
Early Hemorrhagic Transformation after Reperfusion Therapy in Patients with Acute Ischemic Stroke: Analysis of Risk Factors and Predictors
 ,
,  and
and
Abstract
:1. Introduction
2. Material and Methods
2.1. Study Population, Inclusion, and Exclusion Criteria
2.2. Evaluation of Stroke
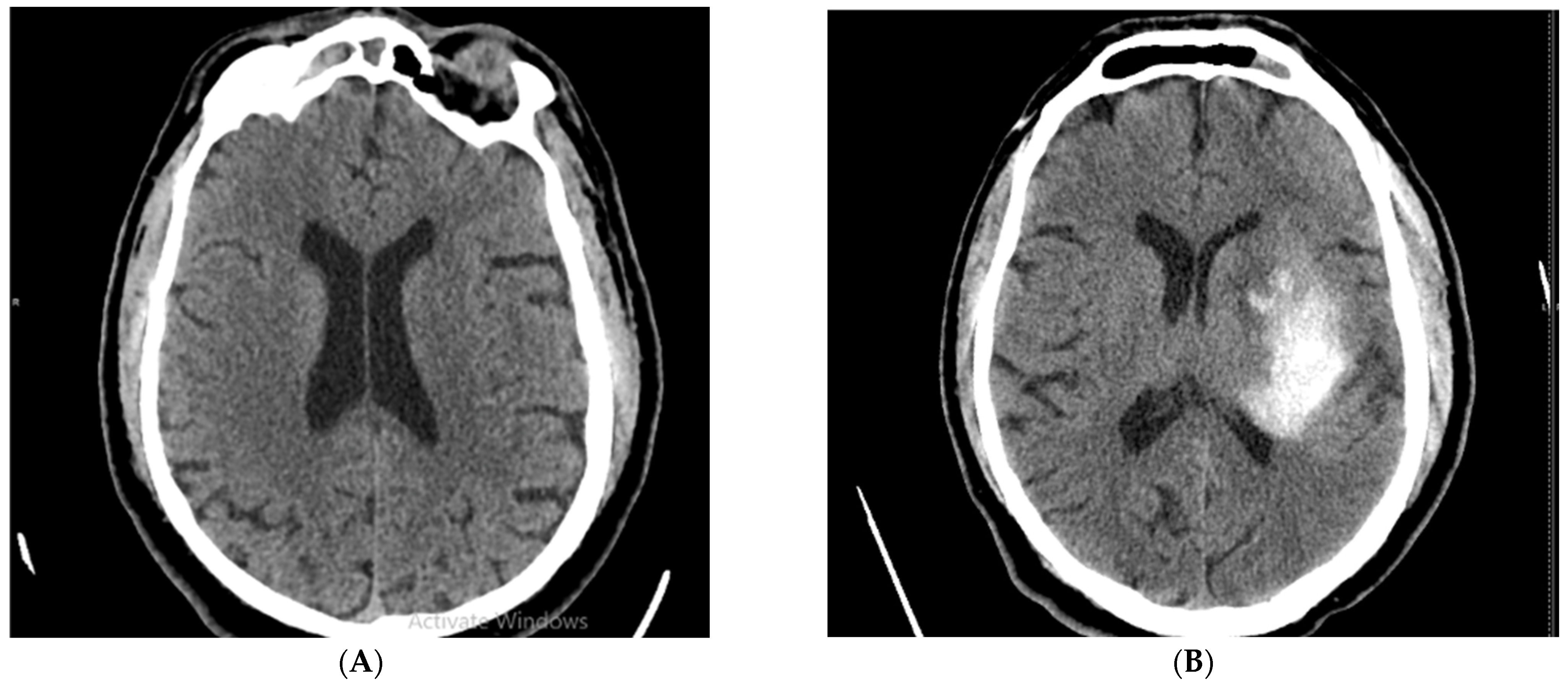
2.3. Evaluation of Hemorrhagic Transformation
2.4. Reperfusion Therapy Protocol
2.5. Stroke Risk Factors
2.6. Statistical Analysis
3. Results
3.1. Incidence of Hemorrhagic Transformation
3.2. Patient Population and Characteristics
3.3. Analysis of Correlations between Stroke Scores and Early HT
3.4. Analysis of Correlations between Type of Reperfusion Therapy and Early HT
3.5. Logistic Regression of Independent Risk Factors Associated with Early HT
3.6. Analysis of Independent of Stroke Scores between Groups
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Katan, M.; Luft, A. Global Burden of Stroke. Semin. Neurol. 2018, 38, 208–211. [Google Scholar] [CrossRef] [PubMed]
- Donkor, E.S. Stroke in the century: A snapshot of the burden, epidemiology, and quality of life. Stroke Res. Treat. 2018, 2018, 3238165. [Google Scholar] [PubMed]
- Stroke Alliance for Europe. The Burden of Stroke in Europe—Challenges for Policy Makers. Available online: https://www.stroke.org.uk/sites/default/files/the_burden_of_stroke_in_europe_-_challenges_for_policy_makers.pdf (accessed on 14 January 2022).
- Cruz-Flores, S. Acute Stroke and Transient Ischemic Attack in the Outpatient Clinic. Med. Clin. N. Am. 2017, 101, 479–494. [Google Scholar] [CrossRef] [PubMed]
- Hachinski, V.; Donnan, G.A.; Gorelick, P.B.; Hacke, W.; Cramer, S.C.; Kaste, M.; Fisher, M.; Brainin, M.; Buchan, A.M.; Lo, E.H.; et al. Stroke: Working toward a prioritized world agenda. Int. J. Stroke 2010, 5, 238–256. [Google Scholar] [CrossRef] [PubMed]
- Uivarosan, D.; Bungau, S.; Tit, D.M.; Moisa, C.; Fratila, O.; Rus, M.; Bratu, O.G.; Diaconu, C.C.; Pantis, C. Financial Burden of Stroke Reflected in a Pilot Center for the Implementation of Thrombolysis. Medicina 2020, 56, 54. [Google Scholar] [CrossRef]
- Spronk, E.; Sykes, G.; Falcione, S.; Munsterman, D.; Joy, T.; Kamtchum-Tatuene, J.; Jickling, G.C. Hemorrhagic Transformation in Ischemic Stroke and the Role of Inflammation. Front. Neurol. 2021, 12, 661955. [Google Scholar] [CrossRef]
- Herpich, F.; Rincon, F. Management of Acute Ischemic Stroke. Crit. Care Med. 2020, 48, 1654–1663. [Google Scholar] [CrossRef]
- Jaillard, A.; Cornu, C.; Durieux, A.; Moulin, T.; Boutitie, F.; Lees, K.R.; Hommel, M. Hemorrhagic transformation in acute ischemic stroke: The MAST-E study. Stroke 1999, 30, 1326–1332. [Google Scholar] [CrossRef]
- Bang, O.Y.; Saver, J.L.; Kim, S.J.; Kim, G.-M.; Chung, C.-S.; Ovbiagele, B.; Lee, K.H.; Liebeskind, D.S.; Collaborators, U.-S.S. Collateral flow averts hemorrhagic transformation after endovascular therapy for acute ischemic stroke. Stroke 2011, 42, 2235–2239. [Google Scholar] [CrossRef]
- Gomez, C.R.; Schneck, M.J.; Biller, J. Recent advances in the management of transient ischemic attacks. F1000Research 2017, 6, 1893. [Google Scholar] [CrossRef]
- Muscari, A.; Faccioli, L.; Lega, M.V.; Lorusso, A.; Masetti, M.; Pastore Trossello, M.; Puddu, G.M.; Spinardi, L.; Zoli, M. Predicting hemorrhagic transformation and its timing from maximum cerebral lesion diameter in nonlacunar ischemic strokes. Brain Behav. 2020, 10, e01497. [Google Scholar] [CrossRef] [PubMed]
- Jickling, G.C.; Liu, D.; Stamova, B.; Ander, B.P.; Zhan, X.; Lu, A.; Sharp, F.R. Hemorrhagic Transformation after Ischemic Stroke in Animals and Humans. J. Cereb. Blood Flow Metab. 2014, 34, 185–199. [Google Scholar] [CrossRef] [PubMed]
- Boehme, A.K.; Esenwa, C.; Elkind, M.S.V. Stroke Risk Factors, Genetics, and Prevention. Circ. Res. 2017, 120, 472–495. [Google Scholar] [CrossRef] [PubMed]
- Thomas, S.E.; Plumber, N.; Venkatapathappa, P.; Gorantla, V. A Review of Risk Factors and Predictors for Hemorrhagic Transformation in Patients with Acute Ischemic Stroke. Int. J. Vasc. Med. 2021, 2021, 4244267. [Google Scholar] [CrossRef]
- Khanevski, A.N.; Bjerkreim, A.T.; Novotny, V.; Næss, H.; Thomassen, L.; Logallo, N.; Kvistad, C.E. Recurrent ischemic stroke: Incidence, predictors, and impact on mortality. Acta Neurol. Scand. 2019, 140, 3–8. [Google Scholar] [CrossRef]
- Liu, Z.; Lin, W.; Lu, Q.; Wang, J.; Liu, P.; Lin, X.; Wang, F.; Shi, Y.; Wang, Q.; Liu, G.; et al. Risk factors affecting the 1-year outcomes of minor ischemic stroke: Results from Xi’an stroke registry study of China. BMC Neurol. 2020, 20, 379. [Google Scholar] [CrossRef]
- János Marcell László, T.H. Hemorrhagic transformation of ischemic stroke. Vasc. Dis. Ther. 2017, 2, 1–25. [Google Scholar]
- Molina, C.A.; Montaner, J.; Abilleira, S.; Ibarra, B.; Romero, F.; Arenillas, J.F.; Alvarez-Sabín, J. Timing of spontaneous recanalization and risk of hemorrhagic transformation in acute cardioembolic stroke. Stroke 2001, 32, 1079–1084. [Google Scholar] [CrossRef]
- Pande, S.; Win, M.; Khine, A.; Zaw, E.; Manoharraj, N.; Lolong, L.; Tin, A. Haemorrhagic transformation following ischaemic stroke: A retrospective study. Sci. Rep. 2020, 10, 5319. [Google Scholar] [CrossRef]
- Mazya, M.; Egido, J.A.; Ford, G.A.; Lees, K.R.; Mikulik, R.; Toni, D.; Wahlgren, N.; Ahmed, N. Predicting the risk of symptomatic intracerebral hemorrhage in ischemic stroke treated with intravenous alteplase: Safe Implementation of Treatments in Stroke (SITS) symptomatic intracerebral hemorrhage risk score. Stroke 2012, 43, 1524–1531. [Google Scholar] [CrossRef]
- Liu, K.; Yan, S.; Zhang, S.; Guo, Y.; Lou, M. Systolic blood pressure variability is associated with severe hemorrhagic transformation in the early stage after thrombolysis. Transl. Stroke Res. 2016, 7, 186–191. [Google Scholar] [CrossRef] [PubMed]
- Tu, H.T.H.; Campbell, B.C.V.; Christensen, S.; Desmond, P.M.; De Silva, D.A.; Parsons, M.W.; Churilov, L.; Lansberg, M.G.; Mlynash, M.; Olivot, J.-M.; et al. Worse Stroke Outcome in Atrial Fibrillation is Explained by More Severe Hypoperfusion, Infarct Growth, and Hemorrhagic Transformation. Int. J. Stroke 2013, 10, 534–540. [Google Scholar] [CrossRef] [PubMed]
- Afzal, B.; Ali, S.A.; Jamil, B. Association Between Raised HbA1c Levels and Hemorrhagic Transformation in Patients With Ischemic Stroke. Cureus 2021, 13, e19935. [Google Scholar] [CrossRef] [PubMed]
- Powers, W.J.; Rabinstein, A.A.; Ackerson, T.; Adeoye, O.M.; Bambakidis, N.C.; Becker, K.; Biller, J.; Brown, M.; Demaerschalk, B.M.; Hoh, B. 2018 guidelines for the early management of patients with acute ischemic stroke: A guideline for healthcare professionals from the American Heart Association/American Stroke Association. Stroke 2018, 49, e46–e99. [Google Scholar] [CrossRef]
- Sabau, M.; Bungau, S.; Buhas, C.L.; Carp, G.; Daina, L.-G.; Judea-Pusta, C.T.; Buhas, B.A.; Jurca, C.M.; Daina, C.M.; Tit, D.M. Legal medicine implications in fibrinolytic therapy of acute ischemic stroke. BMC Med. Ethics 2019, 20, 70. [Google Scholar] [CrossRef]
- Aho, K.; Harmsen, P.; Hatano, S.; Marquardsen, J.; Smirnov, V.E.; Strasser, T. Cerebrovascular disease in the community: Results of a WHO collaborative study. Bull. World Health Organ. 1980, 58, 113. [Google Scholar]
- Sacco, R.L.; Kasner, S.E.; Broderick, J.P.; Caplan, L.R.; Connors, J.J.; Culebras, A.; Elkind, M.S.V.; George, M.G.; Hamdan, A.D.; Higashida, R.T.; et al. An Updated Definition of Stroke for the 21st Century. Stroke 2013, 44, 2064–2089. [Google Scholar] [CrossRef]
- Fiorelli, M.; Bastianello, S.; von Kummer, R.; del Zoppo, G.J.; Larrue, V.; Lesaffre, E.; Ringleb, A.P.; Lorenzano, S.; Manelfe, C.; Bozzao, L. Hemorrhagic transformation within 36 hours of a cerebral infarct: Relationships with early clinical deterioration and 3-month outcome in the European Cooperative Acute Stroke Study I (ECASS I) cohort. Stroke 1999, 30, 2280–2284. [Google Scholar] [CrossRef]
- Montaner, J.; Alvarez-Sabin, J.; Molina, C.; Angles, A.; Abilleira, S.; Arenillas, J.; Monasterio, J. Matrix metalloproteinase expression is related to hemorrhagic transformation after cardioembolic stroke. Stroke 2001, 32, 2762–2767. [Google Scholar] [CrossRef]
- Goldstein, L.B.; Bertels, C.; Davis, J.N. Interrater reliability of the NIH stroke scale. Arch. Neurol. 1989, 46, 660–662. [Google Scholar] [CrossRef]
- Hacke, W.; Kaste, M.; Bluhmki, E.; Brozman, M.; Dávalos, A.; Guidetti, D.; Larrue, V.; Lees, K.R.; Medeghri, Z.; Machnig, T.; et al. Thrombolysis with alteplase 3 to 4.5 hours after acute ischemic stroke. N. Engl. J. Med. 2008, 359, 1317–1329. [Google Scholar] [CrossRef] [PubMed]
- Barber, P.A.; Demchuk, A.M.; Zhang, J.; Buchan, A.M. Validity and reliability of a quantitative computed tomography score in predicting outcome of hyperacute stroke before thrombolytic therapy. ASPECTS Study Group. Alberta Stroke Programme Early CT Score. Lancet 2000, 355, 1670–1674. [Google Scholar] [CrossRef] [PubMed]
- Liu, J.; Wang, Y.; Li, J.; Zhang, S.; Wu, Q.; Wei, C.; Cui, T.; Wu, B.; Willey, J.Z.; Liu, M. Treatment and Outcomes of Thrombolysis Related Hemorrhagic Transformation: A Multi-Center Study in China. Front. Aging Neurosci. 2022, 14, 319. [Google Scholar] [CrossRef] [PubMed]
- Liu, J.; Wang, Y.; Jin, Y.; Guo, W.; Song, Q.; Wei, C.; Li, J.; Zhang, S.; Liu, M. Prediction of Hemorrhagic Transformation After Ischemic Stroke: Development and Validation Study of a Novel Multi-biomarker Model. Front. Aging Neurosci. 2021, 13, 667934. [Google Scholar] [CrossRef]
- Erdoğan, H.A.; Acır, İ.; Yayla, V. Endovascular treatment experience in acute ischemic stroke. J. Neurosci. Neurol. Disord. 2021, 5, 026–028. [Google Scholar]
- The NINDS t-PA Stroke Study Group. Intracerebral hemorrhage after intravenous t-PA therapy for ischemic stroke. Stroke 1997, 28, 2109–2118. [Google Scholar] [CrossRef]
- Kidwell, C.S.; Saver, J.L.; Carneado, J.; Sayre, J.; Starkman, S.; Duckwiler, G.; Gobin, Y.P.; Jahan, R.; Vespa, P.; Villablanca, J.P.; et al. Predictors of hemorrhagic transformation in patients receiving intra-arterial thrombolysis. Stroke 2002, 33, 717–724. [Google Scholar] [CrossRef]
- Luo, A.; Bandela, S.; Mozumder, A.; Lee, B. Predictors of Hemorrhagic Transformation After Mechanical Thrombectomy in Acute Ischemic Stroke (1644). Neurology 2021, 96 (Suppl. S15), 1644. [Google Scholar]
- Wen, L.; Zhang, S.; Wan, K.; Zhang, H.; Zhang, X. Risk factors of haemorrhagic transformation for acute ischaemic stroke in Chinese patients receiving intravenous thrombolysis: A meta-analysis. Medicine 2020, 99, e18995. [Google Scholar] [CrossRef]
- Hacke, W.; Kaste, M.; Fieschi, C.; Toni, D.; Lesaffre, E.; von Kummer, R.; Boysen, G.; Bluhmki, E.; Höxter, G.; Mahagne, M.H.; et al. Intravenous thrombolysis with recombinant tissue plasminogen activator for acute hemispheric stroke. The European Cooperative Acute Stroke Study (ECASS). JAMA 1995, 274, 1017–1025. [Google Scholar] [CrossRef]
- Demchuk, A.M.; Morgenstern, L.B.; Krieger, D.W.; Linda Chi, T.; Hu, W.; Wein, T.H.; Hardy, R.J.; Grotta, J.C.; Buchan, A.M. Serum glucose level and diabetes predict tissue plasminogen activator-related intracerebral hemorrhage in acute ischemic stroke. Stroke 1999, 30, 34–39. [Google Scholar] [CrossRef] [PubMed]
- Jurcau, A.; Ardelean, A.I. Oxidative Stress in Ischemia/Reperfusion Injuries following Acute Ischemic Stroke. Biomedicines 2022, 10, 574. [Google Scholar] [CrossRef] [PubMed]
- Martini, S.R.; Kent, T.A. Hyperglycemia in acute ischemic stroke: A vascular perspective. J. Cereb. Blood Flow Metab. 2007, 27, 435–451. [Google Scholar] [CrossRef]
- Jauch, E.C.; Saver, J.L.; Adams, H.P., Jr.; Bruno, A.; Connors, J.J.; Demaerschalk, B.M.; Khatri, P.; McMullan, P.W., Jr.; Qureshi, A.I.; Rosenfield, K.; et al. Guidelines for the early management of patients with acute ischemic stroke: A guideline for healthcare professionals from the American Heart Association/American Stroke Association. Stroke 2013, 44, 870–947. [Google Scholar] [CrossRef]
- Yeo, L.L.; Paliwal, P.; Teoh, H.L.; Seet, R.C.; Chan, B.P.; Liang, S.; Venketasubramanian, N.; Rathakrishnan, R.; Ahmad, A.; Ng, K.W.; et al. Timing of recanalization after intravenous thrombolysis and functional outcomes after acute ischemic stroke. JAMA Neurol 2013, 70, 353–358. [Google Scholar] [CrossRef] [PubMed]
- Chang, X.; Zhang, X.; Zhang, G. Different Scores Predict the Value of Hemorrhagic Transformation after Intravenous Thrombolysis in Patients with Acute Ischemic Stroke. Evid.-Based Complement. Altern. Med. 2021, 2021, 2468052. [Google Scholar] [CrossRef]
- Shen, Z.; Jin, H.; Lu, Y.; Sun, W.; Liu, R.; Li, F.; Shu, J.; Tai, L.; Li, G.; Chen, H.; et al. Predictors and Prognosis of Symptomatic Intracranial Hemorrhage in Acute Ischemic Stroke Patients Without Thrombolysis: Analysis of Data From the Chinese Acute Ischemic Stroke Treatment Outcome Registry. Front. Neurol. 2021, 12, 727304. [Google Scholar] [CrossRef]
- Hoinoiu, B.; Jiga, L.P.; Nistor, A.; Dornean, V.; Barac, S.; Miclaus, G.; Ionac, M.; Hoinoiu, T. Chronic Hindlimb Ischemia Assessment; Quantitative Evaluation Using Laser Doppler in a Rodent Model of Surgically Induced Peripheral Arterial Occlusion. Diagnostics 2019, 9, 139. [Google Scholar] [CrossRef]
- Akif Topcuoglu, M. Transcranial D oppler ultrasound in neurovascular diseases: Diagnostic and therapeutic aspects. J. Neurochem. 2012, 123, 39–51. [Google Scholar] [CrossRef]
- Caraba, A.; Babalic, F.C.; Iurciuc, S.; Iurciuc, M. The Utility of Major Salivary Gland Ultrasonographic Parameters in the Diagnosis of Sjögren Syndrome. Dis. Mrk. 2019, 2019, 1716848. [Google Scholar] [CrossRef]
- Yan, L.; Zhou, X.; Zheng, Y.; Luo, W.; Yang, J.; Zhou, Y.; He, Y. Research progress in ultrasound use for the diagnosis and treatment of cerebrovascular diseases. Clinics 2019, 74, e715. [Google Scholar] [CrossRef] [PubMed]
- Amzar, D.; Cotoi, L.; Sporea, I.; Timar, B.; Schiller, O.; Schiller, A.; Borlea, A.; Pop, N.G.; Stoian, D. Shear Wave Elastography in Patients with Primary and Secondary Hyperparathyroidism. J. Clin. Med. 2021, 10, 697. [Google Scholar] [CrossRef] [PubMed]
- Tsivgoulis, G.; Eggers, J.R.; Ribo, M.; Perren, F.; Saqqur, M.; Rubiera, M.; Sergentanis, T.N.; Vadikolias, K.; Larrue, V.; Molina, C.A. Safety and efficacy of ultrasound-enhanced thrombolysis: A comprehensive review and meta-analysis of randomized and nonrandomized studies. Stroke 2010, 41, 280–287. [Google Scholar] [CrossRef] [PubMed]
- Eggers, J.; Seidel, G.; Koch, B.; König, I.R. Sonothrombolysis in acute ischemic stroke for patients ineligible for rt-PA. Neurology 2005, 64, 1052–1054. [Google Scholar] [CrossRef]
- Hong, J.M.; Kim, D.S.; Kim, M. Hemorrhagic Transformation After Ischemic Stroke: Mechanisms and Management. Front. Neurol. 2021, 12, 703258. [Google Scholar] [CrossRef]
- Ruan, Y.; Yuan, C.; Liu, Y.; Zeng, Y.; Cheng, H.; Cheng, Q.; Chen, Y.; Huang, G.; He, W.; He, J. High fibrinogen-to-albumin ratio is associated with hemorrhagic transformation in acute ischemic stroke patients. Brain Behav. 2021, 11, e01855. [Google Scholar] [CrossRef] [PubMed]
- Latour, L.L.; Kang, D.W.; Ezzeddine, M.A.; Chalela, J.A.; Warach, S. Early blood–brain barrier disruption in human focal brain ischemia. Ann. Neurol. Off. J. Am. Neurol. Assoc. Child Neurol. Soc. 2004, 56, 468–477. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variables | Without Early HT n = 168 | Early HT n = 43 | p Value |
|---|---|---|---|
| Age, years | 68 (15) | 70 (15) | 0.843 M-W |
| Male sex, n (%) | 103 (61.3%) | 22 (51.2%) | 0.227 Chi2 |
| BMI, kg/m2 | 26.1 (5) | 27.5 (5.2) | 0.764 M-W |
| SBP, mmHg | 153.3 ± 22.83 | 152.4 ± 19.64 | 0.946 unpT |
| DBP, mmHg | 80 (20) | 80 (20) | 0.767 M-W |
| Hypertension, n (%) | 127 (75.6%) | 34 (79.1%) | 0.633 Chi2 |
| T2DM, n (%) | 79 (47.0%) | 25 (58.1%) | 0.193 Chi2 |
| Dyslipidemia, n (%) | 66 (39.3%) | 17 (39.5%) | 0.976 Chi2 |
| AF, n (%) | 48 (28.6%) | 16 (37.2%) | 0.272 Chi2 |
| Smoking, n (%) | 52 (31.0%) | 14 (32.6%) | 0.839 Chi2 |
| Alcohol, n (%) | 52 (31.0%) | 16 (37.2%) | 0.433 Chi2 |
| Platelets count (×109 /L) | 213 (81) | 229 (87) | 0.279 M-W |
| Hemoglobin (g/dL) | 14 (2) | 14 (2) | 0.527 M-W |
| Creatinine (mg/dL) | 1.0 ± 0.25 | 1 (0) | 0.098 M-W |
| TC, mg/dL | 183.5 ± 48.84 | 185.9 ± 39.60 | 0.699 unpT |
| Blood glucose (mg/dL) | 131.01 ± 46.04 | 154.35 ± 63.57 | 0.007 unpT |
| INR | 1.05 ± 0.15 | 1.04 ± 0.10 | 0.538 unpT |
| Variables | Without Early HT n = 168 | Early HT n = 43 | p Value |
|---|---|---|---|
| ASPECTS at admission | 10 (1) | 9 (2) | 0.045 M-W |
| ASPECTS at 24 h | 8 (2) | 6 (3) | <0.001 M-W |
| NIHSS at admission | 13 (9) | 14 (6) | <0.001 M-W |
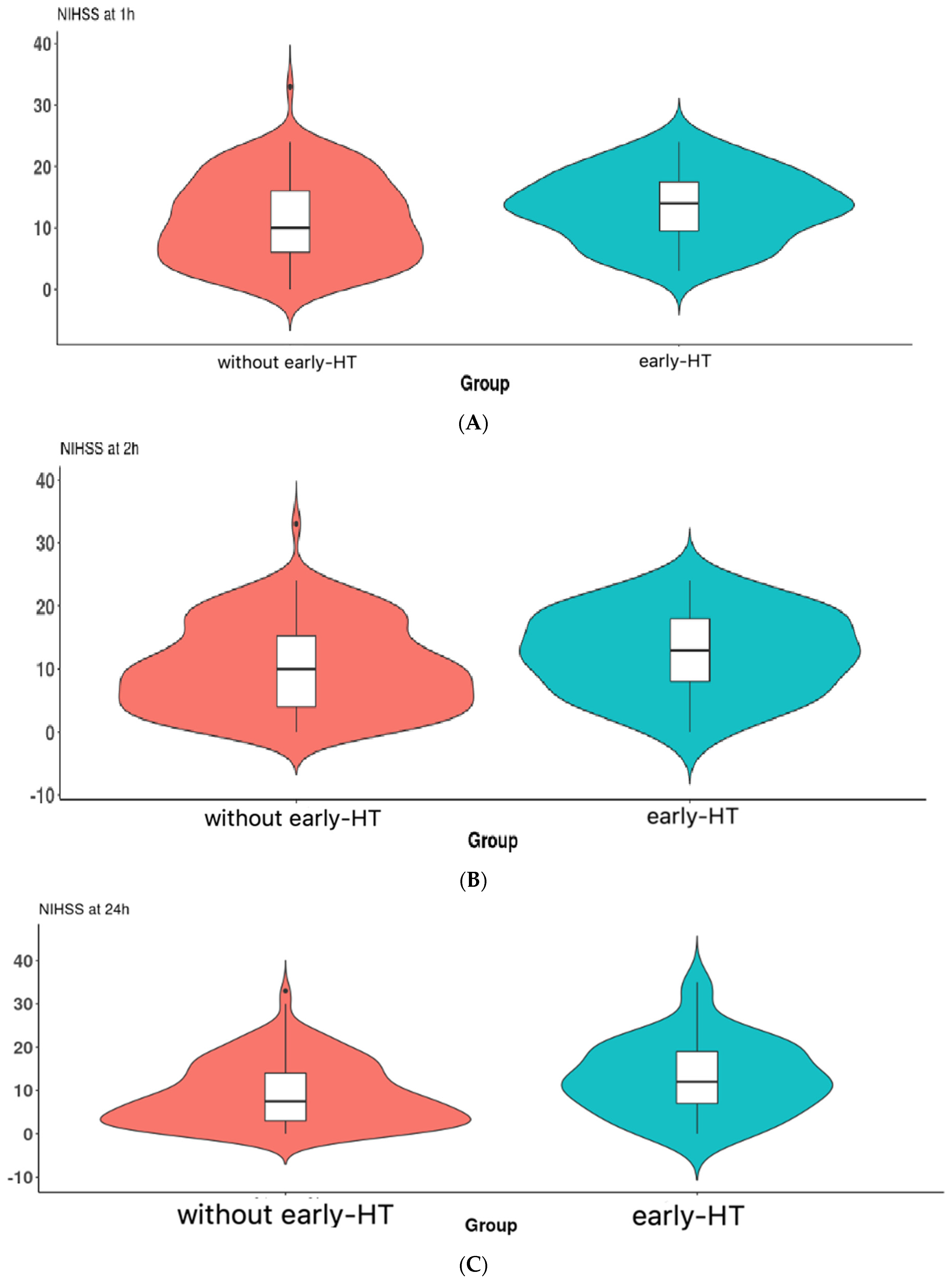
| NIHSS at 1 h | 13 (6) | 14 (8) | 0.040 M-W |
| NIHSS at 2 h | 11 (5) | 14 (11) | 0.032 M-W |
| NIHSS at 24 h | 8 (10) | 13 (11) | 0.007 M-W |
| Variables | Without Early HT n = 168 | Early HT n = 43 | p Value |
|---|---|---|---|
| Intravenous thrombolytic treatment (n = 192) | 157 (154.33) | 35 (37.67) | 0.089 |
| Endovascular treatment (n = 17) | 11 (13.67) | 6 (3.33) |
| Variable | p Values | Adjusted OR (95% CI) |
|---|---|---|
| Male sex (yes) | 0.035 | 2.736 (1.986–7.591) |
| Age, years | 0.294 | 1.022 (0.981–1.064) |
| BMI, kg /m2 | 0.911 | 1.006 (0.909–1.113) |
| Hypertension (yes) | 0.037 | 2.455 (1.481–4.403) |
| T2DM (yes) | 0.212 | 0.585 (0.252–1.357) |
| Dyslipidemia (yes) | 0.460 | 1.387 (0.582–3.310) |
| AF (yes) | 0.644 | 0.816 (0.346–1.929) |
| Smoking (yes) | 0.629 | 1.336 (0.412–4.331) |
| alcohol (yes) | 0.268 | 0.525 (0.168–1.641) |
| SBP, mmHg | 0.478 | 0.993 (0.972–1.013) |
| DBP, mmHg | 0.513 | 1.010 (0.980–1.042) |
| Platelets count (×109/L) | 0.327 | 1.003 (0.997–1.008) |
| Hemoglobin (g/dL) | 0.195 | 1.188 (0.916–1.541) |
| Blood glucose (mg/dL) | 0.042 | 1.207 (1.100–1.915) |
| TC, mg/dL | 0.868 | 1.001 (0.992–1.010) |
| Scores | p Value | Adjusted OR (95% CI) |
|---|---|---|
| ASPECTS at admission | 0.906 | 0.969 (0.575–1.632) |
| ASPECTS at 24 h | 0.016 | 0.601 (0.396–0.911) |
| NIHSS at admission | 0.945 | 0.090 (0.953–1.154) |
| NIHSS at 1 h | 0.927 | 1.007 (0.877–1.156) |
| NIHSS at 2 h | 0.936 | 0.994 (0.859–1.150) |
| NIHSS at 24 h | 0.027 | 1.186 (1.109–2.169) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Iancu, A.; Buleu, F.; Chita, D.S.; Tutelca, A.; Tudor, R.; Brad, S. Early Hemorrhagic Transformation after Reperfusion Therapy in Patients with Acute Ischemic Stroke: Analysis of Risk Factors and Predictors. Brain Sci. 2023, 13, 840. https://doi.org/10.3390/brainsci13050840
Iancu A, Buleu F, Chita DS, Tutelca A, Tudor R, Brad S. Early Hemorrhagic Transformation after Reperfusion Therapy in Patients with Acute Ischemic Stroke: Analysis of Risk Factors and Predictors. Brain Sciences. 2023; 13(5):840. https://doi.org/10.3390/brainsci13050840
Chicago/Turabian StyleIancu, Aida, Florina Buleu, Dana Simona Chita, Adrian Tutelca, Raluca Tudor, and Silviu Brad. 2023. "Early Hemorrhagic Transformation after Reperfusion Therapy in Patients with Acute Ischemic Stroke: Analysis of Risk Factors and Predictors" Brain Sciences 13, no. 5: 840. https://doi.org/10.3390/brainsci13050840