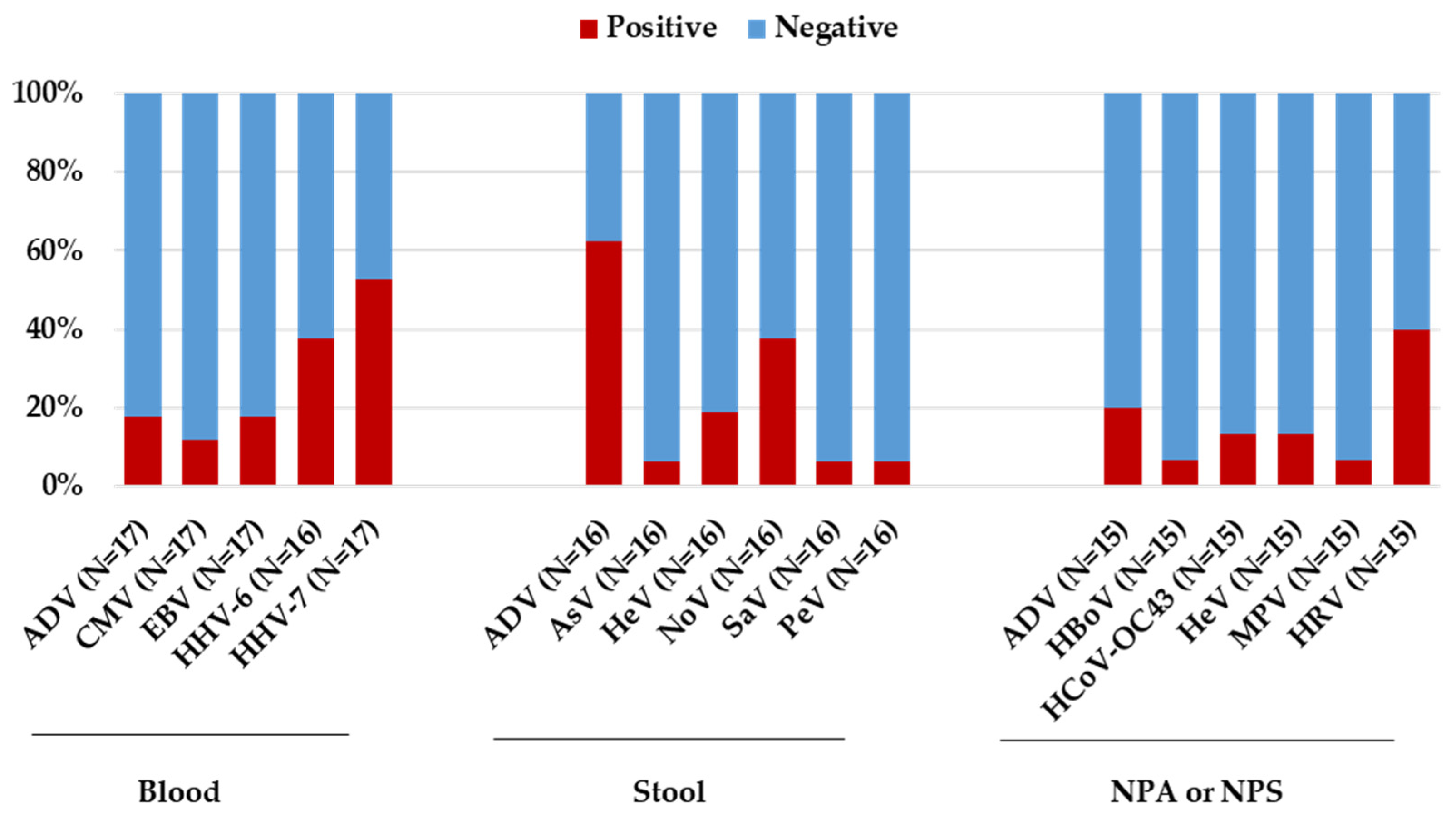
3.2. Laboratory Investigation Results
3.3. Analysis of HHV-6 and HHV-7 Prevalence
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
References
- GOV.UK. Investigation into Acute Hepatitis of Unknown Aetiology in Children in England: Case Update. 2022. Available online: https://www.gov.uk/government/publications/acute-hepatitis-technical-briefing/investigation-into-acute-hepatitis-of-unknown-aetiology-in-children-in-england-case-update (accessed on 27 February 2024).
- Di Dato, F.; Di Giorgio, A.; Mandato, C.; Maggiore, G.; Iorio, R.; Aloi, M.; Antonucci, R.; Banzato, C.; Buccella, V.; Calvo, P.L.; et al. SIGENP Acute Hepatitis Group. Italian children seem to be spared from the mysterious severe acute hepatitis outbreak: A report by SIGENP Acute Hepatitis Group. J. Hepatol. 2022, 77, 1211–1213. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Disease Outbreak News; Acute Hepatitis of Unknown Aetiology in Children—Multi-Country. 12 July 2022. Available online: https://www.who.int/emergencies/disease-outbreak-news/item/2022-DON400 (accessed on 27 February 2024).
- Ho, A.; Orton, R.; Tayler, R.; Asamaphan, P.; Herder, V.; Davis, C.; Tong, L.; Smollett, K.; Manali, M.; Allan, J.; et al. Adeno-associated virus 2 infection in children with non-A-E hepatitis. Nature 2023, 617, 555–563. [Google Scholar] [CrossRef] [PubMed]
- Morfopoulou, S.; Buddle, S.; Montaguth, O.E.T.; Atkinson, L.; Guerra-Assunção, J.A.; Marjaneh, M.M.; Chiozzi, R.Z.; Storey, N.; Campos, L.; Hutchinson, J.C.; et al. Genomic investigations of acute hepatitis of unknown aetiology in children. Nature 2023, 617, 564–573. [Google Scholar] [CrossRef] [PubMed]
- Servellita, V.; Gonzalez, A.S.; Lamson, D.M.; Foresythe, A.; Huh, H.J.; Bazinet, A.L.; Bergman, N.H.; Bull, R.L.; Garcia, K.Y.; Goodrich, J.S.; et al. Adeno-associated virus type 2 in US children with acute severe hepatitis. Nature 2023, 617, 574–580. [Google Scholar] [CrossRef] [PubMed]
- Matthews, P.C.; Campbell, C.; Săndulescu, O.; Matičič, M.; Ruta, S.M.; Rivero-Juárez, A.; van Welzen, B.J.; Tan, B.K.; Garcia, F.; Gherlan, G.S.; et al. Acute severe hepatitis outbreak in children: A perfect storm. What do we know, and what questions remain? Front. Pharmacol. 2022, 13, 1062408. [Google Scholar] [CrossRef]
- European Centre for Disease Prevention and Control. Available online: https://www.ecdc.europa.eu/sites/default/files/documents/Guidance_Testing_Hepatitis_FINAL.pdf (accessed on 27 February 2024).
- Baker, J.M.; Buchfellner, M.; Britt, W.; Sanchez, V.; Potter, J.L.; Ingram, L.A.; Shiau, H.; Sanchez, L.H.G.; Saaybi, S.; Kelly, D.; et al. Acute hepatitis and adenovirus infection among children—Alabama, October 2021–February 2022. MMWR Morb. Mortal. Wkly. Rep. 2022, 71, 638–640. [Google Scholar] [CrossRef] [PubMed]
- de Kleine, R.H.; Lexmond, W.S.; Buescher, G.; Sturm, E.; Kelly, D.; Lohse, A.W.; Lenz, D.; Jørgensen, M.H. Severe acute hepatitis and acute liver failure of unknown origin in children: A questionnaire-based study within 34 paediatric liver centres in 22 European countries and Israel, April 2022. Eurosurveillance 2022, 27, 2200369. [Google Scholar] [CrossRef]
- Kelgeri, C.; Couper, M.; Gupte, G.L.; Brant, A.; Patel, M.; Johansen, L.; Valamparampil, J.; Ong, E.; Hartog, H.; Perera, M.; et al. Clinical spectrum of children with acute hepatitis of unknown cause. N. Engl. J. Med. 2022, 387, 611–619. [Google Scholar] [CrossRef] [PubMed]
- ECDC. Epidemiological Update Issued 25 November 2022: Hepatitis of Unknown Aetiology in Children. European Centre for Disease Prevention and Control: Stockholm, Sweden, 2022; Available online: https://www.ecdc.europa.eu/en/hepatitis/joint-hepatitis-unknown-origin-children-surveillance-bulletin (accessed on 27 February 2024).
- Center for Disease Control and Prevention. Technical Report: Acute Hepatitis of Unknown Cause. 2022. Available online: https://www.cdc.gov/ncird/investigation/hepatitis-unknown-cause/technical-report.html (accessed on 27 February 2024).
- UK Health Security Agency. Investigation into Acute Hepatitis of Unknown Aetiology in Children in England: Technical Briefing 4. 2022. Available online: https://assets.publishing.service.gov.uk/government/uploads/system/uploads/attachment_data/file/1094573/acute-hepatitis-technical-briefing-4.pdf (accessed on 27 February 2024).
- Crenshaw, B.J.; Jones, L.B.; Bell, C.R.; Kumar, S.; Matthews, Q.L. Perspective on Adenoviruses: Epidemiology, Pathogenicity, and Gene Therapy. Biomedicines 2019, 19, 61. [Google Scholar] [CrossRef]
- Ronan, B.A.; Agrwal, N.; Carey, E.J.; De Petris, G.; Kusne, S.; Seville, M.T.; Blair, J.E.; Vikram, H.R. Fulminant hepatitis due to human adenovirus. Infection 2014, 42, 105–111. [Google Scholar] [CrossRef]
- Munoz, F.M.; Piedra, P.A.; Demmler, G.J. Disseminated adenovirus disease in immunocompromised and immunocompetent children. Clin. Infect. Dis. 1998, 27, 1194–1200. [Google Scholar] [CrossRef] [PubMed]
- Hoşnut, F.O.; Canan, O.; Ozçay, F.; Bilezikçi, B. Adenovirus infection as possible cause of acute liver failure in a healthy child: A case report. Turk. J. Gastroenterol. 2008, 19, 281–283. [Google Scholar]
- Peled, N.; Nakar, C.; Huberman, H.; Scherf, E.; Samra, Z.; Finkelstein, Y.; Hoffer, V.; Garty, B.-Z. Adenovirus infection in hospitalized immunocompetent children. Clin. Pediatr. 2004, 43, 223–229. [Google Scholar] [CrossRef] [PubMed]
- Rocholl, C.; Gerber, K.; Daly, J.; Pavia, A.T.; Byington, C.L. Adenoviral infections in children: The impact of rapid diagnosis. Pediatrics 2004, 113 Pt 1, e51–e56. [Google Scholar] [CrossRef] [PubMed]
- Kambhampati, A.K.; Burke, R.M.; Dietz, S.; Sheppard, M.; Almendares, O.; Baker, J.M.; Cates, J.; Stein, Z.; Johns, D.; Smith, A.R.; et al. Trends in acute hepatitis of unspecified etiology and adenovirus stool testing results in children—United States, 2017–2022. MMWR Morb. Mortal. Wkly. Rep. 2022, 71, 797–802. [Google Scholar] [CrossRef] [PubMed]
- Brodin, P. SARS-CoV-2 infections in children: Understanding diverse outcomes. Immunity 2022, 55, 201–209. [Google Scholar] [CrossRef] [PubMed]
- Brodin, P.; Arditi, M. Severe acute hepatitis in children: Investigate SARS-CoV-2 superantigens. Gastroenterol. Hepatol. 2022, 7, 594–595. [Google Scholar] [CrossRef] [PubMed]
- Paraskevis, D.; Papatheodoridis, G.; Sypsa, V.; Sfikakis, P.; Tsiodras, S.; Zaoutis, T. A proposed etiology for an aberrant response to enteric adenovirus infection in previously SARS-CoV-2-infected children with acute hepatitis. J. Pediatr. Infect. Dis. Soc. 2022, 11, 352–353. [Google Scholar] [CrossRef] [PubMed]
- Hashida, T.; Komura, E.; Yoshida, M.; Otsuka, T.; Hibi, S.; Imashuku, S.; Ishizaki, T.; Yamada, A.; Suga, S.; Asano, Y. Hepatitis in association with human herpesvirus-7 infection. Pediatrics 1995, 96, 783–785. [Google Scholar] [CrossRef]
- Somasekar, S.; Lee, D.; Rule, J.; Naccache, S.N.; Stone, M.; Busch, M.P.; Sanders, C.; Lee, W.M.; Chiu, C.Y. Viral surveillance in serum samples from patients with acute liver failure by metagenomic next-generation sequencing. Clin. Infect. Dis. 2017, 65, 1477–1485. [Google Scholar] [CrossRef]
- Mücke, M.M.; Zeuzem, S. The recent outbreak of acute severe hepatitis in children of unknown origin—What is known so far. J. Hepatol. 2022, 77, 237–242. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Pathogens | |
|---|---|
| Blood (whole or serum) | |
| Serology | ADV, CMV, EBV, HAV, HBV, HCV, HDV, HEV, HHV-6, HIV, HSV-1/2, PB19, SARS-CoV-2 anti-S and anti-N, VZV |
| NAAT | ADV, CMV, EBV, HAV, HBV, HCV, HDV, HEV, HeV, HHV-6 and 7, HSV-1/2, PB19 |
| Nasopharyngeal swab or nasopharyngeal aspirate | |
| NAAT | Respiratory viruses screening by multiplex panel assay (including ADV, Flu A, Flu B, HBoV, HCoV-229E, HCoV-NL63, HCoV-OC43, HeV, HRV, PIV 1,2,3 and 4, RSV A and B) SARS-CoV-2 |
| Antigen | SARS-CoV-2 |
| Stool | |
| NAAT | Enteric viruses and bacteria screening by multiplex panel assay (including ADV, Aer, AstV, Cam, CD hyper, CdB, E. coli O157, EAEC, EHEC, EPEC, ETEC, NoV-GI and GII, RotV, Sal, EIEC/Sh, SaV, Yer) HPeV, HeV |
| Pediatric patients, N | 17 |
| Gender, N (%) | |
| Male | 10 (58.8) |
| Female | 7 (41.2) |
| Age (years), Median (IQR) | 2.1 (1.0–7.1) |
| Liver function index U/L, Median (IQR) | |
| ALT | 801 (616–1163) |
| AST | 489 (315–1011) |
| LDH | 518 (417–665) |
| Clinical sign/symptoms, N (%) | |
| Fever | 9 (52.9) |
| Diarrhea | 5 (29.4) |
| Vomiting | 6 (35.3) |
| Jaundice | 4 (23.5) |
| Upper respiratory symptoms † | 4 (23.5) |
| Length of hospitalization (days), Median (IQR) | 9.0 (5.8–16.8) |
| Outcome, N (%) | |
| Hospital discharge without clinical complications | 16 (94.1) |
| Liver Transplantation | 1 (5.9) |
| Death | 0 (0.0) |
| Type of Sample | Pathogen | No. Positive Tests/ No. of Total Specimens Tested (%) |
|---|---|---|
| Blood | ||
| Adenovirus group † | 3/17 (17.6) | |
| Cytomegalovirus | 2/17 (11.8) | |
| Epstein–Barr Virus | 3/17 (17.6) | |
| Human herpesvirus 6 | 6/16 (37.5) | |
| Human herpesvirus 7 | 9/17 (52.9) | |
| Stool | ||
| Adenovirus | 10/16 (62.5) | |
| Astrovirus | 1/16 (6.2) | |
| Enterovirus | 3/16 (18.7) | |
| Norovirus | 6/16 (37.5) | |
| Sapovirus | 1/16 (6.2) | |
| Parecovirus | 1/16 (6.2) | |
| Nasopharyngeal aspirate or nasopharyngeal swab | ||
| Adenovirus | 3/15 (20.0) | |
| Bocavirus | 1/15 (6.7) | |
| Coronavirus OC43 | 2/15 (13.3) | |
| Enterovirus | 2/15 (13.3) | |
| Metapneumovirus | 1/15 (6.7) | |
| Rhinovirus | 6/15 (40.0) | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Di Maio, V.C.; Gentile, L.; Scutari, R.; Colagrossi, L.; Coltella, L.; Ranno, S.; Linardos, G.; Liccardo, D.; Basso, M.S.; Pietrobattista, A.; et al. Acute Hepatitis of Unknown Origin in Children: Analysis of 17 Cases Admitted to the Bambino Gesù Children’s Hospital in Rome. Microorganisms 2024, 12, 826. https://doi.org/10.3390/microorganisms12040826
Di Maio VC, Gentile L, Scutari R, Colagrossi L, Coltella L, Ranno S, Linardos G, Liccardo D, Basso MS, Pietrobattista A, et al. Acute Hepatitis of Unknown Origin in Children: Analysis of 17 Cases Admitted to the Bambino Gesù Children’s Hospital in Rome. Microorganisms. 2024; 12(4):826. https://doi.org/10.3390/microorganisms12040826
Chicago/Turabian StyleDi Maio, Velia Chiara, Leonarda Gentile, Rossana Scutari, Luna Colagrossi, Luana Coltella, Stefania Ranno, Giulia Linardos, Daniela Liccardo, Maria Sole Basso, Andrea Pietrobattista, and et al. 2024. "Acute Hepatitis of Unknown Origin in Children: Analysis of 17 Cases Admitted to the Bambino Gesù Children’s Hospital in Rome" Microorganisms 12, no. 4: 826. https://doi.org/10.3390/microorganisms12040826