
Medical Gas Plasma—A Potent ROS-Generating Technology for Managing Intraoperative Bleeding Complications


1
Department of General, Visceral, Thoracic, and Vascular Surgery, Greifswald University Medical Center, Ferdinand-Sauerbruch-Str., 17475 Greifswald, Germany
2
ZIK plasmatis, Leibniz Institute for Plasma Science and Technology (INP), Felix-Hausdorff-Str. 2, 17489 Greifswald, Germany
*
Author to whom correspondence should be addressed.
†
These authors contributed equally to this work.
Appl. Sci. 2022, 12(8), 3800; https://doi.org/10.3390/app12083800
Submission received: 12 March 2022
/
Revised: 5 April 2022
/
Accepted: 8 April 2022
/
Published: 9 April 2022
(This article belongs to the Special Issue Plasma Medicine Technologies: Volume II)
Abstract
:Cold medical gas plasmas are under pre-clinical investigation concerning their hemostatic activity and could be applied for intra-operative bleeding control in the future. The technological leap innovation was their generation at body temperature, thereby causing no thermal harm to the tissue and ensuring tissue integrity. This directly contrasts with current techniques such as electrocautery, which induces hemostasis by carbonizing the tissue using a heated electrode. However, the necrotized tissue is prone to fall, raising the risk of post-operative complications such as secondary bleedings or infection. In recent years, various studies have reported on the ability of medical gas plasmas to induce blood coagulation, including several suggestions concerning their mode of action. As non-invasive and gentle hemostatic agents, medical gas plasmas could be particularly eligible for vulnerable tissues, e.g., colorectal surgery and neurosurgery. Further, their usage could be beneficial regarding the prevention of post-operative bleedings due to the absence or sloughing of eschar. However, no clinical trials or individual healing attempts for medical gas plasmas have been reported to pave the way for clinical approvement until now, despite promising results in experimental animal models. In this light, the present mini-review aims to emphasize the potential of medical gas plasmas to serve as a hemostatic agent in clinical procedures. Providing a detailed overview of the current state of knowledge, feasible application fields are discussed, and possible obstacles are addressed.
1. Introduction
Intraoperative bleeding is a severe complication of any surgical procedure. Although surgical mortality is low in most elective surgical procedures, bleeding complications can escalate mortality rates from <1% up to 20% [1,2]. Consequently, many scoring systems designed to assess operative morbidity and mortality risk (e.g., POSSUM, TRISS) reflect the impact of major blood loss during surgery [3,4]. Apart from inadequate surgical hemostasis, major risk factors include dilutional thrombocytopenia, systemic clotting factor depletion, and new oral anticoagulants (NOACs). An aging population with multiple comorbidities further contributes to the risk of intraoperative bleeding [5]. Uncontrolled bleeding contributes to a rapidly evolving vicious cycle in which the combination of hemodilution, hypothermia, the consumption of clotting factors, and acidosis further enhances the bleeding [6]. Surgical interventions to manage blood loss include, e.g., topical absorbable hemostats, conventional surgical methods, and electrocauterization, each with its own limitations [7]. In the latter, a direct or alternating current passes through an electrode wire, generating heat and thus necrotizing and profoundly destroying the tissue [8,9]. However, the necrotized tissue can disconnect and fall off, causing secondary bleedings hours and days after surgery. This is similar to scratching of the scab of a skin wound, causing it to bleed again, which is, however, much more severe for internal wounds. Moreover, post-operative complications, including infection, abscess formation, and hematoma, put patients at additional risk [10]. There are cost-intensive developments for intraoperative hemostasis to minimize the thermal damage caused by the heat generated. Well-known manufacturers developed energy-based surgical vessel sealing devices, e.g., the LigaSure technology from Medtronic, the Harmonic from Ethicon Johnson and Johnson, and the Thunderbeat from Olympus. The various sealing instruments have in common the fact that they try to minimize heat generation in the surrounding tissue by means of an insulating layer or structural features, and that they are often contain expensive single-use compartments, raising surgery costs significantly. Hence, an alternative process avoiding or minimizing single-use components providing intraoperative bleeding control in at least a fraction of surgical situations might support cost-effectiveness in the healthcare sector, with similar performance provided.
Blood is composed of several components (Figure 1). Hemostasis is the process of blood clotting at the site of an injury [11], and its molecular mechanisms have been outlined in detail [12,13]. Briefly, hemostasis is a complex orchestrated process that can be subdivided into primary (cellular) and secondary (plasmatic) hemostasis. During primary hemostasis, platelets become activated, involving multiple ligands and downstream signaling of various activated membrane receptors [14]. This results in versatile morphological changes enabling cross-linking of activated platelets, which form an initial white clot. In the following, the plasmatic hemostasis involves to cleavage of the protein fibrinogen to fibrin, which further stabilizes the clot [15]. Due to the many molecules involved in hemostasis, some components and their roles in this process are still not fully understood. For instance, several molecular functions in the process of hemostasis, such as integrin binding, are subject to redox control, as evident by functional disulfide bonds [16], suggesting a role of reactive oxygen and nitrogen species (ROS/RNS).
In 2005, the impact of a novel technology, medical gas plasmas, on blood hemostasis was first reported [17]. Often referred to as the fourth state of matter, gas plasmas are generated by ionizing gases using sufficient energy or temperature supply [18]. Medical gas plasma technology is a multi-component tool featuring a variety of factors, including UV radiation, electric field, and a versatile mix of ROS/RNS being generated simultaneously [19]. All these components are known to have biological consequences when applied at sufficient doses. However, it is established that gas plasma-mediated effects primarily depend on the generation of ROS/RNS [20,21]. The technical leap innovation was the ability to generate gas plasmas at body temperature, distinguishing them from other hemostatic techniques such as electrocauterization or argon plasma coagulation (hotter plasmas way above body temperature) [22]. Until today, several medical product class IIa approved gas plasma devices are available, primarily indicated for disease control and wound healing support in dermatology [23]. Gas plasma jets are of particular interest because of their pencil/scalpel-like utilization across bodily surfaces.
Multiple experimental studies have successfully demonstrated the ability of gas plasmas to serve as hemostatic agents, and several mechanisms have been proposed, with platelet activation receiving particular emphasis [24]. This mini-review aims to summarize the current knowledge on gas plasma-mediated blood coagulation to highlight their potential to be applied for intraoperative bleeding control, providing important implications for possible clinical applications in the future.
2. Platelets in Cellular Blood Hemostasis
2.1. Platelet Functional Morphology
Platelets are non-nucleated cells that arise from the strangulation of megakaryocytes in the bone marrow as well as in the lungs and are released into the bloodstream [25,26], where they circulate for approximately 8–12 days until they are degraded by splenic macrophages or liver Kupffer cells [27]. They play an essential role in blood hemostasis and further immune defense and control of inflammation [28]. Notwithstanding their biological relevance, platelets account for only 7% of all cellular blood components, compared to 93% by red blood cells (erythrocytes) (Figure 1). Platelets are highly adapted to their functions by their structure. Being discoid in shape, they have an overall size of 1.5–3 µM. Their outer region, the so-called hyalomer, is devoid of organelles but enriched with actin filaments and a circumferential band of microtubules, which together enable significant morphological changes upon platelet activation [29]. Platelets contain numerous vesicles, which can be further subdivided into alpha, delta, and lambda-granules (=lysosomes) that are collectively called granulomeres. Alpha and delta granules store various molecules that aid in blood hemostasis, whereas lysosomes contain enzymes involved in the degradation of pathogens. Vesicle exocytosis is facilitated by deep membrane invaginations, the open canalicular system (OCS) [30,31]. Although platelets lack transcribable genetic information due to the lack of a nucleus, they are stunningly still capable of protein biosynthesis as they are equipped with ribosomes, mRNA, and mitochondria of their precursors. Likewise, their internal Ca2+ storage, the dense tubular system, originates from the smooth endoplasmic reticulum of the megakaryocyte [32].
2.2. Primary Hemostasis
Primary hemostasis starts with vasoconstriction within seconds after vascular damage. Thereby, blood flow can be diminished at the side of vascular lesion, and the resulting increase in shear stress promotes platelet adhesion. Platelet adhesion is initiated by the interaction of subendothelial collagen with a blood circulating protein called von Willebrand factor (vWF) produced by endothelial cells and megakaryocytes. Upon endothelial damage in vascular lesions, subendothelial collagen is exposed, and binding of vWF occurs under sufficient pressure and shear-stress conditions [33]. In arterial lesions, vWF serves as a cross-linker between exposed connective tissue and circulating platelets that express a glycoprotein receptor (GPIb-IX-V receptor complex) with specified binding sides for vWF [34,35]. Thus, a first layer of platelets is formed that covers the endothelial damage and further induces activation of multiple hemostatic components [36].
2.3. Signaling Involved in Platelet Activation
Platelet activation is a complex orchestrated process in which various intracellular biochemical reactions cause versatile changes, including the formation of pseudopodia, alterations of the plasma membrane, and release of vesicles [14]. This serves to recruit additional platelets, which attach to the first layer, forming a cross-linked white thrombus that is later solidified by the formation of fibrin [37]. The involved signaling cascades are highly interconnected and predominantly mediated by G-coupled proteins that consist of different subunits and exhibit different functions. Further, various other platelet receptors, e.g., immunoreceptor tyrosine-based activation motif (ITAM) receptors, ligand-dependent ion channels, and glycoprotein receptor complexes, contribute to their impressive ability to react within seconds after a blood vessel’s endothelial wall is disrupted [38].
Several platelet receptors, including the adenosine diphosphate (ADP)-responsive purinergic receptors P2Y12 [39] and P2Y1 [40], the thromboxane receptor TxA2-R [41], and the thrombin protease-activated receptors PAR1/4 [42], are coupled to Gq/Gi proteins. Gq/Gi-induced activation of phospholipase C-β (PLC-β) initiates cleavage of phosphatidylinositol-4,5-bisphosphate (PIP2), a phospholipid mainly located in the inner cell membrane under the emergence of diacylglycerol (DAG) and inositol triphosphate (IP3) [43]. The second messenger DAG further activates protein kinase C (PKC), followed by signaling involved in thromboxane A2 synthesis, vesicle secretion, and activation of phosphodiesterase (PDE) [44]. Upon binding to IP3 receptors located at the dense tubular system, IP3 initiates the distribution of intracellular Ca2+ [45,46].
Besides Gq-mediated signaling, coupling of PAR1/4 to G13 proteins induces activation of the small GTPase Rho, which is crucial for changes in platelet shape [42]. Rho mediates actin polymerization and increases myosin light chain kinase (MLCK) activity by inhibiting its opponent myosin light chain phosphatase (MLCP). Together with increased intracellular Ca2+ level downstream PLC-β activation, this facilitates actin–myosin interactions [43,47].
Integrin activation downstream phosphoinositide 3-kinase (PI3K) signaling is needed for sufficient cellular cross-linking during clot formation [48,49]. PI3K can be activated by Gi proteins [50], but also through glycoprotein VI (GPVI) and the receptor complex GPIb-IX-V [51]. GPVI is a member of the immunoglobulin (Ig) superfamily present on platelets and an established receptor for cellular cross-linking upon contact with collagen [52]. The GPIb-IX-V complex, part of the leucine-rich repeat (LRR) family, is activated upon binding of vWF and essential for platelet adhesion under high shear stress conditions. GPIV-IX-V signaling requires cooperativity of PAR1/4 and vice versa, making the interconnection of both receptors an important driver of platelet activation, especially at low thrombin concentrations [53]. Secondly, PI3K activation can cause increased formation of nitric oxide (NO.) by NO. synthase (NOS) via Akt [54]. Being an uncharged gas, NO. can diffuse across cell membranes and plays a biphasic role in blood hemostasis [55]. Initially, it promotes platelet activation via soluble guanylate cyclase (sGC)/PKG/p38 [47,56], whereas, as blood coagulation progresses, it acts as a suppressant to hemostasis [57].
Platelet activation is finely regulated and can be counteracted by protein kinase A (PKA) signaling. PKA is activated by cyclic adenosine monophosphate (cAMP), which emerges from the cleavage of adenosine triphosphate (ATP) by adenylate cyclase (AC) [58]. PKA mediates multiple responses, such as reducing the intracellular Ca2+ concentration and subsequently decreasing platelet shape change [59]. During primary hemostasis, AC is inhibited downstream signaling of the epinephrine receptor α2A, the prostacyclin (PIG2) receptor, and P2Y12 [60,61] (Figure 2).
2.4. Secondary Hemostasis
Secondary (plasmatic) hemostasis results in the formation of macromolecular complexes of fibrin that further solidify the initial platelet plug [62]. This involves a variety of zymogens (inactive precursors), mainly serine proteases, cofactors, and fibrinogen. Serial activation and feedback amplification loops end in the central conversion of fibrinogen to fibrin by thrombin. This enables covalent cross-linking of individual fibrin molecules to form a stable complex in which platelets and erythrocytes become trapped. Dependent on the initial trigger factor, the stated signaling cascades can be further subdivided into an intrinsic or extrinsic pathway that finally ends up in a common path [63] (Figure 3).
3. Medical Gas Plasma as a Hemostatic Agent
Blood coagulation by medical gas plasma was first described more than 10 years ago [17]. Since then, many studies have emphasized the pro-coagulant potential of medical gas plasmas on blood from healthy donors. Moreover, sufficient hemostasis has been achieved in vivo on mouse saphenous veins [64], rat and mouse livers [8,65,66], and rabbit spleens [67], as well as acute skin wounds of mice and pigs [68,69] (Table A1).
Initially, the clot-promoting effect was attributed to the provision of Ca2+, which initiates platelet activation and enables versatile platelet shape changes [70]. This was suggested as ethylene diamine tetraacetic acid (EDTA)-anticoagulated blood samples, which exhibit decreased free Ca2+ concentration due to chelation, showed increased platelet activation upon medical gas plasma treatment compared to heparin-anticoagulated blood [71]. However, the role of free Ca2+ was further refuted by subsequent studies observing that Ca2+ fluctuations only occur at longer treatment times and thus cannot contribute to the early processes of blood coagulation since visible coagulation processes occur before that [72]. At the same time, dominating effects of temperature and electric field effects were negated, which distinguished gas plasma-mediated blood coagulation clearly from clinically employed argon plasma coagulation (hot plasma) or electrocauterization. Conversely, the suggestion was that medical gas plasma instead interferes in plasmatic hemostasis by direct cleavage of fibrinogen as the aggregate formation of a fibrinogen solution could be observed after gas plasma exposure. In addition, histopathologically visible membrane formation was noted in samples obtained after bleeding control using medical gas plasmas in C57BL/6 mice, and protein aggregation was further investigated. However, scanning electron microscopy (SEM) and macroscopic examination of platelet-rich plasma (PRP) already revealed a pro-coagulant effect on platelets directly, though the underlying mechanisms remained unclear [65,68].
In other biomedical research areas, including wound healing or oncology, gas plasma-mediated effects have been mainly linked to the variety of ROS/RNS being generated simultaneously [20]. Along those lines, it seemed evident that ROS/RNS also play a significant role in gas plasma-mediated platelet activation. In most in vitro gas plasma applications using gas plasma jets, a dominating role of long-lived species such as hydrogen peroxide (H2O2) [73] and hypochlorous acid (HOCl) [74] is evident. Hence, it seemed plausible that addition of these agents would recapitulate the hemostatic action of gas plasma treatment. Surprisingly, this was not the case, independent of the concentration that was added [24]. Vice versa, scavenging of H2O2 via catalase also failed to protect from gas plasma-mediated hemostasis. In general, due to their high reactivity, the influence of short-lived ROS is challenging to control. The influence of superoxide anions (O2.-) in thrombin-mediated platelet activation has been documented [75,76], but scavenging thereof using superoxide dismutase (SOD) could not reduce gas plasma-mediated platelet activation. In the same view, increased platelet aggregation has been observed when exposing PRP to gaseous ozone [77]. NO. is abundantly generated by gas plasma jets [78], being known for its pleiotropic functions in hematology [79], and its role concerning plasma-mediated effects has been discussed [55,57,80]. Diffusion of NO. across the platelet membrane enables platelet activation via sGC, PKG, and p38 activation initially [47,56,57] but acts inhibitory as blood coagulation progresses [57]. However, NO. can additionally react with free oxygenated hemoglobin (Hb) to form Met-Hb and nitrate as a major pathway for NO. elimination in our body [81], which reduces the bioavailability of the latter [82]. In addition to related signal transduction processes in the platelet, this restricts the contribution of NO. to the onset of gas plasma coagulation. Still, the direct effect of gas plasma on platelet activation can only account for a fraction of hemostatic activity observed, which is reasoned with regard to the proportionate biomass among the total hematocrit [24] (Figure 1).
In the course of studying the side effects of medical gas plasma treatment, lysis of blood cells was investigated early already, although cell types seemed to be affected to different degrees [83]. Likewise, Miyamoto and colleagues described membrane formation from lysed erythrocytes as a second mechanism of action, but differences were found depending on the plasma source used [84]. However, in this case, blood coagulation was only traced to the coagulant membrane formation, and platelets’ importance was not further discussed. In 2017, platelets were suggested being the primary mediators of gas plasma-initiated hemostasis, which was demonstrated by using clopidogrel anticoagulation, an inhibitor of platelet aggregation [8]. Strikingly, it was found that platelet activation’s central trigger could be attributed to hemolysis in response to gas plasma exposure [24]. This was demonstrated because the coagulating effect was enhanced in whole blood (WB) compared to platelet-rich plasma (PRP). Furthermore, the blood coagulation could be mimicked by adding equal concentrations of an isotonic hemolysate to WB. Hemolysis as a mediator of platelet activation has been addressed and discussed before in the pathogenesis of vaso-occlusive diseases [85].
During hemolysis, various molecules and DAMPs (damage-associated molecular patterns) are being released, such as hemoglobin, heme, and the nucleotides ADP and ATP [85,86]. The latter can act directly at platelet receptors, thereby activating platelets [87]. In line with this, inhibition of gas plasma coagulation by clopidogrel, whose active metabolite inhibits the ADP receptor P2Y12, was described previously [8,88]. P2Y12 is a Gi-protein coupled receptor whose β/γ subunit can initiate PI3K/Akt/p38 signaling upon activation [47,50] and was later identified as a central pathway. By using Ly294002, a PI3K inhibitor, a decrease in gas plasma-mediated platelet activation by 56% was observed, equaling the predetermined percentage attributed to hemolysis [89]. Using inhibitors of different isoforms of PLC, the contribution of Gq-mediated signaling upon gas plasma exposure could be excluded [43]. In patients with sickle cell disease, free hemoglobin could lead to platelet activation associated with hyperpolarization of the mitochondrial membrane and increased intracellular ROS production. This has been attributed to inhibiting complex V respiratory chain activity [90]. A similar mode of action could be suggested, as hyperpolarization of mitochondrial membrane potential has been observed upon gas plasma exposure [24] (Figure 4).
Studies in various pre-clinical models successfully demonstrated the potential of medical gas plasmas as a putative hemostatic agent for clinical application. Contrary to suggestions made in the beginning, direct effects of gas plasma treatment on either cellular or plasmatic hemostasis as critical drivers of blood coagulation were less observed. Instead, platelet activation could be traced back to ROS/RNS-induced hemolysis, resulting in the local release of hemostatic DAMPs. This directly contrasts with currently applied electrocauterization or argon plasma coagulation that achieves blood hemostasis by tissue carbonization at the injured side.
4. Application Fields and Clinical Obstacles
Medical gas plasma technology provides hemostasis in a localized, controlled, and specific manner when applied to the injured side. Major advantages include preserving tissue integrity, few side effects, and restoring physiological tissue structure (restitutio ad integrum), which is emphasized by long-term studies in vivo [66,67]. In this view, the application of medical gas plasma is particularly eligible for hemostasis in sensitive tissues and several types of surgery in, e.g., unintended colon tissue damage during laporscopy or laparotomie, neurosurgical procedures, or cerebral microhemorrhages (CMBs).
In gastrointestinal surgery, partial hepatectomy is associated with high mortality and morbidity rates. Patients are at particular risk for secondary bleeding, infection, and loss of liver function due to deficient surgical bleeding control [91]. Healing courses after liver and splenic resection in experimental mouse and rabbit models indicated few side effects of intra-operative bleeding control using medical gas plasma technology. Further, physiological tissue structure could be preserved, preventing major loss of functional tissue [66,67] and emphasizing gastrointestinal surgery as a feasible application field for gas plasma-mediated blood coagulation. Preservation of functional tissue and tissue integrity is not only relevant concerning long-term follow up of patients undergoing surgical procedures. Surgical procedures that put patients at high risk for severe post-operative bleedings after sloughing of eschar, such as tonsillectomy [92], could benefit from medical gas plasma technology along similar lines.
Besides surgical application fields, the ability of medical gas plasma to induce fast, local hemolysis with subsequent platelet activation and blood hemostasis could be used to stop acute bleeding, such as epistaxis originating from small artery ruptures located in the Kiesselbach’s plexus. Moreover, portable medical gas plasma devices could be a significant relief for hemophilia patients. Due to a mostly inherited genetic disorder, the process of plasmatic hemostasis is heavily impaired in those patients. By that, spontaneous bleedings occur, often without any preceding visible injuries. Fast local control of such bleedings using medical gas plasma as a home care device could be a relevant, liberating benefit.
Further advantages of medical gas plasma technology include simultaneous disinfection and promotion of wound healing and bleeding control, which have already been addressed in the treatment of chronic wounds [93]. In this regard, another potential benefit could be provided by applying cold physical plasma to acute nonsterile skin wounds. Clinical practice dictates open-wound care for nonsterile wounds or treatment with long-lasting vacuum-assisted wound closure, which requires inpatient treatment or drainage. Due to antimicrobial effects, blood coagulation, and wound healing stimulation, it would be conceivable to provide wound care using gas plasmas [23] (Figure 5).
As overshooting ROS production is linked to increased autoimmunity and the pathogenesis of many other diseases, questioning immune-mediated complications upon exposure to gas plasma-derived ROS seems evident. Antigen-independent proliferation of T cells or generation of neo-cryptic epitopes, which might serve as autoantigens, could put patients at risk for autoimmune reactions. Medical accredited plasma devices have been investigated in clinical trials for wound care since 2010 [94], and clinical data exist from multiple dermatological centers in central Europe. Until now, no evidence indicates increased occurrence of adverse side effects and has neither been reported in follow-up studies in patients [95] nor in mice [96]. Moreover, T-cell-driven skin sensitization could not be observed in a standardized murine model after repeated gas plasma exposure using an OECD accredited assay [97]. It is suggested that the generated ROS mixture does not drive non-specific, redox-mediated T-cell activation, and neither increased phosphorylation of NF-κB [98] nor proliferation [99] could be observed in viable TH cells upon gas plasma treatment per se.
Disadvantages of medical gas plasma predominantly concern application practice, physicochemical heterogeneity of available plasma sources, sterilization, and economic questions. Plasma jet devices require a continuous supply of an inert gas (e.g., argon), which increases treatment costs. However, the expenses should be covered by a few Euros per application. It should be noted that gas plasma treatment is currently under observation of the national health council for cost reimbursement by social healthcare insurance providers, at least in Germany. It is worth noting that available and clinically approved plasma sources differ with regard to the expelled ROS/RNS chemistry [20]. While the chemistry of some sources such as plasma jets is dominated, for instance, by singlet delta and atomic oxygen as well as ozone, other accredited devices such as the DBDs have been found to generate high amounts of NO2 [74,100]. In addition, new application fields, e.g., care of internal bleedings, would require creating suitable endoscopic devices that have been designed by research centers without entering clinical practice [101,102,103]. Moreover, sterilization of gas plasma applicators is a compelling basis for widespread application during surgeries that have to be taken into account. Finally, the scalpel-like application of plasma jets is better suited for hemostatic action in the clinics that flat-shaped dielectric barrier discharges. A scheme of the thus far only plasma jet device approved in Europe for medical applications, the kINPen MED, is shown below (Figure 6). It has been found that direct connection of the plasma jet with its target (Figure 6, right image), such as a bleeding wound, is much more potent that the remote deposition of the cloud of ROS being generated [104].
5. Conclusions
Medical gas plasma has excellent potential to serve as a hemostatic agent with advantages over existing procedures. Intensive research has demonstrated its potential in different application fields, and underlying mechanisms have become increasingly well understood. As a novel potential component of surgical blood hemostasis, gas plasma-induced hemolysis initiates platelet activation via local DAMP release. Upon receptor binding, DAMPS, including hemoglobin or ADP, induce biological downstream signaling, resulting in morphological changes and the release of pro-hemostatic granules by platelets. By that, medical gas plasma provides gentle and physiological blood coagulation and enables the restoration of functional tissue structures. However, investigation of this technology within clinical trials or individual healing attempts on the hemostatic activity of medical gas plasmas are absent thus far. In this light, studying the hemostatic efficacy in humans compared to gold-standard therapies would be worth of being addressed, together with potential pitfalls in the application practice before medical gas plasma treatments can be implemented in clinical care.
Author Contributions
Conceptualization, S.B.; methodology, L.M. and B.P.; resources, S.B.; writing—original draft preparation, L.M., B.P. and S.B.; writing—review and editing, J.v.d.L.; visualization, L.M., B.P. and S.B.; supervision, S.B. and J.v.d.L.; project administration, S.B.; funding acquisition, S.B. All authors have read and agreed to the published version of the manuscript.
Funding
The work was supported by the German Federal Ministry of Education and Research (BMBF, grant number 03Z22DN11 to SB) and the Gerhard-Domagk-Foundation Greifswald, Germany, supporting L.M. and B.P.
Conflicts of Interest
The authors declare no conflict of interest.
Appendix A

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Table A1.
Overview of blood coagulation studies using gas plasma technology, and main findings, sorted by date of appearance. H = human; P = porcine; M = murine; R = rat; Rb = rabbit; D = dog; PRP = platelet-rich blood plasma; PPP = platelet-poor blood plasma.
Table A1.
Overview of blood coagulation studies using gas plasma technology, and main findings, sorted by date of appearance. H = human; P = porcine; M = murine; R = rat; Rb = rabbit; D = dog; PRP = platelet-rich blood plasma; PPP = platelet-poor blood plasma.
| Ref. | Plasma Source | Sample | Species | Main Findings |
|---|---|---|---|---|
| Ex Vivo | ||||
| Fridman et al. (2005) [17] | DBD | - | H |
|
| Fridman et al. (2006) [70] | FE-DBD | PRP, spleen | H | suggested mechanism:
|
| Kalghatgi et al. (2007) [72] | FE-DBD | WB, fibrinogen solution | H |
|
| Chen-Yen et al. [105] (2009) | Plasma jet | WB, PPP, PRP | H |
|
| Dobrynin et al. (2011) [69] | FE-DBD, pin-to-hole spark discharge | skin wound | P |
|
| Baik et al. [83] (2012) | Plasma jet | WB | D |
|
| Miyamoto et al. (2016) [84] | Plasma-Jet (He), BPC-HP1, PN-110/120TPG | WB, isolated RBCs | H |
|
| Bekeschus et al. (2018) [71] | kINPen and kINPen MED (various feed gas admixtures) | WB | H |
suggested mechanism:
|
| Bekeschus et al. (2021) [24] | kINPen and kINPen MED | PRP, WB, BL | H | suggested mechanism:
|
| Jia et al. (2021) [106] | microsecond-pulsed helium plasma jet | WB, PRP | R | suggested mechanism:
|
| in vivo | ||||
| Fridman et al. (2008) [64] | FE-DBD | vena saphena/WB (anticoagulated) | M/H |
|
| Ikehara et al. (2013 [65]) | Plasma jet | femoral artery | M |
|
| Ikehara et al. (2015) | Plasma jet | proteins in buffer solution, skin wound | M |
|
| Aleinik et al. (2017) [66] | DBD | hepatectomy | R |
|
| Nomura et al. (2017) [107] | plasma jet, various gas admixtures | WB, gastric, and liver incision | H/P |
|
| Bekeschus et al. (2017) [8] | kINPen MED | WB, liver incision model | M |
|
| Aleinik et al. (2018) [67] | DBD | splenic surgery | Rb |
|
| Yan et al. (2018) [108] | microsecond-pulsed helium plasma jet | WB, hepatectomy | R |
|
| Rad et al. (2018) [109] | helium plasma jet | liver incision model | M |
|
References
- Porte, R. The risk of bleeding during liver surgery and liver transplantation and effect on outcome. Bloodline Rev. 2001, 1, 14–15. [Google Scholar]
- Nesbakken, A.; Nygaard, K.; Westerheim, O.; Lunde, O.C.; Mala, T. Audit of intraoperative and early postoperative complications after introduction of mesorectal excision for rectal cancer. Eur. J. Surg. 2002, 168, 229–235. [Google Scholar] [CrossRef] [PubMed]
- Copeland, G.P.; Jones, D.; Walters, M. Possum: A scoring system for surgical audit. Br. J. Surg. 1991, 78, 355–360. [Google Scholar] [CrossRef]
- Boyd, C.R.; Tolson, M.A.; Copes, W.S. Evaluating trauma care: The triss method. Trauma score and the injury severity score. J. Trauma 1987, 27, 370–378. [Google Scholar] [PubMed]
- Marietta, M.; Facchini, L.; Pedrazzi, P.; Busani, S.; Torelli, G. Pathophysiology of bleeding in surgery. Transplant. Proc. 2006, 38, 812–814. [Google Scholar] [CrossRef] [PubMed]
- Lynn, M.; Jeroukhimov, I.; Klein, Y.; Martinowitz, U. Updates in the management of severe coagulopathy in trauma patients. Intensive Care Med. 2002, 28 (Suppl. S2), S241–S247. [Google Scholar] [CrossRef] [PubMed]
- Raiser, J.; Zenker, M. Argon plasma coagulation for open surgical and endoscopic applications: State of the art. J. Phys. D Appl. Phys. 2006, 39, 3520–3523. [Google Scholar] [CrossRef]
- Bekeschus, S.; Brüggemeier, J.; Hackbarth, C.; von Woedtke, T.; Partecke, L.-I.; van der Linde, J. Platelets are key in cold physical plasma-facilitated blood coagulation in mice. Clin. Plas. Med. 2017, 7–8, 58–65. [Google Scholar] [CrossRef]
- Carus, T.; Rackebrandt, K. Collateral tissue damage by several types of coagulation (monopolar, bipolar, cold plasma and ultrasonic) in a minimally invasive, perfused liver model. ISRN Surg. 2011, 2011, 518924. [Google Scholar] [CrossRef] [Green Version]
- Castell, D.O. Consensus statement on therapeutic endoscopy and bleeding ulcers. Gastrointest. Endosc. 1990, 36, S62–S65. [Google Scholar]
- Lawson, J.H.; Murphy, M.P. Challenges for providing effective hemostasis in surgery and trauma. Semin. Hematol. 2004, 41, 55–64. [Google Scholar] [CrossRef] [PubMed]
- Mussbacher, M.; Kral-Pointner, J.B.; Salzmann, M.; Schrottmaier, W.C.; Assinger, A. Mechanisms of hemostasis: Contributions of platelets, coagulation factors, and the vessel wall. In Fundamentals of Vascular Biology; Geiger, M., Ed.; Springer International Publishing: Cham, Switzerland, 2019; pp. 145–169. [Google Scholar]
- Valsami, S.; Asmis, L.M. A brief review of 50 years of perioperative thrombosis and hemostasis management. Semin. Hematol. 2013, 50, 79–87. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yun, S.H.; Sim, E.H.; Goh, R.Y.; Park, J.I.; Han, J.Y. Platelet activation: The mechanisms and potential biomarkers. Biomed. Res. Int. 2016, 2016, 9060143. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Guzzetta, N.A.; Miller, B.E. Principles of hemostasis in children: Models and maturation. Paediatr. Anaesth. 2011, 21, 3–9. [Google Scholar] [CrossRef]
- Mor-Cohen, R. Disulfide bonds as regulators of integrin function in thrombosis and hemostasis. Antioxid. Redox Signal. 2016, 24, 16–31. [Google Scholar] [CrossRef]
- Fridman, G.; Peddinghaus, M.; Fridman, A.; Balasubramanian, M.; Gutsol, A.; Friedman, G. Use of Non-Thermal Atmospheric Pressure Plasma Discharge for Coagulation and Sterilization of Surface Wounds. In Proceedings of the 32nd IEEE International Conference on Plasma Science, Traverse City, MI, USA, 4–8 June 2005; p. 257. [Google Scholar]
- Langmuir, I. Oscillations in ionized gases. Proc. Natl. Acad. Sci. USA 1928, 14, 627–637. [Google Scholar] [CrossRef] [Green Version]
- Reuter, S.; von Woedtke, T.; Weltmann, K.D. The kinpen-a review on physics and chemistry of the atmospheric pressure plasma jet and its applications. J. Phys. D Appl. Phys. 2018, 51, 233001. [Google Scholar] [CrossRef] [Green Version]
- Privat-Maldonado, A.; Schmidt, A.; Lin, A.; Weltmann, K.D.; Wende, K.; Bogaerts, A.; Bekeschus, S. Ros from physical plasmas: Redox chemistry for biomedical therapy. Oxid. Med. Cell. Longev. 2019, 2019, 9062098. [Google Scholar] [CrossRef] [Green Version]
- Von Woedtke, T.; Schmidt, A.; Bekeschus, S.; Wende, K.; Weltmann, K.D. Plasma medicine: A field of applied redox biology. In Vivo 2019, 33, 1011–1026. [Google Scholar] [CrossRef] [Green Version]
- Graves, D.B. Low temperature plasma biomedicine: A tutorial review. Phys. Plasmas 2014, 21, 080901. [Google Scholar] [CrossRef] [Green Version]
- Bekeschus, S.; von Woedtke, T.; Emmert, S.; Schmidt, A. Medical gas plasma-stimulated wound healing: Evidence and mechanisms. Redox Biol. 2021, 46, 102116. [Google Scholar] [CrossRef] [PubMed]
- Bekeschus, S.; Poschkamp, B.; van der Linde, J. Medical gas plasma promotes blood coagulation via platelet activation. Biomaterials 2021, 278, 120433. [Google Scholar] [CrossRef] [PubMed]
- Scurfield, G.; Radley, J.M. Aspects of platelet formation and release. Am. J. Hematol. 1981, 10, 285–296. [Google Scholar] [CrossRef]
- Lefrancais, E.; Ortiz-Munoz, G.; Caudrillier, A.; Mallavia, B.; Liu, F.; Sayah, D.M.; Thornton, E.E.; Headley, M.B.; David, T.; Coughlin, S.R.; et al. The lung is a site of platelet biogenesis and a reservoir for haematopoietic progenitors. Nature 2017, 544, 105–109. [Google Scholar] [CrossRef] [PubMed]
- Lebois, M.; Josefsson, E.C. Regulation of platelet lifespan by apoptosis. Platelets 2016, 27, 497–504. [Google Scholar] [CrossRef] [PubMed]
- Vieira-de-Abreu, A.; Campbell, R.A.; Weyrich, A.S.; Zimmerman, G.A. Platelets: Versatile effector cells in hemostasis, inflammation, and the immune continuum. Semin. Immunopathol. 2012, 34, 5–30. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- White, J.G.; Krumwiede, M.; Burris, S.M.; Heagan, B. Isolation of microtubule coils from platelets after exposure to aggregating agents. Am. J. Pathol. 1986, 125, 319–326. [Google Scholar]
- White, J.G.; Clawson, C.C. The surface-connected canalicular system of blood platelets—A fenestrated membrane system. Am. J. Pathol. 1980, 101, 353–364. [Google Scholar]
- White, J.G. Platelets are covercytes, not phagocytes: Uptake of bacteria involves channels of the open canalicular system. Platelets 2005, 16, 121–131. [Google Scholar] [CrossRef]
- Rosado, J.A. Acidic ca(2+) stores in platelets. Cell Calcium 2011, 50, 168–174. [Google Scholar] [CrossRef]
- Farndale, R.W.; Sixma, J.J.; Barnes, M.J.; de Groot, P.G. The role of collagen in thrombosis and hemostasis. J. Thromb. Haemost. 2004, 2, 561–573. [Google Scholar] [CrossRef] [PubMed]
- Di Stasio, E.; De Cristofaro, R. The effect of shear stress on protein conformation: Physical forces operating on biochemical systems: The case of von willebrand factor. Biophys. Chem. 2010, 153, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Siedlecki, C.A.; Lestini, B.J.; Kottke-Marchant, K.K.; Eppell, S.J.; Wilson, D.L.; Marchant, R.E. Shear-dependent changes in the three-dimensional structure of human von willebrand factor. Blood 1996, 88, 2939–2950. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Reininger, A.J.; Heijnen, H.F.; Schumann, H.; Specht, H.M.; Schramm, W.; Ruggeri, Z.M. Mechanism of platelet adhesion to von willebrand factor and microparticle formation under high shear stress. Blood 2006, 107, 3537–3545. [Google Scholar] [CrossRef]
- Tomaiuolo, M.; Brass, L.F.; Stalker, T.J. Regulation of platelet activation and coagulation and its role in vascular injury and arterial thrombosis. Interv. Cardiol. Clin. 2017, 6, 1–12. [Google Scholar] [CrossRef] [Green Version]
- Clemetson, K.J.; Clemetson, J.M. Platelet receptor signalling. Hematol. J. 2004, 5 (Suppl. S3), S159–S163. [Google Scholar] [CrossRef]
- Hollopeter, G.; Jantzen, H.M.; Vincent, D.; Li, G.; England, L.; Ramakrishnan, V.; Yang, R.B.; Nurden, P.; Nurden, A.; Julius, D.; et al. Identification of the platelet adp receptor targeted by antithrombotic drugs. Nature 2001, 409, 202–207. [Google Scholar] [CrossRef] [Green Version]
- Ayyanathan, K.; Webbs, T.E.; Sandhu, A.K.; Athwal, R.S.; Barnard, E.A.; Kunapuli, S.P. Cloning and chromosomal localization of the human P2Y1 purinoceptor. Biochem. Biophys. Res. Commun. 1996, 218, 783–788. [Google Scholar] [CrossRef]
- Hirata, M.; Hayashi, Y.; Ushikubi, F.; Yokota, Y.; Kageyama, R.; Nakanishi, S.; Narumiya, S. Cloning and expression of cdna for a human thromboxane A2 receptor. Nature 1991, 349, 617–620. [Google Scholar] [CrossRef]
- Xu, W.F.; Andersen, H.; Whitmore, T.E.; Presnell, S.R.; Yee, D.P.; Ching, A.; Gilbert, T.; Davie, E.W.; Foster, D.C. Cloning and characterization of human protease-activated receptor 4. Proc. Natl. Acad. Sci. USA 1998, 95, 6642–6646. [Google Scholar] [CrossRef] [Green Version]
- Stalker, T.J.; Newman, D.K.; Ma, P.; Wannemacher, K.M.; Brass, L.F. Platelet signaling. In Handbook of Experimental Pharmacology; Springer: Berlin/Heidelberg, Germany, 2012; pp. 59–85. [Google Scholar] [CrossRef] [Green Version]
- Harper, M.T.; Poole, A.W. Diverse functions of protein kinase c isoforms in platelet activation and thrombus formation. J. Thromb. Haemost. 2010, 8, 454–462. [Google Scholar] [CrossRef] [PubMed]
- Bergmeier, W.; Stefanini, L. Novel molecules in calcium signaling in platelets. J. Thromb. Haemost. 2009, 7 (Suppl. S1), 187–190. [Google Scholar] [CrossRef] [PubMed]
- Shattil, S.J.; Kim, C.; Ginsberg, M.H. The final steps of integrin activation: The end game. Nat. Rev. Mol. Cell Biol. 2010, 11, 288–300. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Li, Z.; Delaney, M.K.; O’Brien, K.A.; Du, X. Signaling during platelet adhesion and activation. Arterioscler. Thromb. Vasc. Biol. 2010, 30, 2341–2349. [Google Scholar] [CrossRef] [Green Version]
- Guidetti, G.F.; Canobbio, I.; Torti, M. Pi3k/akt in platelet integrin signaling and implications in thrombosis. Adv. Biol. Regul. 2015, 59, 36–52. [Google Scholar] [CrossRef]
- Pasquet, J.M.; Bobe, R.; Gross, B.; Gratacap, M.P.; Tomlinson, M.G.; Payrastre, B.; Watson, S.P. A collagen-related peptide regulates phospholipase cγ2 via phosphatidylinositol 3-kinase in human platelets. Biochem. J. 1999, 342, 171–177. [Google Scholar] [CrossRef]
- Hirsch, E.; Bosco, O.; Tropel, P.; Laffargue, M.; Calvez, R.; Altruda, F.; Wymann, M.; Montrucchio, G. Resistance to thromboembolism in pi3kγ-deficient mice. FASEB J. 2001, 15, 2019–2021. [Google Scholar] [CrossRef]
- Watanabe, N.; Nakajima, H.; Suzuki, H.; Oda, A.; Matsubara, Y.; Moroi, M.; Terauchi, Y.; Kadowaki, T.; Suzuki, H.; Koyasu, S.; et al. Functional phenotype of phosphoinositide 3-kinase p85α-null platelets characterized by an impaired response to gp vi stimulation. Blood 2003, 102, 541–548. [Google Scholar] [CrossRef] [Green Version]
- Clemetson, K.J.; McGregor, J.L.; James, E.; Dechavanne, M.; Luscher, E.F. Characterization of the platelet membrane glycoprotein abnormalities in bernard-soulier syndrome and comparison with normal by surface-labeling techniques and high-resolution two-dimensional gel electrophoresis. J. Clin. Investig. 1982, 70, 304–311. [Google Scholar] [CrossRef] [Green Version]
- Berndt, M.C.; Gregory, C.; Kabral, A.; Zola, H.; Fournier, D.; Castaldi, P.A. Purification and preliminary characterization of the glycoprotein ib complex in the human platelet membrane. Eur. J. Biochem. 1985, 151, 637–649. [Google Scholar] [CrossRef]
- Woulfe, D.S. Akt signaling in platelets and thrombosis. Expert Rev. Hematol. 2010, 3, 81–91. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lancaster, J.R., Jr. A tutorial on the diffusibility and reactivity of free nitric oxide. Nitric Oxide 1997, 1, 18–30. [Google Scholar] [CrossRef] [PubMed]
- Dangel, O.; Mergia, E.; Karlisch, K.; Groneberg, D.; Koesling, D.; Friebe, A. Nitric oxide-sensitive guanylyl cyclase is the only nitric oxide receptor mediating platelet inhibition. J. Thromb. Haemost. 2010, 8, 1343–1352. [Google Scholar] [CrossRef] [PubMed]
- Li, Z.; Xi, X.; Gu, M.; Feil, R.; Ye, R.D.; Eigenthaler, M.; Hofmann, F.; Du, X. A stimulatory role for cgmp-dependent protein kinase in platelet activation. Cell 2003, 112, 77–86. [Google Scholar] [CrossRef] [Green Version]
- Smolenski, A. Novel roles of camp/cgmp-dependent signaling in platelets. J. Thromb. Haemost. 2012, 10, 167–176. [Google Scholar] [CrossRef] [Green Version]
- El-Daher, S.S.; Patel, Y.; Siddiqua, A.; Hassock, S.; Edmunds, S.; Maddison, B.; Patel, G.; Goulding, D.; Lupu, F.; Wojcikiewicz, R.J.; et al. Distinct localization and function of (1,4,5)ip(3) receptor subtypes and the (1,3,4,5)ip(4) receptor gap1(ip4bp) in highly purified human platelet membranes. Blood 2000, 95, 3412–3422. [Google Scholar] [CrossRef]
- Jantzen, H.M.; Milstone, D.S.; Gousset, L.; Conley, P.B.; Mortensen, R.M. Impaired activation of murine platelets lacking gα(i2). J. Clin. Investig. 2001, 108, 477–483. [Google Scholar] [CrossRef]
- Katsuyamaa, M.; Sugimotoa, Y.; Nambab, T.; Irie, A.; Negishi, M.; Narumiyab, S.; Ichikawa, A. Cloning and expression of a cdna for the human prostacyclin receptor. FEBS J. 1994, 344, 74–78. [Google Scholar] [CrossRef] [Green Version]
- Stassen, J.M.; Arnout, J.; Deckmyn, H. The hemostatic system. Curr. Med. Chem. 2004, 11, 2245–2260. [Google Scholar] [CrossRef]
- Revel-Vilk, S.; Rand, M.L.; Israels, S.J. Primary and secondary hemostasis, regulators of coagulation, and fibrinolysis: Understanding the basics. In SickKids Handbook of Pediatric Thrombosis and Hemostasis; Karger Publishers: Basel, Switzerland, 2013; pp. 5–13. [Google Scholar]
- Fridman, G.; Friedman, G.; Gutsol, A.; Shekhter, A.B.; Vasilets, V.N.; Fridman, A. Applied plasma medicine. Plasma Process. Polym. 2008, 5, 503–533. [Google Scholar] [CrossRef]
- Ikehara, Y.; Sakakita, H.; Shimizu, N.; Ikehara, S.; Nakanishi, H. Formation of membrane-like structures in clotted blood by mild plasma treatment during hemostasis. J. Photopolym. Sci. Technol. 2013, 26, 555–557. [Google Scholar] [CrossRef] [Green Version]
- Aleinik, A.; Baikov, A.; Dambaev, G.; Semichev, E.; Bushlanov, P. Liver hemostasis by using cold plasma. Surg. Innov. 2017, 24, 253–258. [Google Scholar] [CrossRef] [PubMed]
- Aleinik, A.; Baikov, A.; Shevtsova, N.; Semichev, E.; Bushlanov, P.; Turgunova, N. Application of cold plasma for performing a typical resection of the spleen. Biomed. Phys. Eng. Express 2018, 4, 055026. [Google Scholar] [CrossRef]
- Ikehara, S.; Sakakita, H.; Ishikawa, K.; Akimoto, Y.; Yamaguchi, T.; Yamagishi, M.; Kim, J.; Ueda, M.; Ikeda, J.; Nakanishi, H.; et al. Plasma blood coagulation without involving the activation of platelets and coagulation factors. Plasma Process. Polym. 2015, 12, 1348–1353. [Google Scholar] [CrossRef]
- Dobrynin, D.; Wu, A.; Kalghatgi, S.; Park, S.; Shainsky, N.; Wasko, K.; Dumani, E.; Ownbey, R.; Joshi, S.; Sensenig, R.; et al. Live pig skin tissue and wound toxicity of cold plasma treatment. Plasma Med. 2011, 1, 93–108. [Google Scholar] [CrossRef] [Green Version]
- Fridman, G.; Peddinghaus, M.; Ayan, H.; Fridman, A.; Balasubramanian, M.; Gutsol, A.; Brooks, A.; Friedman, G. Blood coagulation and living tissue sterilization by floating-electrode dielectric barrier discharge in air. Plasma Chem. Plasma Process. 2006, 26, 425–442. [Google Scholar] [CrossRef]
- Bekeschus, S.; Brüggemeier, J.; Hackbarth, C.; Weltmann, K.-D.; von Woedtke, T.; Partecke, L.-I.; van der Linde, J. The feed gas composition determines the degree of physical plasma-induced platelet activation for blood coagulation. Plasma Sources Sci. Technol. 2018, 27, 034001. [Google Scholar] [CrossRef]
- Kalghatgi, S.U.; Fridman, G.; Cooper, M.; Nagaraj, G.; Peddinghaus, M.; Balasubramanian, M.; Vasilets, V.N.; Gutsol, A.F.; Fridman, A.; Friedman, G. Mechanism of blood coagulation by nonthermal atmospheric pressure dielectric barrier discharge plasma. IEEE Trans. Plasma Sci. 2007, 35, 1559–1566. [Google Scholar] [CrossRef]
- Winter, J.; Wende, K.; Masur, K.; Iseni, S.; Dunnbier, M.; Hammer, M.U.; Tresp, H.; Weltmann, K.D.; Reuter, S. Feed gas humidity: A vital parameter affecting a cold atmospheric-pressure plasma jet and plasma-treated human skin cells. J. Phys. D Appl. Phys. 2013, 46, 295401. [Google Scholar] [CrossRef]
- Wende, K.; Williams, P.; Dalluge, J.; Gaens, W.V.; Aboubakr, H.; Bischof, J.; von Woedtke, T.; Goyal, S.M.; Weltmann, K.D.; Bogaerts, A.; et al. Identification of the biologically active liquid chemistry induced by a nonthermal atmospheric pressure plasma jet. Biointerphases 2015, 10, 029518. [Google Scholar] [CrossRef] [Green Version]
- Bekeschus, S.; Schmidt, A.; Niessner, F.; Gerling, T.; Weltmann, K.D.; Wende, K. Basic research in plasma medicine—A throughput approach from liquids to cells. J. Vis. Exp. 2017, e56331. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Salvemini, D.; de Nucci, G.; Sneddon, J.M.; Vane, J.R. Superoxide anions enhance platelet adhesion and aggregation. Br. J. Pharmacol. 1989, 97, 1145–1150. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bocci, V.; Valacchi, G.; Rossi, R.; Giustarini, D.; Paccagnini, E.; Pucci, A.M.; Simplicio, P.D. Studies on the biological effects of ozone: 9. Effects of ozone on human platelets. Platelets 2010, 10, 110–116. [Google Scholar] [CrossRef]
- Iseni, S.; Zhang, S.; van Gessel, A.F.H.; Hofmann, S.; van Ham, B.T.J.; Reuter, S.; Weltmann, K.D.; Bruggeman, P.J. Nitric oxide density distributions in the effluent of an RF argon APPJ: Effect of gas flow rate and substrate. New J. Phys. 2014, 16, 123011. [Google Scholar] [CrossRef] [Green Version]
- Leo, F.; Hutzler, B.; Ruddiman, C.A.; Isakson, B.E.; Cortese-Krott, M.M. Cellular microdomains for nitric oxide signaling in endothelium and red blood cells. Nitric Oxide 2020, 96, 44–53. [Google Scholar] [CrossRef]
- Lackmann, J.W.; Bruno, G.; Jablonowski, H.; Kogelheide, F.; Offerhaus, B.; Held, J.; Schulz-von der Gathen, V.; Stapelmann, K.; von Woedtke, T.; Wende, K. Nitrosylation vs. Oxidation—How to modulate cold physical plasmas for biological applications. PLoS ONE 2019, 14, e0216606. [Google Scholar] [CrossRef] [Green Version]
- Gow, A.J.; Luchsinger, B.P.; Pawloski, J.R.; Singel, D.J.; Stamler, J.S. The oxyhemoglobin reaction of nitric oxide. Proc. Natl. Acad. Sci. USA 1999, 96, 9027–9032. [Google Scholar] [CrossRef] [Green Version]
- Ki, S.H.; Sin, S.; Shin, J.H.; Kwon, Y.W.; Chae, M.W.; Uhm, H.S.; Baik, K.Y.; Choi, E.H. Hemoglobin as a diagnosing molecule for biological effects of atmospheric-pressure plasma. Plasma Chem. Plasma Process. 2018, 38, 937–952. [Google Scholar] [CrossRef]
- Baik, K.Y.; Kim, Y.H.; Hur, E.-H. Selective toxicity on canine blood cells by using atmospheric-pressure plasma jets. J. Korean Phys. Soc. 2012, 60, 965–969. [Google Scholar] [CrossRef]
- Miyamoto, K.; Ikehara, S.; Takei, H.; Akimoto, Y.; Sakakita, H.; Ishikawa, K.; Ueda, M.; Ikeda, J.; Yamagishi, M.; Kim, J.; et al. Red blood cell coagulation induced by low-temperature plasma treatment. Arch. Biochem. Biophys. 2016, 605, 95–101. [Google Scholar] [CrossRef]
- Helms, C.C.; Marvel, M.; Zhao, W.; Stahle, M.; Vest, R.; Kato, G.J.; Lee, J.S.; Christ, G.; Gladwin, M.T.; Hantgan, R.R.; et al. Mechanisms of hemolysis-associated platelet activation. J. Thromb. Haemost. 2013, 11, 2148–2154. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mendonca, R.; Silveira, A.A.; Conran, N. Red cell damps and inflammation. Inflamm. Res. 2016, 65, 665–678. [Google Scholar] [CrossRef] [PubMed]
- Kim, S.; Kunapuli, S.P. P2y12 receptor in platelet activation. Platelets 2011, 22, 56–60. [Google Scholar] [CrossRef] [PubMed]
- Savi, P.; Herbert, J.M. Clopidogrel and ticlopidine: P2y12 adenosine diphosphate-receptor antagonists for the prevention of atherothrombosis. Semin. Thromb. Hemost. 2005, 31, 174–183. [Google Scholar] [CrossRef]
- Sapey, E.; Greenwood, H.; Walton, G.; Mann, E.; Love, A.; Aaronson, N.; Insall, R.H.; Stockley, R.A.; Lord, J.M. Phosphoinositide 3-kinase inhibition restores neutrophil accuracy in the elderly: Toward targeted treatments for immunosenescence. Blood 2014, 123, 239–248. [Google Scholar] [CrossRef] [Green Version]
- Cardenes, N.; Corey, C.; Geary, L.; Jain, S.; Zharikov, S.; Barge, S.; Novelli, E.M.; Shiva, S. Platelet bioenergetic screen in sickle cell patients reveals mitochondrial complex v inhibition, which contributes to platelet activation. Blood 2014, 123, 2864–2872. [Google Scholar] [CrossRef] [Green Version]
- Lorenzo, C.S.; Limm, W.M.; Lurie, F.; Wong, L.L. Factors affecting outcome in liver resection. HPB 2005, 7, 226–230. [Google Scholar] [CrossRef] [Green Version]
- Lane, J.C.; Dworkin-Valenti, J.; Chiodo, L.; Haupert, M. Postoperative tonsillectomy bleeding complications in children: A comparison of three surgical techniques. Int. J. Pediatr. Otorhinolaryngol. 2016, 88, 184–188. [Google Scholar] [CrossRef]
- Bekeschus, S.; Schmidt, A.; Weltmann, K.-D.; von Woedtke, T. The plasma jet kinpen—A powerful tool for wound healing. Clin. Plas. Med. 2016, 4, 19–28. [Google Scholar] [CrossRef]
- Isbary, G.; Morfill, G.; Schmidt, H.U.; Georgi, M.; Ramrath, K.; Heinlin, J.; Karrer, S.; Landthaler, M.; Shimizu, T.; Steffes, B.; et al. A first prospective randomized controlled trial to decrease bacterial load using cold atmospheric argon plasma on chronic wounds in patients. Br. J. Dermatol. 2010, 163, 78–82. [Google Scholar] [CrossRef]
- Metelmann, H.-R.; Vu, T.T.; Do, H.T.; Le, T.N.B.; Hoang, T.H.A.; Phi, T.T.T.; Luong, T.M.L.; Doan, V.T.; Nguyen, T.T.H.; Nguyen, T.H.M.; et al. Scar formation of laser skin lesions after cold atmospheric pressure plasma (cap) treatment: A clinical long term observation. Clin. Plas. Med. 2013, 1, 30–35. [Google Scholar] [CrossRef]
- Schmidt, A.; Woedtke, T.V.; Stenzel, J.; Lindner, T.; Polei, S.; Vollmar, B.; Bekeschus, S. One year follow-up risk assessment in skh-1 mice and wounds treated with an argon plasma jet. Int. J. Mol. Sci. 2017, 18, 868. [Google Scholar] [CrossRef] [PubMed]
- Van der Linde, J.; Liedtke, K.R.; Matthes, R.; Kramer, A.; Heidecke, C.-D.; Partecke, L.I. Repeated cold atmospheric plasma application to intact skin does not cause sensitization in a standardized murine model. Plasma Med. 2017, 7, 383–393. [Google Scholar] [CrossRef]
- Bekeschus, S.; Rödder, K.; Schmidt, A.; Stope, M.B.; von Woedtke, T.; Miller, V.; Fridman, A.; Weltmann, K.-D.; Masur, K.; Metelmann, H.-R.; et al. Cold physical plasma selects for specific t helper cell subsets with distinct cells surface markers in a caspase-dependent and nf-κb-independent manner. Plasma Process. Polym. 2016, 13, 1144–1150. [Google Scholar] [CrossRef]
- Bekeschus, S.; von Woedtke, T.; Kramer, A.; Weltmann, K.-D.; Masur, K. Cold physical plasma treatment alters redox balance in human immune cells. Plasma Med. 2013, 3, 267–278. [Google Scholar] [CrossRef]
- Arndt, S.; Schmidt, A.; Karrer, S.; von Woedtke, T. Comparing two different plasma devices kinpen and adtec steriplas regarding their molecular and cellular effects on wound healing. Clin. Plas. Med. 2018, 9, 24–33. [Google Scholar] [CrossRef]
- Bastin, O.; Thulliez, M.; Servais, J.; Nonclercq, A.; Delchambre, A.; Hadefi, A.; Deviere, J.; Reniers, F. Optical and electrical characteristics of an endoscopic dbd plasma jet. Plasma Med. 2020, 10, 71–90. [Google Scholar] [CrossRef]
- Winter, J.; Nishime, T.M.C.; Glitsch, S.; Luhder, H.; Weltmann, K.D. On the development of a deployable cold plasma endoscope. Contrib. Plasma Phys. 2018, 58, 404–414. [Google Scholar] [CrossRef]
- Zuo, X.; Wei, Y.; Chen, L.W.; Meng, Y.D.; Team, P.M. Non-equilibrium atmospheric pressure microplasma jet: An approach to endoscopic therapies. Phys. Plasmas 2013, 20, 083507. [Google Scholar] [CrossRef]
- Miebach, L.; Freund, E.; Clemen, R.; Weltmann, K.D.; Metelmann, H.R.; von Woedtke, T.; Gerling, T.; Wende, K.; Bekeschus, S. Conductivity augments ros and rns delivery and tumor toxicity of an argon plasma jet. Free Radic. Biol. Med. 2022, 180, 210–219. [Google Scholar] [CrossRef]
- Cheng-Yen, C.; Hsin-Wen, F.; Kuo, S.P.; Jenghwa, C.; Pedersen, T.; Mills, T.J.; Cheng-Chiu, H. Blood clotting by low-temperature air plasma. IEEE Trans. Plasma Sci. 2009, 37, 993–999. [Google Scholar] [CrossRef]
- Jia, B.; Liu, J.; Yin, S.; Liu, Z.; Zheng, S.; Yan, K. Low temperature plasma treatment of rat blood is accompanied by platelet aggregation. Plasma Chem. Plasma Process. 2021, 41, 955–972. [Google Scholar] [CrossRef]
- Nomura, Y.; Takamatsu, T.; Kawano, H.; Miyahara, H.; Okino, A.; Yoshida, M.; Azuma, T. Investigation of blood coagulation effect of nonthermal multigas plasma jet in vitro and in vivo. J. Surg. Res. 2017, 219, 302–309. [Google Scholar] [CrossRef] [PubMed]
- Yan, K.P.; Jin, Q.K.; Zheng, C.; Deng, G.L.; Yin, S.Y.; Liu, Z. Pulsed cold plasma-induced blood coagulation and its pilot application in stanching bleeding during rat hepatectomy. Plasma Sci. Technol. 2018, 20, 044005. [Google Scholar] [CrossRef] [Green Version]
- Shahbazi Rad, Z.; Abbasi Davani, F.; Etaati, G. Determination of proper treatment time for in vivo blood coagulation and wound healing application by non-thermal helium plasma jet. Australas. Phys. Eng. Sci. Med. 2018, 41, 905–917. [Google Scholar] [CrossRef]
Figure 1.
Blood and compartments, including segmentation of the hematocrit across weight-correlated abundancies of erythrocytes, thrombocytes, and leukocytes. Created with biorender.com (accessed on 1 February 2022).
Figure 1.
Blood and compartments, including segmentation of the hematocrit across weight-correlated abundancies of erythrocytes, thrombocytes, and leukocytes. Created with biorender.com (accessed on 1 February 2022).

Figure 2.
Simplified scheme of signaling involved in platelet activation. Created with motifolio.com (accessed on 1 February 2022).
Figure 2.
Simplified scheme of signaling involved in platelet activation. Created with motifolio.com (accessed on 1 February 2022).
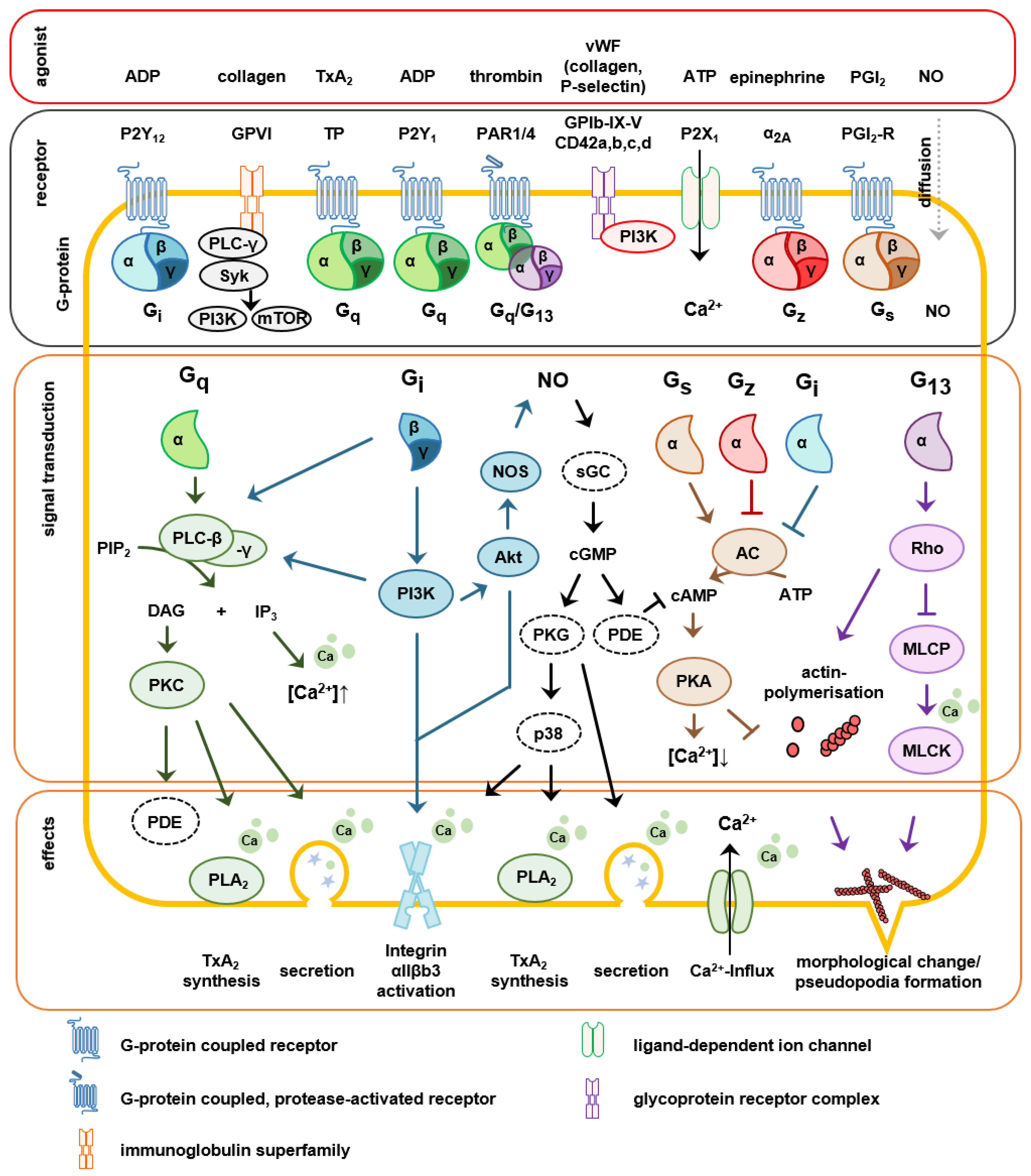
Figure 3.
Simplified scheme of blood coagulation upon vessel injury. Created with biorender.com (accessed on 1 February 2022).
Figure 3.
Simplified scheme of blood coagulation upon vessel injury. Created with biorender.com (accessed on 1 February 2022).
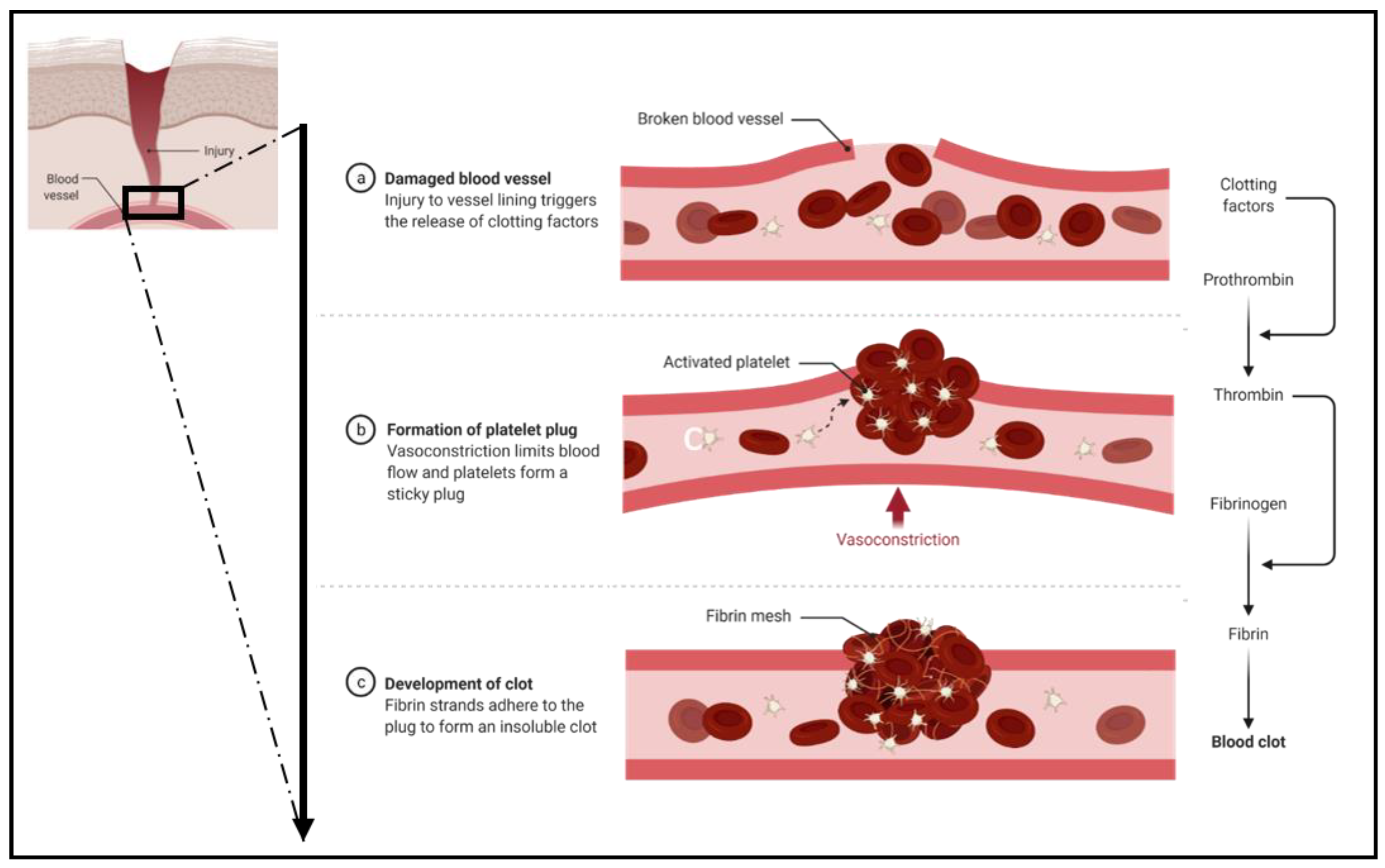
Figure 4.
Putative modes of action of gas plasma during hemostasis. Created with biorender.com (accessed on 1 February 2022).
Figure 4.
Putative modes of action of gas plasma during hemostasis. Created with biorender.com (accessed on 1 February 2022).
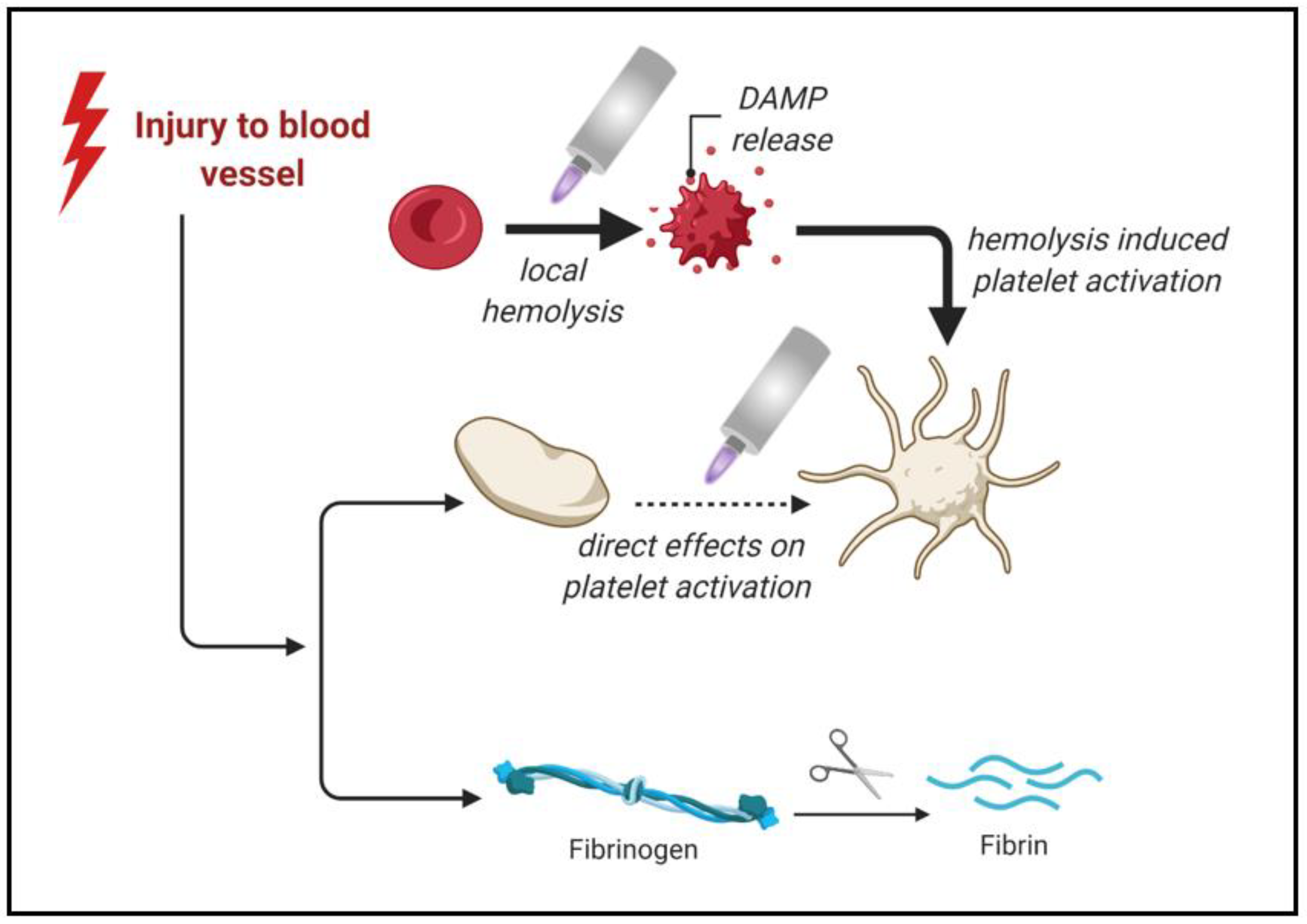
Figure 5.
Potential fields of application of gas plasma-mediated hemostatic activity. Created with biorender.com (accessed on 1 February 2022).
Figure 5.
Potential fields of application of gas plasma-mediated hemostatic activity. Created with biorender.com (accessed on 1 February 2022).
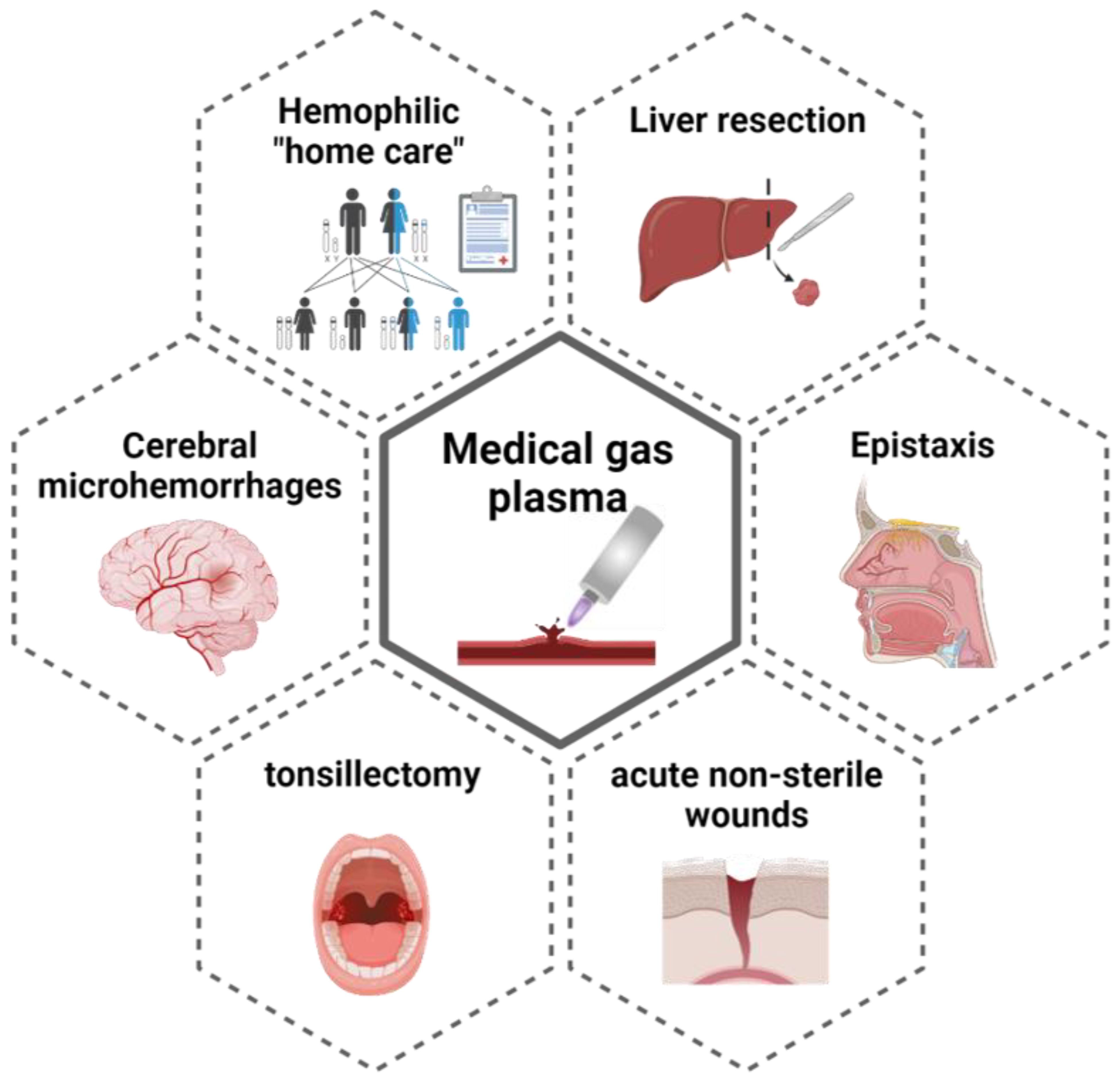
Figure 6.
The approved (medical device class IIa) atmospheric pressure argon plasma jet kINPen MED. Current medical indications are decontamination and promotion of wound healing. (Left) Scheme of a prototype of the kINPen plasma jet with argon gas used as feed gas that is excited in a high-frequency electrode before driven out into the ambient air to generate reactive oxyxgen and nitrogen species. (Middle) kINPen MED equipped with a space. (Right) kINPen MED plasma jet connecting to the skin. Image reproduced from [93].
Figure 6.
The approved (medical device class IIa) atmospheric pressure argon plasma jet kINPen MED. Current medical indications are decontamination and promotion of wound healing. (Left) Scheme of a prototype of the kINPen plasma jet with argon gas used as feed gas that is excited in a high-frequency electrode before driven out into the ambient air to generate reactive oxyxgen and nitrogen species. (Middle) kINPen MED equipped with a space. (Right) kINPen MED plasma jet connecting to the skin. Image reproduced from [93].

Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
MDPI and ACS Style
Miebach, L.; Poschkamp, B.; van der Linde, J.; Bekeschus, S. Medical Gas Plasma—A Potent ROS-Generating Technology for Managing Intraoperative Bleeding Complications. Appl. Sci. 2022, 12, 3800. https://doi.org/10.3390/app12083800
AMA Style
Miebach L, Poschkamp B, van der Linde J, Bekeschus S. Medical Gas Plasma—A Potent ROS-Generating Technology for Managing Intraoperative Bleeding Complications. Applied Sciences. 2022; 12(8):3800. https://doi.org/10.3390/app12083800
Chicago/Turabian StyleMiebach, Lea, Broder Poschkamp, Julia van der Linde, and Sander Bekeschus. 2022. "Medical Gas Plasma—A Potent ROS-Generating Technology for Managing Intraoperative Bleeding Complications" Applied Sciences 12, no. 8: 3800. https://doi.org/10.3390/app12083800
Note that from the first issue of 2016, this journal uses article numbers instead of page numbers. See further details here.