Early Screening of the Autism Spectrum Disorders: Validity Properties and Cross-Cultural Generalizability of the First Year Inventory in Italy

 , ,
, ,
Abstract
:1. Introduction
The First Year Inventory: Measure Description and Critical Analysis of the Validation Studies
2. Materials and Methods
2.1. Procedure
2.2. Measure
2.3. Participants
2.4. Analytic Strategy
3. Results
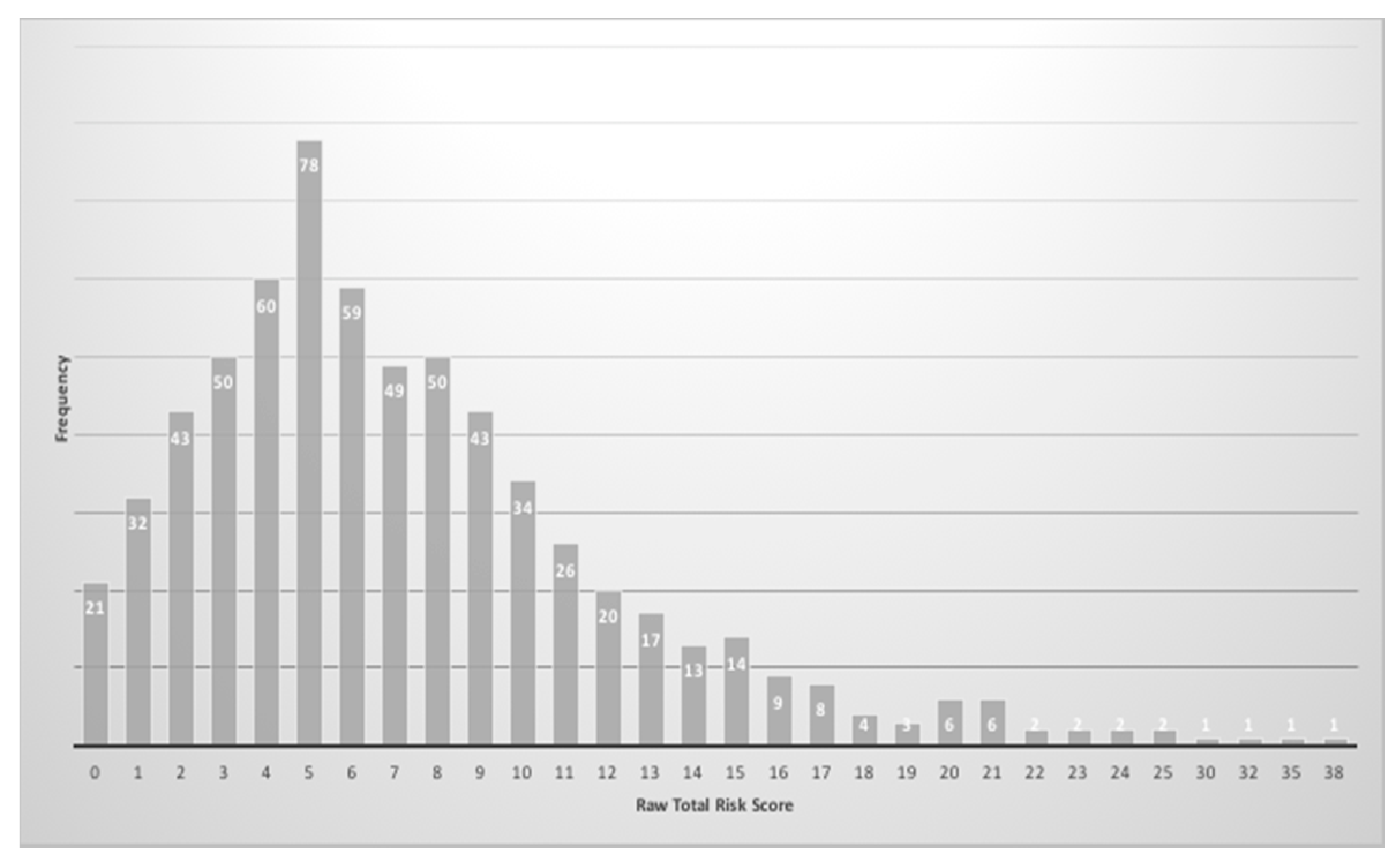
3.1. Preliminary Analysis
3.2. Generalisability
3.3. Construct Validity
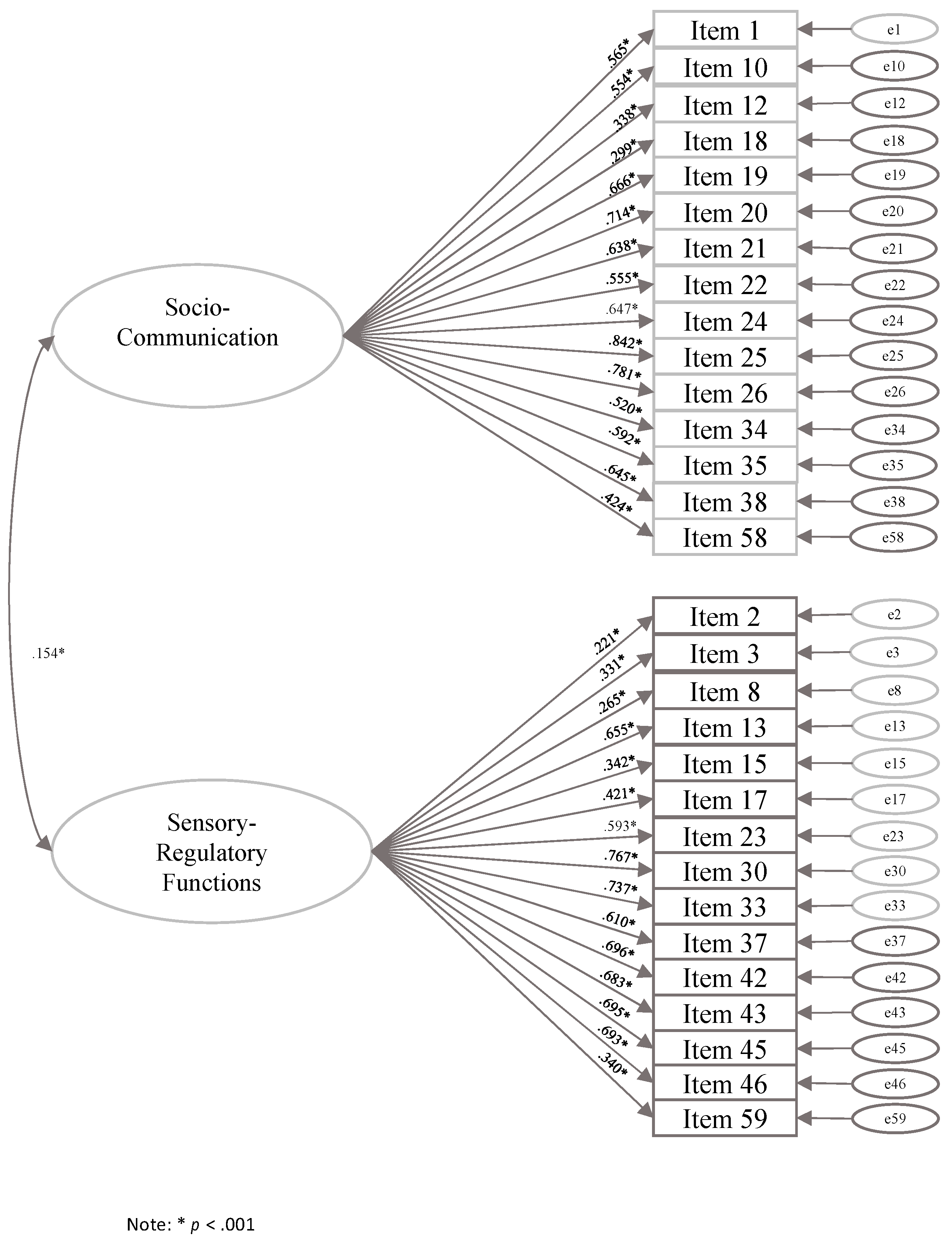
3.4. Internal Consistency and Factorial Analyses
4. Discussion
5. Limitation
6. Conclusions and Implication
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders (DSM-5); Raffaello Cortina: Milan, Italy, 2014. [Google Scholar]
- Christensen, D.L.; Maenner, M.J.; Bilder, D.; Constantino, J.N.; Daniels, J.; Durkin, M.S.; Fitzgerald, R.T.; Kurzius-Spencer, M.; Pettygrove, S.D.; Robinson, C.; et al. Prevalence and Characteristics of Autism Spectrum Disorder Among Children Aged 4 Years—Early Autism and Developmental Disabilities Monitoring Network, Seven Sites, United States, 2010, 2012, and 2014. MMWR Surveill. Summ. 2019, 68, 1–19. [Google Scholar] [CrossRef] [Green Version]
- American Academy Pediatric Report. Available online: https://www.aap.org/en-us/about-the-aap/Councils/Council-on-Children-with-Disabilities/Pages/COCWD.aspx (accessed on 17 February 2020).
- Allison, C.; Baron-Cohen, S.; Wheelwright, S.; Charman, T.; Richler, J.; Pasco, G.; Brayne, C. The Q-CHAT (Quantitative CHecklist for Autism in Toddlers): A normally distributed quantitative measure of autistic traits at 18–24 months of age: Preliminary report. JADD 2008, 38, 1414–1425. [Google Scholar] [CrossRef]
- Baron-Cohen, S.; Allen, J.; Gillberg, C. Can autism be detected at 18 months? The needle, the haystack, and the CHAT. Br. J. Psych. 1992, 161, 839–843. [Google Scholar] [CrossRef] [PubMed]
- Robins, D.L.; Fein, D.; Barton, M.L.; Green, J.A. The Modified Checklist for Autism in Toddlers: An initial study investigating the early detection of autism and pervasive developmental disorders. JADD 2001, 31, 131–144. [Google Scholar] [CrossRef] [PubMed]
- Dietz, C.; Swinkels, S.; van Daalen, E.; van Engeland, H.; Buitelaar, J.K. Screening for Autistic Spectrum Disorder in Children Aged 14–15 Months. II: Population Screening with the Early Screening of Autistic Traits Questionnaire (ESAT). Design and General Findings. JADD 2006, 36, 713–722. [Google Scholar] [CrossRef] [PubMed]
- Reznick, J.S.; Baranek, G.T.; Reavis, S.; Watson, L.R.; Crais, E.R. A parent-report instrument for identifying one-year-olds at risk for an eventual diagnosis of autism: The first year inventory. JADD 2007, 37, 1691–1710. [Google Scholar] [CrossRef] [PubMed]
- Levante, A.; Petrocchi, S.; Lecciso, F. Systematic review protocol of measures for early detection of risk for Autism Spectrum Disorders in toddlers. Lifesp. Disabil. 2019, 22, 55–75. [Google Scholar]
- Robins, D.L.; Casagrande, K.; Barton, M.; Chen, C.M.A.; Dumont-Mathieu, T.; Fein, D. Validation of the modified checklist for autism in toddlers, revised with follow-up (M-CHAT-R/F). Pediatrics 2014, 133, 37–45. [Google Scholar] [CrossRef] [Green Version]
- Feldman, M.A.; Ward, R.A.; Savona, D.; Regehr, K.; Parker, K.; Hudson, M.; Holden, J.A. Development and Initial Validation of Parent Report Measure of the Behavioral development of infants at risk for Autism Spectrum Disorders. JADD 2012, 42, 13–22. [Google Scholar] [CrossRef]
- Albores-Gallo, L.; Roldán-Ceballos, O.; Villarreal-Valdes, G.; Betanzos-Cruz, B.X.; Santos-Sánchez, C.; Martínez-Jaime, M.M.; Hilton, C.L. M-CHAT Mexican version validity and reliability and some cultural considerations. ISRN Neur. 2012, 408694. [Google Scholar] [CrossRef] [Green Version]
- Baduel, S.; Guillon, Q.; Afzali, M.H.; Foudon, N.; Kruck, J.; Rogé, B. The French version of the modified-checklist for autism in toddlers (M-CHAT): A validation study on a French sample of 24 months old children. JADD 2017, 47, 297–304. [Google Scholar] [CrossRef] [PubMed]
- Brennan, L.; Fein, D.; Como, A.; Rathwell, I.C.; Chen, C.M. Use of the Modified Checklist for Autism, Revised with Follow Up-Albanian to Screen for ASD in Albania. JADD 2016, 46, 3392–3407. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Canal-Bedia, R.; García-Primo, P.; Martín-Cilleros, M.V.; Santos-Borbujo, J.; Guisuraga-Fernández, Z.; Herráez-García, L.; Posada-de La Paz, M. Modified checklist for autism in toddlers: Cross-cultural adaptation and validation in Spain. JADD 2011, 41, 1342–1351. [Google Scholar] [CrossRef] [PubMed]
- Carakovac, M.; Jovanovic, J.; Kalanj, M.; Rudic, N.; Aleksic–Hil, O.; Aleksic, B.; Pejovic–Milovancevic, M. Serbian language version of the modified checklist for autism in toddlers, revised, with follow-up: Cross-cultural adaptation and assessment of reliability. Sci. Rep. 2016, 6, 38222. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chlebowski, C.; Robins, D.L.; Barton, M.L.; Fein, D. Large-scale use of the modified checklist for autism in low-risk toddlers. Pediatrics 2013, 131, e1121–e1127. [Google Scholar] [CrossRef] [Green Version]
- Cuesta-Gómez, J.L.; Andrea Manzone, L.; Posada-De-La-Paz, M. Modified checklist for autism in toddler cross-cultural adaptation for Argentina. Int. J. Dev. Dis. 2016, 62, 117–123. [Google Scholar] [CrossRef]
- Guo, C.; Luo, M.; Wang, X.; Huang, S.; Meng, Z.; Shao, J.; Jing, J. Reliability and Validity of the Chinese Version of Modified Checklist for Autism in Toddlers, Revised, with Follow-Up (M-CHAT-R/F). JADD 2019, 49, 185–196. [Google Scholar] [CrossRef]
- Inada, N.; Koyama, T.; Inokuchi, E.; Kuroda, M.; Kamio, Y. Reliability and validity of the Japanese version of the Modified Checklist for autism in toddlers (M-CHAT). Res. Aut. Spec. Dis. 2011, 5, 330–336. [Google Scholar] [CrossRef]
- Kleinman, J.M.; Robins, D.L.; Ventola, P.E.; Pandey, J.; Boorstein, H.C.; Esser, E.L.; Barton, M. The modified checklist for autism in toddlers: A follow-up study investigating the early detection of autism spectrum disorders. JADD 2008, 38, 827–839. [Google Scholar] [CrossRef] [Green Version]
- Scarpa, A.; Reyes, N.M.; Patriquin, M.A.; Lorenzi, J.; Hassenfeldt, T.A.; Desai, V.J.; Kerkering, K.W. The modified checklist for autism in toddlers: Reliability in a diverse rural American sample. JADD 2013, 43, 2269–2279. [Google Scholar] [CrossRef]
- Seif Eldin, A.; Habib, D.; Noufal, A.; Farrag, S.; Bazaid, K.; Al-Sharbati, M.; Gaddour, N. Use of M-CHAT for a multinational screening of young children with autism in the Arab countries. Int. Rev. Psych. 2008, 20, 281–289. [Google Scholar] [CrossRef] [PubMed]
- Seung, H.; Ji, J.; Kim, S.J.; Sung, I.; Youn, Y.A.; Hong, G.; Youm, H.K. Examination of the Korean modified checklist of autism in toddlers: Item response theory. JADD 2015, 45, 2744–2757. [Google Scholar] [CrossRef] [PubMed]
- Snow, A.V.; Lecavalier, L. Sensitivity and specificity of the Modified Checklist for Autism in Toddlers and the Social Communication Questionnaire in preschoolers suspected of having pervasive developmental disorders. Autism 2008, 12, 627–644. [Google Scholar] [CrossRef] [PubMed]
- Stenberg, N.; Bresnahan, M.; Gunnes, N.; Hirtz, D.; Hornig, M.; Lie, K.K.; Schjølberg, S. Identifying children with autism spectrum disorder at 18 months in a general population sample. Ped. Per. Epid. 2014, 28, 255–262. [Google Scholar] [CrossRef] [Green Version]
- Ruta, L.; Arduino, G.M.; Gagliano, A.; Apicella, F.; Leonardi, E.; Fama, F.I.; Chericoni, N.; Costanzo, V.; Turco, N.; Tartarisco, G.; et al. Psychometric properties, factor structure and cross-cultural validity of the quantitative checklist for autism in toddlers (q-chat) in an Italian community setting. Res. Aut. Spec. Dis. 2019, 64, 39–48. [Google Scholar] [CrossRef]
- Ruta, L.; Chiarotti, F.; Arduino, G.M.; Apicella, F.; Leonardi, E.; Maggio, R.; Tartarisco, G. Validation of the Quantitative CHecklist for Autism in Toddlers (Q-CHAT) in an Italian clinical sample of young children with Autism and Other Developmental Disorders. Front. Psych. 2019, 10, 488. [Google Scholar] [CrossRef] [Green Version]
- Sallows, G.O.; Graupner, T.D. Intensive behavioral treatment for children with autism: Four-year outcome and predictors. Am. J. Ment. Retard. 2005, 110, 417–438. [Google Scholar] [CrossRef]
- Lecciso, F.; Levante, A.; Signore, F.; Petrocchi, S. Preliminary evidence of the Structural Validity and measurement invariance of the Quantitative-CHecklist for Autism in Toddler (Q-CHAT) on Italian unselected children. EJASA 2019, 12, 320–340. [Google Scholar] [CrossRef]
- Magiati, I.; Goh, D.A.; Lim, S.J.; Gan, D.Z.Q.; Leong, J.C.L.; Allison, C.; Chong, Y.S. The psychometric properties of the Quantitative-Checklist for Autism in Toddlers (Q-CHAT) as a measure of autistic traits in a community sample of Singaporean infants and toddlers. Mol. Aut. 2015, 6, 40. [Google Scholar] [CrossRef] [Green Version]
- Ben-Sasson, A.; Carter, A.S. The application of the first year inventory for ASD screening in Israel. JADD 2012, 42, 1906–1916. [Google Scholar] [CrossRef]
- Muratori, F.; Narzisi, A.; Calderoni, S.; Fulceri, F.; Apicella, F.; Tancredi, R. Identificazione dei bambini con autismo ad un anno di età: Uno studio con la forma retrospettiva del First Year Inventory (FYI). Aut. Dis. Svil. 2009, 7, 339–356. [Google Scholar]
- Turner-Brown, L.M.; Baranek, G.T.; Reznick, J.S.; Watson, L.R.; Crais, E.R. The First Year Inventory: A longitudinal follow-up of 12-month-old to 3-year-old children. Autism 2013, 17, 527–540. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Watson, L.R.; Baranek, G.T.; Crais, E.R.; Reznick, J.S.; Dykstra, J.; Perryman, T. The first year inventory: Retrospective parent responses to a questionnaire designed to identify one-year-olds at risk for autism. JADD 2007, 37, 49–61. [Google Scholar] [CrossRef] [PubMed]
- Bryson, S.E.; Zwaigenbaum, L.; McDermott, C.; Rombough, V.; Brian, J. The Autism Observation Scale for Infants: Scale development and reliability data. JADD 2008, 38, 731–738. [Google Scholar] [CrossRef] [PubMed]
- Mullen, E.M. Mullen Scales of Early Learning; American Guidance Service: Circle Pines, MN, USA, 1995. [Google Scholar]
- Davidovitch, M.; Stein, N.; Koren, G.; Friedman, B.C. Deviations from Typical Developmental Trajectories Detectable at 9 Months of Age in Low Risk Children Later Diagnosed with Autism Spectrum Disorder. JADD 2018, 48, 2854–2869. [Google Scholar] [CrossRef]
- Bridgett, D.J.; Burt, N.M.; Edwards, E.S.; Deater-Deckard, K. Intergenerational transmission of self-regulation: A multidisciplinary review and integrative conceptual framework. Psych. Bul. 2015, 141, 602. [Google Scholar] [CrossRef]
- Tirosh, E.; Bettesh-Bendrian, S.; Golan, G.; Tamir, A.; Cohen-Dar, M. Regulatory disorders in Israeli infants: Epidemiologic perspective. J. Child Neur. 2003, 18, 748–754. [Google Scholar] [CrossRef]
- Fabio, R.A.; Oliva, P.; Murdaca, A.M. Systematic and emotional contents in overselectivity processes in autism. Res. Aut. Dis. 2011, 5, 575–583. [Google Scholar]
- Neuman, A.; Greenberg, D.F.; Labovitz, D.R.; Suzuki, L.A. Cross-cultural adaptation of the sensory profile: Establishing linguistic equivalency of the hebrew version. Occ. Ther. Inter. 2004, 11, 112–130. [Google Scholar] [CrossRef]
- Petrocchi, S.; Rotenberg, K.J.; Levante, A.; Lecciso, F. Children’s trust in social workers: Scale development and relations to children’s engagement with social workers. Child Fam. Soc. Work 2018, 23, 239–247. [Google Scholar] [CrossRef]
- Petrocchi, S.; Iannello, P.; Lecciso, F.; Levante, A.; Antonietti, A.; Schulz, P. Interpersonal trust in doctor-patient relation: Evidence from dyadic analysis and association with quality of dyadic communication. Soc. Sci. Med. 2019, 235, 112391. [Google Scholar] [CrossRef] [PubMed]
- Anderson, D.K.; Liang, J.W.; Lord, C. Predicting young adult outcome among more and less cognitively able individuals with autism spectrum disorders. J. Child Psych. Psych. 2014, 55, 485–494. [Google Scholar] [CrossRef] [PubMed]
- Lecciso, F.; Petrocchi, S.; Savazzi, F.; Marchetti, A.; Nobile, M.; Molteni, M. The association between maternal resolution of the diagnosis of autism, maternal mental representations of the relationship with the child, and children’s attachment. Lifesp. Disabil. 2013, 16, 21–38. [Google Scholar]
- Dawson, G.; Rogers, S.; Munson, J.; Smith, M.; Winter, J.; Greenson, J.; Donaldson, A.; Varley, J. Randomized, controlled trial of an intervention for toddlers with autism: The Early Start Denver Model. Pediatrics 2010, 125, e17–e23. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Robins, D.L.; Dumont-Mathieu, T.M. Early screening for autism spectrum disorders: Update on the modified checklist for autism in toddlers and other measures. J. Dev. Behav. Ped. 2006, 27, S111–S119. [Google Scholar] [CrossRef] [PubMed] [Green Version]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Males M(ds) | Females M(ds) | t | Cohen’s d | |
|---|---|---|---|---|
| Social–Communication domain | 2.83 (3.08) | 2.64 (3.03) | t(648) = 0.766 | - |
| Social orienting & receptive communication | 1.13 (2.69) | 1.26 (2.84) | t(648) = −0.582 | - |
| Social-affective engagement | 2.02 (3.70) | 2.23 (4.01) | t(648) = −0.691 | - |
| Imitation | 1.44 (3.79) | 1.29 (4.25) | t(648) = 0.467 | - |
| Expressive communication | 6.71 (7.79) | 5.79 (7.17) | t(648) = 1.567 | - |
| Sensory–Regulatory Functions domain | 4.07 (4.01) | 3.49 (3.65) | t(648) = 1.921 | - |
| Sensory processing | 3.71 (5.14) | 3.72 (5.32) | t(648) = −0.029 | - |
| Regulatory patterns | 4.54 (9.35) | 3.72 (7.8) | t(643.626) = 1.224 | - |
| Reactivity | 2.08 (5.32) | 1.26 (4.42) | t(643.169) = 2.145 * | 0.17 |
| Repetitive behaviors | 5.94 (7.02) | 5.25 (6.41) | t(648) = 1.303 | - |
| Total score | 3.44 (2.68) | 3.06 (2.52) | t(648) = 1.867 | - |
| Low Educational Level M(ds) | High Educational Level M(ds) | t | Cohen’s d | |
|---|---|---|---|---|
| Social–Communication domain | 3.45 (3.76) | 2.54 (2.80) | t(197.576) = 2.736 * | 0.27 |
| Social orienting & receptive communication | 1.04 (2.54) | 1.22 (2.82) | t(630) = −0.695 * | 0.07 |
| Social–affective engagement | 2.98 (4.80) | 1.82 (3.46) | t(194.269) = 2.719 * | 0.27 |
| Imitation | 1.90 (5.23) | 1.26 (3.60) | t(189.821) = 1.378 | - |
| Expressive communication | 7.90 (8.37) | 5.84 (7.19) | t(215.355) = 2.692 * | 0.26 |
| Sensory–Regulatory Functions domain | 4.65 (4.15) | 3.59 (3.81) | t(630) = 2.895 * | 0.06 |
| Sensory processing | 4.90 (6.18) | 3.45 (4.93) | t(205.617) = 2.594 * | 0.26 |
| Regulatory patterns | 4.03 (7.93) | 4.37 (9.20) | t(630) = −0.406 | - |
| Reactivity | 2.52 (5.59) | 1.44 (4.59) | t(208.993) = 2.121 * | 0.21 |
| Repetitive behaviors | 7.16 (7.51) | 5.10 (6.33) | t(212.843) = 3.028 * | 0.30 |
| Total score | 4.05 (3.03) | 3.06 (2.45) | t(207.011) = 3.615 * | 0.36 |
| Never | Seldom | Sometimes | Often | |||||
|---|---|---|---|---|---|---|---|---|
| ItS | AS | ItS | AS | ItS | AS | ItS | AS | |
| 1. Does your baby turn to look at you when you call your baby’s name? | 0 | <1 | 0.3 | 1 | 2.3 | 8 | 97.4 | 91 |
| 2. Does your baby seem bothered by loud sounds? | 21.2 | 8 | 25.3 | 39 | 41.6 | 46 | 11.7 | 7 |
| 3. Does your baby seem overly sensitive to your touch (for example, fuss or pull away when you touch him or her)? | 71.2 | 64 | 19.4 | 31 | 6.2 | 5 | 2.4 | <1 |
| 4. During familiar games like ‘‘I’m gonna get you,’’ does your baby get excited because he or she knows what will happen next? | 1.4 | <1 | 0.6 | <1 | 7 | 8 | 90.7 | 92 |
| 5. Does your baby seem to have trouble hearing? | 97 | 94 | 1.2 | 5 | 0.2 | 1 | 0.5 | <1 |
| 6. When you and your baby are facing each other, does your baby turn his or her eyes to avoid looking at you? | 81.7 | 53 | 11.9 | 30 | 4.7 | 15 | 1.1 | 2 |
| 7. In new or strange situations, does your baby look at your face for comfort? | 3.3 | 1 | 7.2 | 6 | 28.6 | 40 | 60.4 | 53 |
| 8. Does your baby ignore loud or startling sounds? | 65.3 | 34 | 20.5 | 42 | 10.7 | 21 | 2 | 3 |
| 9. Does your baby spit out certain textures of foods, such as lumpy or chunky pieces? | 25.3 | 11 | 18.4 | 25 | 35.3 | 48 | 19.6 | 16 |
| 10. When you point to something interesting, does your baby turn to look at it? | 0.5 | 1 | 1.4 | 4 | 13.2 | 39 | 83.9 | 56 |
| 11. Is your baby content to play alone for an hour or more at a time? | 35.6 | 27 | 28.2 | 29 | 22.2 | 31 | 13.1 | 13 |
| 12. Does your baby look at people when they begin talking, even when they are not talking directly to your baby? | 0.3 | <1 | 1.4 | 3 | 15.2 | 44 | 83 | 53 |
| 13. Does your baby rock his or her body back and forth over and over? | 61 | 54 | 14.8 | 24 | 16.7 | 15 | 7 | 7 |
| 14. Does your baby look up from playing with a favorite toy if you show him or her a different toy? | 1.7 | <1 | 3.8 | 2 | 31.1 | 39 | 62.7 | 59 |
| 15. Does your baby get upset when you need to switch your baby from one activity to another one? | 34.1 | 7 | 28.5 | 35 | 30 | 53 | 7 | 5 |
| 16. Is it easy to understand your baby’s facial expressions? | 0.8 | <1 | 0.9 | 1 | 6.1 | 14 | 90.7 | 85 |
| 17. Does your baby forcefully press his or her face, head, or body against people or furniture? | 79.6 | 38 | 10 | 27 | 7.6 | 24 | 2.1 | 11 |
| 18. Does your baby smile while looking at you? | 0.2 | <1 | 0.2 | <1 | 5.2 | 9 | 94.2 | 91 |
| 19. Does your baby try to get your attention to show you something interesting? | 1.4 | 7 | 3.5 | 16 | 26.6 | 40 | 67.9 | 37 |
| 20. Does your baby try to get your attention to play games like peek-a-boo? | 3.8 | 5 | 5 | 15 | 25 | 41 | 65.4 | 39 |
| 21. Does your baby try to get your attention to obtain a favorite toy or food? | 1.4 | 2 | 2.3 | 9 | 14.6 | 32 | 81.1 | 57 |
| 22. Does your baby try to get your attention to play physical games, like swinging, tickling, or being tossed in the air? | 4.6 | 10 | 9.1 | 23 | 33.9 | 40 | 51.9 | 26 |
| 23. When your baby is awake and you pick him or her up, does your baby’s body feel loose or floppy? | 87.4 | 81 | 7 | 14 | 3.3 | 4 | 1.4 | 1 |
| 24. Does your baby copy or imitate you when you make sounds or noises with your mouth? | 0.9 | 1 | 2.6 | 4 | 22.7 | 32 | 73.5 | 63 |
| 25. Does your baby copy or imitate your actions, like sticking out your tongue, clapping your hands, or shaking your head? | 0.9 | <1 | 1.5 | 2 | 9.9 | 23 | 87.5 | 75 |
| 26. Does your baby copy or imitate you when you do something with a toy or object, like shaking a rattle or banging a spoon on the table? | 0.8 | <1 | 1.1 | 1 | 9.7 | 22 | 88.3 | 77 |
| 27. Is it difficult to calm your baby once he or she becomes upset? | 33.9 | 20 | 41.7 | 62 | 19.9 | 17 | 4.1 | 1 |
| 28. Are your baby’s sleeping and waking patterns regular from day to day? | 1.7 | 1 | 6.1 | 4 | 11.8 | 20 | 80.2 | 75 |
| 29. Does your baby try to get your attention by making sounds and looking at you at the same time? | 3.7 | 1 | 6.4 | 4 | 26.5 | 30 | 62.7 | 65 |
| 30. Does your baby get stuck doing a simple activity over and over? | 79.3 | 36 | 14.6 | 45 | 4 | 16 | 1.1 | 3 |
| 31. Does your baby seem interested in other babies his or her age? | 0.5 | <1 | 0.8 | 5 | 9.5 | 28 | 89 | 67 |
| 32. Does your baby babble by putting sounds together, such as ‘ba-ba’, ‘ga-ga-ga’, or ‘ba-dee’? | 8.1 | <1 | 3.2 | 1 | 11.7 | 8 | 76.6 | 91 |
| 33. Does your baby enjoy staring at a bright light for long periods of time? | 62.56 | 49 | 22.1 | 32 | 11.7 | 15 | 2.9 | 4 |
| 34. Does your baby use gestures such as raising arms to be picked up, shaking head, or waving bye-bye? | 0.2 | <1 | 0.3 | 3 | 3.7 | 12 | 95.9 | 85 |
| 35. When you say ‘‘Where’s (a familiar person or object)?’’ without pointing or showing, will your baby look at the person or object named? | 0.6 | 4 | 2 | 10 | 13.7 | 35 | 83.3 | 51 |
| 36. Does your baby use the first finger and tip of the thumb to pick up a very small object like a raisin or a Cheerio? | 1.4 | <1 | 1.9 | 1 | 5.9 | 5 | 90.4 | 94 |
| 37. Does your baby seem to get stuck on playing with a part of a toy (such as an eyeball, label, wheel or tag), instead of the whole toy? | 16.1 | 14 | 18.1 | 32 | 34.1 | 39 | 31.4 | 15 |
| 38. Does your baby communicate with you by using his or her finger to point at objects or pictures? | 5.6 | 12 | 5.8 | 18 | 19.2 | 24 | 69.4 | 46 |
| 39. Do you get the feeling that your baby plays or communicates with you less now than in the past? | 87.8 | 80 | 4.4 | 14 | 1.7 | 5 | 5.3 | 1 |
| 40. Do your baby’s eyes line up together when looking at an object? | 5.8 | 1 | 1.5 | 1 | 4.3 | 3 | 85.8 | 95 |
| 41. Are your baby’s feeding patterns regular from day to day? | 1.2 | 1 | 1.1 | 2 | 7.3 | 19 | 90 | 78 |
| 42. Does your baby enjoy rubbing or scratching toys or objects for long periods of time? | 40.6 | 49 | 21 | 34 | 22.8 | 13 | 14.9 | 4 |
| 43. Does your baby seem to get his or her body stuck in a position or posture that is hard to move out of? | 77.9 | 70 | 13.7 | 23 | 6.2 | 6 | 1.2 | 1 |
| 44. Does your baby enjoy making objects spin over and over in the same way? | 43.2 | 32 | 21.4 | 33 | 26.3 | 27 | 8.7 | 8 |
| 45. While lying down, does your baby enjoy kicking his or her feet over and over for long periods of time? | 32.1 | 42 | 18.1 | 33 | 30.1 | 19 | 19.2 | 6 |
| 46. Does your baby stare at his or her fingers while wiggling them in front of his or her eyes? | 47.8 | 32 | 17.4 | 35 | 24.4 | 27 | 10 | 6 |
| 47. Which of the following best describes your baby’s typical play with a favorite toy? | 10.4 | 12 | 30.6 | 55 | 58.3 | 33 | ||
| 48. Which of the following describes your baby’s interest in toys on a typical day? | 4.7 | 3 | 23.4 | 27 | 71.2 | 70 | ||
| 49. When you introduce your baby to a new game (peek-a-boo, so-big, patty-cake, etc.) how does your baby respond? | 86.6 | 29 | 11.9 | 63 | 0.9 | 6 | 0.2 | 2 |
| 50. What do you typically have to do to get your baby to look up from playing with a favorite toy? | 68.2 | 43 | 25.4 | 54 | 5.9 | 3 | ||
| 51. What is your baby’s usual reaction to somewhat painful experiences, like bumping his or her head? | 2.7 | 4 | 89.2 | 93 | 7.5 | 3 | ||
| 52. What do you typically have to do to get your baby to turn towards you? | 88.9 | 71 | 9.3 | 25 | 1.5 | 4 | ||
| 53. What do you typically have to do to get your baby to smile or laugh at you? | 92.1 | 92 | 6.5 | 8 | 0.9 | <1 | ||
| 54. On a typical night, how many hours does your baby sleep? | 4.9 | 13 | 36.7 | 71 | 46.9 | 14 | 11.1 | 2 |
| 55. On a typical night, how many times does your baby wake up? | 27.5 | 51 | 55.1 | 43 | 16.7 | 6 | ||
| 56. Which of the following best describes your baby’s skill level? | 19.8 | 48 | 44.9 | 44 | 29.5 | 6 | 5.2 | 2 |
| 57. Which of the following best describes your baby’s typical day? | 76.3 | 28 | 21.2 | 59 | 1.7 | 11 | 0.2 | 2 |
| 58. If you start a game by copying or imitating a sound your baby makes, what does your baby typically do? | 0.6 | <1 | 7 | 11 | 26.9 | 35 | 64.4 | 54 |
| 59. When your baby is awake and not eating, does your baby keep a toy or object in his or her mouth? | 22.1 | 29 | 37.4 | 50 | 30.6 | 17 | 9.4 | 4 |
| 60. Which of the following best describes the way your baby coordinates his or her eyes and hands while playing with a toy? | 89.8 | 81 | 7.3 | 19 | 1.5 | <1 | 0.9 | <1 |
| Never | Seldom | Sometimes | Often | |||||
|---|---|---|---|---|---|---|---|---|
| ItS | ISS | ItS | ISS | ItS | ISS | ItS | ISS | |
| 3. Does your baby seem overly sensitive to your touch (for example, fuss or pull away when you touch him or her)? | 71.2 | 83 | 19.4 | 14 | 6.2 | 2.1 | 2.4 | 1.3 |
| 6. When you and your baby are facing each other, does your baby turn his or her eyes to avoid looking at you? | 81.7 | 70 | 11.9 | 21 | 4.7 | 7 | 1.1 | 1 |
| 9. Does your baby spit out certain textures of foods, such as lumpy or chunky pieces? | 25.3 | 26 | 18.4 | 38 | 35.3 | 30 | 19.6 | 7 |
| 13. Does your baby rock his or her body back and forth over and over? | 61 | 39 | 14.8 | 25 | 16.7 | 31 | 7 | 10 |
| 17. Does your baby forcefully press his or her face, head, or body against people or furniture? | 79.6 | 59 | 10 | 23 | 7.6 | 15 | 2.1 | 3 |
| 23. When your baby is awake and you pick him or her up, does your baby’s body feel loose or floppy? | 87.4 | 26 | 7 | 16 | 3.3 | 28 | 1.4 | 30 |
| 30. Does your baby get stuck doing a simple activity over and over? | 79.3 | 25 | 14.6 | 40 | 4 | 31 | 1.1 | 4 |
| 35. When you say “Where’s (a familiar person or object)?” without pointing or showing, will your baby look at the person or object named? | 0.6 | 11 | 2 | 14 | 13.7 | 39 | 83.3 | 36 |
| 37. Does your baby seem to get stuck on playing with a part of a toy (such as an eyeball, label, wheel or tag), instead of the whole toy? | 16.1 | 9 | 18.1 | 20 | 34.1 | 37 | 31.4 | 34 |
| 43. Does your baby seem to get his or her body stuck in a position or posture that is hard to move out of? | 77.9 | 53 | 13.7 | 38 | 6.2 | 8 | 1.2 | 2 |
| 48. Which of the following describes your baby’s interest in toys on a typical day? | 4.7 | 5 | 23.4 | 41 | 71.2 | 55 | ||
| 55. On a typical night, how many times does your baby wake up? | 27.5 | 20 | 55.1 | 61 | 16.7 | 19 | ||
| 56. Which of the following best describes your baby’s skill level? | 19.8 | 14 | 44.9 | 54 | 29.5 | 26 | 5.2 | 6 |
| 58. If you start a game by copying or imitating a sound your baby makes, what does your baby typically do? | 0.6 | 0.4 | 7 | 19 | 26.9 | 51 | 64.4 | 30 |
| Reznick et al., (2007) n = 1300 | Ben-Sasson and Carter, (2012) n = 471 | Italian Sample n = 657 | |
|---|---|---|---|
| Range | 0–50 (theoretical range) | 0–33.88 | 0–20.32 |
| Modal score | 0 | 0 | |
| Median score | 5.75 | 9.13 | 2.74 |
| Mean score | - | 10.40 (sd = 6.38) | 3.29 (sd = 2.74) |
| Total risk score (≥95th percentile) | 17.75 * | 22.55 | 17 |
| Total risk mean score (≥95th percentile) | - | - | 8.15 |
| Social–Communication domain score (95th percentile) | - | 27.85 | 7 |
| Sensory–Regulatory Functions domain (95th percentile) | - | 26.95 | 10 |
| Total risk score (98th percentile) | 22.62 ** | 28.14 | 21 |
| Children at risk on 95th percentile | - | 4.88% | 4.87% |
| FYI Construct | Social–Communication Domain | Sensory–Regulatory Functions Domain | |||||
|---|---|---|---|---|---|---|---|
| 1 | 2 | 3 | 4 | 5 | 6 | 7 | |
| Social Orienting a Receptive Communication | 0.16 *** (0.42 **) | 0.32 *** (0.38 **) | 0.12 *** (0.42 **) | 0.07 (0.19 **) | 0.08 * (0.10 **) | 0.10 * (0.13 **) | 0.13 ** (0.12 **) |
| Social-Affective Engagement (1) | 0.28 *** (0.33 **) | 0.30 *** (0.49 **) | −0.01 (0.03) | 0.04 (0.04) | 0.08 * (−0.01) | 0.11 ** (0.04) | |
| Imitation (2) | 0.20 *** (0.35 **) | 0.07 (0.12 **) | 0.09 * (0.03) | 0.13 *** (0.10 **) | 0.09 * (0.02) | ||
| Expressive Communication (3) | −0.05 (0.07) | 0.05 (0.03) | 0.06 (0.03) | −0.01 (0.04) | |||
| Sensory Processing (4) | 0.14 *** (0.18 **) | 0.13 ** (0.30 **) | 0.34 *** (0.38 **) | ||||
| Regulatory Pattern (5) | 0.08 * (0.15 **) | 0.06 (0.11 **) | |||||
| Reactivity (6) | 0.14 *** (0.10 **) | ||||||
| Repetitive Behavior (7) | |||||||
| 1 | 2 | |
|---|---|---|
| FYI_1 | 0.544 (0.091) | −0.196 |
| FYI_10 | 0.550 (0.051) | −0.092 |
| FYI_12 | 0.345 (0.055) | −0.025 |
| FYI_18 | 0.304 (0.082) | −0.045 |
| FYI_19 | 0.655 (0.039) | −0.159 |
| FYI_20 | 0.708 (0.036) | −0.131 |
| FYI_21 | 0.625 (0.047) | −0.168 |
| FYI_22 | 0.570 (0.038) | −0.005 |
| FYI_24 | 0.653 (0.037) | −0.046 |
| FYI_25 | 0.851 (0.031) | −0.003 |
| FYI_26 | 0.787 (0.034) | −0.004 |
| FYI_34 | 0.522 (0.080) | −0.047 |
| FYI_35 | 0.578 (0.049) | −0.160 |
| FYI_38 | 0.642 (0.036) | −0.114 |
| FYI_58 | 0.425 (0.047) | −0.040 |
| FYI_2 | 0.017 | 0.239 (0.044) |
| FYI_3 | −0.037 | 0.335 (0.051) |
| FYI_8 | −0.061 | 0.258 (0.048) |
| FYI_9 | 0.054 | 0.198 (0.046) |
| FYI_13 | −0.106 | 0.651 (0.035) |
| FYI_15 | −0.087 | 0.337 (0.041) |
| FYI_17 | 0.003 | 0.434 (0.052) |
| FYI_23 | −0.149 | 0.583 (0.059) |
| FYI_30 | −0.049 | 0.774 (0.036) |
| FYI_33 | −0.158 | 0.729 (0.029) |
| FYI_37 | −0.112 | 0.607 (0.032) |
| FYI_42 | −0.048 | 0.701 (0.027) |
| FYI_43 | −0.080 | 0.682 (0.039) |
| FYI_45 | −0.072 | 0.695 (0.028) |
| FYI_46 | −0.075 | 0.693 (0.028) |
| FYI_59 | −0.034 | 0.343 (0.040) |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Levante, A.; Petrocchi, S.; Massagli, A.; Filograna, M.R.; De Giorgi, S.; Lecciso, F. Early Screening of the Autism Spectrum Disorders: Validity Properties and Cross-Cultural Generalizability of the First Year Inventory in Italy. Brain Sci. 2020, 10, 108. https://doi.org/10.3390/brainsci10020108
Levante A, Petrocchi S, Massagli A, Filograna MR, De Giorgi S, Lecciso F. Early Screening of the Autism Spectrum Disorders: Validity Properties and Cross-Cultural Generalizability of the First Year Inventory in Italy. Brain Sciences. 2020; 10(2):108. https://doi.org/10.3390/brainsci10020108
Chicago/Turabian StyleLevante, Annalisa, Serena Petrocchi, Angelo Massagli, Maria Rosaria Filograna, Serafino De Giorgi, and Flavia Lecciso. 2020. "Early Screening of the Autism Spectrum Disorders: Validity Properties and Cross-Cultural Generalizability of the First Year Inventory in Italy" Brain Sciences 10, no. 2: 108. https://doi.org/10.3390/brainsci10020108