


A Study of Differential Resting-State Brain Functional Activity in Males and Females with Recurrent Depressive Disorder
Abstract
:1. Introduction
2. Methods
2.1. Subjects
2.2. Scan Acquisition
2.3. Image Processing
2.3.1. fMRI Data Preprocessing
2.3.2. ReHo Analysis
2.4. Statistical Analyses
2.4.1. Clinical Data Analysis
2.4.2. fMRI Data Analysis
3. Results
3.1. Characteristics of the Research Samples
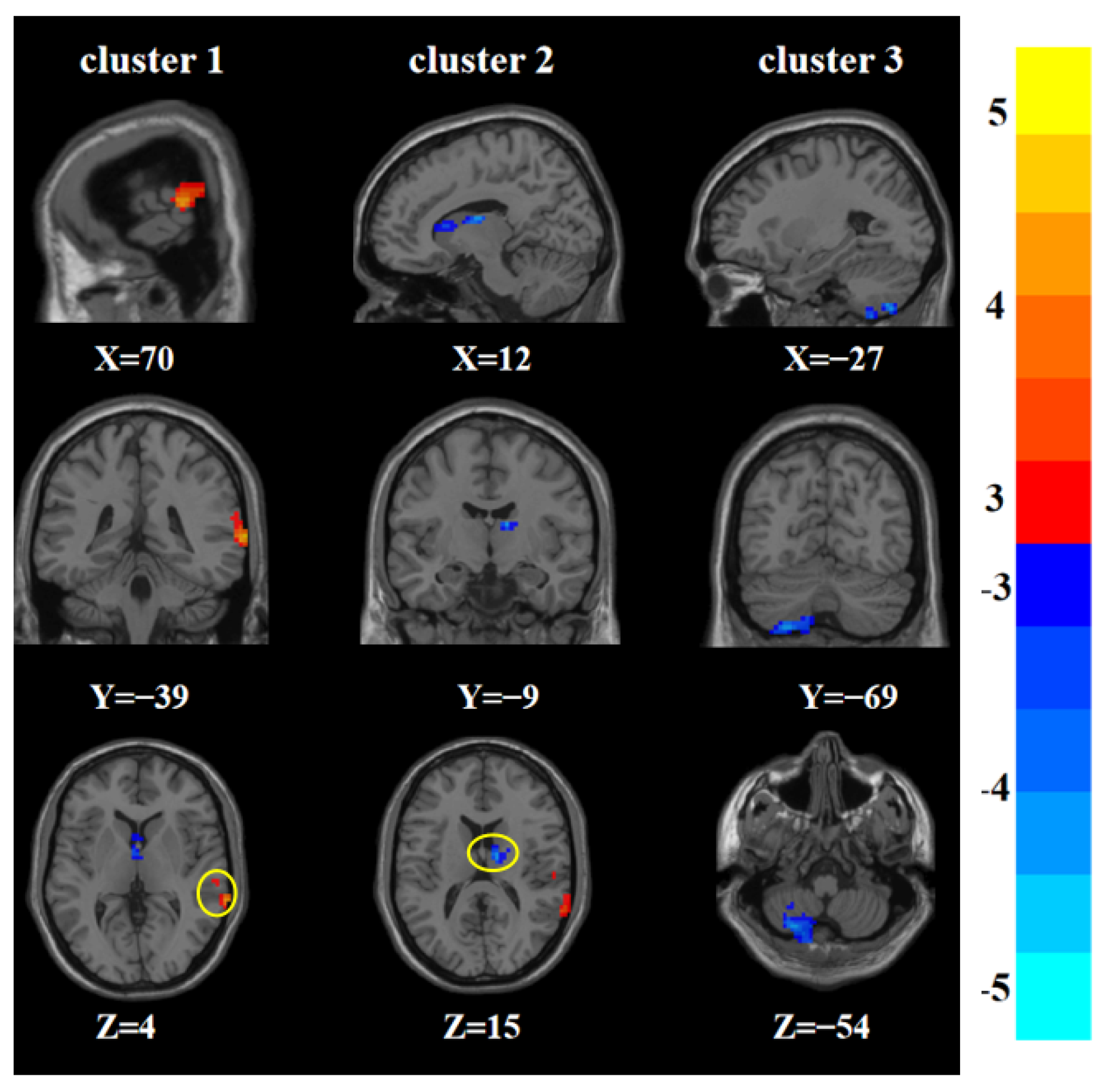
3.2. Main Effects of Sex, Group, and Sex-by-Group Interaction in ReHo among the Four Groups
3.3. Post-Hoc Analysis Effects of the Sex-by-Group Interaction in ReHo among the Four Groups
3.4. Correlation Analysis
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Schechter, L.E. Major depressive disorder. Curr. Pharm. Des. 2005, 11, 143–144. [Google Scholar] [CrossRef] [PubMed]
- Malh, G.S.; Mann, J.J. Depression. Lancet 2018, 392, 2299–2312. [Google Scholar] [CrossRef]
- Hiller, W.; Dichtl, G.; Hecht, H.; Hundt, W.; Mombour, W.; von Zerssen, D. Evaluating the new ICD-10 categories of depressive episode and recurrent depressive disorder. J. Affect. Disord. 1994, 31, 49–60. [Google Scholar] [CrossRef]
- Sun, J.; Chen, L.; He, J.; Du, Z.; Ma, Y.; Wang, Z.; Guo, C.; Luo, Y.; Gao, D.; Hong, Y.; et al. Altered Brain Function in First-Episode and Recurrent Depression: A Resting-State Functional Magnetic Resonance Imaging Study. Front. Neurosci. 2022, 16, 876121. [Google Scholar] [CrossRef] [PubMed]
- Roca, M.; Armengol, S.; García-García, M.; Rodriguez-Bayón, A.; Ballesta, I.; Serrano, M.J.; Comas, A.; Gili, M. Clinical differences between first and recurrent episodes in depressive patients. Compr. Psychiatry 2011, 52, 26–32. [Google Scholar] [CrossRef]
- Roca, M.; López-Navarro, E.; Monzón, S.; Vives, M.; García-Toro, M.; García-Campayo, J.; Harrison, J.; Gili, M. Cognitive impairment in remitted and non-remitted depressive patients: A follow-up comparison between first and recurrent episodes. Eur. Neuropsychopharmacol. 2015, 25, 1991–1998. [Google Scholar] [CrossRef]
- Zu, S.; Wang, D.; Fang, J.; Xiao, L.; Zhu, X.; Wu, W.; Wang, G.; Hu, Y. Comparison of Residual Depressive Symptoms, Functioning, and Quality of Life Between Patients with Recurrent Depression and First Episode Depression After Acute Treatment in China. Neuropsychiatr. Dis. Treat. 2021, 17, 3039–3051. [Google Scholar] [CrossRef]
- Andrade, L.; Caraveo-Anduaga, J.J.; Berglund, P.; Bijl, R.V.; De Graaf, R.; Vollebergh, W.; Dragomirecká, E.; Kohn, R.; Keller, M.; Kessler, R.C.; et al. The epidemiology of major depressive episodes: Results from the International Consortium of Psychiatric Epidemiology (ICPE) Surveys. Int. J. Methods Psychiatr. Res. 2003, 12, 3–21. [Google Scholar] [CrossRef] [Green Version]
- Holtzheimer, P.E.; Mayberg, H.S. Stuck in a rut: Rethinking depression and its treatment. Trends Neurosci. 2011, 34, 1–9. [Google Scholar] [CrossRef] [Green Version]
- Liu, C.H.; Zhang, G.Z.; Li, B.; Li, M.; Woelfer, M.; Walter, M.; Wang, L. Role of inflammation in depression relapse. J. Neuroinflamm. 2019, 16, 90. [Google Scholar] [CrossRef]
- Kessler, R.C.; Berglund, P.; Demler, O.; Jin, R.; Koretz, D.; Merikangas, K.R.; Rush, A.J.; Walters, E.E.; Wang, P.S. The epidemiology of major depressive disorder: Results from the National Comorbidity Survey Replication (NCS-R). JAMA 2003, 289, 3095–3105. [Google Scholar] [CrossRef]
- Black, G.; Roberts, R.M.; Li-Leng, T. Depression in rural adolescents: Relationships with gender and availability of mental health services. Rural Remote Health 2012, 12, 2092. [Google Scholar] [CrossRef]
- Jaffee, S.R.; Sligo, J.L.; McAnally, H.M.; Bolton, A.E.; Baxter, J.M.; Hancox, R.J. Early-onset and recurrent depression in parents increases risk of intergenerational transmission to adolescent offspring. J. Child Psychol. Psychiatry 2021, 62, 979–988. [Google Scholar] [CrossRef]
- Kupfer, D.J.; Frank, E.; Carpenter, L.L.; Neiswanger, K. Family history in recurrent depression. J. Affect. Disord. 1989, 17, 113–119. [Google Scholar] [CrossRef]
- Van Loo, H.M.; Aggen, S.H.; Gardner, C.O.; Kendler, K.S. Sex similarities and differences in risk factors for recurrence of major depression. Psychol. Med. 2018, 48, 1685–1693. [Google Scholar] [CrossRef]
- Moskvina, V.; Farmer, A.; Jones, I.R.; Brewster, S.; Ferrero, F.; Gill, M.; Jones, L.A.; Maier, W.; Mors, O.; Owen, M.J.; et al. Sex differences in symptom patterns of recurrent major depression in siblings. Depress. Anxiety 2008, 25, 527–534. [Google Scholar] [CrossRef]
- Curry, J.F.; Shepherd-Banigan, M.; Van Voorhees, E.; Wagner, H.R.; Kelley, M.L.; Strauss, J.; Naylor, J.; Veterans Affairs Mid-Atlantic MIRECC Women Veterans Work Group; Veterans Affairs Mid-Atlantic MIRECC Work Group. Sex differences in predictors of recurrent major depression among current-era military veterans. Psychol. Serv. 2021, 18, 275–284. [Google Scholar] [CrossRef]
- Frank, E.; Carpenter, L.L.; Kupfer, D.J. Sex differences in recurrent depression: Are there any that are significant? Am. J. Psychiatry 1988, 145, 41–45. [Google Scholar] [CrossRef]
- Zhang, F.F.; Peng, W.; Sweeney, J.A.; Jia, Z.Y.; Gong, Q.Y. Brain structure alterations in depression: Psychoradiological evidence. CNS Neurosci. Ther. 2018, 24, 994–1003. [Google Scholar] [CrossRef] [Green Version]
- Barch, D.M.; Tillman, R.; Kelly, D.; Whalen, D.; Gilbert, K.; Luby, J.L. Hippocampal volume and depression among young children. Psychiatry Res. Neuroimaging 2019, 288, 21–28. [Google Scholar] [CrossRef]
- Gangadin, S.S.; Nasib, L.G.; Sommer, I.E.C.; Mandl, R.C.W. MRI investigation of immune dysregulation in schizophrenia. Curr. Opin. Psychiatry 2019, 32, 164–169. [Google Scholar] [CrossRef] [PubMed]
- Han, K.M.; De Berardis, D.; Fornaro, M.; Kim, Y.K. Differentiating between bipolar and unipolar depression in functional and structural MRI studies. Prog. Neuropsychopharmacol. Biol. Psychiatry 2019, 91, 20–27. [Google Scholar] [CrossRef] [PubMed]
- Sun, J.; Du, Z.; Ma, Y.; Chen, L.; Wang, Z.; Guo, C.; Luo, Y.; Gao, D.; Hong, Y.; Zhang, L.; et al. Altered functional connectivity in first-episode and recurrent depression: A resting-state functional magnetic resonance imaging study. Front. Neurol. 2022, 13, 922207. [Google Scholar] [CrossRef] [PubMed]
- Yüksel, D.; Dietsche, B.; Konrad, C.; Dannlowski, U.; Kircher, T.; Krug, A. Neural correlates of working memory in first episode and recurrent depression: An fMRI study. Prog. Neuropsychopharmacol. Biol. Psychiatry 2018, 84 Pt A, 39–49. [Google Scholar] [CrossRef]
- Runia, N.; Yücel, D.E.; Lok, A.; de Jong, K.; Denys, D.A.; van Wingen, G.A.; Bergfeld, I.O. The neurobiology of treatment-resistant depression: A systematic review of neuroimaging studies. Neurosci. Biobehav. Rev. 2022, 132, 433–448. [Google Scholar] [CrossRef] [PubMed]
- Keller, S.S.; Baker, G.; Downes, J.J.; Roberts, N. Quantitative MRI of the prefrontal cortex and executive function in patients with temporal lobe epilepsy. Epilepsy Behav. 2009, 15, 186–195. [Google Scholar] [CrossRef] [PubMed]
- Miskin, N.; Thesen, T.; Barr, W.B.; Butler, T.; Wang, X.; Dugan, P.; Kuzniecky, R.; Doyle, W.K.; Devinsky, O.; Blackmon, K. Prefrontal lobe structural integrity and trail making test, part B: Converging findings from surface-based cortical thickness and voxel-based lesion symptom analyses. Brain Imaging Behav. 2016, 10, 675–685. [Google Scholar] [CrossRef] [PubMed]
- Yang, X.; Peng, Z.; Ma, X.; Meng, Y.; Li, M.; Zhang, J.; Song, X.; Liu, Y.; Fan, H.; Zhao, L.; et al. Sex differences in the clinical characteristics and brain gray matter volume alterations in unmedicated patients with major depressive disorder. Sci. Rep. 2017, 7, 2515. [Google Scholar] [CrossRef]
- Hu, X.; Zhang, L.; Liang, K.; Cao, L.; Liu, J.; Li, H.; Gao, Y.; Hu, Y.; Kuang, W.; Sweeney, J.A.; et al. Sex-specific alterations of cortical morphometry in treatment-naïve patients with major depressive disorder. Neuropsychopharmacology 2022, 47, 2002–2009. [Google Scholar] [CrossRef]
- Kliamovich, D.; Jones, S.A.; Chiapuzio, A.M.; Baker, F.C.; Clark, D.B.; Nagel, B.J. Sex-specific patterns of white matter microstructure are associated with emerging depression during adolescence. Psychiatry Res. Neuroimaging 2021, 315, 111324. [Google Scholar] [CrossRef]
- Jenkins, L.M.; Kendall, A.D.; Kassel, M.T.; Patrón, V.; Gowins, J.; Dion, C.; Shankman, S.; Weisenbach, S.; Maki, P.; Langenecker, S. Considering sex differences clarifies the effects of depression on facial emotion processing during fMRI. J. Affect. Disord. 2018, 225, 129–136. [Google Scholar] [CrossRef]
- Mei, L.; Wang, Y.; Liu, C.; Mou, J.; Yuan, Y.; Qiu, L.; Gong, Q. Study of Sex Differences in Unmedicated Patients With Major Depressive Disorder by Using Resting State Brain Functional Magnetic Resonance Imaging. Front. Neurosci. 2022, 16, 814410. [Google Scholar] [CrossRef] [PubMed]
- Yao, Z.; Yan, R.; Wei, M.; Tang, H.; Qin, J.; Lu, Q. Gender differences in brain activity and the relationship between brain activity and differences in prevalence rates between male and female major depressive disorder patients: A resting-state fMRI study. Clin. Neurophysiol. 2014, 125, 2232–2239. [Google Scholar] [CrossRef] [PubMed]
- Zang, Y.; Jiang, T.; Lu, Y.; He, Y.; Tian, L. Regional homogeneity approach to fMRI data analysis. Neuroimage 2004, 22, 394–400. [Google Scholar] [CrossRef]
- Sun, J.F.; Chen, L.M.; He, J.K.; Wang, Z.; Guo, C.-L.; Ma, Y.; Luo, Y.; Gao, D.-Q.; Hong, Y.; Fang, J.-L.; et al. A Comparative Study of Regional Homogeneity of Resting-State fMRI Between the Early-Onset and Late-Onset Recurrent Depression in Adults. Front. Psychol. 2022, 13, 849847. [Google Scholar] [CrossRef] [PubMed]
- Chen, J.D.; Liu, F.; Xun, G.L.; Chen, H.-F.; Hu, M.-R.; Guo, X.-F.; Xiao, C.-Q.; Wooderson, S.C.; Guo, W.-B.; Zhao, J.-P. Early and late onset, first-episode, treatment-naive depression: Same clinical symptoms, different regional neural activities. J. Affect. Disord. 2012, 143, 56–63. [Google Scholar] [CrossRef] [PubMed]
- Chao-Gan, Y.; Yu-Feng, Z. DPARSF: A MATLAB Toolbox for “Pipeline” Data Analysis of Resting-State fMRI. Front. Syst. Neurosci. 2010, 4, 13. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Brosch, K.; Stein, F.; Meller, T.; Schmitt, S.; Yuksel, D.; Ringwald, K.G.; Pfarr, J.-K.; Waltemate, L.; Lemke, H.; Opel, N.; et al. DLPFC volume is a neural correlate of resilience in healthy high-risk individuals with both childhood maltreatment and familial risk for depression. Psychol. Med. 2021; 1–7, ahead of print. [Google Scholar] [CrossRef]
- Nejati, V.; Majidinezhad, M.; Nitsche, M. The role of the dorsolateral and ventromedial prefrontal cortex in emotion regulation in females with major depressive disorder (MDD): A tDCS study. J. Psychiatr. Res. 2022, 148, 149–158. [Google Scholar] [CrossRef]
- Elliott, R. Executive functions and their disorders. Br. Med. Bull. 2003, 65, 49–59. [Google Scholar] [CrossRef] [Green Version]
- Vasic, N.; Wolf, R.C.; Walter, H. Exekutive Funktionen bei depressiven Patienten. Zur Rolle der präfrontalen Aktivierung Executive functions in patients with depression. The role of prefrontal activation. Nervenarzt 2007, 78, 628–640. [Google Scholar] [CrossRef]
- Harika-Germaneau, G.; Wassouf, I.; Le Tutour, T.; Guillevin, R.; Doolub, D.; Rostami, R.; Delbreil, A.; Langbour, N.; Jaafari, N. Baseline Clinical and Neuroimaging Biomarkers of Treatment Response to High-Frequency rTMS Over the Left DLPFC for Resistant Depression. Front. Psychiatry 2022, 13, 894473. [Google Scholar] [CrossRef]
- Peng, H.; Zheng, H.; Li, L.; Liu, J.; Zhang, Y.; Shan, B.; Zhang, L.; Yin, Y.; Liu, J.; Li, W.; et al. High-frequency rTMS treatment increases white matter FA in the left middle frontal gyrus in young patients with treatment-resistant depression. J. Affect. Disord. 2012, 136, 249–257. [Google Scholar] [CrossRef]
- DeRubeis, R.J.; Siegle, G.J.; Hollon, S.D. Cognitive therapy versus medication for depression: Treatment outcomes and neural mechanisms. Nat. Rev. Neurosci. 2008, 9, 788–796. [Google Scholar] [CrossRef] [Green Version]
- Guan, M.; Wang, Z.; Shi, Y.; Xie, Y.; Ma, Z.; Liu, Z.; Liu, J.; Gao, X.; Tan, Q.; Wang, H. Altered Brain Function and Causal Connectivity Induced by Repetitive Transcranial Magnetic Stimulation Treatment for Major Depressive Disorder. Front. Neurosci. 2022, 16, 855483. [Google Scholar] [CrossRef]
- Penfield, W.; Faulk, M., Jr. The insula; further observations on its function. Brain 1955, 78, 445–470. [Google Scholar] [CrossRef]
- Nagai, M.; Kishi, K.; Kato, S. Insular cortex and neuropsychiatric disorders: A review of recent literature. Eur. Psychiatry 2007, 22, 387–394. [Google Scholar] [CrossRef]
- Cauda, F.; D’Agata, F.; Sacco, K.; Duca, S.; Geminiani, G.; Vercelli, A. Functional connectivity of the insula in the resting brain. Neuroimage 2011, 55, 8–23. [Google Scholar] [CrossRef]
- Reynolds, S.M.; Zahm, D.S. Specificity in the projections of prefrontal and insular cortex to ventral striatopallidum and the extended amygdala. J. Neurosci. 2005, 25, 11757–11767. [Google Scholar] [CrossRef] [Green Version]
- Ongür, D.; Price, J.L. The organization of networks within the orbital and medial prefrontal cortex of rats, monkeys and humans. Cereb. Cortex 2000, 10, 206–219. [Google Scholar] [CrossRef]
- Liu, C.H.; Ma, X.; Yuan, Z.; Song, L.-P.; Jing, B.; Lu, H.-Y.; Tang, L.-R.; Fan, J.; Walter, M.; Liu, C.-Z.; et al. Decreased Resting-State Activity in the Precuneus Is Associated With Depressive Episodes in Recurrent Depression. J. Clin. Psychiatry 2017, 78, e372–e382. [Google Scholar] [CrossRef] [PubMed]
- Wang, L.; Li, K.; Zhang, Q.; Zeng, Y.; Dai, W.; Su, Y.; Wang, G.; Tan, Y.; Jin, Z.; Yu, X.; et al. Short-term effects of escitalopram on regional brain function in first-episode drug-naive patients with major depressive disorder assessed by resting-state functional magnetic resonance imaging. Psychol. Med. 2014, 44, 1417–1426. [Google Scholar] [CrossRef] [PubMed]
- Brennan, D.; Wu, T.; Fan, J. Morphometrical Brain Markers of Sex Difference. Cereb. Cortex 2021, 31, 3641–3649. [Google Scholar] [CrossRef] [PubMed]
- Young, K.D.; Bodurka, J.; Drevets, W.C. Functional neuroimaging of sex differences in autobiographical memory recall in depression. Psychol. Med. 2017, 47, 2640–2652. [Google Scholar] [CrossRef] [PubMed]
- Zhou, L.; Tian, N.; Geng, Z.J.; Wu, B.K.; Dong, L.Y.; Wang, M.R. Diffusion tensor imaging study of brain precentral gyrus and postcentral gyrus during normal brain aging process. Brain Behav. 2020, 10, e01758. [Google Scholar] [CrossRef]
- Geng, J.; Yan, R.; Shi, J.; Chen, Y.; Mo, Z.; Shao, J.; Wang, X.; Yao, Z.; Lu, Q. Altered regional homogeneity in patients with somatic depression: A resting-state fMRI study. J. Affect. Disord. 2019, 246, 498–505. [Google Scholar] [CrossRef]
- Liu, P.; Tu, H.; Zhang, A.; Yang, C.; Liu, Z.; Lei, L.; Wu, P.; Sun, N.; Zhang, K. Brain functional alterations in MDD patients with somatic symptoms: A resting-state fMRI study. J. Affect. Disord. 2021, 295, 788–796. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variable | Male RDE (n = 19) | Female RDE (n = 21) | Male HCs (n = 20) | Female HCs (n = 22) | t(F)/χ2 | p Value |
|---|---|---|---|---|---|---|
| Age (years) | 39.78 ± 11.24 | 40.42 ± 13.58 | 39.90 ± 11.30 | 41.59 ± 11.85 | 0.098 | 0.961 a |
| Education (years) | 13.89 ± 2.74 | 13.42 ± 3.41 | 15.50 ± 3.50 | 13.77 ± 4.17 | 0.752 | 0.525 b |
| Duration of illness (months) | 28.57 ± 16.97 | 25.94 ± 11.50 | NA | NA | 0.578 | 0.567 C |
| HAMD-17 score | 22.34 ± 3.45 | 23.04 ± 3.72 | NA | NA | −0.180 | 0.858 C |
| Frequency of recurrence | 1.78 ± 0.85 | 1.85 ± 0.79 | NA | NA | −0.260 | 0.796 C |
| Clusters | Brain Regions | Peak Coordinates (MNI) | Cluster Size | T/F Values | ||
|---|---|---|---|---|---|---|
| X | Y | Z | ||||
| Main effects of sex (Male vs. Female) | ||||||
| 1 | Right middle temporal gyrus | 70 | −39 | 4 | 115 | 4.222 a |
| 2 | Right thalamus | 12 | −9 | 15 | 102 | −4.500 a |
| 3 | Left posterior cerebellar lobe | −27 | −69 | −54 | 166 | −4.601 a |
| Sex-by-group interaction effects | ||||||
| 1 | Left middle frontal gyrus | −24 | 12 | 45 | 25 | 24.895 b |
| 2 | Left precentral gyrus | −30 | −24 | 60 | 25 | 21.278 b |
| 3 | Right insula | 40 | 18 | −15 | 28 | 21.722 b |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sun, J.; Gao, S.; Ma, Y.; Guo, C.; Du, Z.; Luo, Y.; Chen, L.; Wang, Z.; Li, X.; Xu, K.; et al. A Study of Differential Resting-State Brain Functional Activity in Males and Females with Recurrent Depressive Disorder. Brain Sci. 2022, 12, 1508. https://doi.org/10.3390/brainsci12111508
Sun J, Gao S, Ma Y, Guo C, Du Z, Luo Y, Chen L, Wang Z, Li X, Xu K, et al. A Study of Differential Resting-State Brain Functional Activity in Males and Females with Recurrent Depressive Disorder. Brain Sciences. 2022; 12(11):1508. https://doi.org/10.3390/brainsci12111508
Chicago/Turabian StyleSun, Jifei, Shanshan Gao, Yue Ma, Chunlei Guo, Zhongming Du, Yi Luo, Limei Chen, Zhi Wang, Xiaojiao Li, Ke Xu, and et al. 2022. "A Study of Differential Resting-State Brain Functional Activity in Males and Females with Recurrent Depressive Disorder" Brain Sciences 12, no. 11: 1508. https://doi.org/10.3390/brainsci12111508