

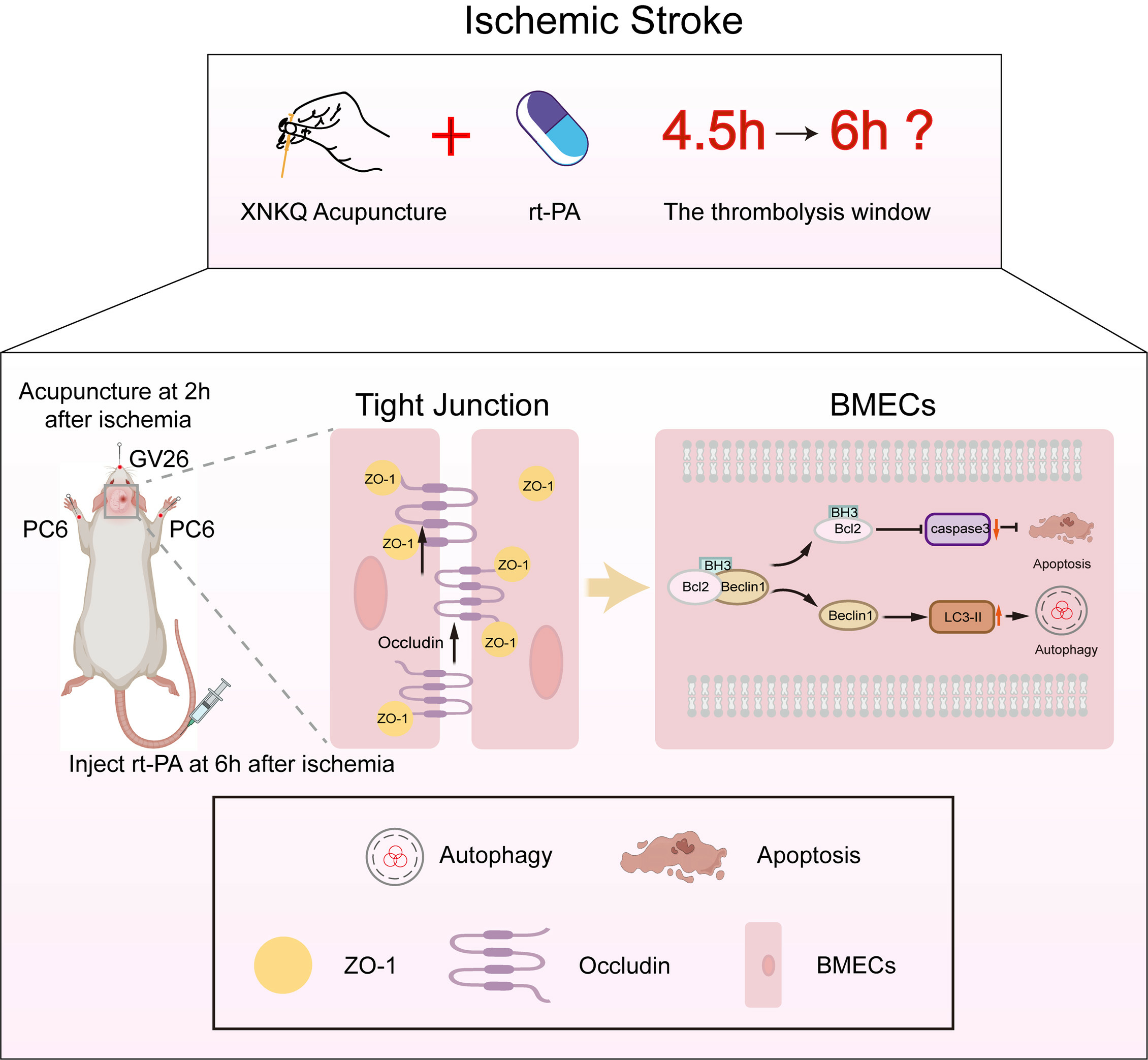
Acupuncture Extended the Thrombolysis Window by Suppressing Blood–Brain Barrier Disruption and Regulating Autophagy–Apoptosis Balance after Ischemic Stroke
Abstract
:
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
1. Introduction
2. Materials and Methods
2.1. Animals
2.2. Animal Grouping
2.3. The Embolic Stroke Model Establishment
2.4. Acupuncture Treatment
2.5. rt-PA Thrombolysis Treatment
2.6. Behavioral Testing
2.7. Measurement of Infarct Volume
2.8. Measurement of Hemorrhagic Transformation
2.9. Hematoxylin and Eosin Staining
2.10. TUNEL Staining
2.11. Measurement of Blood–Brain Barrier Permeability
2.12. Library Preparation, RNA Sequencing and Bioinformatic Analysis
2.13. Transmission Electron Microscopy
2.14. Western Blotting
2.15. Co-Immunoprecipitation
2.16. Immunofluorescence Staining
2.17. Statistical Analysis
3. Results
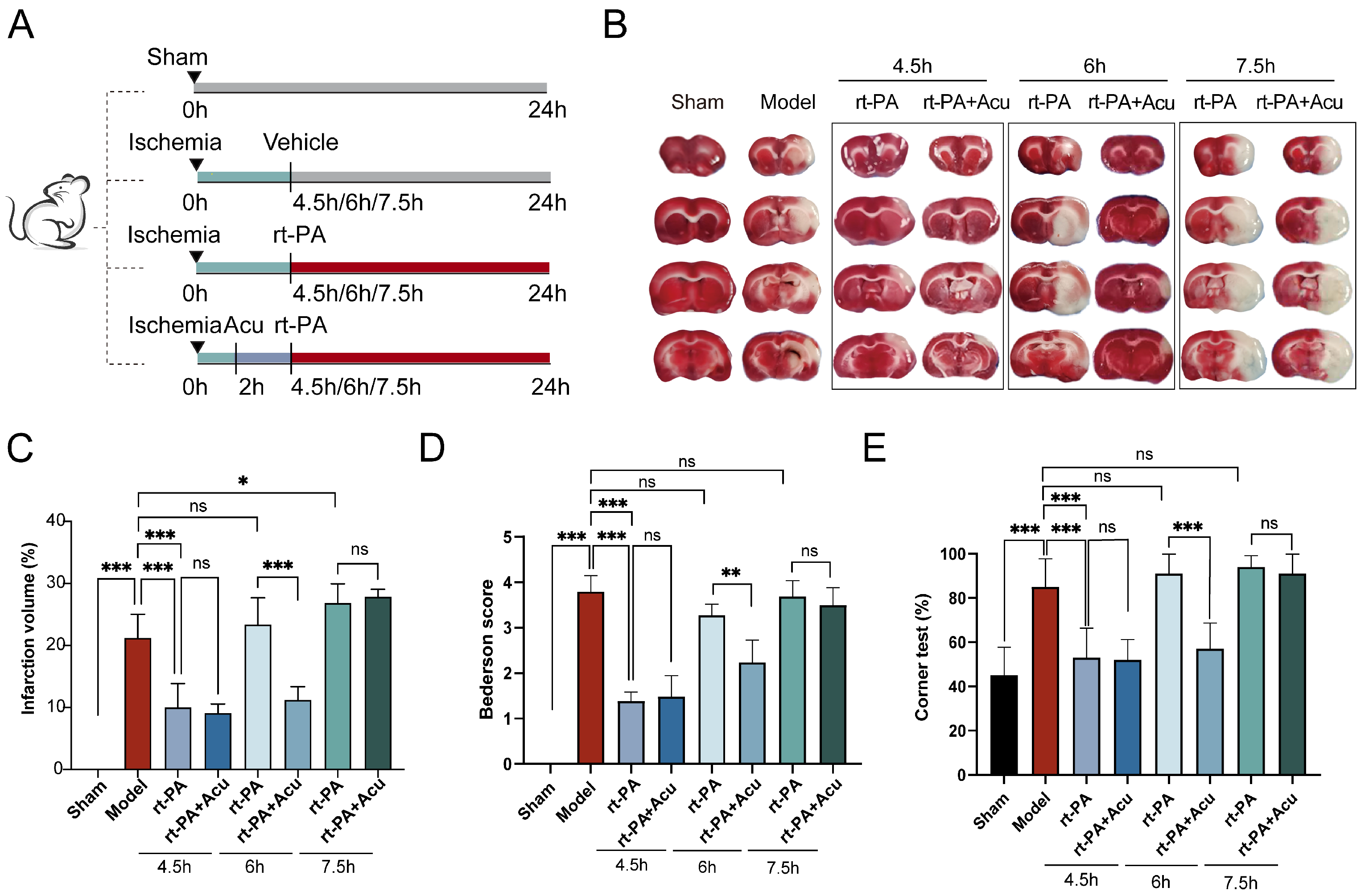
3.1. Acupuncture Extended the rt-PA Time Window to 6 h in the Embolic Stroke Model
3.2. Acupuncture Reduced Hemorrhagic Transformation and Cerebral Edema Caused by Delayed Thrombolysis with rt-PA
3.3. Transcriptome Analysis Revealed Acupuncture Can Ameliorate the Disruption of Blood Brain Barrier Components Caused by Delayed Thrombolysis
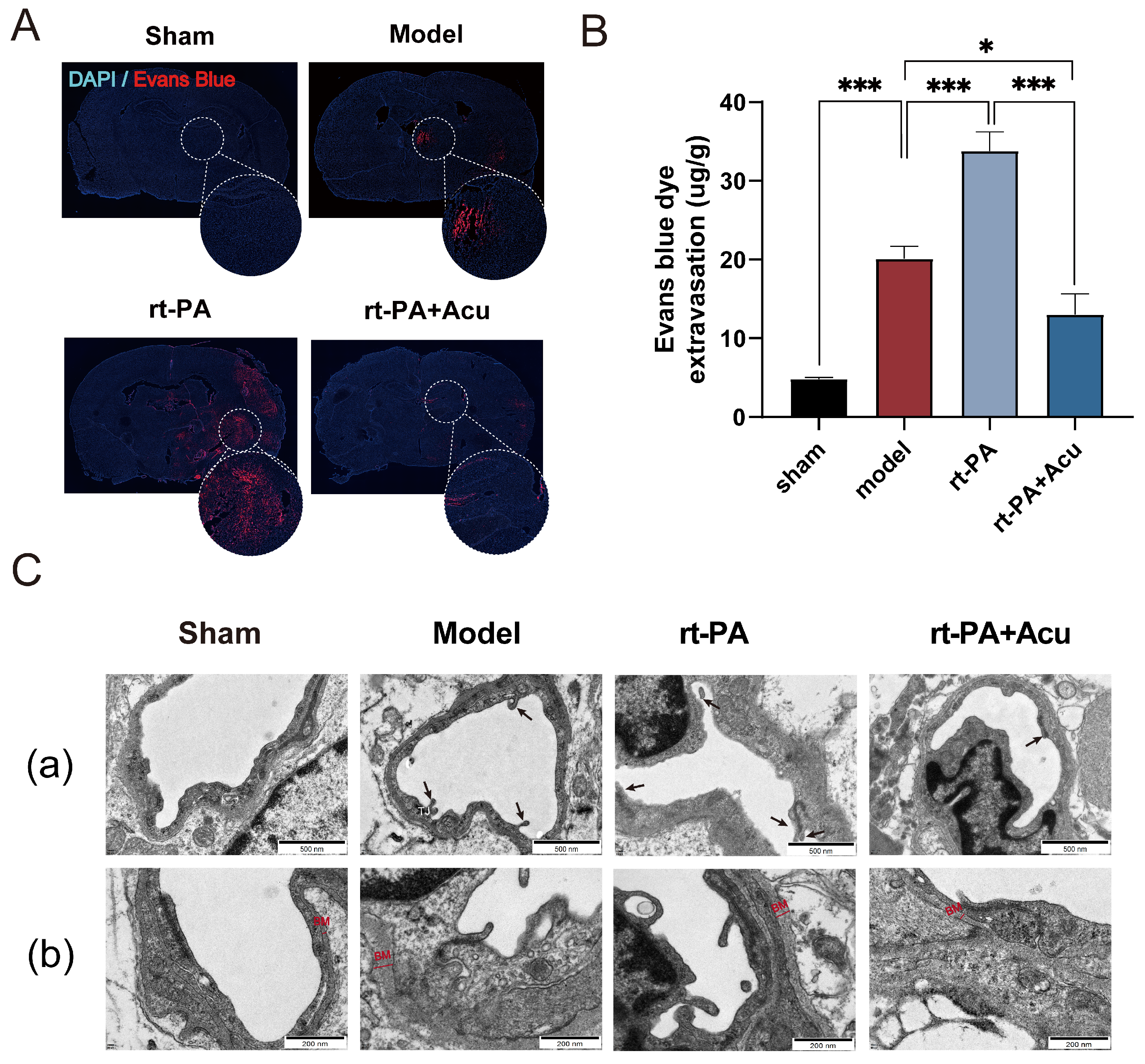
3.4. Acupuncture Suppressed Blood–Brain Barrier Leakage Induced by Delayed rt-PA Thrombolysis
3.5. Acupuncture Restored the Down-Regulation Expression of Tight Junction Proteins
3.6. Acupuncture Suppressed BMECs Apoptosis after Delayed rt-PA Thrombolysis
3.7. Acupuncture Restored the Balance of BMECs Autophagy and Apoptosis through Modulation of Bcl-2-Beclin1 Complex
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Tu, W.J.; Zhao, Z.; Yin, P.; Cao, L.; Zeng, J.; Chen, H.; Fan, D.; Fang, Q.; Gao, P.; Gu, Y.; et al. Estimated Burden of Stroke in China in 2020. JAMA Netw. Open 2023, 6, e231455. [Google Scholar] [CrossRef] [PubMed]
- Walter, K. What Is Acute Ischemic Stroke? JAMA 2022, 327, 885. [Google Scholar] [CrossRef] [PubMed]
- Zhang, S.; Wang, D.; Li, L. Recombinant tissue-type plasminogen activator (rt-PA) effectively restores neurological function and improves prognosis in acute ischemic stroke. Am. J. Transl. Res. 2023, 15, 3460–3467. [Google Scholar] [PubMed]
- Teekaput, C.; Thiankhaw, K.; Tanprawate, S.; Teekaput, K.; Chai-Adisaksopha, C. Outcomes of asymptomatic recombinant tissue plasminogen activator associated intracranial hemorrhage. PLoS ONE 2022, 17, e0272257. [Google Scholar] [CrossRef] [PubMed]
- Liu, C.; Xie, J.; Sun, S.; Li, H.; Li, T.; Jiang, C.; Chen, X.; Wang, J.; Le, A.; Wang, J.; et al. Hemorrhagic Transformation After Tissue Plasminogen Activator Treatment in Acute Ischemic Stroke. Cell Mol. Neurobiol. 2022, 42, 621–646. [Google Scholar] [CrossRef] [PubMed]
- Yoshimura, S.; Sakai, N.; Yamagami, H.; Uchida, K.; Beppu, M.; Toyoda, K.; Matsumaru, Y.; Matsumoto, Y.; Kimura, K.; Takeuchi, M.; et al. Endovascular Therapy for Acute Stroke with a Large Ischemic Region. N. Engl. J. Med. 2022, 386, 1303–1313. [Google Scholar] [CrossRef] [PubMed]
- Jiang, X.; Andjelkovic, A.V.; Zhu, L.; Yang, T.; Bennett, M.V.L.; Chen, J.; Keep, R.F.; Shi, Y. Blood-brain barrier dysfunction and recovery after ischemic stroke. Prog Neurobiol. 2018, 163–164, 144–171. [Google Scholar] [CrossRef] [PubMed]
- Dudvarski Stankovic, N.; Teodorczyk, M.; Ploen, R.; Zipp, F.; Schmidt, M.H.H. Microglia-blood vessel interactions: A double-edged sword in brain pathologies. Acta Neuropathol. 2016, 131, 347–363. [Google Scholar] [CrossRef] [PubMed]
- Zhang, J.; Yuan, L.; Zhang, X.; Hamblin, M.H.; Zhu, T.; Meng, F.; Li, Y.; Chen, Y.E.; Yin, K.J. Altered long non-coding RNA transcriptomic profiles in brain microvascular endothelium after cerebral ischemia. Exp. Neurol. 2016, 277, 162–170. [Google Scholar] [CrossRef]
- Sandoval, K.E.; Witt, K.A. Blood-brain barrier tight junction permeability and ischemic stroke. Neurobiol. Dis. 2008, 32, 200–219. [Google Scholar] [CrossRef]
- Ishikawa, M.; Zhang, J.H.; Nanda, A.; Granger, D.N. Inflammatory responses to ischemia and reperfusion in the cerebral microcirculation. Front. Biosci. 2004, 9, 1339–1347. [Google Scholar] [CrossRef]
- Li, F.; Mao, Q.; Wang, J.; Zhang, X.; Lv, X.; Wu, B.; Yan, T.; Jia, Y. Salidroside inhibited cerebral ischemia/reperfusion-induced oxidative stress and apoptosis via Nrf2/Trx1 signaling pathway. Metab. Brain Dis. 2022, 37, 2965–2978. [Google Scholar] [CrossRef]
- Song, H.; Chen, X.; Yu, Y.; Zhang, L. Xingnao Kaiqiao acupuncture combined with Angong Niuhuang Wan for a patient under persistent vegetative state: A case report. Front. Med. 2018, 12, 334–339. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Z.H.; Zhang, X.C.; Ni, G.X. Thrombolysis combined with acupuncture therapy for acute cerebral infarction: A Meta-analysis of randomized controlled trials. Zhen Ci Yan Jiu 2021, 46, 431–438. [Google Scholar] [CrossRef] [PubMed]
- Yang, Z.X.; Xie, J.H.; Liu, Y.P.; Miao, G.X.; Wang, Y.H.; Wu, S.M.; Li, Y. Systematic review of long-term Xingnao Kaiqiao needling effcacy in ischemic stroke treatment. Neural Regen. Res. 2015, 10, 583–588. [Google Scholar] [CrossRef] [PubMed]
- Yang, Z.X.; Xie, J.H.; Liu, D.D. Xingnao Kaiqiao needling method for acute ischemic stroke: A meta-analysis of safety and efficacy. Neural Regen. Res. 2017, 12, 1308–1314. [Google Scholar] [CrossRef]
- Dong, H.; Ni, G.X. Comparison of Therapeutic Effects of Acupuncture with Consciousness Restoring Needling Method Com-bined with Western Medicine on Acute Anterior and Posterior Cerebral Infarction. J. Tradit. Chin. Med. 2018, 59, 2031–2033+2056. [Google Scholar]
- Yang, J.; Hua, Z.; Chen, Q. Effect of Xingnao Kaiqiao Acupuncture combined with Alteplase Thrombolysis on the Inflam-matory Reaction and Blood Circulation in Patients with Acute Cerebral Infarction. J. Emerg. Tradit. Chin. Med. 2023, 32, 1576–1579. [Google Scholar]
- Zhang, Q.; Tao, H.; Chen, J. Efficacy of Xingnao Kaiqiao Acupuncture Combined with Alteplase IntravenousThrombolysis on Acute Cerebral Infarction Patients with Neurological Defect. J. Emerg. Tradit. Chin. Med. 2018, 27, 1956–1959. [Google Scholar]
- Costa, V.; Aprile, M.; Esposito, R.; Ciccodicola, A. RNA-Seq and human complex diseases: Recent accomplishments and future perspectives. Eur. J. Hum. Genet. 2013, 21, 134–142. [Google Scholar] [CrossRef]
- Kestner, R.I.; Mayser, F.; Vutukuri, R.; Hansen, L.; Gunther, S.; Brunkhorst, R.; Devraj, K.; Pfeilschifter, W. Gene Expression Dynamics at the Neurovascular Unit During Early Regeneration After Cerebral Ischemia/Reperfusion Injury in Mice. Front. Neurosci. 2020, 14, 280. [Google Scholar] [CrossRef] [PubMed]
- Deshpande, D.; Chhugani, K.; Chang, Y.; Karlsberg, A.; Loeffler, C.; Zhang, J.; Muszynska, A.; Munteanu, V.; Yang, H.; Rotman, J.; et al. RNA-seq data science: From raw data to effective interpretation. Front. Genet. 2023, 14, 997383. [Google Scholar] [CrossRef] [PubMed]
- Zhang, L.; Zhang, R.L.; Jiang, Q.; Ding, G.; Chopp, M.; Zhang, Z.G. Focal embolic cerebral ischemia in the rat. Nat. Protoc. 2015, 10, 539–547. [Google Scholar] [CrossRef] [PubMed]
- Menzies, S.A.; Hoff, J.T.; Betz, A.L. Middle cerebral artery occlusion in rats: A neurological and pathological evaluation of a reproducible model. Neurosurgery 1992, 31, 100–106. [Google Scholar] [CrossRef]
- Choudhri, T.F.; Hoh, B.L.; Solomon, R.A.; Connolly, E.S., Jr.; Pinsky, D.J. Use of a spectrophotometric hemoglobin assay to objectively quantify intracerebral hemorrhage in mice. Stroke 1997, 28, 2296–2302. [Google Scholar] [CrossRef]
- Cardiff, R.D.; Miller, C.H.; Munn, R.J. Manual hematoxylin and eosin staining of mouse tissue sections. Cold Spring Harb. Protoc. 2014, 2014, 655–658. [Google Scholar] [CrossRef]
- Love, M.I.; Huber, W.; Anders, S. Moderated estimation of fold change and dispersion for RNA-seq data with DESeq2. Genome Biol. 2014, 15, 550. [Google Scholar] [CrossRef]
- Yu, G.; Wang, L.G.; Han, Y.; He, Q.Y. clusterProfiler: An R package for comparing biological themes among gene clusters. Omics A J. Integr. Biol. 2012, 16, 284–287. [Google Scholar] [CrossRef]
- Chen, Y.; Wang, X. miRDB: An online database for prediction of functional microRNA targets. Nucleic Acids Res. 2020, 48, D127–D131. [Google Scholar] [CrossRef]
- Si, Z.; Liu, J.; Hu, K.; Lin, Y.; Liu, J.; Wang, A. Effects of thrombolysis within 6 hours on acute cerebral infarction in an improved rat embolic middle cerebral artery occlusion model for ischaemic stroke. J. Cell Mol. Med. 2019, 23, 2468–2474. [Google Scholar] [CrossRef]
- Thiebaut, A.M.; Gauberti, M.; Ali, C.; Martinez De Lizarrondo, S.; Vivien, D.; Yepes, M.; Roussel, B.D. The role of plasminogen activators in stroke treatment: Fibrinolysis and beyond. Lancet Neurol. 2018, 17, 1121–1132. [Google Scholar] [CrossRef]
- Deng, Y.H.; He, H.Y.; Yang, L.Q.; Zhang, P.Y. Dynamic changes in neuronal autophagy and apoptosis in the ischemic penumbra following permanent ischemic stroke. Neural Regen. Res. 2016, 11, 1108–1114. [Google Scholar] [CrossRef] [PubMed]
- Cecchelli, R.; Berezowski, V.; Lundquist, S.; Culot, M.; Renftel, M.; Dehouck, M.P.; Fenart, L. Modelling of the blood-brain barrier in drug discovery and development. Nat. Rev. Drug Discov. 2007, 6, 650–661. [Google Scholar] [CrossRef] [PubMed]
- Tian, D.S.; Qin, C.; Zhou, L.Q.; Yang, S.; Chen, M.; Xiao, J.; Shang, K.; Bosco, D.B.; Wu, L.J.; Wang, W. FSAP aggravated endothelial dysfunction and neurological deficits in acute ischemic stroke due to large vessel occlusion. Signal Transduct. Target. Ther. 2022, 7, 6. [Google Scholar] [CrossRef] [PubMed]
- Lu, D.; Mai, H.C.; Liang, Y.B.; Xu, B.D.; Xu, A.D.; Zhang, Y.S. Beneficial Role of Rosuvastatin in Blood-Brain Barrier Damage Following Experimental Ischemic Stroke. Front. Pharmacol. 2018, 9, 926. [Google Scholar] [CrossRef]
- Hu, X.; De Silva, T.M.; Chen, J.; Faraci, F.M. Cerebral Vascular Disease and Neurovascular Injury in Ischemic Stroke. Circ. Res. 2017, 120, 449–471. [Google Scholar] [CrossRef] [PubMed]
- Broughton, B.R.; Reutens, D.C.; Sobey, C.G. Apoptotic mechanisms after cerebral ischemia. Stroke 2009, 40, e331–e339. [Google Scholar] [CrossRef]
- Czabotar, P.E.; Lessene, G.; Strasser, A.; Adams, J.M. Control of apoptosis by the BCL-2 protein family: Implications for physiology and therapy. Nat. Rev. Mol. Cell Biol. 2014, 15, 49–63. [Google Scholar] [CrossRef]
- Wei, Y.; Pattingre, S.; Sinha, S.; Bassik, M.; Levine, B. JNK1-mediated phosphorylation of Bcl-2 regulates starvation-induced autophagy. Mol. Cell 2008, 30, 678–688. [Google Scholar] [CrossRef]
- Ghavami, S.; Shojaei, S.; Yeganeh, B.; Ande, S.R.; Jangamreddy, J.R.; Mehrpour, M.; Christoffersson, J.; Chaabane, W.; Moghadam, A.R.; Kashani, H.H.; et al. Autophagy and apoptosis dysfunction in neurodegenerative disorders. Prog. Neurobiol. 2014, 112, 24–49. [Google Scholar] [CrossRef]
- Song, Y.; Zhang, X.; Zhang, J.; Wang, S.; Bai, Y.; Xu, B.; Lu, M.; Ni, G.X. Effect of Xingnao Kaiqiao acupuncture on safety of rt-PA intravenous thrombolysis in patients with cerebral infarction: A randomized controlled trial. Chin. Acupunct. Moxi-Bustion 2022, 42, 961–965. [Google Scholar]
- Messlinger, K.; Balcziak, L.K.; Russo, A.F. Cross-talk signaling in the trigeminal ganglion: Role of neuropeptides and other mediators. J. Neural Transm. 2020, 127, 431–444. [Google Scholar] [CrossRef] [PubMed]
- Li, J.; He, J.; Du, Y.; Cui, J.; Ma, Y.; Zhang, X. Electroacupuncture improves cerebral blood flow and attenuates moderate ischemic injury via Angiotensin II its receptors-mediated mechanism in rats. BMC Complement. Altern. Med. 2014, 14, 441. [Google Scholar] [CrossRef] [PubMed]
- Han, L.; Wang, Y.; Wang, G.; Chen, Y.; Lin, H.; Zhang, Y.; Shen, Y. Acupuncture ameliorates neurological function in rats with cerebral ischemia-reperfusion by regulating the opening of large-conductance Ca2+-activated potassium channels. Brain Behav. 2021, 11, e2286. [Google Scholar] [CrossRef] [PubMed]
- Yang, L.; Yang, B.C.; Zhang, C.X.; Tong, J. Protective effects of acupuncture and LGNHFD on expressions of vascular endothelial growth factor, basic fibroblast growth factor, and cluster of differentiation 34 in rats with cerebral ischemia-reperfusion injury. J. Tradit. Chin. Med. 2021, 41, 463–470. [Google Scholar] [CrossRef] [PubMed]
- Zhang, W.; Han, L.; Wen, Y.; Su, L.; Li, Y.; Luo, X. Electroacupuncture reverses endothelial cell death and promotes angiogenesis through the VEGF/Notch signaling pathway after focal cerebral ischemia-reperfusion injury. Brain Behav. 2023, 13, e2912. [Google Scholar] [CrossRef]
- Zhang, C.; Wen, Y.; Fan, X.N.; Tian, G.; Zhou, X.Y.; Deng, S.Z.; Meng, Z.H. Therapeutic effects of different durations of acupuncture on rats with middle cerebral artery occlusion. Neural Regen. Res. 2015, 10, 159–164. [Google Scholar] [CrossRef]
- Sha, R.; Zhang, B.; Han, X.; Peng, J.; Zheng, C.; Zhang, F.; Huang, X. Electroacupuncture Alleviates Ischemic Brain Injury by Inhibiting the miR-223/NLRP3 Pathway. Med. Sci. Monit. 2019, 25, 4723–4733. [Google Scholar] [CrossRef]
- Xing, Y.; Zhang, M.; Li, W.B.; Dong, F.; Zhang, F. Mechanisms Involved in the Neuroprotection of Electroacupuncture Therapy for Ischemic Stroke. Front. Neurosci. 2018, 12, 929. [Google Scholar] [CrossRef]
- Kim, Y.R.; Kim, H.N.; Ahn, S.M.; Choi, Y.H.; Shin, H.K.; Choi, B.T. Electroacupuncture promotes post-stroke functional recovery via enhancing endogenous neurogenesis in mouse focal cerebral ischemia. PLoS ONE 2014, 9, e90000. [Google Scholar] [CrossRef]
- Hsiu, H.; Huang, S.M.; Chen, C.T.; Hsu, C.L.; Hsu, W.C. Acupuncture stimulation causes bilaterally different microcirculatory effects in stroke patients. Microvasc. Res. 2011, 81, 289–294. [Google Scholar] [CrossRef] [PubMed]
- Wang, L.; Su, X.T.; Cao, Y.; Yang, N.N.; Hao, X.W.; Li, H.P.; Wang, Q.Y.; Yang, J.W. Potential mechanisms of acupuncture in enhancing cerebral perfusion of ischemic stroke. Front. Neurol. 2022, 13, 1030747. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Q.; Jia, M.; Wang, Y.; Wang, Q.; Wu, J. Cell Death Mechanisms in Cerebral Ischemia-Reperfusion Injury. Neurochem. Res. 2022, 47, 3525–3542. [Google Scholar] [CrossRef] [PubMed]
- Przykaza, L. Understanding the Connection Between Common Stroke Comorbidities, Their Associated Inflammation, and the Course of the Cerebral Ischemia/Reperfusion Cascade. Front. Immunol. 2021, 12, 782569. [Google Scholar] [CrossRef] [PubMed]
- Liu, L.L.; Liu, P.N.; Li, X.A.; Li, Y.N. Ultra-early electroacupuncture rehabilitation for intravenous thrombolysis-induced cerebral infarction. Eur. Rev. Med. Pharmacol. Sci. 2023, 27, 10419–10426. [Google Scholar] [CrossRef]
- Daneman, R.; Agalliu, D.; Zhou, L.; Kuhnert, F.; Kuo, C.J.; Barres, B.A. Wnt/beta-catenin signaling is required for CNS, but not non-CNS, angiogenesis. Proc. Natl. Acad. Sci. USA 2009, 106, 641–646. [Google Scholar] [CrossRef] [PubMed]
- Xu, P.; Zhang, X.; Liu, Q.; Xie, Y.; Shi, X.; Chen, J.; Li, Y.; Guo, H.; Sun, R.; Hong, Y.; et al. Microglial TREM-1 receptor mediates neuroinflammatory injury via interaction with SYK in experimental ischemic stroke. Cell Death Dis. 2019, 10, 555. [Google Scholar] [CrossRef] [PubMed]
- Napoli, J.L. Cellular retinoid binding-proteins, CRBP, CRABP, FABP5: Effects on retinoid metabolism, function and related diseases. Pharmacol. Ther. 2017, 173, 19–33. [Google Scholar] [CrossRef] [PubMed]
- Abdullahi, W.; Tripathi, D.; Ronaldson, P.T. Blood-brain barrier dysfunction in ischemic stroke: Targeting tight junctions and transporters for vascular protection. Am. J. Physiol. Cell Physiol. 2018, 315, C343–C356. [Google Scholar] [CrossRef]
- Candelario-Jalil, E.; Dijkhuizen, R.M.; Magnus, T. Neuroinflammation, Stroke, Blood-Brain Barrier Dysfunction, and Imaging Modalities. Stroke 2022, 53, 1473–1486. [Google Scholar] [CrossRef]
- Zhang, L.; Bai, W.; Sun, L.; Lin, Y.; Tian, M. Targeting Non-Coding RNA for CNS Injuries: Regulation of Blood-Brain Barrier Functions. Neurochem. Res. 2023, 48, 1997–2016. [Google Scholar] [CrossRef] [PubMed]
- Hernandes, M.S.; Xu, Q.; Griendling, K.K. Role of NADPH Oxidases in Blood-Brain Barrier Disruption and Ischemic Stroke. Antioxidants 2022, 11, 1966. [Google Scholar] [CrossRef] [PubMed]
- Zhang, K.; Jiang, Y.; Wang, B.; Li, T.; Shang, D.; Zhang, X. Mesenchymal Stem Cell Therapy: A Potential Treatment Targeting Pathological Manifestations of Traumatic Brain Injury. Oxid. Med. Cell. Longev. 2022, 2022, 4645021. [Google Scholar] [CrossRef] [PubMed]
- Garcia-Prat, L.; Martinez-Vicente, M.; Perdiguero, E.; Ortet, L.; Rodriguez-Ubreva, J.; Rebollo, E.; Ruiz-Bonilla, V.; Gutarra, S.; Ballestar, E.; Serrano, A.L.; et al. Autophagy maintains stemness by preventing senescence. Nature 2016, 529, 37–42. [Google Scholar] [CrossRef] [PubMed]









Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zhang, Z.; Lu, T.; Li, S.; Zhao, R.; Li, H.; Zhang, X.; Li, Y.; Xia, Y.; Ni, G. Acupuncture Extended the Thrombolysis Window by Suppressing Blood–Brain Barrier Disruption and Regulating Autophagy–Apoptosis Balance after Ischemic Stroke. Brain Sci. 2024, 14, 399. https://doi.org/10.3390/brainsci14040399
Zhang Z, Lu T, Li S, Zhao R, Li H, Zhang X, Li Y, Xia Y, Ni G. Acupuncture Extended the Thrombolysis Window by Suppressing Blood–Brain Barrier Disruption and Regulating Autophagy–Apoptosis Balance after Ischemic Stroke. Brain Sciences. 2024; 14(4):399. https://doi.org/10.3390/brainsci14040399
Chicago/Turabian StyleZhang, Zhihui, Tianliang Lu, Shanshan Li, Ruyu Zhao, Honglei Li, Xinchang Zhang, Yiyang Li, Yawen Xia, and Guangxia Ni. 2024. "Acupuncture Extended the Thrombolysis Window by Suppressing Blood–Brain Barrier Disruption and Regulating Autophagy–Apoptosis Balance after Ischemic Stroke" Brain Sciences 14, no. 4: 399. https://doi.org/10.3390/brainsci14040399