Surface Topography-Based Positioning Accuracy of Maxillary Templates Fabricated by the CAD/CAM Technique for Orthognathic Surgery without an Intermediate Splint


Abstract
:1. Introduction
2. Materials and Methods
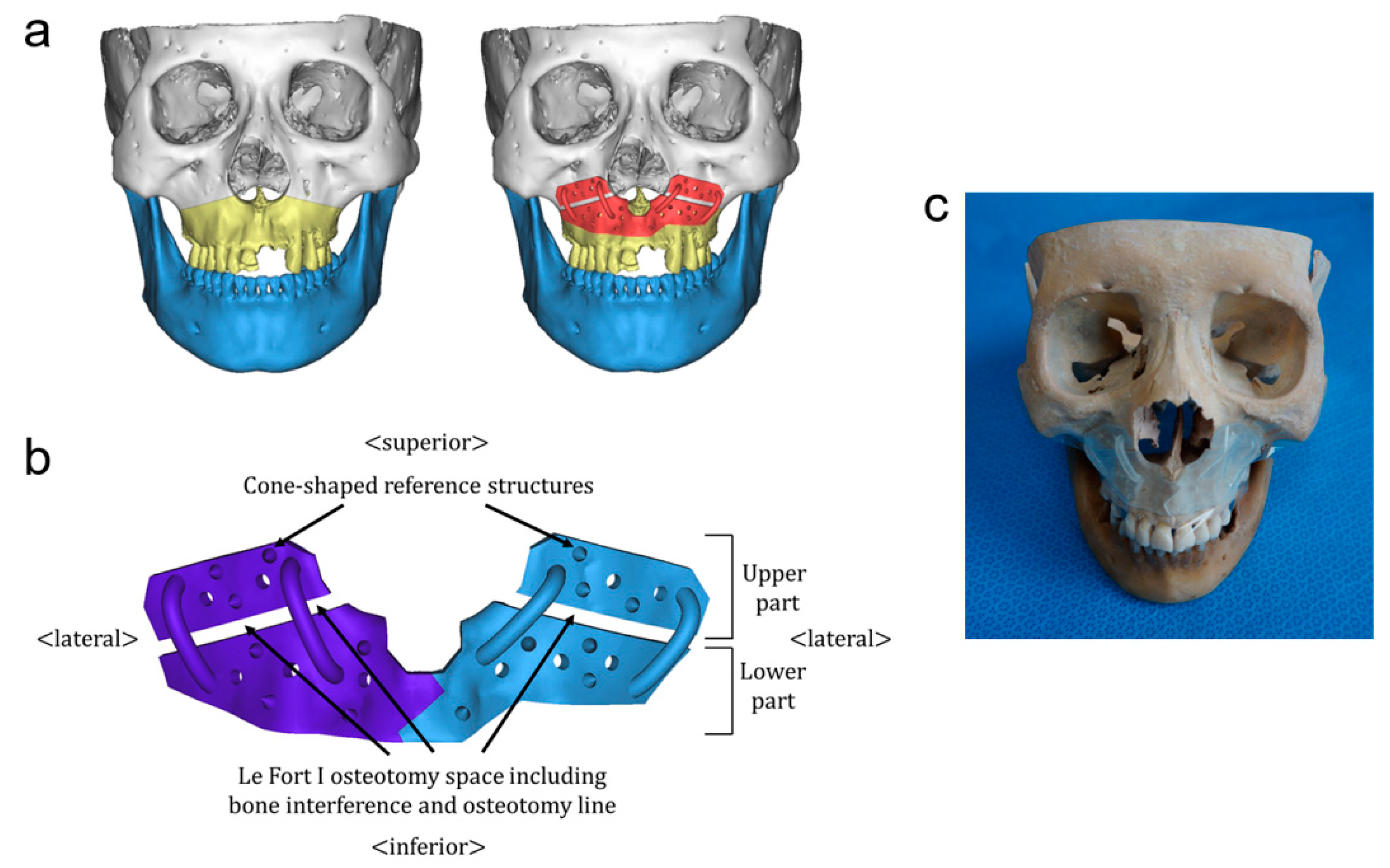
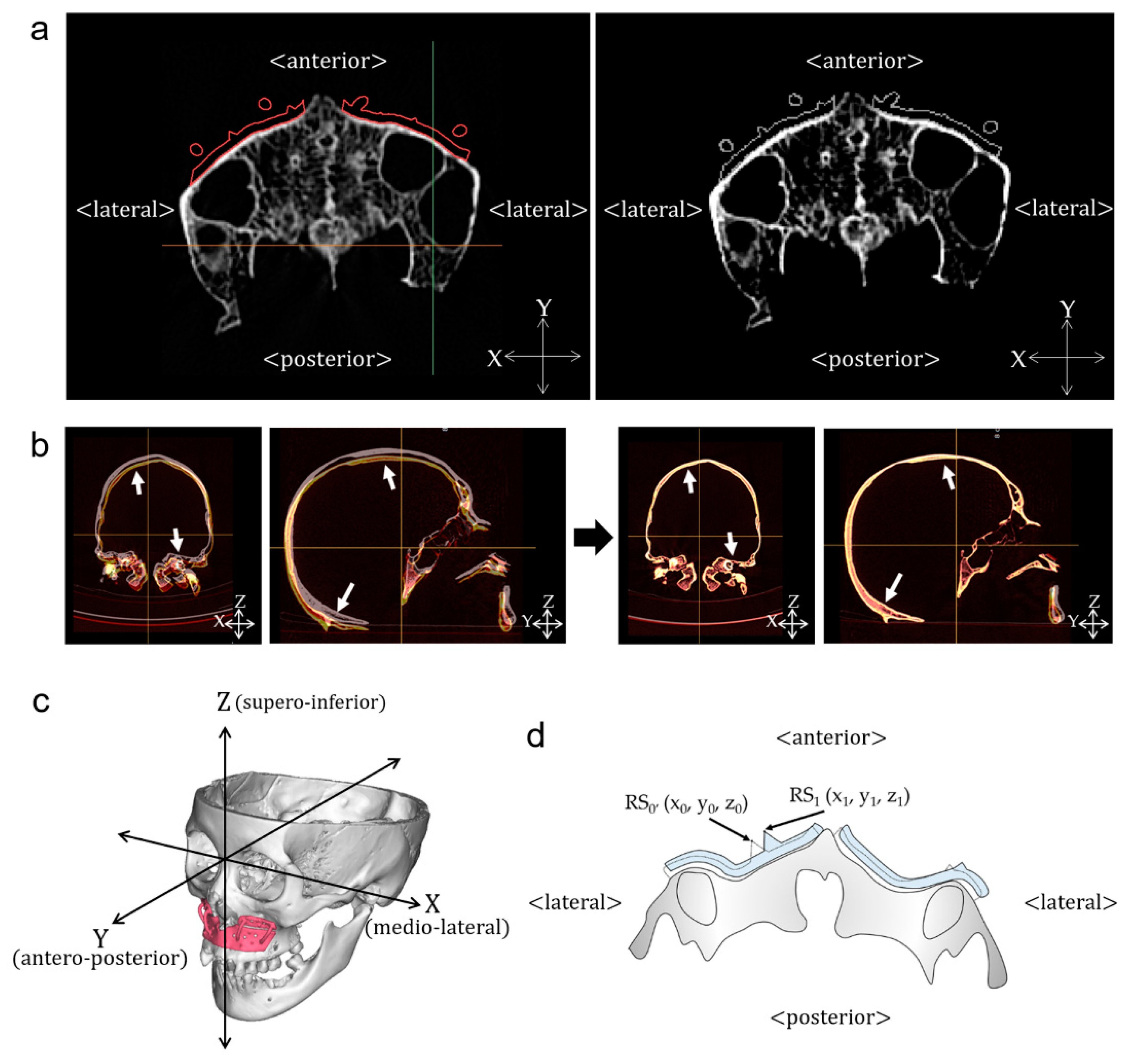
2.1. Design of CAD/CAM-Based Surgical Templates
2.2. Deviation of the CAD/CAM-Based Surgical Templates
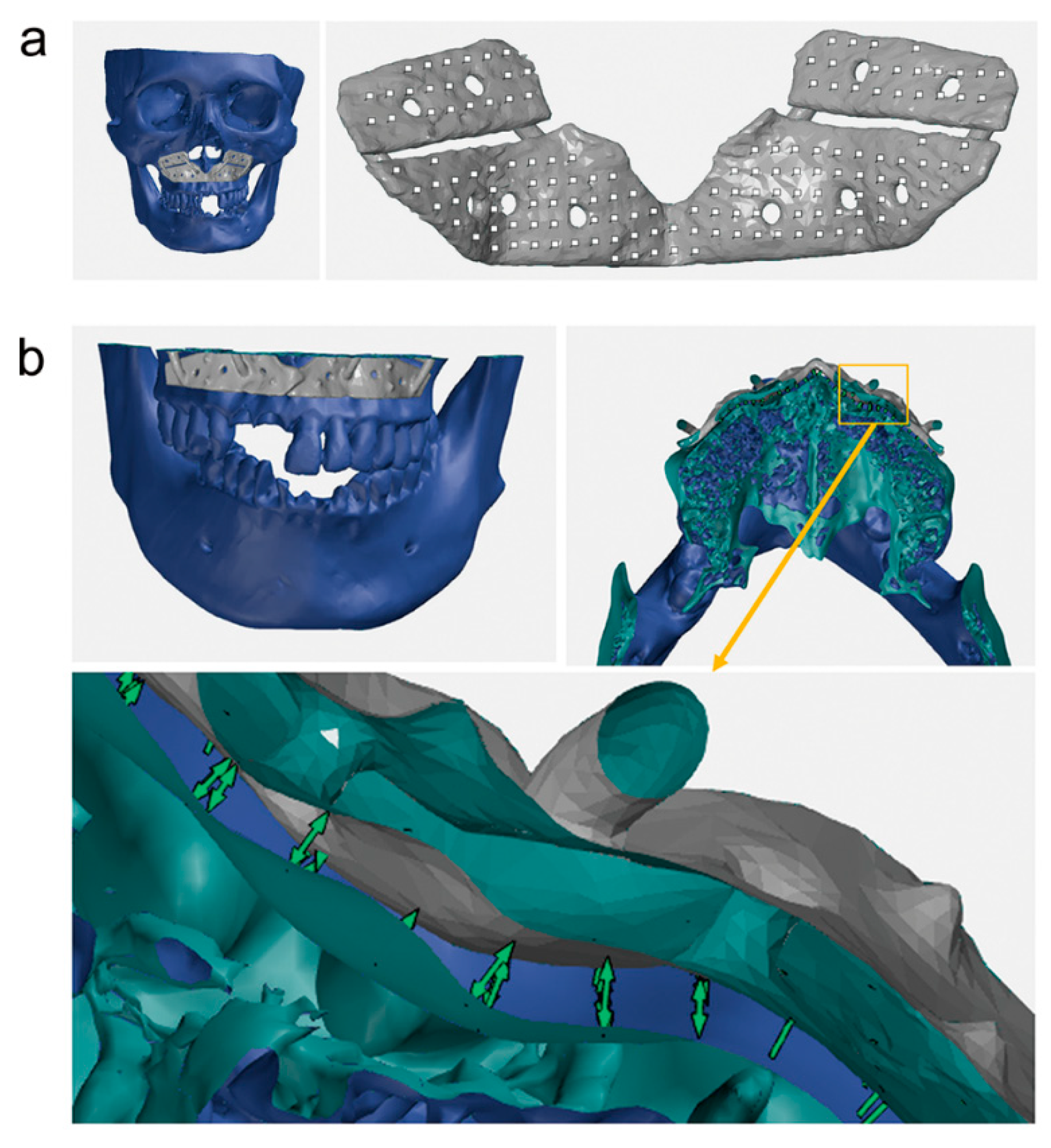
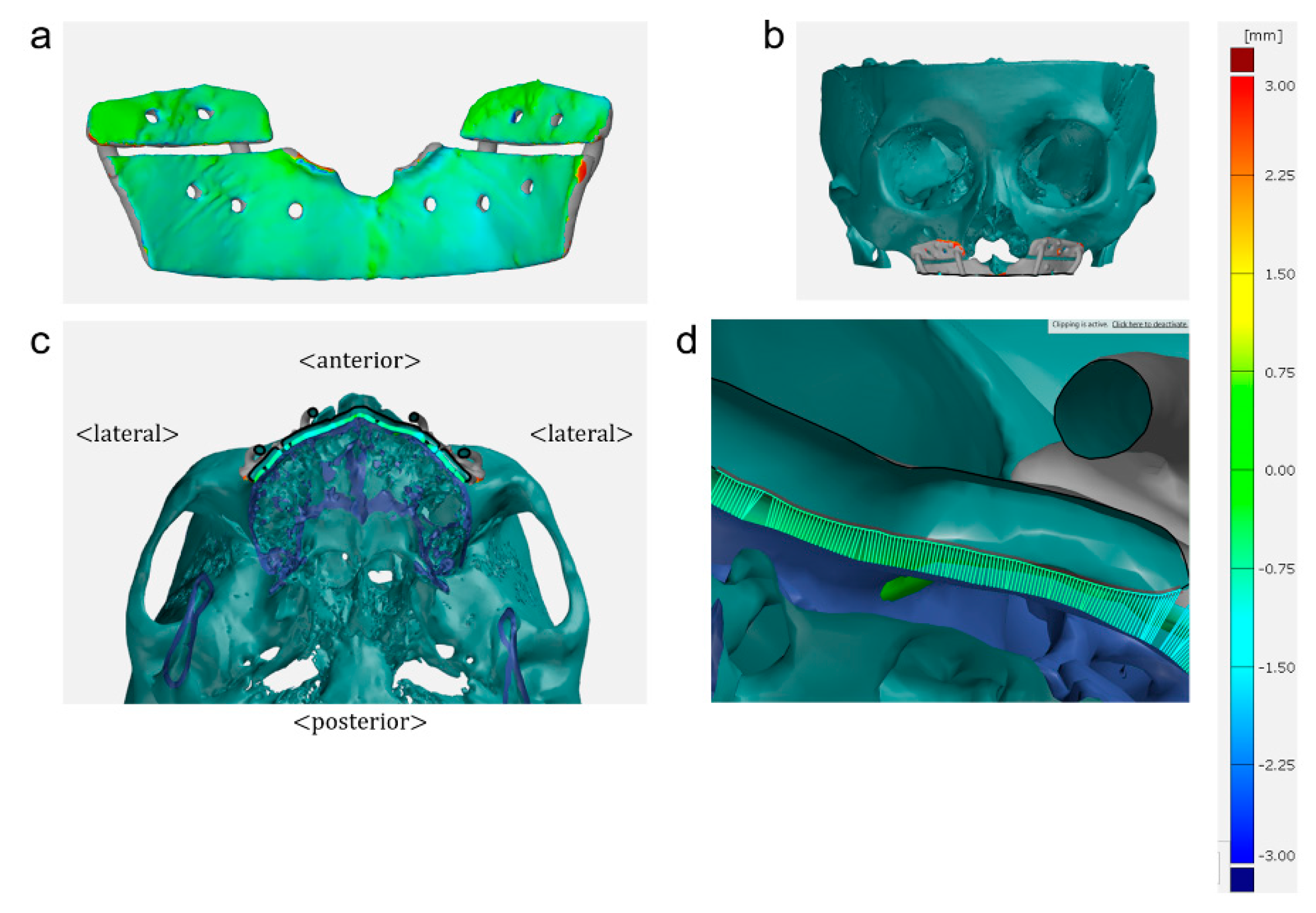
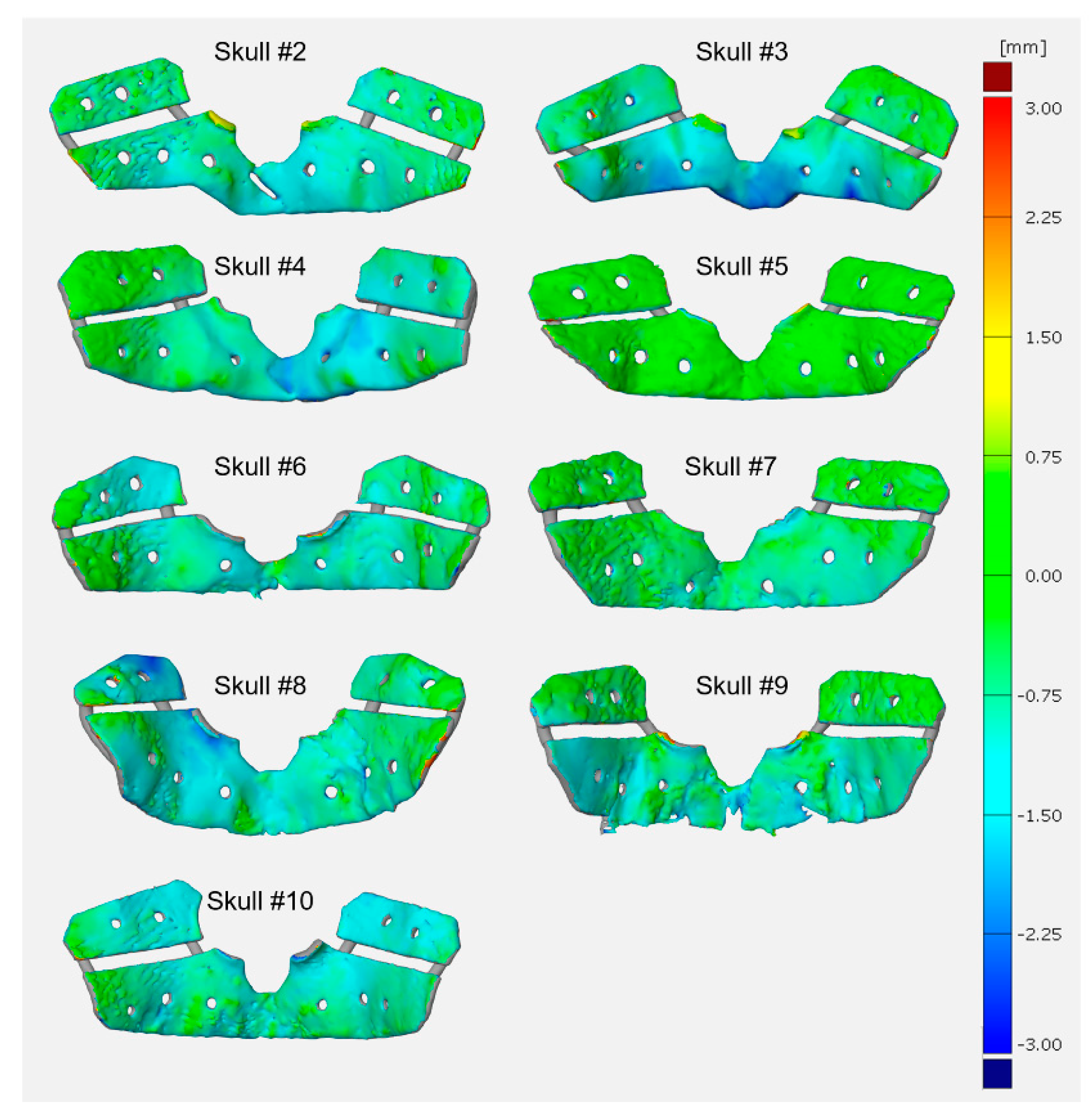
2.3. Fitness of the CAD/CAM-Based Surgical Templates
2.4. Statistical Analysis
3. Results
3.1. Deviation of the CAD/CAM-Based Surgical Templates
3.2. Fitness of the CAD/CAM-Based Surgical Templates
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Han, J.J.; Yang, H.J.; Hwang, S.J. Repositioning of the Maxillomandibular Complex Using Maxillary Template Adjusted Only by Maxillary Surface Configuration Without an Intermediate Splint in Orthognathic Surgery. J. Craniofacial Surg. 2016, 27, 1550–1553. [Google Scholar] [CrossRef] [PubMed]
- Li, B.; Zhang, L.; Sun, H.; Yuan, J.; Shen, S.G.; Wang, X. A novel method of computer aided orthognathic surgery using individual CAD/CAM templates: A combination of osteotomy and repositioning guides. Br. J. Oral Maxillofac. Surg. 2013, 51, e239–e244. [Google Scholar] [CrossRef] [PubMed]
- Suojanen, J.; Leikola, J.; Stoor, P. The use of patient-specific implants in orthognathic surgery: A series of 32 maxillary osteotomy patients. J. Cranio Maxillofac. Surg. 2016, 44, 1913–1916. [Google Scholar] [CrossRef] [PubMed]
- Ellis, E., 3rd. Accuracy of model surgery: Evaluation of an old technique and introduction of a new one. J. Oral Maxillofac. Surg. 1990, 48, 1161–1167. [Google Scholar] [CrossRef]
- Olszewski, R.; Reychler, H. Limitations of orthognathic model surgery: Theoretical and practical implications. Rev. Stomatol. Chir. Maxillofac. 2004, 105, 165–169. [Google Scholar] [CrossRef]
- Bai, S.; Shang, H.; Liu, Y.; Zhao, J.; Zhao, Y. Computer-aided design and computer-aided manufacturing locating guides accompanied with prebent titanium plates in orthognathic surgery. J. Oral Maxillofac. Surg. 2012, 70, 2419–2426. [Google Scholar] [CrossRef]
- Ferguson, J.W.; Luyk, N.H. Control of vertical dimension during maxillary orthognathic surgery. A clinical trial comparing internal and external fixed reference points. J. Cranio Maxillofac. Surg. 1992, 20, 333–336. [Google Scholar] [CrossRef]
- Kahnberg, K.E.; Sunzel, B.; Astrand, P. Planning and control of vertical dimension in Le Fort I osteotomies. J. Cranio Maxillofac. Surg. 1990, 18, 267–270. [Google Scholar] [CrossRef]
- Zinser, M.J.; Sailer, H.F.; Ritter, L.; Braumann, B.; Maegele, M.; Zoller, J.E. A paradigm shift in orthognathic surgery? A comparison of navigation, computer-aided designed/computer-aided manufactured splints, and “classic” intermaxillary splints to surgical transfer of virtual orthognathic planning. J. Oral Maxillofac. Surg. 2013, 71, 2151.e1–2151.e21. [Google Scholar] [CrossRef]
- Sharifi, A.; Jones, R.; Ayoub, A.; Moos, K.; Walker, F.; Khambay, B.; McHugh, S. How accurate is model planning for orthognathic surgery? Int. J. Oral Maxillofac. Surg. 2008, 37, 1089–1093. [Google Scholar] [CrossRef]
- Kwon, T.G.; Mori, Y.; Minami, K.; Lee, S.H. Reproducibility of maxillary positioning in Le Fort I osteotomy: A 3-dimensional evaluation. J. Oral Maxillofac. Surg. 2002, 60, 287–293. [Google Scholar] [CrossRef] [PubMed]
- Mulier, D.; Shaheen, E.; Shujaat, S.; Fieuws, S.; Jacobs, R.; Politis, C. How accurate is digital-assisted Le Fort I maxillary osteotomy? A three-dimensional perspective. Int. J. Oral Maxillofac. Surg. 2019. [Google Scholar] [CrossRef] [PubMed]
- Aboul-Hosn Centenero, S.; Hernandez-Alfaro, F. 3D planning in orthognathic surgery: CAD/CAM surgical splints and prediction of the soft and hard tissues results—Our experience in 16 cases. J. Cranio Maxillofac. Surg. 2012, 40, 162–168. [Google Scholar] [CrossRef] [PubMed]
- Chen, X.; Li, X.; Xu, L.; Sun, Y.; Politis, C.; Egger, J. Development of a computer-aided design software for dental splint in orthognathic surgery. Sci. Rep. 2016, 6, 38867. [Google Scholar] [CrossRef]
- Li, B.; Wei, H.; Zeng, F.; Li, J.; Xia, J.J.; Wang, X. Application of A Novel Three-dimensional Printing Genioplasty Template System and Its Clinical Validation: A Control Study. Sci. Rep. 2017, 7, 5431. [Google Scholar] [CrossRef]
- Kwon, T.G. Accuracy and reliability of three-dimensional computer-assisted planning for orthognathic surgery. Maxillofac. Plast. Reconstr. Surg. 2018, 40, 14. [Google Scholar] [CrossRef]
- Tominaga, K.; Habu, M.; Tsurushima, H.; Takahashi, O.; Yoshioka, I. CAD/CAM splint based on soft tissue 3D simulation for treatment of facial asymmetry. Maxillofac. Plast. Reconstr. Surg. 2016, 38, 4. [Google Scholar] [CrossRef]
- Brunso, J.; Franco, M.; Constantinescu, T.; Barbier, L.; Santamaria, J.A.; Alvarez, J. Custom-Machined Miniplates and Bone-Supported Guides for Orthognathic Surgery: A New Surgical Procedure. J. Oral Maxillofac. Surg. 2016, 74, 1061.e1–1061.e12. [Google Scholar] [CrossRef]
- Gander, T.; Bredell, M.; Eliades, T.; Rucker, M.; Essig, H. Splintless orthognathic surgery: A novel technique using patient-specific implants (PSI). J. Cranio Maxillofac. Surg. 2015, 43, 319–322. [Google Scholar] [CrossRef]
- Mazzoni, S.; Bianchi, A.; Schiariti, G.; Badiali, G.; Marchetti, C. Computer-aided design and computer-aided manufacturing cutting guides and customized titanium plates are useful in upper maxilla waferless repositioning. J. Oral Maxillofac. Surg. 2015, 73, 701–707. [Google Scholar] [CrossRef]
- Polley, J.W.; Figueroa, A.A. Orthognathic positioning system: Intraoperative system to transfer virtual surgical plan to operating field during orthognathic surgery. J. Oral Maxillofac. Surg. 2013, 71, 911–920. [Google Scholar] [CrossRef] [PubMed]
- Lim, S.H.; Kim, M.K.; Kang, S.H. Genioplasty using a simple CAD/CAM (computer-aided design and computer-aided manufacturing) surgical guide. Maxillofac. Plast. Reconstr. Surg. 2015, 37, 44. [Google Scholar] [CrossRef] [PubMed]
- Salvato, G.; Chiavenna, C.; Meazzini, M.C. Guide surgery osteotomy system (GSOS) a new device for treatment in orthognathic surgery. J. Cranio Maxillofac. Surg. 2014, 42, 234–238. [Google Scholar] [CrossRef] [PubMed]
- Suojanen, J.; Leikola, J.; Stoor, P. The use of patient-specific implants in orthognathic surgery: A series of 30 mandible sagittal split osteotomy patients. J. Cranio Maxillofac. Surg. 2017, 45, 990–994. [Google Scholar] [CrossRef] [PubMed]
- Yamauchi, K.; Yamaguchi, Y.; Katoh, H.; Takahashi, T. Tooth-bone CAD/CAM surgical guide for genioplasty. Br. J. Oral Maxillofac. Surg. 2016, 54, 1134–1135. [Google Scholar] [CrossRef]
- Yun, P.Y. The application of three-dimensional printing techniques in the fi eld of oral and maxillofacial surgery. J. Korean Assoc. Oral Maxillofac. Surg. 2015, 41, 169–170. [Google Scholar] [CrossRef]
- Heufelder, M.; Wilde, F.; Pietzka, S.; Mascha, F.; Winter, K.; Schramm, A.; Rana, M. Clinical accuracy of waferless maxillary positioning using customized surgical guides and patient specific osteosynthesis in bimaxillary orthognathic surgery. J. Cranio Maxillofac. Surg. 2017, 45, 1578–1585. [Google Scholar] [CrossRef]
- Chang, H.W.; Lin, H.H.; Chortrakarnkij, P.; Kim, S.G.; Lo, L.J. Intraoperative navigation for single-splint two-jaw orthognathic surgery: From model to actual surgery. J. Cranio Maxillofac. Surg. 2015, 43, 1119–1126. [Google Scholar] [CrossRef]
- Lin, H.H.; Chang, H.W.; Lo, L.J. Development of customized positioning guides using computer-aided design and manufacturing technology for orthognathic surgery. Int. J. Comput. Assist. Radiol. Surg. 2015, 10, 2021–2033. [Google Scholar] [CrossRef]
- Bai, S.; Bo, B.; Bi, Y.; Wang, B.; Zhao, J.; Liu, Y.; Feng, Z.; Shang, H.; Zhao, Y. CAD/CAM surface templates as an alternative to the intermediate wafer in orthognathic surgery. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endod. 2010, 110, e1–e7. [Google Scholar] [CrossRef]
- Han, J.J.; Hwang, S.J. Three-dimensional analysis of postoperative returning movement of perioperative condylar displacement after bilateral sagittal split ramus osteotomy for mandibular setback with different fixation methods. J. Cranio Maxillofac. Surg. 2015, 43, 1918–1925. [Google Scholar] [CrossRef] [PubMed]
- Ghang, M.H.; Kim, H.M.; You, J.Y.; Kim, B.H.; Choi, J.P.; Kim, S.H.; Choung, P.H. Three-dimensional mandibular change after sagittal split ramus osteotomy with a semirigid sliding plate system for fixation of a mandibular setback surgery. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. 2013, 115, 157–166. [Google Scholar] [CrossRef] [PubMed]
- Szymor, P.; Kozakiewicz, M.; Olszewski, R. Accuracy of open-source software segmentation and paper-based printed three-dimensional models. J. Cranio Maxillofac. Surg. 2016, 44, 202–209. [Google Scholar] [CrossRef] [PubMed]
- Kwon, T.G.; Choi, J.W.; Kyung, H.M.; Park, H.S. Accuracy of maxillary repositioning in two-jaw surgery with conventional articulator model surgery versus virtual model surgery. Int. J. Oral Maxillofac. Surg. 2014, 43, 732–738. [Google Scholar] [CrossRef] [PubMed]
- Li, K.Y.; Luo, W.J.; Huang, J.Z.; Chan, Y.C.; Pratikto; Faridah, D. Operational Temperature Effect on Positioning Accuracy of a Single-Axial Moving Carrier. Appl. Sci. 2017, 7, 420. [Google Scholar] [CrossRef] [Green Version]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Skull No. | Medio-Lateral | Antero-Posterior | Supero-Inferior | |||
|---|---|---|---|---|---|---|
| Mean ± SD (Range) | p-Value * | Mean ± SD (Range) | p-Value * | Mean ± SD (Range) | p-Value * | |
| 1 | 0.26 ± 0.20 | 0.055 | 0.26 ± 0.23 | 0.005 * | 0.69 ± 0.33 | 0.001 * |
| (0.03–0.71) | (0.02–0.78) | (0.01–1.16) | ||||
| 2 | 0.35 ± 0.26 | 0.708 | 0.27 ± 0.13 | 0.115 | 0.38 ± 0.22 | 0.195 |
| (0.02–0.85) | (0.03–0.50) | (0.02–0.79) | ||||
| 3 | 0.53 ± 0.21 | 0.754 | 1.22 ± 0.41 | 0.001 * | 0.82 ± 0.31 | 0.001 * |
| (0.13–0.93) | (0.62–1.72) | (0.14–1.28) | ||||
| 4 | 0.34 ± 0.17 | 0.002 * | 0.96 ± 0.71 | 0.001 * | 1.57 ± 0.83 | 0.001 * |
| (0.08–0.71) | (0.01–2.13) | (0.46–2.83) | ||||
| 5 | 0.50 ± 0.17 | 0.001 * | 0.23 ± 0.15 | 0.016 * | 0.21 ± 0.14 | 0.138 |
| (0.15–0.78) | (0.02–0.51) | (0.02–0.41) | ||||
| 6 | 0.51 ± 0.29 | 0.067 | 0.41 ± 0.22 | 0.043 * | 0.45 ± 0.30 | 0.001 * |
| (0.01–1.08) | (0.13–0.89) | (0.06–0.96) | ||||
| 7 | 0.36 ± 0.21 | 0.003 * | 0.23 ± 0.18 | 0.076 | 0.58 ± 0.41 | 0.012 * |
| (0.09–0.74) | (0.00–0.54) | (0.02–1.25) | ||||
| 8 | 0.53 ± 0.41 | 0.001 * | 0.93 ± 0.95 | 0.004 * | 0.86 ± 0.66 | 0.001 * |
| (0.00–1.36) | (0.10–2.64) | (0.17–2.41) | ||||
| 9 | 0.35 ± 0.52 | 0.287 | 0.42 ± 0.66 | 0.592 | 0.85 ± 0.67 | 0.002 * |
| (0.04–2.05) | (0.05–2.72) | (0.05–2.75) | ||||
| 10 | 0.34 ± 0.16 | 0.178 | 0.54 ± 0.33 | 0.029 * | 0.50 ± 0.25 | 0.001 * |
| (0.10–0.58) | (0.04–1.09) | (0.11–0.98) | ||||
| For all skulls | 0.41 ± 0.30 | 0.001 * | 0.55 ± 0.59 | 0.001* | 0.69 ± 0.59 | 0.001 * |
| Skull No. | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 | Mean ± SD |
|---|---|---|---|---|---|---|---|---|---|---|---|
| RMSD | 0.90 | 0.68 | 1.66 | 2.18 | 0.65 | 0.92 | 0.87 | 1.84 | 1.48 | 0.93 | 1.21 ± 0.54 |
| Contact area | 1287.33 | 1246.00 | 1323.66 | 1223.51 | 1141.05 | 1129.16 | 1318.19 | 1402.49 | 1489.61 | 1765.33 | 1332.63 ± 187.56 |
| Skull No. | Number of the Created Surface Points on the Inner Surface of the Template | Distance between the Surface Point Created on the Inner Surface of the Template and Its Projected Point on the Underlying Bone (mm) | |
|---|---|---|---|
| Mean ± SD | Maximum | ||
| 1 | 188 | 0.73 ± 0.22 | 1.11 |
| 2 | 179 | 0.86 ± 0.27 | 1.57 |
| 3 | 184 | 1.01 ± 0.53 | 2.38 |
| 4 | 178 | 0.82 ± 0.45 | 1.83 |
| 5 | 146 | 0.17 ± 0.10 | 0.52 |
| 6 | 149 | 0.79 ± 0.30 | 1.33 |
| 7 | 201 | 0.51 ± 0.28 | 1.18 |
| 8 | 163 | 0.94 ± 0.40 | 2.26 |
| 9 | 188 | 0.74 ± 0.35 | 1.74 |
| 10 | 272 | 0.89 ± 0.27 | 1.65 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Han, J.J.; Hwang, S.J. Surface Topography-Based Positioning Accuracy of Maxillary Templates Fabricated by the CAD/CAM Technique for Orthognathic Surgery without an Intermediate Splint. Appl. Sci. 2019, 9, 4928. https://doi.org/10.3390/app9224928
Han JJ, Hwang SJ. Surface Topography-Based Positioning Accuracy of Maxillary Templates Fabricated by the CAD/CAM Technique for Orthognathic Surgery without an Intermediate Splint. Applied Sciences. 2019; 9(22):4928. https://doi.org/10.3390/app9224928
Chicago/Turabian StyleHan, Jeong Joon, and Soon Jung Hwang. 2019. "Surface Topography-Based Positioning Accuracy of Maxillary Templates Fabricated by the CAD/CAM Technique for Orthognathic Surgery without an Intermediate Splint" Applied Sciences 9, no. 22: 4928. https://doi.org/10.3390/app9224928