

Analysing the Evidence of the Effects of Climate Change, Air Pollutants, and Occupational Factors in the Appearance of Cataracts


Abstract
:1. Introduction
2. Materials and Methods
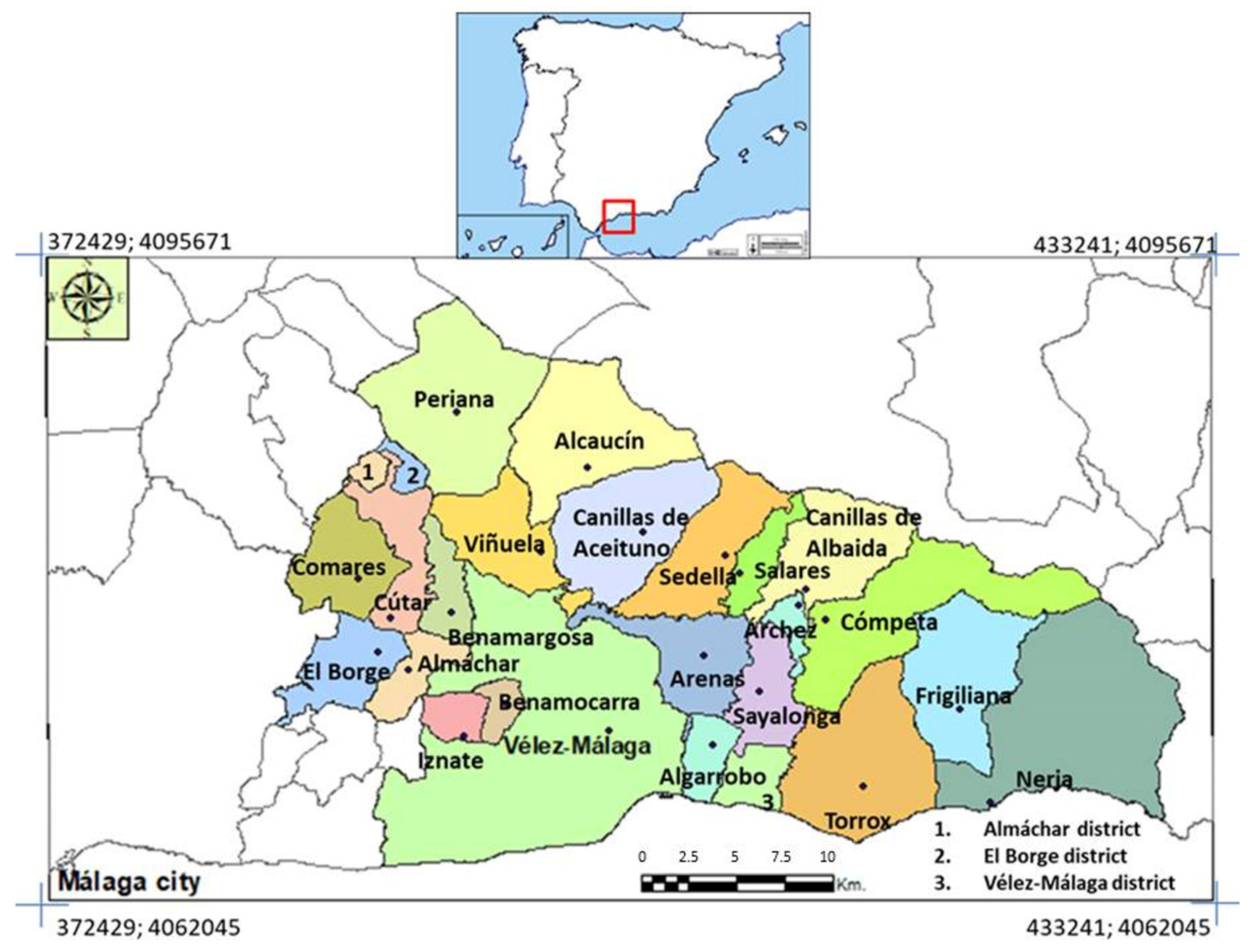
2.1. Study Area
2.2. Cataract Dataset and Demographic Analysis
2.3. Climate Trends and Air Pollution Analysis
2.4. Statistical Analysis
3. Results
3.1. Dataset Description
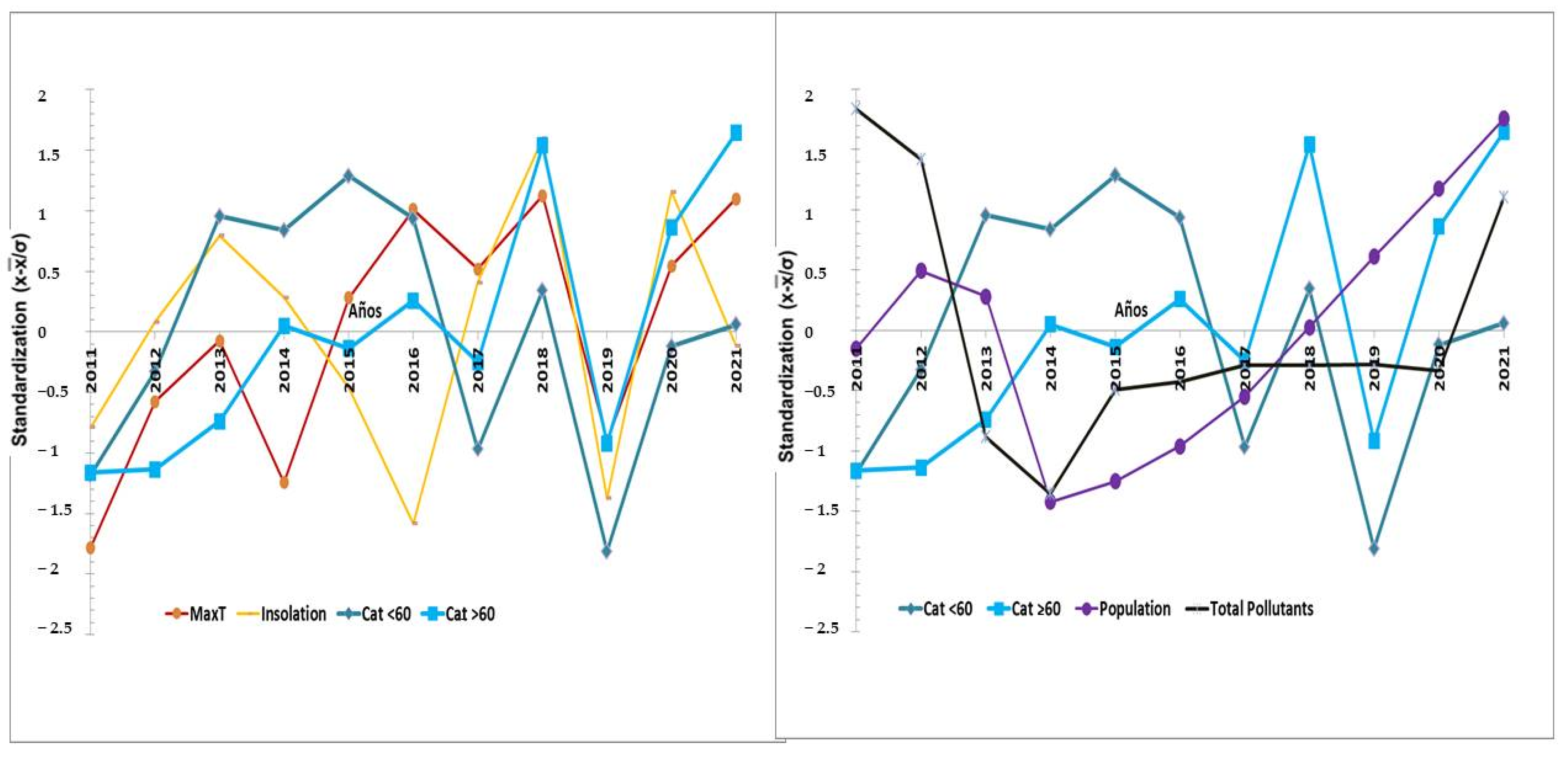
3.2. Trend Analysis
3.3. Temporal Bivariate Correlation Model
3.4. Spatial Bivariate Correlation Model
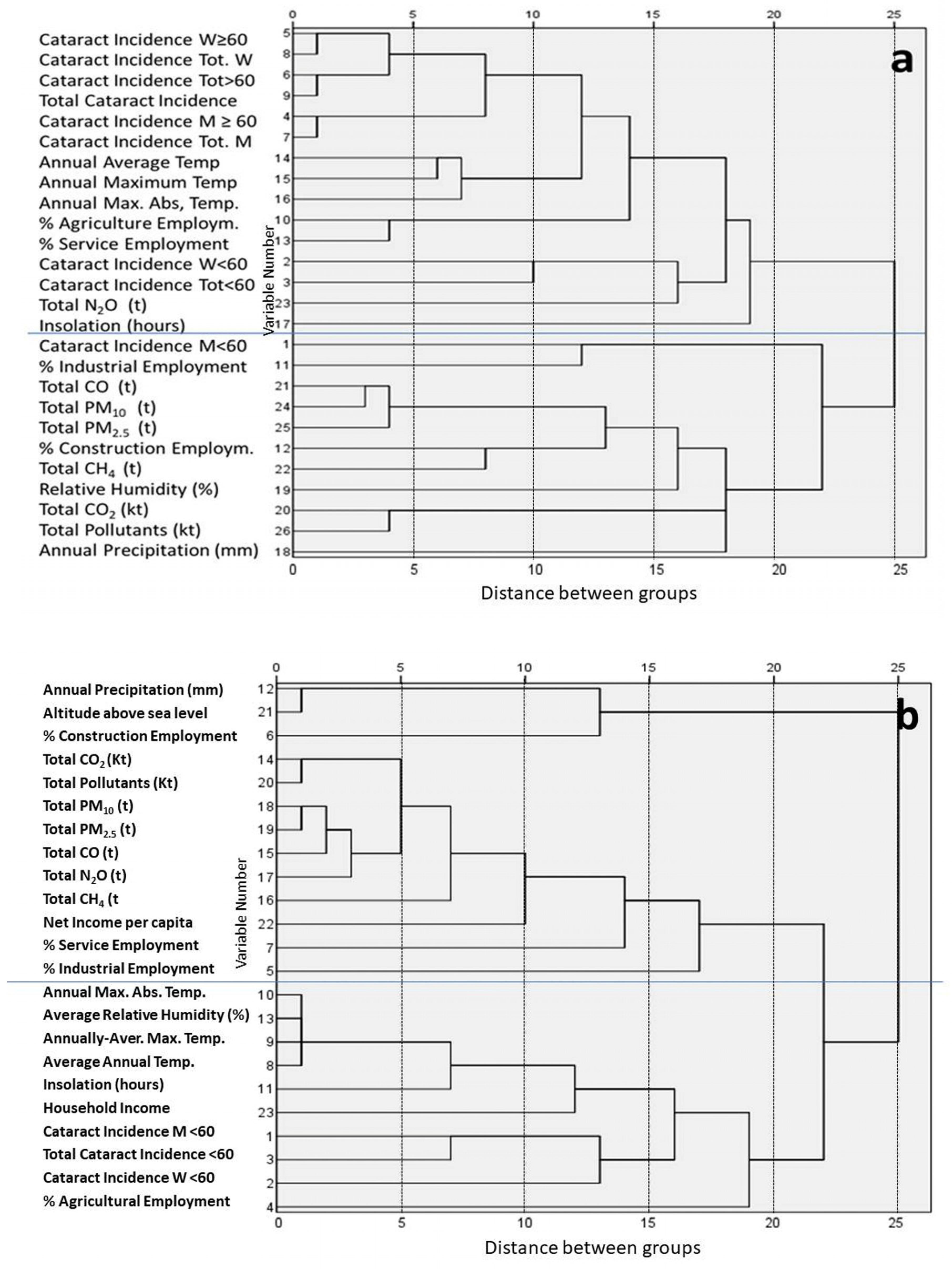
3.5. Cluster Analysis
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Data Availability Statement
Conflicts of Interest
References
- WHO. Cambio Climático y Salud. Informe 2021. 2021. Available online: https://www.who.int/es/news-room/fact-sheets/detail/climate-change-and-health (accessed on 30 January 2022).
- Patz, J.A.; Campbel-Lendrum, D.; Holloway, T.; Foley, J.A. Impact of regional climate change on human health. Nature 2005, 438, 310–317. [Google Scholar] [CrossRef] [PubMed]
- Mora, C.; McKenzie, T.; Gaw, I.M.; Dean, J.M.; von Hammerstein, H.; Knudson, T.A.; Setter, R.O.; Smith, C.Z.; Webster, K.M.; Patz, J.A.; et al. Over half of known human pathogenic diseases can be aggravated by climate change. Nat. Clim. Chang. 2022, 12, 869–875. [Google Scholar] [CrossRef] [PubMed]
- Marx, W.; Haunchild, R.; Bornmann, L. Heat waves: A hot topic in climate change research. Theor. Appl. Climatol. 2021, 146, 781–800. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Hettiarachchi, S.; Wasko, C.; Sharma, A. Increase in flood risk resulting from a developed urban watershed—the role of storm temporal patterns. Hydrol. Earth Syst. Sci. 2018, 22, 2041–2056. [Google Scholar] [CrossRef]
- Swain, D.L.; Wing, O.E.J.; Bates, P.D.; Done, J.M.; Johnson, K.A.; Cameron, D.R. Increased flood exposure due to climate change and population growth in the United States. Earth’s Future 2020, 8, e2020EF001778. [Google Scholar] [CrossRef]
- Williamson, C.E.; Zepp, R.G.; Lucas, R.M.; Mandronich, S.; Austin, A.T.; Ballaré, C.L.; Norval, M.; Sulzberger, B.; Bais, A.; McKenzie, R.L.; et al. Solar ultraviolet radiation in a changing climate. Nat. Clim. Change 2014, 4, 431–441. [Google Scholar] [CrossRef]
- Münzel, T.; Hahad, O.; Daiber, A.; Landrigan, P.J. Soil and water pollution and human health: What should cardiologist worry about? Cardiovasc. Res. 2023, 119, 440–449. [Google Scholar] [CrossRef] [PubMed]
- Yuan, X.; Wang, Y.; Ji, P.; Wu, P.; Sheffield, J.; Otkin, J.A. A global transition to flash drought under climate change. Science 2023, 380, 187–191. [Google Scholar] [CrossRef] [PubMed]
- Backlund, P.; Janetos, A.C.; Schimel, D.S. The Effects of Climate Change on Agriculture, Land Resources, Water Resources and Biodiversity in the United States. Synthesis and Assessment. Product 43. Report by the US Climate Change Science Program and the Subcommittee on Global Change Research. 2008; p. 362. Available online: https://www.usda.gov/sites/default/files/documents/CCSPFinalReport.pdf (accessed on 25 February 2022).
- Guida, C.; Gargiulo, C.; Papa, R.; Carpentieri, G. Vulnerability and Exposure of Mediterranean Coastal Cities to Climate Change-Related Phenomena. Environ. Sci. Proc. 2022, 21, 79. [Google Scholar] [CrossRef]
- Riordan, E.C.; Rundel, P.W. Land Use compounds habitat losses under projected Climate Change in a Threatened California Ecosystem. PLoS ONE 2014, 2014, e86487. [Google Scholar] [CrossRef]
- Tirado, M.C.; Clarke, R.; Jaykus, L.A.; McQuatters-Gollop, A.; Frank, J.M. Climate change and food safety: A review. Food Res. Int. 2010, 43, 1745–1765. [Google Scholar] [CrossRef]
- Rupasinghe, R.; Chomel, B.B.; Martínez-López, B. Climate change and zoonoses: A review of the current status, knowledge gaps, and future trends. Acta Trop. 2022, 226, 106225. [Google Scholar] [CrossRef] [PubMed]
- Cissé, G. Food-borne and water-borne diseases under climate change in low- and middle- income countries: Further efforts needed for reducing environmental health exposure risks. Acta Trop. 2019, 194, 181–188. [Google Scholar] [CrossRef] [PubMed]
- Sanz, M.J.; Galán, E. Impactos y Riesgos Derivados del Cambio Climático en España; Ministerio Para la Transición Ecológica y el Reto Demográfico: Madrid, Spain, 2021; p. 213. Available online: https://adaptecca.es/sites/default/files/documentos/impactosyriesgosccespanawebfinal_tcm30-518210_0.pdf (accessed on 16 November 2022).
- Senciales-González, J.M.; Echevarría-Lucas, L.; Rodrigo-Comino, J. Impact of climate change and human health in Spain. The first approach to the State-of-the-Art. In Climate Change and Impact on Human Health: Global Case Studies; Akhtar, R., Ed.; Springer: Cham, Switzerland, 2023; pp. 253–282. [Google Scholar] [CrossRef]
- Bielory, L.; Lyons, K.; Goldberg, R. Climate change and allergic disease. Curr. Allergy Asthma Rep. 2012, 12, 485–494. [Google Scholar] [CrossRef] [PubMed]
- Jalbert, I.; Golebiowski, B. Environmental aeroallergens and allergic rhino-conjunctivitis. Curr. Opin. Allergy Clin. Immunol. 2015, 15, 476–481. [Google Scholar] [CrossRef] [PubMed]
- Alves, M.; Novaes, P.; Morraye, M.d.A.; Reinach, P.S.; Rocha, E.M. Is dry eye an environmental disease? Arq. Bras. Oftalmol. 2014, 77, 193–200. [Google Scholar] [CrossRef] [PubMed]
- Zhong, J.-Y.; Lee, Y.-C.; Hsieh, C.-J.; Tseng, C.-C.; Yiin, L.-M. Association between Dry Eye Disease, Air Pollution and Weather Changes in Taiwan. Int. J. Environ. Res. Public Health 2018, 15, 2269. [Google Scholar] [CrossRef]
- Malik, S.M.; Awan, H.; Khan, N. Mapping vulnerability to climate change and its repercussions on human health in Pakistan. Glob. Health 2012, 8, 31. [Google Scholar] [CrossRef]
- Qassim, A.; Viki, M.; Ng, S.K.; Jersmann, H.; Casson, R.J. Climate and season: The effects on ophthalmic diseases. Clin. Exp. Ophthalmol. 2016, 45, 385–392. [Google Scholar] [CrossRef]
- Yam, J.C.S.; Kwok, A.K.H. Ultraviolet light and ocular diseases. Int. Ophthalmol. 2014, 34, 383–400. [Google Scholar] [CrossRef]
- Oliva, M.; Taylor, H. Ultraviolet Radiation and the Eye. Int. Ophthalmol. Clin. 2005, 45, 1–17. [Google Scholar] [PubMed]
- Gupta, V.B.; Rajagopala, M.; Ravishankar, B. Etiopathogenesis of cataract: An appraisal. Indian J. Ophthalmol. 2014, 62, 103–110. [Google Scholar] [CrossRef] [PubMed Central]
- Cullen, A.P. Ozone Depletion and Solar Ultraviolet Radiation: Ocular Effects, a United Nations Environment Programme Perspective. Eye Contact Lens Sci. Clin. Pract. 2011, 37, 185–190. [Google Scholar] [CrossRef] [PubMed]
- IARC Working Group on the Evaluation of Carcinogenic Risk to Humans, 2023. Solar and Ultraviolet Radiation. Available online: https://www.ncbi.nlm.nih.gov/books/NBK401588/ (accessed on 18 April 2023).
- Auger, N.; Rhéaume, M.-A.; Bilodeau-Bertrand, M.; Tang, T.; Kosatsky, T. Climate and the eye: Case-crossover analysis of retinal detachment after exposure to ambient heat. Environ. Res. 2017, 157, 103–109. [Google Scholar] [CrossRef] [PubMed]
- Saxena, R.; Srivastava, S.; Trivedi, D.; Anand, E.; Joshi, S.; Gupta, S.K. Impact of environmental pollution on the eye. Acta Ophthalmol. Scand. 2003, 81, 491–494. [Google Scholar] [CrossRef]
- Shubhrica, D. Effect of Environment on Eyes: A Review. Indian J. Clin. Pract. 2013, 24, 381–384. Available online: https://issuu.com/ijcp/docs/ijcp_sep_2013_web_83ae527bbe8a87 (accessed on 15 February 2022).
- Gupta, P.; Muthukumar, A. Minor to Chronic Eye Disorders Due to Environmental Pollution: A review. J. Ophthalmic Inflamm. Infect. 2018, 2, 108. Available online: https://www.walshmedicalmedia.com/open-access/minor-to-chronic-eye-disorders-due-to-environmental-pollution-a-review-17751.html (accessed on 15 February 2022).
- McCarty, C.A.; Taylor, H.R. The genetics of caratacts. Investig. Ophthalmol. Vis. Sci. 2001, 42, 1677–1678. Available online: https://iovs.arvojournals.org/article.aspx?articleid=2200006 (accessed on 16 February 2022).
- Dantas, A.P.; Brandt, C.T.; Leal, D.N.B. Manifestações oculares em pacientes que tiveram desnutrição nos primeiros seis meses de vida. Arq. Bras. Oftalmol. 2005, 68, 753–756. [Google Scholar] [CrossRef]
- Fernández-Araque, A.; Aranda, A.G.; Pardo, C.L.; Aragüés, A.R. Los antioxidantes en el proceso de patologías oculares. Nutr. Hosp. 2017, 34, 469–478. [Google Scholar] [CrossRef]
- Bowling, B. Kanski Oftalmología Clínica. Un Enfoque Sistemático; Elsevier: Barcelona, Spain, 2016; p. 273. [Google Scholar]
- Mukesh, B.N.; Le, A.; Dimitrov, P.N.; Ahmed, S.; Taylor, H.R.; McCarty, C.A. Development of cataracts and associated risk factors. The visual impairment Project. Arch. Ophthalmol. 2006, 124, 79–85. [Google Scholar] [CrossRef] [PubMed]
- Roberts, J.E. Ultraviolet radiation as a risk factor for cataract and macular degeneration. Eye Contact Lens 2011, 37, 246–249. [Google Scholar] [CrossRef] [PubMed]
- Ng, A.L.; Marcet, M.; Lai, J.S.; Yeung, J.C. Age-Related true exfoliation of the Lens Capsule: Phacoemulsification Surgery Results. Case Rep. Ophthalmol. 2015, 6, 401–407. [Google Scholar] [CrossRef]
- Shin, J.; Lee, H.; Kim, H. Association between Exposure to Ambient Air Pollution and Age-Related Cataract: A Nationwide Population-Based Retrospective Cohort Study. Int. J. Environ. Res. Public Health 2020, 17, 9231. [Google Scholar] [CrossRef] [PubMed]
- Alimaw, Y.A.; Hussen, M.S.; Tefera, T.K.; Yibekal, B.T. Knowledge about cataract and associated factors among adults in Gondar town, northwest Ethiopia. PLoS ONE 2019, 14, e0215809. [Google Scholar] [CrossRef] [PubMed]
- Chandler, H.L.; Reuter, K.S.; Sinnott, L.T.; Nichols, J.J. Prevention of UV-Induced Damage to the Anterior Segment Using Class I UV-Absorbing Hydrogel Contact Lenses. Investig. Ophthalmol. Vis. Sci. 2010, 51, 172–178. [Google Scholar] [CrossRef]
- Echevarría, L.; Senciales, J.M.; Medialdea, M.E.; Rodrigo, J. Impact of Climate Change on Eye Diseases and Associated Economical Costs. Int. J. Environ. Res. Public Health 2021, 18, 7197. [Google Scholar] [CrossRef] [PubMed]
- Das, G.K.; Boriwal, K.; Chhabra, P.; Sahu, P.K.; Kumar, S.; Kumar, N. Presenile cataract and its risk factors: A case control. J. Fam. Med. Prim. Care 2019, 8, 2120–2123. [Google Scholar] [PubMed Central]
- Praveen, M.R.; Shah, G.D.; Vasavada, A.R.; Mehta, P.G.; Gilbert, C.; Bhagat, G. A study to explore the risk for the early onset of cataract in India. Eye 2009, 24, 686–694. [Google Scholar] [CrossRef]
- REDIAM. Indicadores de Calidad del Aire Junta de Andalucía. 2013. Available online: https://www.juntadeandalucia.es/medioambiente/portal/acceso-rediam/indicadores-ambientales/indicadores-ambientales-2013 (accessed on 2 February 2023).
- Rodrigo-Comino, J. Cuantificación de los gradientes térmicos a nivel superficial a lo largo del Rheinland-Pfalz (Renania-Palatinado, Alemania). Baetica 2013, 35, 75–98. [Google Scholar] [CrossRef]
- Senciales-González, J.M.; Rodrigo-Comino, J.; Smith, P. Surveying topographical changes and climate variations to detect the urban heat island in the city of Málaga (Spain). Cuad. Investig. Geográfica 2020, 46, 521–543. [Google Scholar] [CrossRef]
- Gobierno de España Ministerio de Transportes, Movilidad y Agenda Urbana. Available online: https://www.transportes.gob.es/ (accessed on 16 March 2022).
- Galán-Madruga, D.; Fernández-Patier, R. Implicación de los NOx en la Química Atmosférica. Revista Electrónic@ de Medio Ambiente. UCM, Diciembre de 2006. 2006, p. 14. Available online: https://www.ucm.es/data/cont/media/www/pag-41377/2006%202%20david%20galan%20y%20otro.pdf (accessed on 2 February 2023).
- Jiménez López, M.D. Dinámica de Gases Invernadero (CO2, N2O y CH4) en el Golfo de Cádiz (Campañas Stoca 2015). Proyecto presentado por Puerto Real, 2 de Octubre del 2015. Máster en Oceanografía Universidad de Cádiz. 2015. Available online: https://rodin.uca.es/handle/10498/18698 (accessed on 2 February 2023).
- Helsel, D.R.; Frans, L.M. Regional Kendall Test for trend. Environ. Sci. Technol. 2006, 40, 4066–4073. [Google Scholar] [CrossRef] [PubMed]
- Mann, H.B. Non parametric test against trend. Econometrica 1945, 13, 245–249. [Google Scholar] [CrossRef]
- Kendall, M.G. Rank Correlation Methods, 4th ed.; Charles Griffin: London, UK, 1975. [Google Scholar]
- Miró, J.; Estrela, M.J.; Pastor, F.; Millán, M. Análisis comparativo de tendencias en la precipitación, por distintos inputs, entre los dominios hidrológicos del Segura y del Júcar (1958–2008). Investig. Geográficas 2009, 49, 129–157. [Google Scholar] [CrossRef]
- Europa Press. La Cirugía de Catarata es Uno de los Procedimientos Quirúrgicos Más Comunes. 2015. Available online: https://www.infosalus.com/asistencia/noticia-cirugia-catarata-procedimientos-quirurgicos-mas-comunes-20150518140228.html (accessed on 26 June 2023).
- Sasaki, K.; Hockwin, O. Progress in Lens and Cataract Research: In Honour of Professor Kazuyuki Sasaki; Karger Medical and Scientific Publishers: Basel, Switzerland, 2002. [Google Scholar] [CrossRef]
- Estelle, I. Cambio Climático—Escenario Actual, Salud e Implicancias en la Población Chilena. 2020. Available online: https://www.academia.edu/42152825/CAMBIO_CLIM%C3%81TICO_ESCENARIO_ACTUAL_SALUD_E_IMPLICANCIAS_EN_LA_POBLACI%C3%93N_CHILENA (accessed on 13 April 2020).
- de Irazazábal Gómez-Ulla, F.; Ondategui Parra, S. Informe Sobre la Ceguera en España. 2009. Available online: https://www.seeof.es/archivos/articulos/adjunto_20_1.pdf (accessed on 23 January 2021).
- Ministerio de Sanidad, Servicios Sociales e Igualdad. Informe Anual del Sistema Nacional de Salud 2015–2016. 2015. Available online: https://www.sanidad.gob.es/estadEstudios/estadisticas/sisInfSanSNS/tablasEstadisticas/Inf_Anual_SNS_2015.1.pdf (accessed on 15 September 2020).
- Vidal, M.J.; Labeaga, J.M.; Casado, P.; Madrigal, A.; López, J.; Montero, A.; Meil, G. Informe 2016: Las Personas Mayores en España Datos estadísticos estatales y por Comunidades Autónomas; Ministerio de Sanidad, Servicios Sociales e Igualdad, IMSERSO: Madrid, Spain, 2017; p. 540. Available online: http://ibdigital.uib.es/greenstone/collect/portal_social/index/assoc/msan0206.dir/msan0206.pdf (accessed on 5 June 2023).
- Expansión. Statistical Data from 2010 to 2021. Available online: https://datosmacro.expansion.com/estado/presupuestos/espana-comunidades-autonomas/andalucia?sc=PR-G-F-31&anio=2021 (accessed on 15 May 2023).
- Taylor, H.R. Pseudoexfoliation, an environmental disease? Trans. Ophthalmol. Soc. UK 1979, 99, 302–307. [Google Scholar] [PubMed]
- Stein, J.D.; Pasquale, L.R.; Talwar, N.; Kim, D.S.; Reed, D.M.; Nan, B.; Kang, J.H.; Wiggs, J.L.; Richards, J.E. Geographic and Climatic Factors Associated with Exfoliation Syndrome. Arch Ophthalmol 2011, 129, 1053–1060. [Google Scholar] [CrossRef] [PubMed]
- Resnikoff, S.; Filliard, G.; Dell’Aquila, B. Climatic droplet keratopathy, exfoliation syndrome, and cataract. Br. J. Ophthalmol. 1991, 75, 734–736. [Google Scholar] [CrossRef]
- Gray, R.H.; Johnson, G.J.; Freedman, A. Climatic droplet keratopathy. Surv. Ophthalmol. 1992, 36, 241–253. [Google Scholar] [CrossRef]
- Consejería de Salud Junta de Andalucia. Informe Inicial Sobre Adaptación al Cambio Climático en el Ámbito de Salud. 2012. Available online: https://www.juntadeandalucia.es/medioambiente/portal_web/web/temas_ambientales/clima/actuaciones_cambio_climatico/adaptacion/vulnerabilidad_impactos_medidas/isis/isi_salud.pdf (accessed on 24 May 2021).
- Eye Care Institute. What Causes Cataract. Santa Rosa, CA, USA. 2023. Available online: https://www.see-eci.com/our-services/cataracts/what-causes-cataract/ (accessed on 17 March 2023).
- Kim, J.; Kim, S. Temperature Estimation Adaptive to Variables over Distance Using Infrared–LiDAR. Appl. Sci. 2021, 11, 4063. [Google Scholar] [CrossRef]
- Lv, X.; Gao, X.; Hu, K.; Yao, Y.; Zeng, Y.; Chen, H. Associations of Humidity and Temperature with Cataracts among Older Adults in China. Front. Public Health 2022, 10, 872030. [Google Scholar] [CrossRef] [PubMed Central]
- Fuller-Thomson, E.; Deng, Z.D.; Fuller-Thomson, E.G. Association between area temperature and severe vision impairment in a nationally representative sample of olders americans. Ophthalmic Epidemiol. 2023, 20, 2023. [Google Scholar] [CrossRef] [PubMed]
- MITECO. Cambio Climático y Salud Humana. 2023. Available online: https://www.miteco.gob.es/es/cambio-climatico/temas/impactos-vulnerabilidad-y-adaptacion/16_salud_humana_2_tcm30-178509.pdf (accessed on 27 February 2023).
- Mohan, M.; Sperduto, R.D.; Angra, S.K.; Mathur, R.L.; Jaffery, N.; Chhabra, V.K.; Vajpayee, R.B.; Kalra, V.K.; Pandya, C.B. India-US casecontrol study of age-related cataracts India-US case-control study group. Arch. Ophthalmol. 1989, 107, 670–676. [Google Scholar] [CrossRef] [PubMed]
- Zodpey, S.; Ughade, S. Exposure to cheaper cooking fuels and risk of age-related cataracts in women. Indian J. Occup. Environ. Med. 1999, 3, 159–161. [Google Scholar] [CrossRef] [PubMed]
- Alryalat, S.A.; Toubasi, A.A.; Patnaik, J.L.; Kahook, M.Y. The impact of air pollution and climate change on eye health: A global review. Rev. Environ. Health, 2022; 29, 209. [Google Scholar] [CrossRef]
- Chua, S.Y.L.; Khawaja, A.P.; Desai, P.; Rahi, J.S.; Day, A.C.; Hammond, C.J.; Khaw, P.T.; Foster, P.J. The Association of Ambient Air Pollution With Cataract Surgery in UK Biobank Participants: Prospective Cohort Study. Investig. Ophthalmol. Vis. Sci. 2021, 62, 7. [Google Scholar] [CrossRef] [PubMed]
- Adams, D.R. The nature of the ocular lesions produced experimentally by naphthalene. Br. J. Ophthalmol. 1930, 14, 49–60. [Google Scholar] [CrossRef]
- Rodrigo-Comino, J.; Senciales, J.M. A Regional Geography Approach to Understanding the Environmental Changes as a Consequence of the COVID-19 Lockdown in Highly Populated Spanish Cities. Appl. Sci. 2021, 11, 2912. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
{kind=link}
| Population (a) | Cataracts (b) | Standardized Cumulative Incidence (c) | |||||||
|---|---|---|---|---|---|---|---|---|---|
| Group (Years) | 15–59 | ≥60 | Total | 15–59 | ≥60 | Total | 15–59 | ≥60 | Total |
| Men | 48,639 | 18,474 | 67,113 | 502 | 4130 | 4632 | 0.0064 | 0.0506 | 0.0588 |
| Women | 46,728 | 20,382 | 67,110 | 361 | 4494 | 4855 | 0.0048 | 0.0503 | 0.0612 |
| Total | 95,367 | 38,856 | 134,223 | 863 | 8624 | 9487 | 0.0056 | 0.0504 | 0.0600 |
| Year/Variable | Number of Cataracts (≥60 Years) | Number of Cataracts 15–59 Years | Total Cataracts | Cataracts Incidence Men 15–59 | Cataracts Incidence Women 15–59 | Total Cataracts Incidence 15–59 | Cataracts Incidence Men ≥60 | Cataracts Incidence Women ≥60 | Total Cataracts Incidence ≥60 | Total Cataracts Incidence Men | Total Cataracts Incidence Women | Total Cataracts Incidence |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 2011 | 606 | 65 | 671 | 4.82 | 3.57 | 4.21 | 37.19 | 32.40 | 34.68 | 42.01 | 35.97 | 38.88 |
| 2012 | 626 | 76 | 702 | 5.91 | 3.80 | 4.87 | 34.29 | 35.49 | 34.92 | 40.21 | 39.28 | 39.79 |
| 2013 | 687 | 91 | 778 | 7.10 | 4.61 | 5.88 | 36.51 | 40.74 | 38.73 | 43.62 | 45.35 | 44.61 |
| 2014 | 734 | 87 | 821 | 6.15 | 5.41 | 5.78 | 38.66 | 53.15 | 46.28 | 44.81 | 58.56 | 52.06 |
| 2015 | 711 | 92 | 803 | 6.70 | 5.56 | 6.14 | 45.18 | 43.88 | 44.50 | 51.87 | 49.43 | 50.63 |
| 2016 | 783 | 88 | 871 | 7.35 | 4.33 | 5.86 | 51.80 | 45.06 | 48.28 | 59.15 | 49.39 | 54.14 |
| 2017 | 716 | 66 | 782 | 4.32 | 4.43 | 4.37 | 45.73 | 42.08 | 43.40 | 50.05 | 46.51 | 47.78 |
| 2018 | 1028 | 82 | 1110 | 6.37 | 4.40 | 5.40 | 60.99 | 60.16 | 60.56 | 67.36 | 64.56 | 65.96 |
| 2019 | 643 | 57 | 700 | 4.77 | 2.64 | 3.72 | 40.73 | 33.60 | 37.00 | 45.51 | 36.23 | 40.72 |
| 2020 | 964 | 78 | 1042 | 6.53 | 3.52 | 5.04 | 56.75 | 51.59 | 54.06 | 63.28 | 55.11 | 59.10 |
| 2021 | 1126 | 81 | 1207 | 4.68 | 5.68 | 5.18 | 57.99 | 64.83 | 61.56 | 62.67 | 70.52 | 66.73 |
| Variable | 2010 | 2011 | 2012 | 2013 | 2014 | 2015 | 2016 | 2017 | 2018 | 2019 | 2020 |
|---|---|---|---|---|---|---|---|---|---|---|---|
| 1. Agriculture Employment % | 7.42 | 7.81 | 8.23 | 9.58 | 10.16 | 11.20 | 11.54 | 13.17 | 13.22 | 11.75 | 12.37 |
| 2. Industrial Employment % | 4.83 | 5.03 | 5.01 | 5.36 | 5.34 | 5.36 | 4.80 | 4.67 | 4.46 | 4.90 | 4.20 |
| 3. Construction Employment % | 32.98 | 31.55 | 30.81 | 24.21 | 20.56 | 16.72 | 15.20 | 14.03 | 12.98 | 12.73 | 12.51 |
| 4. Services Employment % | 54.76 | 55.61 | 55.96 | 60.84 | 63.93 | 66.73 | 68.45 | 68.13 | 69.34 | 70.62 | 70.92 |
| 5. Average Annual Temperature (°C) | 16.70 | 16.95 | 16.83 | 16.52 | 17.09 | 17.41 | 17.28 | 17.35 | 16.48 | 17.06 | 17.31 |
| 6. Annually Averaged Maximum Temperature (°C) | 21.07 | 21.69 | 21.94 | 21.35 | 22.12 | 22.49 | 22.24 | 22.55 | 21.52 | 22.25 | 22.54 |
| 7. Annual Maximum Absolute Temperature (°C) | 27.10 | 27.54 | 28.30 | 26.65 | 28.10 | 28.63 | 28.04 | 28.48 | 26.35 | 27.88 | 28.93 |
| 8. Insolation (a) | 2168 | 2265 | 2345 | 2288 | 2205 | 2080 | 2301 | 2433 | 2104 | 2385 | 2244 |
| 9. Sum of Annual Precipitation (mm) | 880.4 | 568.0 | 529.0 | 473.0 | 564.7 | 408.7 | 564.7 | 341.4 | 842.8 | 336.3 | 336.3 |
| 10. Average Annual Relative Humidity (%) | 53.6 | 54.6 | 53.3 | 55.5 | 55.2 | 54.1 | 55.2 | 52.3 | 52.7 | 50.0 | 53.7 |
| 11. Total CO2 | 408.2 | 401.3 | 323.2 | 304.8 | 318.1 | 322.1 | 328.6 | 331.1 | 335.6 | 338.0 | 352.7 |
| 12. Total CO | 3111 | 2933 | 2871 | 2505 | 3225 | 2448 | 2417 | 2260 | 2231 | 2265 | 2599 |
| 13. Total CH4 | 1021.1 | 964.4 | 891.5 | 852.7 | 862.6 | 854.7 | 871.9 | 864.7 | 827.6 | 801.4 | 792.7 |
| 14. Total N2O | 86.7 | 83.3 | 82.0 | 87.0 | 94.7 | 84.0 | 85.9 | 86.6 | 84.5 | 85.9 | 91.5 |
| 15. Total PM10 | 350.2 | 356.2 | 349.2 | 327.4 | 390.0 | 320.4 | 311.6 | 295.1 | 287.9 | 293.0 | 337.0 |
| 16. Total PM2.5 | 278.8 | 282.5 | 270.8 | 255.3 | 308.8 | 252.2 | 239.4 | 223.5 | 216.0 | 219.9 | 229.8 |
| 17. Total pollutants | 400.6 | 393.8 | 320.2 | 301.8 | 316.2 | 318.7 | 324.7 | 326.9 | 331.1 | 333.2 | 386.4 |
| Variable | Z-Score | Tau (M-K) | (S) | p |
|---|---|---|---|---|
| Cataracts’ standardized annual incidence in men ≥ 60 years old | 3.22 | 0.673 | 37 | 0.004 |
| Cataracts’ standardized annual incidence in women ≥ 60 years old | 2.33 | 0.491 | 27 | 0.036 |
| Total standardized annual incidence in people ≥ 60 years old | 2.86 | 0.600 | 33 | 0.01 |
| Total standardized annual incidence in men | 3.04 | 0.636 | 35 | 0.006 |
| Total standardized cataracts annual incidence | 2.86 | 0.600 | 33 | 0.01 |
| % Agricultural employment | 4.11 | 0.822 | 37 | <0.001 |
| % Industrial employment | −2.06 | −0.539 | −24 | 0.031 |
| % Construction employment | −5.01 | −1 | −45 | <0.001 |
| % Services employment | 4.65 | 0.956 | 43 | <0.001 |
| Total CO | −2.86 | −0.511 | −23 | 0.047 |
| Total CH4 | −3.58 | −0.644 | −29 | 0.009 |
| Total PM10 | −2.86 | −0.556 | −25 | 0.029 |
| Total PM2.5 | −3.4 | −0.689 | −31 | 0.005 |
| Occupational or Environmental Variable | Cataracts Incidence Men 15–59 | Cataracts Incidence Women 14–59 | Total Cataracts Incidence 15–59 | Cataracts Incidence Men ≥60 | Cataracts Incidence Women ≥60 | Total Cataracts Incidence ≥60 | Total Cataracts Incidence Men | Total Cataracts Incidence Women | Total Cataracts Incidence |
|---|---|---|---|---|---|---|---|---|---|
| 1. % Agriculture Employment % | −0.17 (0.62) | −0.06 (0.88) | −0.15 (0.74) | 0.77 (<0.05) | 0.53 (0.07) | 0.67 (<0.05) | 0.73 (<0.05) | 0.50 (0.10) | 0.64 (<0.05) |
| 2. Industrial Employment | 0.69 (<0.05) | 0.23 (0.51) | 0.61 (<0.05) | −0.35 (0.28) | −0.25 (0.48) | −0.31 (0.36) | −0.27 (0.43) | −0.21 (0.55) | −0.25 (0.47) |
| 3. Construction Employment % | 0.15 (0.67) | −0.01 (0.96) | 0.10 (0.79) | −0.80 (<0.05) | −0.56 (0.05) | −0.70 (<0.05) | −0.77 (<0.05) | −0.53 (0.07) | −0.67 (<0.05) |
| 4. Services Employment % | −0.18 (0.61) | 0.02 (0.95) | −0.11 (0.76) | 0.81 (<0.05) | 0.56 (0.05) | 0.70 (<0.05) | 0.77 (<0.05) | 0.53 (0.07) | 0.67 (<0.05) |
| 5. Average Annual Temperature (°C) | 0.18 (0.61) | 0.35 (0.29) | 0.34 (0.31) | 0.73 (<0.05) | 0.51 (0.08) | 0.64 (<0.05) | 0.74 (<0.05) | 0.51 (0.08) | 0.65 (<0.05) |
| 6. Annually Averaged Maximum Temperature (°C) | 0.28 (0.42) | 0.35 (0.29) | 0.40 (0.21) | 0.82 (<0.05) | 0.65 (<0.05) | 0.76 (<0.05) | 0.84 (<0.05) | 0.64 (<0.05) | 0.77 (<0.05) |
| 7. Annual Maximum Absolute Temperature (°C) | 0.32 (0.35) | 0.50 (0.09) | 0.52 (0.08) | 0.63 (<0.05) | 0.55 (0.05) | 0.62 (<0.05) | 0.66 (<0.05) | 0.56 (<0.05) | 0.64 (<0.05) |
| 8. Annual Insolation (hours) | 0.16 (0.65) | 0.20 (0.57) | 0.23 (0.51) | 0.31 (0.36) | 0.49 (0.1) | 0.43 (0.17) | 0.33 (0.33) | 0.48 (0.11) | 0.44 (0.16) |
| 9. Sum of Annual Precipitation (mm.) | −0.46 (0.13) | −0.53 (0.07) | −0.64 (<0.05) | −0.71 (<0.05) | −0.85 (<0.05) | −0.83 (<0.05) | −0.75 (<0.05) | −0.85 (<0.05) | −0.86 (<0.05) |
| 10. Annual Average Relative Humidity (%); | −0.15 (0.68) | 0.53 (0.07) | 0.21 (0.54) | −0.49 (0.11) | −0.18 (0.62) | −0.34 (0.31) | −0.50 (0.10) | −0.12 (0.73) | −0.31 (0.36) |
| 11. Total CO2 (Kt/year) | −0.40 (0.21) | −0.41 (0.2) | −0.52 (0.08) | −0.30 (0.37) | −0.41 (0.20) | −0.38 (0.24) | −0.34 (0.30) | −0.43 (0.18) | −0.41 (0.20) |
| 12. Total CO (t/year) | 0.10 (0.78) | 0.30 (0.37) | 0.25 (0.47) | −0.54 (0.06) | −0.40 (0.22) | −0.49 (0.11) | −0.52 (0.07) | −0.35 (0.29) | −0.45 (0.15) |
| 13. Total CH4 (t/year) | −0.10 (0.77) | −0.26 (0.45) | −0.22 (0.52) | −0.64 (<0.05) | −0.65 (<0.05) | −0.68 (<0.05) | −0.64 (<0.05) | −0.63 (<0.05) | −0.68 (<0.05) |
| 14. Total N2O (t/year) | −0.15 (0.67) | 0.62 (<0.05) | 0.26 (0.45) | 0.34 (0.31) | 0.42 (0.19) | 0.41 (0.21) | 0.32 (0.34) | 0.45 (0.15) | 0.41 (0.20) |
| 15. Total PM10 (t/year) | 0.19 (0.59) | 0.52 (0.08) | 0.44 (0.16) | −0.46 (0.14) | −0.23 (0.51) | −0.35 (0.30) | −0.43 (0.18) | −0.17 (0.63) | −0.30 (0.38) |
| 16. Total PM2.5 (t/year) | 0.30 (0.38) | 0.34 (0.31) | 0.41 (0.20) | −0.59 (<0.05) | −0.43 (0.17) | −0.53 (0.07) | −0.55 (0.06) | −0.38 (0.24) | −0.48 (0.12) |
| 17. Total Pollutants (Kt/year) | −0.49 (0.11) | −0.21 (0.54) | −0.46 (0.14) | −0.14 (0.70) | −0.18 (0.62) | −0.17 (0.64) | −0.19 (0.59) | −0.19 (0.60) | −0.20 (0.57) |
| Occupational, Socioeconomic, or Environmental Variable | Cumulative Incidence of Cataracts in Men 15–59 Years Old | Cumulative Incidence of Cataracts in Women 15–59 Years Old | Total Cumulative Incidence of Cataracts in those 15–59 Years Old |
|---|---|---|---|
| % Agricultural employment | 0.33 (0.11) | 0.95 (<0.05) | 0.85 (<0.05) |
| % Industrial employment | −0.18 (0.41) | 0.21 (0.32) | 0.03 (0.87) |
| % Construction employment | 0.18 (0.41) | 0.12 (0.59) | 0.42 (<0.05) |
| % Services employment | −0.27 (0.21) | −0.38 (0.05) | −0.42 (<0.05) |
| Average Annual Temperature | 0.28 (0.18 | 0.16 (0.46) | 0.22 (0.29) |
| Annually Averaged Maximum Temperature | 0.47 (<0.05) | 0.6 (<0.05) | 0.52 (<0.05) |
| Annual Maximum Absolute Temperature | 0.47 (<0.05) | 0.6 (<0.05) | 0.52 (<0.05) |
| Annual Insolation (hours) | 0.47 (<0.05) | 0.6 (<0.05) | 0.52 (<0.05) |
| Sum of Annual Precipitation (mm.) | 0.42 (<0.05) | 0.62 (<0.05) | 0.47 (<0.05) |
| Average Annual Relative Humidity | −0.47 (0.17) | −0.60 (<0.05) | −0.52 (<0.05) |
| Average CO2 (Kt) | 0.47 (<0.05) | 0.60 (<0.05) | 0.52 (<0.05) |
| Average CO (t) | 0.70 (<0.05) | 0.31 (0.13) | 0.32 (0.11) |
| Average CH4 (t) | 0.66 (0.13) | 0.23 (0.27) | 0.32 (0.11) |
| Average N2O (t) | 0.90 (<0.05) | 0.18 (0.41) | 0.34 (0.09) |
| Average PM10 (t) | 0.67 (<0.05) | 0.24 (0.26) | 0.30 (0.14) |
| Average PM2.5 (t) | 0.66 (<0.05) | 0.24 (0.26) | 0.31 (0.13) |
| Total Pollutants (Kt) | 0.66 (<0.05) | 0.24 (0.25) | 0.31 (0.13) |
| Altitude above sea level | 0.70 (<0.05) | 0.31 (0.13) | 0.32 (0.11) |
| Net income per capita | −0.47 (<0.05) | −0.60 (<0.05) | −0.52 (<0.05) |
| Household income | 0.32 (0.12) | 0.04 (0.87) | −0.05 (0.82) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Echevarría-Lucas, L.; Senciales-González, J.M.; Rodrigo-Comino, J. Analysing the Evidence of the Effects of Climate Change, Air Pollutants, and Occupational Factors in the Appearance of Cataracts. Environments 2024, 11, 87. https://doi.org/10.3390/environments11050087
Echevarría-Lucas L, Senciales-González JM, Rodrigo-Comino J. Analysing the Evidence of the Effects of Climate Change, Air Pollutants, and Occupational Factors in the Appearance of Cataracts. Environments. 2024; 11(5):87. https://doi.org/10.3390/environments11050087
Chicago/Turabian StyleEchevarría-Lucas, Lucía, José Mª Senciales-González, and Jesús Rodrigo-Comino. 2024. "Analysing the Evidence of the Effects of Climate Change, Air Pollutants, and Occupational Factors in the Appearance of Cataracts" Environments 11, no. 5: 87. https://doi.org/10.3390/environments11050087