
The Effect of Beta-Carotene on Cognitive Function: A Systematic Review

 , ,
, ,  , , and
, , and 
Abstract
:1. Introduction
2. Methods
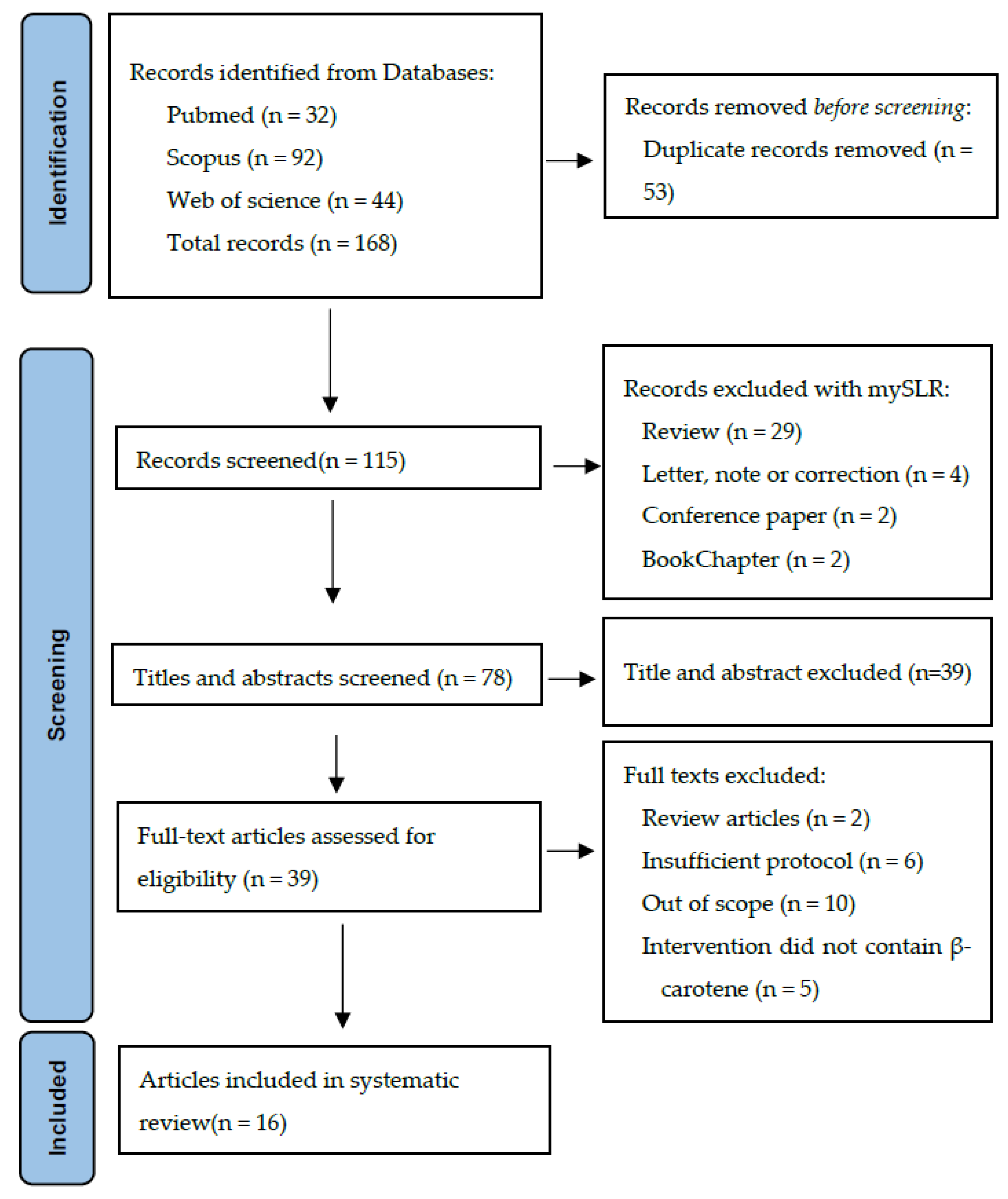
2.1. Paper Location and Selection
2.2. Study Selection and Data Extraction
2.3. Quality Assessment and Levels of Evidence
2.4. Results Presentation
3. Results
3.1. Characteristics of the Studies Included

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Study | Location | Level of Evidence | Study Design | Participant Characteristics | Dietary Intake/Intervention | Conditions | Outcome of Interest | Cognitive Test Used | Reference |
|---|---|---|---|---|---|---|---|---|---|
| Zhong et al. (2023) | USA | 4 | Cross-sectional | n = 2009; 985 males and 1024 females; aged >60 y | Dietary BC intake: Q1 (≤338 μg/d); Q2 (338 to ≤819 μg/d); Q3 (819 to ≤2222.5 μg/d); Q4 (>2222.5 μg/d) | Participants in NHANES 2011–2014 older than 60 y that had completed data on cognitive function | Memory Processing speed and working memory Categorical verbal fluency | CERAD WL DSST AFT | [29] |
| Beydoun et al. (2020) | USA | 3 | Prospective cohort | n = 1251; male; aged 30–65 y at baseline | Dietary BC intake: overall, 1819 ± 2882 μg/d; T1 = 309 ± 289 μg/d; T2 = 1226 ± 987 μg/d; T3 = 3980 ± 4152 μg/d | Healthy subjects; BC intake assessed at V1; cognitive performance assessed at V1 (2004–2009) and V2 (2009–2013) | Global cognition Attention Learning/memory Executive function Visuo-spatial/visuo-construction ability Psychomotor speed Language/verbal | MMSE CVLT Digit span test BVRT AFT BTA TMT A/B CDT | [30] |
| Yuan et al. (2020) | USA | 3 | Prospective cohort | n = 49493; female (nurses); mean age 48 y | Dietary BC intake: Q1 = 2.5 ± 0.5 mg/d; without supplements 2.3 ± 5.4 mg/d; Q5 = 8.6 ± 2.1 mg/d; without supplements 6.9 ± 2.1 mg/d | Healthy subjects; FFQs collected at baseline and periodically until 2006; self-reported SCF in 2012 and 2014 | General memory Executive function Attention Visuospatial skills | Assessment of SCF based on 7 yes/no questions on recent changes | [31] |
| Li et al. (2015) | China | 2 | Intervention | n = 276; 116 male and 160 female; aged 67.06 ± 5.33 y | Groups A, B, C, and D received 200 mg/d VE and 300 mg/d VC, combined with 16.7, 8.4, 5.6, or 0 mg/d BC, respectively. Group E: 5 mg/d VE | Healthy subjects; 5 groups A-E (n = 60 per group, there were 24 drop outs); 16 weeks of intervention; cognitive function assessed prior to and after the intervention | Global cognitive function | MMSE HDS | [33] |
| Nooyens et al. (2015) | Netherland | 3 | Prospective cohort | n = 2613; both sexes; aged 43–70 y at baseline | Dietary intake at baseline and follow-up through a validated self-administered semi-quantitative FFQ. Estimated BC intake: 1480 ± 593 μg/d | Healthy subjects; cognitive performance assessed 5 y after baseline | Global cognitive function Memory Processing speed Cognitive flexibility | 15 Words Learning test Stroop test WFT Letter digit substitution test | [34] |
| Kesse-Guyot et al. (2011) | France | 2 | Randomized double-blind placebo-controlled trial | n = 4447; both sexes; aged 45–60 y | Multivitamin (6 mg/d BC) or placebo | Healthy subjects; 8 y of intervention; cognitive performance assessed 6 y after the end of the intervention | Episodic memory Executive function Verbal memory Verbal fluency | TMT FDST RI-48 Semantic fluency Phonemic fluency | [37] |
| Péneau et al. (2011) | France | 3 | Prospective cohort | n = 2533; male and female; aged 45–60 y at baseline | Dietary intake of FVs grouped based on their nutrient content: folate-rich FVs and BC-rich FVs | Healthy subjects; cognitive performance assessed 13 y after baseline | Episodic memory Lexical semantic memory Mental flexibility Working memory | RI-48 Verbal fluency test TMT FDST | [38] |
| Kang et al. (2009) | USA | 2 | 2 × 2 × 2 randomized placebo-controlled trial | n = 2824; female; aged >65 y | BC (50 mg every other day) or placebo alone or combined with VE, VC, or both | Women with cardiovascular disease; 3.5 y of intervention | Global cognition Verbal memory Category fluency | TICS EBMT CFT | [42] |
| Grodstein et al. (2007) | USA | 2 | Randomized double-blind placebo-controlled trial | n = 4052; male; mean age 55.9 y | 50 mg BC on alternate days | Healthy subjects; 18 y of intervention | Global cognition Verbal memory Category fluency | TICS EBMT CFT | [40] |
| Wolters et al. (2005) | Germany | 2 | Randomized double-blind placebo-controlled trial | n = 220; female; aged 60–91 y | Multivitamin (9 mg/d BC) or placebo | Healthy subjects, free-living women; 6 months of intervention | Total Intellectual Quotient Intelligence Assessment of mild up to severe memory disorders | WAIS-III KAI BAT | [41] |
| Smith et al. (1999) | UK | 2 | Randomized double-blind placebo-controlled trial | n = 205; male and female; aged 60–80 y | Multivitamin (12 mg/d BC) or placebo | 12 months of intervention | Episodic memory Psychomotor speed Attention | NART score CFQ score | [39] |
| Study | Location | Level of Evidence | Study Design | Participant Characteristics | Blood Levels | Condition | Outcome of Interest | Cognitive Test Used | Reference |
|---|---|---|---|---|---|---|---|---|---|
| Gerger et al. (2019) | Germany | 2 | Multi-centered randomized controlled trial | n = 56; female; aged 73.1 ± 5,8 y | BC (μM): 0.74 ± 0.65 | Subjects with mild cognitive impairment participating in the NeuroExercise study | Global cognition Verbal memory Working memory Attention Executive function | MoCA ISLT ONB TMT | [32] |
| Johnson et al. (2013) | USA(Georgia) | 4 | Cross-sectional | n = 298, of which 78 were octogenarians and 220 centenarians; male and female | BC (nmol/L): octogenarians, 568 ± 855; centenarians, 460 ± 432 | Institutionalized and community-dwelling subjects compared; study conducted from 2001 to 2009 | Memory processing speed Attention Executive functioning | MMSE GDRS SIB FOME WAIS-III Similarities subtest BDS COWAT | [35] |
| Akbaraly et al. (2007) | France | 4 | Cross-sectional | n = 589; 361 female and 228 male; aged 73.5 ± 3 y | Trans-BC levels, 0.73 ± 0.52 μmol/L; cis-BC levels, 0.10 ± 0.12 μmol/L | Healthy old subjects | Global cognition Motor speed Working memory Executive function Attention and logical reasoning Verbal fluency | MMSE TMTA TMTB DSST WFT | [36] |
| Perkins et al. (1999) | USA | 4 | Cross-sectional | n = 4809; female; aged >60 y | BC normalized on units of total cholesterol: <0.06; 0.06–0.09; 0.09–0.15; >0.15 | Elderly, multi-ethnic group followed from 1988 to 1994 | Memory | Assessed using delayed recall (6 points from a story and 3 words), with poor memory defined by a combined score < 4 | [43] |
| Perrig et al. (1997) | Switzerland | 4 | Longitudinal and cross-sectional comparisons | n = 442; 312 male, 132 female; aged 65 to 94 y | BC measured in 1971 (T1) and 1993 (T2); BC levels (µg/dL): T1, 0.51 ± 0.31; T2, 0.72 ± 0.48 | Healthy old subjects selected in T2 by random sampling from a large cohort established in T1; cognitive function assessed in T2 | Implicit and explicit memory Working memory Semantic memory | Free recall and recognitionWAIS-R Vocabulary test | [28] |
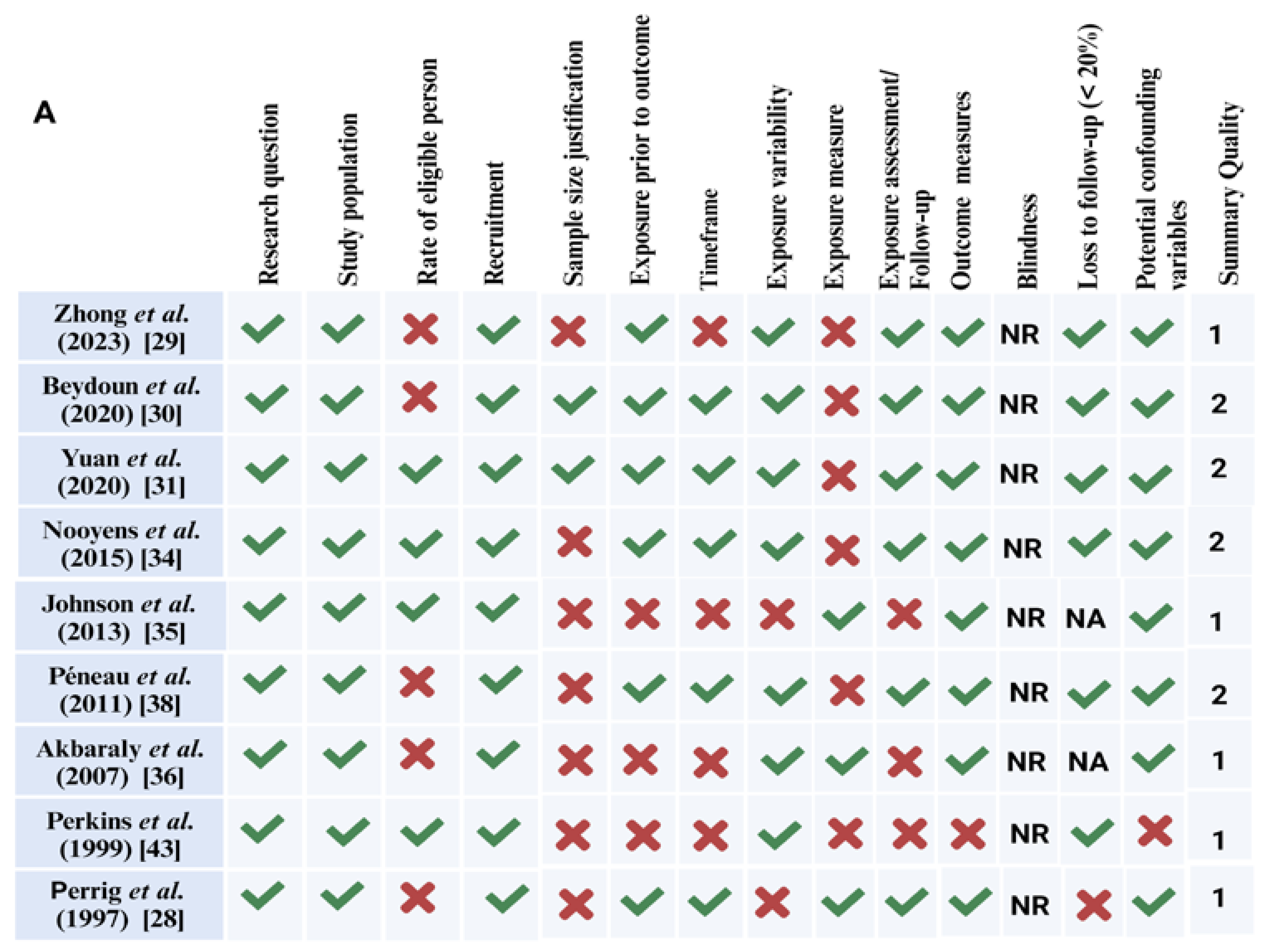
3.2. Risk of Bias Assessment
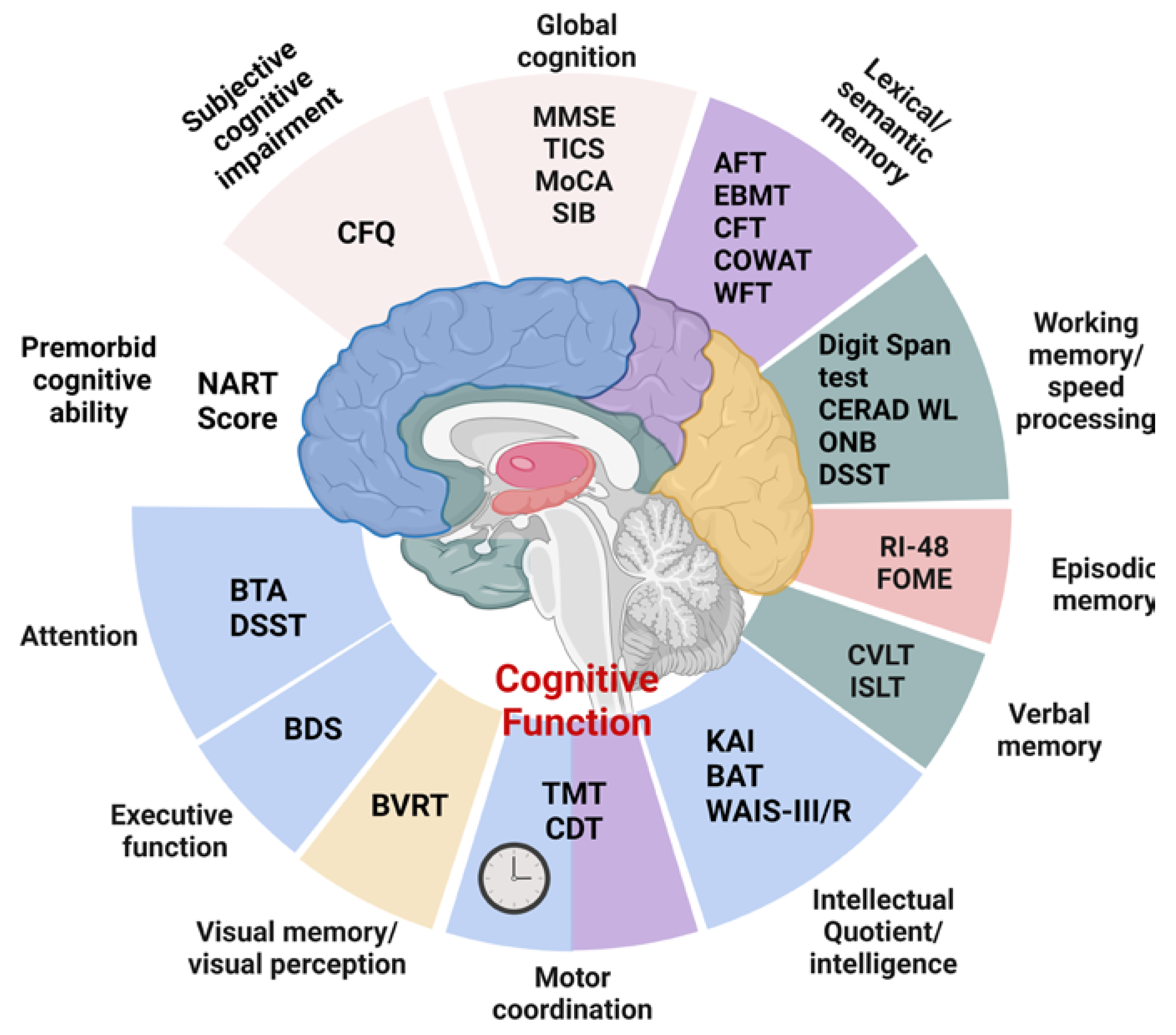
3.3. Topic Identification
3.3.1. Topic 2: Antioxidants: β-carotene Dietary Intake and Its Relationship with Cognitive Function
3.3.2. Topic 1. The Impact of β-carotene Supplementation with a Multivitamin on Cognitive Performance
4. Discussion
5. Conclusions
6. Strength and Limitation
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| AFT | Animal Fluency Test |
| BAT | Berliner Amnesie Test |
| BC | β-carotene |
| BDNF | Brain-Derived Neurotrophic Factor |
| BDS | Behavioral Dyscontrol Scale |
| BTA | Brief Test of Attention |
| BVRT | Benton Visual Retention Test |
| CERAD WL | Consortium to Establish a Registry for Alzheimer’s Disease Word Learning |
| CFQ score | Cognitive Failures Questionnaire |
| CDT | Clock Drawing Test |
| CFT | Category Fluency Test |
| CVLT | California Verbal Learning Test |
| COWAT | Controlled Oral Word Association Test |
| DCS | Doetinchem Cohort Study |
| DFR | Delayed Free Recall |
| DSST | Digit Symbol Substitution Test |
| EBMT | East Boston Memory Test |
| FDST | Forward digit span test |
| FFQ | Food Frequency Questionnaire |
| FOME | Fuld Object Memory Evaluation |
| FVs | Fruit and vegetables |
| GDRS | Global Deterioration Rating Scale |
| HDS | Hasegawa Dementia Scale |
| ISLT | International Shopping List Task |
| RI-48 | Cued Recall Test |
| KAI | Kurztest fuer Allgemeine Intelligenz |
| LDA | Latent Dirichlet Allocation |
| MMSE | Mini-mental state examination |
| MoCA | Montreal Cognitive Assessment |
| NART | National Adult Reading Test |
| NIH | National Institutes of Health |
| ONB | One Back Task |
| PHS | Physicians’ Health Study |
| PHSII | Physicians’ Health Study II |
| SIB | Severe Impairment Battery |
| NHANES | National Health and Nutrition Examination Survey |
| NHS | Nurses’ Health Study |
| SCF | Subjective Cognitive Function |
| TICS | Telephone Interview of Cognitive Status |
| TMT | Trail Making Test |
| TMTA | Trail Making Test A |
| TMTB | Trail Making Test B |
| VA | Vitamin A |
| VE | Vitamin E |
| VC | Vitamin C |
| WAIS-III | Wechsler Adult Intelligence Scale Revised |
| WFT | Word Fluency Test |
| WACS | Women’s Antioxidant Cardiovascular Study |
References
- Robinson, M. Encyclopedia of Quality of Life and Well-being Research. Ref. Rev. 2015, 29, 22. [Google Scholar] [CrossRef]
- Birle, C.; Slavoaca, D.; Balea, M.; Livint Popa, L.; Muresanu, I.; Stefanescu, E.; Vacaras, V.; Dina, C.; Strilciuc, S.; Popescu, B.O.; et al. Cognitive function: Holarchy or holacracy? Neurol. Sci. 2021, 42, 89–99. [Google Scholar] [CrossRef] [PubMed]
- Cione, E.; Abrego Guandique, D.M.; Caroleo, M.C.; Luciani, F.; Colosimo, M.; Cannataro, R. Liver Damage and microRNAs: An Update. Curr. Issues Mol. Biol. 2022, 45, 78–91. [Google Scholar] [CrossRef] [PubMed]
- Iannone, F.; Montesanto, A.; Cione, E.; Crocco, P.; Caroleo, M.C.; Dato, S.; Rose, G.; Passarino, G. Expression patterns of muscle-specific miR-133b and miR-206 correlate with nutritional status and sarcopenia. Nutrients 2020, 12, 297. [Google Scholar] [CrossRef] [PubMed]
- Van Dijk, D.M.; Van Rhenen, W.; Murre, J.M.J.; Verwijk, E. Cognitive functioning, sleep quality, and work performance in non-clinical burnout: The role of working memory. PLoS ONE 2020, 15, e0231906. [Google Scholar] [CrossRef] [PubMed]
- Williams, A.M.; Ford, P.R.; Eccles, D.W.; Ward, P. Perceptual-cognitive expertise in sport and its acquisition: Implications for applied cognitive psychology. Appl. Cogn. Psychol. 2011, 25, 432–442. Available online: http://ovidsp.ovid.com/ovidweb.cgi?T=JS&PAGE=reference&D=emed10&NEWS=N&AN=2011280445 (accessed on 9 July 2023). [CrossRef]
- Hernández-Mendo, A.; Reigal, R.E.; López-Walle, J.M.; Serpa, S.; Samdal, O.; Morales-Sánchez, V.; Juárez-Ruiz de Mier, R.; Tristán-Rodríguez, J.L.; Rosado, A.F.; Falco, C. Physical Activity, Sports Practice, and Cognitive Functioning: The Current Research Status. Front. Psychol. 2019, 10, 2658. [Google Scholar] [CrossRef]
- Murman, D.L. The Impact of Age on Cognition. Semin. Hear. 2015, 36, 111–121. Available online: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4906299/ (accessed on 9 July 2023). [CrossRef]
- Pais, R.; Ruano, L.; Carvalho, O.P.; Barros, H. Global cognitive impairment prevalence and incidence in community dwelling older adults—A systematic review. Geriatrics 2020, 5, 84. [Google Scholar] [CrossRef]
- Walczak, P.; Janowski, M. Chemobrain as a Product of Growing Success in Chemotherapy—Focus On Glia As Both A Victim And A Cure. Neuropsychiatry 2019, 9, 2207. [Google Scholar] [CrossRef]
- Fehlauer, F.; Tribius, S.; Mehnert, A.; Rades, D. Health-related quality of life in long term breast cancer survivors treated with breast conserving therapy: Impact of age at therapy. Breast Cancer Res. Treat. 2005, 92, 217–222. [Google Scholar] [CrossRef] [PubMed]
- Sukel, K. Lifting the fog. New Sci. 2022, 254, 38–41. [Google Scholar] [CrossRef] [PubMed]
- Guo, P.; Benito Ballesteros, A.; Yeung, S.P.; Liu, R.; Saha, A.; Curtis, L.; Cheke, L.G. COVCOG 2: Cognitive and Memory Deficits in Long COVID: A Second Publication From the COVID and Cognition Study. Front. Aging Neurosci. 2022, 14, 804937. Available online: https://pubmed.ncbi.nlm.nih.gov/35370620/ (accessed on 9 July 2023). [CrossRef] [PubMed]
- Guo, P.; Benito Ballesteros, A.; Yeung, S.P.; Liu, R.; Saha, A.; Curtis, L.; Cheke, L.G. COVCOG 1: Factors Predicting Physical, Neurological and Cognitive Symptoms in Long COVID in a Community Sample. A First Publication From the COVID and Cognition Study. Front. Aging Neurosci. 2022, 14, 804922. Available online: https://pubmed.ncbi.nlm.nih.gov/35370617/ (accessed on 9 July 2023). [CrossRef] [PubMed]
- Kandlur, A.; Satyamoorthy, K.; Gangadharan, G. Oxidative Stress in Cognitive and Epigenetic Aging: A Retrospective Glance. Front. Mol. Neurosci. 2020, 13, 41. [Google Scholar] [CrossRef] [PubMed]
- Berr, C.; Balansard, B.; Arnaud, J.; Roussel, A.M.; Alpérovitch, A. Cognitive decline is associated with systemic oxidative stress: The EVA study. Etude du Vieillissement Artériel. J. Am. Geriatr. Soc. 2000, 48, 1285–1291. Available online: http://www.ncbi.nlm.nih.gov/pubmed/11037017 (accessed on 9 July 2023). [CrossRef] [PubMed]
- Zhang, J.; Lei, W.; Chen, X.; Wang, S.; Qian, W. Oxidative stress response induced by chemotherapy in leukemia treatment (Review). Mol. Clin. Oncol. 2018, 8, 391–399. [Google Scholar] [CrossRef] [PubMed]
- Bohn, T.; Bonet, M.L.; Borel, P.; Keijer, J.; Landrier, J.F.; Milisav, I.; Ribot, J.; Riso, P.; Winklhofer-Roob, B.; Sharoni, Y.; et al. Mechanistic aspects of carotenoid health benefits—Where are we now? Nutr. Res. Rev. 2021, 34, 276–302. [Google Scholar] [CrossRef]
- Rodriguez-Concepcion, M.; Avalos, J.; Bonet, M.L.; Boronat, A.; Gomez-Gomez, L.; Hornero-Mendez, D.; Limon, M.C.; Meléndez-Martínez, A.J.; Olmedilla-Alonso, B.; Palou, A.; et al. A global perspective on carotenoids: Metabolism, biotechnology, and benefits for nutrition and health. Prog. Lipid Res. 2018, 70, 62–93. [Google Scholar] [CrossRef]
- Shete, V.; Quadro, L. Mammalian metabolism of β-carotene: Gaps in knowledge. Nutrients 2013, 5, 4849–4868. [Google Scholar] [CrossRef]
- Jenab, M.; Salvini, S.; Van Gils, C.H.; Brustad, M.; Shakya-Shrestha, S.; Buijsse, B.; Verhagen, H.; Touvier, M.; Biessy, C.; Wallström, P.; et al. Dietary intakes of retinol, β-carotene, vitamin D and vitamin E in the european prospective investigation into cancer and nutrition cohort. Eur. J. Clin. Nutr. 2009, 63, S150–S178. [Google Scholar] [CrossRef] [PubMed]
- Saari, J.C. Vitamin A and Vision. In The Biochemistry of Retinoid Signaling II. Subcellular Biochemistry; Asson-Batres, M., Rochette-Egly, C., Eds.; Springer: Dordrecht, The Netherland, 2016; Volume 81, pp. 231–259. [Google Scholar] [CrossRef]
- Huang, Z.; Liu, Y.; Qi, G.; Brand, D.; Zheng, S.G. Role of vitamin A in the immune system. J. Clin. Med. 2018, 7, 258. [Google Scholar] [CrossRef] [PubMed]
- Malivindi, R.; Rago, V.; De Rose, D.; Gervasi, M.C.; Cione, E.; Russo, G.; Aquila, S. Influence of all-trans retinoic acid on sperm metabolism and oxidative stress: Its involvement in the physiopathology of varicocele-associated male infertility. J. Cell. Physiol. 2018, 233, 9526–9537. Available online: http://www.embase.com/search/results?subaction=viewrecord&from=export&id=L624279221%0A (accessed on 9 July 2023). [CrossRef] [PubMed]
- Ammirato, S.; Felicetti, A.M.; Rogano, D.; Linzalone, R.; Corvello, V. Digitalising the Systematic Literature Review process: The MySLR platform. Knowl. Manag. Res. Pract. 2022, 21, 777–794. [Google Scholar] [CrossRef]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. J. Clin. Epidemiol. 2009, 62, 1006–1012. [Google Scholar] [CrossRef] [PubMed]
- Melnyk, B.M.; Fineout-Overholt, E. Evidence-Based Practice in Nursing & Healthcare: A Guide to Best Practice, 5th ed.; Wolters Kluwer: Philadelphia, PA, USA, 2023; ISBN 9781975185725. [Google Scholar]
- Perrig, W.J.; Perrig, P.; Stähelin, H.B. The relation between antioxidants and memory performance in the old and very old. J. Am. Geriatr. Soc. 1997, 45, 718–724. [Google Scholar] [CrossRef]
- Zhong, Q.; Sun, W.; Qin, Y.; Xu, H. Association of Dietary α-Carotene and β-Carotene Intake with Low Cognitive Performance in Older Adults: A Cross-Sectional Study from the National Health and Nutrition Examination Survey. Nutrients 2023, 15, 239. [Google Scholar] [CrossRef] [PubMed]
- Beydoun, M.A.; Canas, J.A.; Fanelli-Kuczmarski, M.T.; Maldonado, A.I.; Shaked, D.; Kivimaki, M.; Evans, M.K.; Zonderman, A.B. Association of antioxidant vitamins a, c, e and carotenoids with cognitive performance over time: A cohort study of middle-aged adults. Nutrients 2020, 12, 3558. [Google Scholar] [CrossRef]
- Yuan, C.; Fondell, E.; Ascherio, A.; Okereke, O.I.; Grodstein, F.; Hofman, A.; Willett, W.C. Long-Term Intake of Dietary Carotenoids Is Positively Associated with Late-Life Subjective Cognitive Function in a Prospective Study in US Women. J. Nutr. 2020, 150, 1871–1879. [Google Scholar] [CrossRef]
- Gerger, P.; Pai, R.K.; Stuckenschneider, T.; Falkenreck, J.; Weigert, H.; Stahl, W.; Weber, B.; Nelles, G.; Spazzafumo, L.; Schneider, S.; et al. Associations of lipophilic micronutrients with physical and cognitive fitness in persons with mild cognitive impairment. Nutrients 2019, 11, 902. [Google Scholar] [CrossRef]
- Li, Y.; Liu, S.; Man, Y.; Li, N.; Zhou, Y. Effects of vitamins E and C combined with β carotene on cognitive function in the elderly. Exp. Ther. Med. 2015, 9, 1489–1493. [Google Scholar] [CrossRef] [PubMed]
- Nooyens, A.C.J.; Milder, I.E.J.; Van Gelder, B.M.; Bueno-De-Mesquita, H.B.; Van Boxtel, M.P.J.; Verschuren, W.M.M. Diet and cognitive decline at middle age: The role of antioxidants. Br. J. Nutr. 2015, 113, 1410–1417. [Google Scholar] [CrossRef] [PubMed]
- Johnson, E.J.; Vishwanathan, R.; Johnson, M.A.; Hausman, D.B.; Davey, A.; Scott, T.M.; Poon, L.W. Relationship between serum and brain carotenoids, α -tocopherol, and retinol concentrations and cognitive performance in the oldest old from the georgia centenarian study. J. Aging Res. 2013, 2013, 951786. Available online: http://www.embase.com/search/results?subaction=viewrecord&from=export&id=L369322094%0A (accessed on 9 July 2023). [CrossRef] [PubMed]
- Akbaraly, N.T.; Faure, H.; Gourlet, V.; Favier, A.; Berr, C. Plasma carotenoid levels and cognitive performance in an elderly population: Results of the EVA study. Cereb. Cortex 2014, 24, 308–316. [Google Scholar] [CrossRef]
- Kesse-Guyot, E.; Fezeu, L.; Jeandel, C.; Ferry, M.; Andreeva, V.; Amieva, H.; Galan, P. French adults’ cognitive performance after daily supplementation with antioxidant vitamins and minerals at nutritional doses: A post hoc analysis of the supplementation in vitamins and mineral antioxidants (SU.VI.MAX) trial. Am. J. Clin. Nutr. 2011, 94, 892–899. [Google Scholar] [CrossRef]
- Péneau, S.; Galan, P.; Jeandel, C.; Ferry, M.; Andreeva, V.; Hercberg, S.; Kesse-Guyot, E. Fruit and vegetable intake and cognitive function in the SU.VI.MAX 2 prospective study. Am. J. Clin. Nutr. 2011, 94, 1295–1303. [Google Scholar] [CrossRef] [PubMed]
- Smith, A.P.; Clark, R.E.; Nutt, D.J.; Haller, J.; Hayward, S.G.; Perry, K. Vitamin C, Mood and Cognitive Functioning in the Elderly. Nutr. Neurosci. 1999, 2, 249–256. [Google Scholar] [CrossRef] [PubMed]
- Grodstein, F.; Kang, J.H.; Glynn, R.J.; Cook, N.R.; Gaziano, J.M. A randomized trial of beta carotene supplementation and cognitive function in men: The physicians’ health study II. Arch. Intern. Med. 2007, 167, 2184–2190. [Google Scholar] [CrossRef]
- Wolters, M.; Hickstein, M.; Flintermann, A.; Tewes, U.; Hahn, A. Cognitive performance in relation to vitamin status in healthy elderly German women—The effect of 6-month multivitamin supplementation. Prev. Med. 2005, 41, 253–259. [Google Scholar] [CrossRef]
- Kang, J.H.; Cook, N.R.; Manson, J.E.; Buring, J.E.; Albert, C.M.; Grodstein, F. Vitamin E, Vitamin C, Beta carotene, and cognitive function among women with or at risk of cardiovascular disease: The women’s antioxidant and cardiovascular study. Circulation 2009, 119, 2772–2780. [Google Scholar] [CrossRef]
- Perkins, A.J.; Hendrie, H.C.; Callahan, C.M.; Gao, S.; Unverzagt, F.W.; Xu, Y.; Hall, K.S.; Hui, S.L. Association of antioxidants with memory in a multiethnic elderly sample using the Third National Health and Nutrition Examination survey. Am. J. Epidemiol. 1999, 150, 37–44. [Google Scholar] [CrossRef] [PubMed]
- NIH. Quality Assessment Tool for Observational Cohort and Cross-Sectional Studies—National Institutes of Health. Available online: https://www.nhlbi.nih.gov/health-pro/guidelines/in-develop/cardiovascular-risk-reduction/tools/cohort (accessed on 9 July 2023).
- Bohn, T.; Mcdougall, G.J.; Alegría, A.; Alminger, M.; Arrigoni, E.; Aura, A.-M.; Brito, C.; Cilla, A.; El, S.N.; Karakaya, S.; et al. Mind the gap-deficits in our knowledge of aspects impacting the bioavailability of phytochemicals and their metabolites-a position paper focusing on carotenoids and polyphenols. Mol. Nutr. Food Res. 2015, 59, 1307–1323. [Google Scholar] [CrossRef] [PubMed]
- Bohn, T.; Desmarchelier, C.; Dragsted, L.O.; Nielsen, C.S.; Stahl, W.; Rühl, R.; Keijer, J.; Borel, P. Host-related factors explaining interindividual variability of carotenoid bioavailability and tissue concentrations in humans. Mol. Nutr. Food Res. 2017, 61, 1600685. [Google Scholar] [CrossRef] [PubMed]
- Plassman, B.L.; Langa, K.M.; Fischer, G.G.; Heeringa, S.G.; Weir, D.R.; Ofstedal, M.B.; Burke, J.R.; Hurd, M.D.; Potter, G.G.; Rodgers, W.L.; et al. Prevalence of Dementia in the United States: The Aging, demographics, and memory study. Neuroepidemiology 2007, 29, 125–132. [Google Scholar] [CrossRef] [PubMed]
- Fillenbaum, G.G.; van Belle, G.; Morris, J.C.; Mohs, R.C.; Mirra, S.S.; Davis, P.C.; Tariot, P.N.; Silverman, J.M.; Clark, C.M.; Welsh-Bohmer, K.A.; et al. Consortium to Establish a Registry for Alzheimer’s Disease (CERAD): The first twenty years. Alzheimer’s Dement. 2008, 4, 96–109. [Google Scholar] [CrossRef] [PubMed]
- Bacchetti, T.; Turco, I.; Urbano, A.; Morresi, C.; Ferretti, G. Relationship of fruit and vegetable intake to dietary antioxidant capacity and markers of oxidative stress: A sex-related study. Nutrition 2019, 61, 164–172. [Google Scholar] [CrossRef] [PubMed]
- Maruff, P.; Thompson, T.A.C.; Wilson, P.H.; Snyder, P.J.; Pietrzak, R.H.; Darby, D.; Buschke, H. Sensitivity and Test-Retest Reliability of the International Shopping List Test in Assessing Verbal Learning and Memory in Mild Alzheimer’s Disease. Arch. Clin. Neuropsychol. 2011, 26, 412–424. [Google Scholar]
- Jama, J.W.; Launer, L.J.; Witteman, J.C.M.; Den Breeijen, J.H.; Breteler, M.M.B.; Grobbee, D.E.; Hofman, A. Dietary antioxidants and cognitive function in a population-based sample of older persons: The Rotterdam Study. Am. J. Epidemiol. 1996, 144, 275–280. Available online: https://login.pallas2.tcl.sc.edu/login?url=http://search.ebscohost.com/login.aspx?direct=true&db=ccm&AN=107147513&site=ehost-live (accessed on 9 July 2023). [CrossRef]
- Chen, L.; Yoo, S.E.; Na, R.; Liu, Y.; Ran, Q. Cognitive impairment and increased Aβ levels induced by paraquat exposure are attenuated by enhanced removal of mitochondrial H2O2. Neurobiol. Aging 2012, 33, e15–e432. [Google Scholar] [CrossRef]
- Marcelino, G.; Machate, D.J.; Freitas, K.d.C.; Hiane, P.A.; Maldonade, I.R.; Pott, A.; Asato, M.A.; Candido, C.J.; Guimarães, R.D.C.A. β-Carotene: Preventive Role for Type 2 Diabetes Mellitus and Obesity: A Review. Molecules 2020, 25, 5803. [Google Scholar] [CrossRef]
- Rondanelli, M.; Faliva, M.; Peroni, G.; Moncaglieri, F.; Infantino, V.; Naso, M.; Perna, S. Focus on Pivotal Role of Dietary Intake (Diet and Supplement) and Blood Levels of Tocopherols and Tocotrienols in Obtaining Successful Aging. Int. J. Mol. Sci. 2015, 16, 23227–23249. [Google Scholar] [CrossRef] [PubMed]
- Fiedor, J.; Burda, K. Potential Role of Carotenoids as Antioxidants in Human Health and Disease. Nutrients 2014, 6, 466–488. [Google Scholar] [CrossRef] [PubMed]
- Chen, J.; Li, F.; Li, Z.; McClements, D.J.; Xiao, H. Encapsulation of carotenoids in emulsion-based delivery systems: Enhancement of β-carotene water-dispersibility and chemical stability. Food Hydrocoll. 2017, 69, 49–55. [Google Scholar] [CrossRef]
- Hix, L.M.; Lockwood, S.F.; Bertram, J.S. Bioactive carotenoids: Potent antioxidants and regulators of gene expression. Redox Rep. 2004, 9, 181–191. [Google Scholar] [CrossRef] [PubMed]
- Naz, H.; Islam, A.; Ahmad, F.; Hassan, M.I. Calcium/calmodulin-dependent protein kinase IV: A multifunctional enzyme and potential therapeutic target. Prog. Biophys. Mol. Biol. 2016, 121, 54–65. [Google Scholar] [CrossRef] [PubMed]
- Naz, H.; Khan, P.; Tarique, M.; Rahman, S.; Meena, A.; Ahamad, S.; Luqman, S.; Islam, A.; Ahmad, F.; Hassan, M.I. Binding studies and biological evaluation of β-carotene as a potential inhibitor of human calcium/calmodulin-dependent protein kinase IV. Int. J. Biol. Macromol. 2017, 96, 161–170. [Google Scholar] [CrossRef] [PubMed]
- Silalahi, J. Anticancer and health protective properties of citrus fruit components. Asia Pac. J. Clin. Nutr. 2002, 11, 79–84. [Google Scholar] [CrossRef] [PubMed]
- Kim, N.R.; Kim, H.Y.; Kim, M.H.; Kim, H.M.; Jeong, H.J. Improvement of depressive behavior by Sweetme Sweet PumpkinTM and its active compound, β-carotene. Life Sci. 2016, 147, 39–45. [Google Scholar] [CrossRef]
- Lu, B.; Nagappan, G.; Lu, Y. BDNF and Synaptic Plasticity, Cognitive Function, and Dysfunction. Neurotrophic Factors 2014, 220, 223–250. [Google Scholar]
- Miranda, M.; Morici, J.F.; Zanoni, M.B.; Bekinschtein, P. Brain-Derived Neurotrophic Factor: A Key Molecule for Memory in the Healthy and the Pathological Brain. Front. Cell. Neurosci. 2019, 13, 363. [Google Scholar] [CrossRef]
- Wołoszynowska-Fraser, M.U.; Kouchmeshky, A.; McCaffery, P. Vitamin A and Retinoic Acid in Cognition and Cognitive Disease. Annu. Rev. Nutr. 2020, 40, 247–272. [Google Scholar] [CrossRef]
- Mishra, S.; Kelly, K.K.; Rumian, N.L.; Siegenthaler, J.A. Retinoic Acid Is Required for Neural Stem and Progenitor Cell Proliferation in the Adult Hippocampus. Stem Cell Rep. 2018, 10, 1705–1720. [Google Scholar] [CrossRef]
- Husson, M.; Enderlin, V.; Delacourte, A.; Ghenimi, N.; Alfos, S.; Pallet, V.; Higueret, P. Retinoic acid normalizes nuclear receptor mediated hypo-expression of proteins involved in β-amyloid deposits in the cerebral cortex of vitamin A deprived rats. Neurobiol. Dis. 2006, 23, 1–10. [Google Scholar] [CrossRef]
- Hu, P.; Bretsky, P.; Crimmins, E.M.; Guralnik, J.M.; Reuben, D.B.; Seeman, T.E. Association between serum beta-carotene levels and decline of cognitive function in high-functioning older persons with or without apolipoprotein E 4 alleles: MacArthur studies of successful aging. J. Gerontol.—Ser. A Biol. Sci. Med. Sci. 2006, 61, 616–620. [Google Scholar] [CrossRef]





| Study | Methods | Results | Reference |
|---|---|---|---|
| Zhong et al. (2023) | Dietary intake | Q1 of BC vs. Q4 had lower risks of both CERAD WL decline [odds ratio (OR) = 0.63, 95% confidence interval (CI): 0.44–0.90] and AFT decline (OR = 0.66, 95% CI: 0.47–0.94). Q3 of BC dietary intake had a significantly decreased risk of lower DSST scores (OR = 0.67, 95% CI: 0.48–0.83). For males, dietary BC intake was associated with a decreased risk of AFT decline (OR = 0.51, 95% CI: 0.30–0.85). For females, dietary BC intake was associated with decreased risks of CERAD WL and AFT decline (OR = 0.37, 95% CI: 0.21–0.64; OR = 0.58, 95% CI: 0.37–0.91, respectively) | [29] |
| Yuan et al. (2020) | Dietary intake | Long-term intakes of total BC and dietary BC were each associated with lower odds of moderate and poor SCF (OR = 0.77 in Q5; p < 0.001) | [31] |
| Beydoun et al. (2020) | Dietary intake | BC intake was associated with a faster decline and poorer performance on the CDT | [30] |
| Gerger et al. (2019) | Serum levels | Positive correlation of BC serum concentration with verbal memory assessed through the ISLT (p < 0.01) | [32] |
| Nooyens et al. (2015) | Dietary intake | No association between BC intake and cognitive decline | [34] |
| Johnson et al. (2013) | Serum levels | BC serum concentrations positively correlated with most measures of better cognitive function (p < 0.05) | [35] |
| Péneau et al. (2011) | Dietary intake of BC-rich FVs | The intake of BC-rich FVs was negatively associated with executive functioning scores (p = 0.02) | [38] |
| Akbaraly et al. (2007) | Serum levels | No associations were found between lower BC serum levels and cognitive impairment | [36] |
| Perkins et al. (1999) | Serum levels | Decreasing serum levels of BC were not associated with poor memory performance | [43] |
| Perrig et al. (1997) | Serum levels | BC serum concentration (β0.106, p = 0.035) remained a significant predictor of semantic memory performance | [28] |
| Study | Supplementation | Results | Reference |
|---|---|---|---|
| Li et al. (2015) | Daily VE (200 mg) and VC (300 mg) combined with BC at 16.7 (group A), 8.4 (group B), 5.6 (group C), or 0 mg/day (group D) or VE alone (5 mg) (group E) for 16 weeks | MMSE scores in A and B were 23.49 ± 4.40 and 23.44 ± 3.62, respectively, significantly higher compared to E (22.32 ± 4.23; p < 0.05). HDS scores in A and B were 22.46 ± 4.96 and 21.38 ± 3.97, respectively, significantly higher than the corresponding scores prior to the treatment (18.68 ± 5.77 for A and 19.75 ± 5.46 for B; p < 0.05). HDS scores in A and B (22.46 ± 4.96 and 21.38 ± 3.97; p < 0.05) were significantly higher compared to E (18.87 ± 4.70; p < 0.05). | [33] |
| Kesse-Guyot et al. (2011) | Daily VC (120 mg), BC (6 mg), VE (30 mg), selenium (100 μg), and zinc (20 mg) in combination or placebo for 8 y | Subjects receiving active antioxidant supplementation had better episodic memory scores (mean difference: 0.61; 95% CI: 0.02, 1.20). | [37] |
| Kang et al. (2009) | BC (50 mg) every other day or placebo, either alone or combined with VE every other day (402 mg), VC daily (500 mg), or both, for 3.5 y | They found that BC supplements were beneficial among those with low dietary intakes of total carotenoids but not among those with higher intakes (p for interaction = 0.02). | [42] |
| Grodstein et al. (2007) | BC 50 mg every other day for 18 y | Improvement in global cognitive score (p = 0.03), verbal memory (p = 0.007), and TICS score (p = 0.04). | [40] |
| Wolters et al. (2005) | Multivitamin capsule (9 mg/d BC) for 6 months | No effect on cognitive performance. | [41] |
| Smith et al. (1999) | 12 mg/d BC, 400 mg/d VE, and 500 mg/d VC in combination or placebo for 1 y | There were very few significant differences between the placebo and multivitamin groups. | [39] |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Abrego-Guandique, D.M.; Bonet, M.L.; Caroleo, M.C.; Cannataro, R.; Tucci, P.; Ribot, J.; Cione, E. The Effect of Beta-Carotene on Cognitive Function: A Systematic Review. Brain Sci. 2023, 13, 1468. https://doi.org/10.3390/brainsci13101468
Abrego-Guandique DM, Bonet ML, Caroleo MC, Cannataro R, Tucci P, Ribot J, Cione E. The Effect of Beta-Carotene on Cognitive Function: A Systematic Review. Brain Sciences. 2023; 13(10):1468. https://doi.org/10.3390/brainsci13101468
Chicago/Turabian StyleAbrego-Guandique, Diana Marisol, Maria Luisa Bonet, Maria Cristina Caroleo, Roberto Cannataro, Paola Tucci, Joan Ribot, and Erika Cione. 2023. "The Effect of Beta-Carotene on Cognitive Function: A Systematic Review" Brain Sciences 13, no. 10: 1468. https://doi.org/10.3390/brainsci13101468