
Impact of Repetitive Transcranial Magnetic Stimulation on Cognitive and Psychiatric Dysfunction in Patients with Fibromyalgia: A Double-Blinded, Randomized Clinical Trial

 , , , , and
, , , , and
Abstract
:1. Introduction
2. Materials and Methods
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Leon-Llamas, J.L.; Murillo-Garcia, A.; Villafaina, S.; Domínguez-Muñoz, F.J.; Morenas, J.; Gusi, N. Relationship between Kinesiophobia and Mobility, Impact of the Disease, and Fear of Falling in Women with and without Fibromyalgia: A Cross-Sectional Study. Int. J. Environ. Res. Public Health 2022, 19, 8257. [Google Scholar] [CrossRef]
- Siracusa, R.; Paola, R.D.; Cuzzocrea, S.; Impellizzeri, D. Fibromyalgia: Pathogenesis, Mechanisms, Diagnosis and Treatment Options Update. Int. J. Mol. Sci. 2021, 22, 3891. [Google Scholar] [CrossRef] [PubMed]
- Fitzcharles, M.A.; Cohen, S.P.; Clauw, D.J.; Littlejohn, G.; Usui, C.; Häuser, W. Nociplastic pain: Towards an understanding of prevalent pain conditions. Lancet 2021, 397, 2098–2110. [Google Scholar] [CrossRef] [PubMed]
- Giesecke, T.; Gracely, R.H.; Williams, D.A.; Geisser, M.E.; Petzke, F.W.; Clauw, D.J. The relationship between depression, clinical pain, and experimental pain in a chronic pain cohort. Arthritis Rheum 2005, 52, 1577–1584. [Google Scholar] [CrossRef] [PubMed]
- Arnold, L.M.; Bennett, R.M.; Crofford, L.J.; Dean, L.E.; Clauw, D.J.; Goldenberg, D.L.; Fitzcharles, M.A.; Paiva, E.S.; Staud, R.; Sarzi-Puttini, P.; et al. AAPT Diagnostic Criteria for Fibromyalgia. J. Pain 2019, 20, 611–628. [Google Scholar] [CrossRef] [PubMed]
- Muñoz Ladrón de Guevara, C.; Fernández-Serrano, M.J.; Reyes Del Paso, G.A.; Duschek, S. Executive function impairments in fibromyalgia syndrome: Relevance of clinical variables and body mass index. PLoS ONE 2018, 13, e0196329. [Google Scholar] [CrossRef] [PubMed]
- Duque, L.; Fricchione, G. Fibromyalgia and its New Lessons for Neuropsychiatry. Med. Sci. Monit. Basic Res. 2019, 25, 169–178. [Google Scholar] [CrossRef] [PubMed]
- Leung, A.; Donohue, M.; Xu, R.; Lee, R.; Lefaucheur, J.P.; Khedr, E.M.; Saitoh, Y.; André-Obadia, N.; Rollnik, J.; Wallace, M.; et al. rTMS for suppressing neuropathic pain: A meta-analysis. J. Pain 2009, 10, 1205–1216. [Google Scholar] [CrossRef] [PubMed]
- Khedr, E.M.; Kotb, H.; Kamel, N.F.; Ahmed, M.A.; Sadek, R.; Rothwell, J.C. Longlasting antalgic effects of daily sessions of repetitive transcranial magnetic stimulation in central and peripheral neuropathic pain. J. Neurol. Neurosurg. Psychiatry 2005, 76, 833–838. [Google Scholar] [CrossRef]
- Ahmed, M.A.; Darwish, E.S.; Khedr, E.M.; El Serogy, Y.M.; Ali, A.M. Effects of low versus high frequencies of repetitive transcranial magnetic stimulation on cognitive function and cortical excitability in Alzheimer’s dementia. J. Neurol. 2012, 259, 83–92. [Google Scholar] [CrossRef]
- Khedr, E.M.; Mohamed, K.O.; Ali, A.M.; Hasan, A.M. The effect of repetitive transcranial magnetic stimulation on cognitive impairment in Parkinson’s disease with dementia: Pilot study. Restor. Neurol. Neurosci. 2020, 38, 55–66. [Google Scholar] [CrossRef] [PubMed]
- Khedr, E.M.; Elbeh, K.; Saber, M.; Abdelrady, Z.; Abdelwarith, A. A double blind randomized clinical trial of the effectiveness of low frequency rTMS over right DLPFC or OFC for treatment of obsessive-compulsive disorder. J. Psychiatr. Res. 2022, 156, 122–131. [Google Scholar] [CrossRef]
- Vida, R.G.; Sághy, E.; Bella, R.; Kovács, S.; Erdősi, D.; Józwiak-Hagymásy, J.; Zemplényi, A.; Tényi, T.; Osváth, P.; Voros, V. Efficacy of repetitive transcranial magnetic stimulation (rTMS) adjunctive therapy for major depressive disorder (MDD) after two antidepressant treatment failures: Meta-analysis of randomized sham-controlled trials. BMC Psychiatry 2023, 23, 545. [Google Scholar] [CrossRef] [PubMed]
- Saltychev, M.; Laimi, K. Effectiveness of repetitive transcranial magnetic stimulation in patients with fibromyalgia: A meta-analysis. Int. J. Rehabil. Res. 2017, 40, 11–18. [Google Scholar] [CrossRef] [PubMed]
- Leung, A.; Shirvalkar, P.; Chen, R.; Kuluva, J.; Vaninetti, M.; Bermudes, R.; Poree, L.; Wassermann, E.M.; Kopell, B.; Levy, R. Transcranial Magnetic Stimulation for Pain, Headache, and Comorbid Depression: INS-NANS Expert Consensus Panel Review and Recommendation. Neuromodulation 2020, 23, 267–290. [Google Scholar] [CrossRef] [PubMed]
- Lefaucheur, J.P.; André-Obadia, N.; Antal, A.; Ayache, S.S.; Baeken, C.; Benninger, D.H.; Cantello, R.M.; Cincotta, M.; de Carvalho, M.; De Ridder, D.; et al. Evidence-based guidelines on the therapeutic use of repetitive transcranial magnetic stimulation (rTMS). Clin. Neurophysiol. 2014, 125, 2150–2206. [Google Scholar] [CrossRef] [PubMed]
- Moscatelli, F.; Monda, V.; Limone, P.; Marsala, G.; Mancini, N.; Monda, M.; Messina, A.; De Maria, A.; Scarinci, A.; Monda, A.; et al. Acute non invasive brain stimulation improves performances in volleyball players. Physiol. Behav. 2023, 271, 114356. [Google Scholar] [CrossRef]
- Moscatelli, F.; Toto, G.A.; Valenzano, A.; Cibelli, G.; Monda, V.; Limone, P.; Mancini, N.; Messina, A.; Marsala, G.; Messina, G.; et al. High frequencies (HF) repetitive transcranial magnetic stimulation (rTMS) increase motor coordination performances in volleyball players. BMC Neurosci. 2023, 24, 30. [Google Scholar] [CrossRef]
- Lefaucheur, J.P.; Aleman, A.; Baeken, C.; Benninger, D.H.; Brunelin, J.; Di Lazzaro, V.; Filipović, S.R.; Grefkes, C.; Hasan, A.; Hummel, F.C.; et al. Evidence-based guidelines on the therapeutic use of repetitive transcranial magnetic stimulation (rTMS): An update (2014–2018). Clin. Neurophysiol. 2020, 131, 474–528. [Google Scholar] [CrossRef]
- Moisset, X.; de Andrade, D.C.; Bouhassira, D. From pulses to pain relief: An update on the mechanisms of rTMS-induced analgesic effects. Eur. J. Pain 2016, 20, 689–700. [Google Scholar] [CrossRef]
- Dall’Agnol, L.; Medeiros, L.F.; Torres, I.L.; Deitos, A.; Brietzke, A.; Laste, G.; de Souza, A.; Vieira, J.L.; Fregni, F.; Caumo, W. Repetitive transcranial magnetic stimulation increases the corticospinal inhibition and the brain-derived neurotrophic factor in chronic myofascial pain syndrome: An explanatory double-blinded, randomized, sham-controlled trial. J. Pain 2014, 15, 845–855. [Google Scholar] [CrossRef] [PubMed]
- Xiong, H.Y.; Zheng, J.J.; Wang, X.Q. Non-invasive Brain Stimulation for Chronic Pain: State of the Art and Future Directions. Front. Mol. Neurosci. 2022, 15, 888716. [Google Scholar] [CrossRef] [PubMed]
- Short, B.; Borckardt, J.J.; George, M.; Beam, W.; Reeves, S.T. Non-invasive brain stimulation approaches to fibromyalgia pain. J. Pain Manag. 2009, 2, 259–276. [Google Scholar] [PubMed]
- Avery, D.H.; Zarkowski, P.; Krashin, D.; Rho, W.K.; Wajdik, C.; Joesch, J.M.; Haynor, D.R.; Buchwald, D.; Roy-Byrne, P. Transcranial magnetic stimulation in the treatment of chronic widespread pain: A randomized controlled study. J. ECT 2015, 31, 57–66. [Google Scholar] [CrossRef] [PubMed]
- Choo, Y.J.; Kwak, S.G.; Chang, M.C. Effectiveness of Repetitive Transcranial Magnetic Stimulation on Managing Fibromyalgia: A Systematic Meta-Analysis. Pain Med. 2022, 23, 1272–1282. [Google Scholar] [CrossRef] [PubMed]
- Sun, P.; Fang, L.; Zhang, J.; Liu, Y.; Wang, G.; Qi, R. Repetitive Transcranial Magnetic Stimulation for Patients with Fibromyalgia: A Systematic Review with Meta-Analysis. Pain Med. 2022, 23, 499–514. [Google Scholar] [CrossRef] [PubMed]
- Yang, S.; Chang, M.C. Effect of Repetitive Transcranial Magnetic Stimulation on Pain Management: A Systematic Narrative Review. Front. Neurol. 2020, 11, 114. [Google Scholar] [CrossRef] [PubMed]
- Wolfe, F.; Clauw, D.J.; Fitzcharles, M.A.; Goldenberg, D.L.; Katz, R.S.; Mease, P.; Russell, A.S.; Russell, I.J.; Winfield, J.B.; Yunus, M.B. The American College of Rheumatology preliminary diagnostic criteria for fibromyalgia and measurement of symptom severity. Arthritis Care Res. 2010, 62, 600–610. [Google Scholar] [CrossRef]
- Wolfe, F.; Clauw, D.J.; Fitzcharles, M.A.; Goldenberg, D.L.; Häuser, W.; Katz, R.L.; Mease, P.J.; Russell, A.S.; Russell, I.J.; Walitt, B. 2016 Revisions to the 2010/2011 fibromyalgia diagnostic criteria. Semin. Arthritis Rheum 2016, 46, 319–329. [Google Scholar] [CrossRef]
- Bennett, R. The Fibromyalgia Impact Questionnaire (FIQ): A review of its development, current version, operating characteristics and uses. Clin. Exp. Rheumatol. 2005, 23, S154–S162. [Google Scholar]
- Nasreddine, Z.S.; Phillips, N.A.; Bédirian, V.; Charbonneau, S.; Whitehead, V.; Collin, I.; Cummings, J.L.; Chertkow, H. The Montreal Cognitive Assessment, MoCA: A brief screening tool for mild cognitive impairment. J. Am. Geriatr. Soc. 2005, 53, 695–699. [Google Scholar] [CrossRef] [PubMed]
- Kim, H.; Yu, K.H.; Lee, B.C.; Kim, B.C.; Kang, Y. Validity of the Montreal Cognitive Assessment (MoCA) Index Scores: A Comparison with the Cognitive Domain Scores of the Seoul Neuropsychological Screening Battery (SNSB). Dement. Neurocogn. Disord. 2021, 20, 28–37. [Google Scholar] [CrossRef] [PubMed]
- Rahman, T.T.; El Gaafary, M.M. Montreal Cognitive Assessment Arabic version: Reliability and validity prevalence of mild cognitive impairment among elderly attending geriatric clubs in Cairo. Geriatr. Gerontol. Int. 2009, 9, 54–61. [Google Scholar] [CrossRef] [PubMed]
- Carlesimo, G.A.; Caltagirone, C.; Gainotti, G. The Mental Deterioration Battery: Normative data, diagnostic reliability and qualitative analyses of cognitive impairment. The Group for the Standardization of the Mental Deterioration Battery. Eur. Neurol. 1996, 36, 378–384. [Google Scholar] [CrossRef] [PubMed]
- Shallice, T. Specific impairments of planning. Philosophical Transactions of the Royal Society of London. B Biol. Sci. 1982, 298, 199–209. [Google Scholar]
- Giovagnoli, A.R.; Del Pesce, M.; Mascheroni, S.; Simoncelli, M.; Laiacona, M.; Capitani, E. Trail making test: Normative values from 287 normal adult controls. Ital. J. Neurol. Sci. 1996, 17, 305–309. [Google Scholar] [CrossRef] [PubMed]
- Arnett, J.A.; Labovitz, S.S. Effect of physical layout in performance of the Trail Making Test. Psychol. Assess. 1995, 7, 220. [Google Scholar] [CrossRef]
- Orsini, A.; Grossi, D.; Capitani, E.; Laiacona, M.; Papagno, C.; Vallar, G. Verbal and spatial immediate memory span: Normative data from 1355 adults and 1112 children. Ital. J. Neurol. Sci. 1987, 8, 537–548. [Google Scholar] [CrossRef] [PubMed]
- Obeid, S.; Hallit, C.A.E.; Haddad, C.; Hany, Z.; Hallit, S. Validation of the Hamilton Depression Rating Scale (HDRS) and sociodemographic factors associated with Lebanese depressed patients. L’encephale 2018, 44, 397–402. [Google Scholar] [CrossRef]
- Hamilton, M. The assessment of anxiety states by rating. Br. J. Med. Psychol. 1959, 32, 50–55. [Google Scholar] [CrossRef]
- Hallit, S.; Haddad, C.; Hallit, R.; Akel, M.; Obeid, S.; Haddad, G.; Soufia, M.; Khansa, W.; Khoury, R.; Kheir, N.; et al. Validation of the Hamilton Anxiety Rating Scale and State Trait Anxiety Inventory A and B in Arabic among the Lebanese population. Clin. Epidemiol. Glob. Health 2020, 8, 1104–1109. [Google Scholar] [CrossRef]
- Pridmore, S.; Fernandes Filho, J.A.; Nahas, Z.; Liberatos, C.; George, M.S. Motor threshold in transcranial magnetic stimulation: A comparison of a neurophysiological method and a visualization of movement method. J. ECT 1998, 14, 25–27. [Google Scholar] [CrossRef] [PubMed]
- Sampson, S.M.; Rome, J.D.; Rummans, T.A. Slow-frequency rTMS reduces fibromyalgia pain. Pain Med. 2006, 7, 115–118. [Google Scholar] [CrossRef] [PubMed]
- Bohning, D.E. Introduction and Overview of TMS Physics; American Psychiatric Press: Washington, DC, USA, 2000; pp. 13–44. [Google Scholar]
- Sluka, K.A.; Clauw, D.J. Neurobiology of fibromyalgia and chronic widespread pain. Neuroscience 2016, 338, 114–129. [Google Scholar] [CrossRef]
- Bennett, R.M.; Jones, J.; Turk, D.C.; Russell, I.J.; Matallana, L. An internet survey of 2,596 people with fibromyalgia. BMC Musculoskelet. Disord. 2007, 8, 27. [Google Scholar] [CrossRef] [PubMed]
- Yağcı, İ.; Ağırman, M.; Öztürk, D.; Eren, B. Is the transcranial magnetic stimulation an adjunctive treatment in fibromyalgia patients? Turk. J. Phys. Med. Rehabil. 2014, 60, 206–211. [Google Scholar] [CrossRef]
- Lee, S.J.; Kim, D.Y.; Chun, M.H.; Kim, Y.G. The effect of repetitive transcranial magnetic stimulation on fibromyalgia: A randomized sham-controlled trial with 1-mo follow-up. Am. J. Phys. Med. Rehabil. 2012, 91, 1077–1085. [Google Scholar] [CrossRef] [PubMed]
- Fitzgibbon, B.M.; Hoy, K.E.; Knox, L.A.; Guymer, E.K.; Littlejohn, G.; Elliot, D.; Wambeek, L.E.; McQueen, S.; Elford, K.A.; Lee, S.J.; et al. Evidence for the improvement of fatigue in fibromyalgia: A 4-week left dorsolateral prefrontal cortex repetitive transcranial magnetic stimulation randomized-controlled trial. Eur. J. Pain 2018, 22, 1255–1267. [Google Scholar] [CrossRef] [PubMed]
- Mhalla, A.; Baudic, S.; de Andrade, D.C.; Gautron, M.; Perrot, S.; Teixeira, M.J.; Attal, N.; Bouhassira, D. Long-term maintenance of the analgesic effects of transcranial magnetic stimulation in fibromyalgia. Pain 2011, 152, 1478–1485. [Google Scholar] [CrossRef]
- Boyer, L.; Dousset, A.; Roussel, P.; Dossetto, N.; Cammilleri, S.; Piano, V.; Khalfa, S.; Mundler, O.; Donnet, A.; Guedj, E. rTMS in fibromyalgia: A randomized trial evaluating QoL and its brain metabolic substrate. Neurology 2014, 82, 1231–1238. [Google Scholar] [CrossRef]
- Short, B.E.; Borckardt, J.J.; Anderson, B.S.; Frohman, H.; Beam, W.; Reeves, S.T.; George, M.S. Ten sessions of adjunctive left prefrontal rTMS significantly reduces fibromyalgia pain: A randomized, controlled pilot study. Pain 2011, 152, 2477–2484. [Google Scholar] [CrossRef] [PubMed]
- Tanwar, S.; Mattoo, B.; Kumar, U.; Bhatia, R. Repetitive transcranial magnetic stimulation of the prefrontal cortex for fibromyalgia syndrome: A randomised controlled trial with 6-months follow up. Adv. Rheumatol. 2020, 60, 34. [Google Scholar] [CrossRef] [PubMed]
- Izquierdo-Alventosa, R.; Inglés, M.; Cortés-Amador, S.; Gimeno-Mallench, L.; Sempere-Rubio, N.; Serra-Añó, P. Effectiveness of high-frequency transcranial magnetic stimulation and physical exercise in women with fibromyalgia: A randomized controlled trial. Phys. Ther. 2021, 101, pzab159. [Google Scholar] [CrossRef] [PubMed]
- Bilir, I.; Askin, A.; Sengul, I.; Tosun, A. Effects of High-Frequency Neuronavigated Repetitive Transcranial Magnetic Stimulation in Fibromyalgia Syndrome: A Double-Blinded, Randomized Controlled Study. Am. J. Phys. Med. Rehabil. 2021, 100, 138–146. [Google Scholar] [CrossRef] [PubMed]
- Passard, A.; Attal, N.; Benadhira, R.; Brasseur, L.; Saba, G.; Sichere, P.; Perrot, S.; Januel, D.; Bouhassira, D. Effects of unilateral repetitive transcranial magnetic stimulation of the motor cortex on chronic widespread pain in fibromyalgia. Brain 2007, 130, 2661–2670. [Google Scholar] [CrossRef] [PubMed]
- Ferreira Kdos, S.; Oliver, G.Z.; Thomaz, D.C.; Teixeira, C.T.; Foss, M.P. Cognitive deficits in chronic pain patients, in a brief screening test, are independent of comorbidities and medication use. Arq. Neuropsiquiatr. 2016, 74, 361–366. [Google Scholar] [CrossRef] [PubMed]
- Glass, J.M. Cognitive dysfunction in fibromyalgia and chronic fatigue syndrome: New trends and future directions. Curr. Rheumatol. Rep. 2006, 8, 425–429. [Google Scholar] [CrossRef] [PubMed]
- Glass, J.M. Review of cognitive dysfunction in fibromyalgia: A convergence on working memory and attentional control impairments. Rheum. Dis. Clin. N. Am. 2009, 35, 299–311. [Google Scholar] [CrossRef]
- Barbey, A.K.; Colom, R.; Grafman, J. Dorsolateral prefrontal contributions to human intelligence. Neuropsychologia 2013, 51, 1361–1369. [Google Scholar] [CrossRef]
- Li, Y.; Wang, L.; Jia, M.; Guo, J.; Wang, H.; Wang, M. The effects of high-frequency rTMS over the left DLPFC on cognitive control in young healthy participants. PLoS ONE 2017, 12, e0179430. [Google Scholar] [CrossRef]
- Baudic, S.; Attal, N.; Mhalla, A.; Ciampi de Andrade, D.; Perrot, S.; Bouhassira, D. Unilateral repetitive transcranial magnetic stimulation of the motor cortex does not affect cognition in patients with fibromyalgia. J. Psychiatr. Res. 2013, 47, 72–77. [Google Scholar] [CrossRef] [PubMed]
- Boyer, L.; Richieri, R.; Faget, C.; Padovani, R.; Vaillant, F.; Mundler, O.; Lançon, C.; Auquier, P.; Guedj, E. Functional involvement of superior temporal sulcus in quality of life of patients with schizophrenia. Psychiatry Res. 2012, 202, 155–160. [Google Scholar] [CrossRef] [PubMed]
- Moulier, V.; Gaudeau-Bosma, C.; Isaac, C.; Allard, A.C.; Bouaziz, N.; Sidhoumi, D.; Braha-Zeitoun, S.; Benadhira, R.; Thomas, F.; Januel, D. Effect of repetitive transcranial magnetic stimulation on mood in healthy subjects. Socioaffect. Neurosci. Psychol. 2016, 6, 29672. [Google Scholar] [CrossRef] [PubMed]
- Hausknecht, J.P.; Halpert, J.A.; Di Paolo, N.T.; Moriarty Gerrard, M.O. Retesting in selection: A meta-analysis of coaching and practice effects for tests of cognitive ability. J. Appl. Psychol. 2007, 92, 373–385. [Google Scholar] [CrossRef]
- Heilbronner, R.L.; Sweet, J.J.; Attix, D.K.; Krull, K.R.; Henry, G.K.; Hart, R.P. Official position of the American Academy of Clinical Neuropsychology on serial neuropsychological assessments: The utility and challenges of repeat test administrations in clinical and forensic contexts. Clin. Neuropsychol. 2010, 24, 1267–1278. [Google Scholar] [CrossRef]
- Scharfen, J.; Jansen, K.; Holling, H. Retest effects in working memory capacity tests: A meta-analysis. Psychon. Bull. Rev. 2018, 25, 2175–2199. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Sham Group (n = 20) (Mean ± SD) | Active Group (n = 20) (Mean ± SD) | Z | p-Value | |
|---|---|---|---|---|
| Age | 34.55 ± 8.32 34(14) | 31.9 ± 7.49 31(10) | −1.002 | 0.316 |
| Gender | ||||
| Males | 8(40%) | 9(45%) | 0.102 | 0.5 |
| Females | 12(60%) | 11(55%) | ||
| Education years | ||||
| Less than 5 years | 7(35%) | 8(40%) | 0.107 | 0.5 |
| 5 or more years | 13(65%) | 12(60%) | ||
| Duration of illness Median IQR | 6.60 ± 3.33 5.50(4.8) | 8.30 ± 3.17 8.25(4) | −1.79 | 0.073 |
| Fibromyalgia Impact Questionnaire (FIQ) Median IQR | 58.05 ± 15.02 59.5(25) | 63.25 ± 9.87 65(17) | −0.92 | 0.357 |
| Hamilton Depression Rating Scale (HDRS) Median IQR | 18.75 ± 2.40 19(5) | 18.90 ± 2.19 19(4) | −0.205 | 0.838 |
| Hamilton Anxiety Rating Scale (HARS) Median IQR | 20.70 ± 1.92 20.5(3) | 21.45 ± 2.01 21(3) | −1.094 | 0.274 |
| Montreal Cognitive Assessment (MoCA) Median IQR | 23.25 ± 1.83 23(4) | 23.10 ± 2.04 23(4) | −0.205 | 0.837 |
| Rey Auditory Verbal Learning Test (RAVLT) (sum of trials1–5 immediate real) Median (IQR) | 27.4 ± 4.005 26.5(7) | 26.9 ± 4.11 26(8) | −0.421 | 0.674 |
| Rey Auditory Verbal Learning Test (RAVLT) (delayed recall) Median (IQR) | 3.5 ± 1.05 3.5(1) | 3.25 ± 1.33 3(2) | −0.980 | 0.327 |
| Tower of London test (TOL) (total score) Median (IQR) | 20.12 ± 1.84 20(3.1) | 19.62 ± 1.74 19.85(2.8) | −0.758 | 0.448 |
| Tower of London test (TOL) (solution time in seconds) Median (IQR) | 27.28 ± 5.79 26.5(10.5) | 27.35 ± 5.81 26.5(10.5) | −0.41 | 0.968 |
| Tower of London test (TOL) (execution time in seconds) Median (IQR) | 14.01 ± 4.17 14.5(7.8) | 14.17 ± 4.04 14.5(7.8) | −0.204 | 0.839 |
| Trail Making Test (TMT) part A Median (IQR) | 70.5 ± 7.22 70(10) | 69.7 ± 5.84 70(10) | −0.108 | 0.914 |
| Trail Making Test (TMT) part B Median (IQR) | 112.8 ± 8.49 113(14) | 112.75 ± 8.84 113(16) | −0.027 | 0.978 |
| Digit Span Test (DST) forward Median (IQR) | 5.11 ± 0.67 5.15(1.1) | 5.09 ± 0.59 5.05(1.1) | −0.149 | 0.882 |
| Digit Span Test (DST) Backward Median (IQR) | 4.52 ± 0.625 4.55(1.1) | 4.40 ± 0.648 4.45(1.2) | −0.569 | 0.570 |
| Sham Group (n = 20) | Active Group (n = 20) | X2 | p-Value | |
|---|---|---|---|---|
| TCA and pregabalin/gabapentin | 0(0%) | 5(25%) | 6.091 | 0.107 |
| SSRI and pregabalin/gabapentin | 6(30%) | 5(25%) | ||
| SNRI and pregabalin/gabapentin | 10(50%) | 6(30%) | ||
| TCA, SSRI/SNRI, and pregabalin/gabapentin | 4(20%) | 4(20%) |
| Variable Assessment | Group I (Active rTMS) n = 20 | Group II (+Sham rTMS) n = 20 | p-Value | Group I (Active rTMS) n = 20 | Group II (+Sham rTMS) n = 20 | p-Value |
|---|---|---|---|---|---|---|
| Mean Difference ± SD (Pre–Post 1 Month after Sessions) | Mean Difference ± SD (Pre–Post 1 Month after Sessions) | Mean Difference ± SD (Pre–Post 3 Month after Session) | Mean Difference ± SD (Pre–Post 3 Months after Sessions) | |||
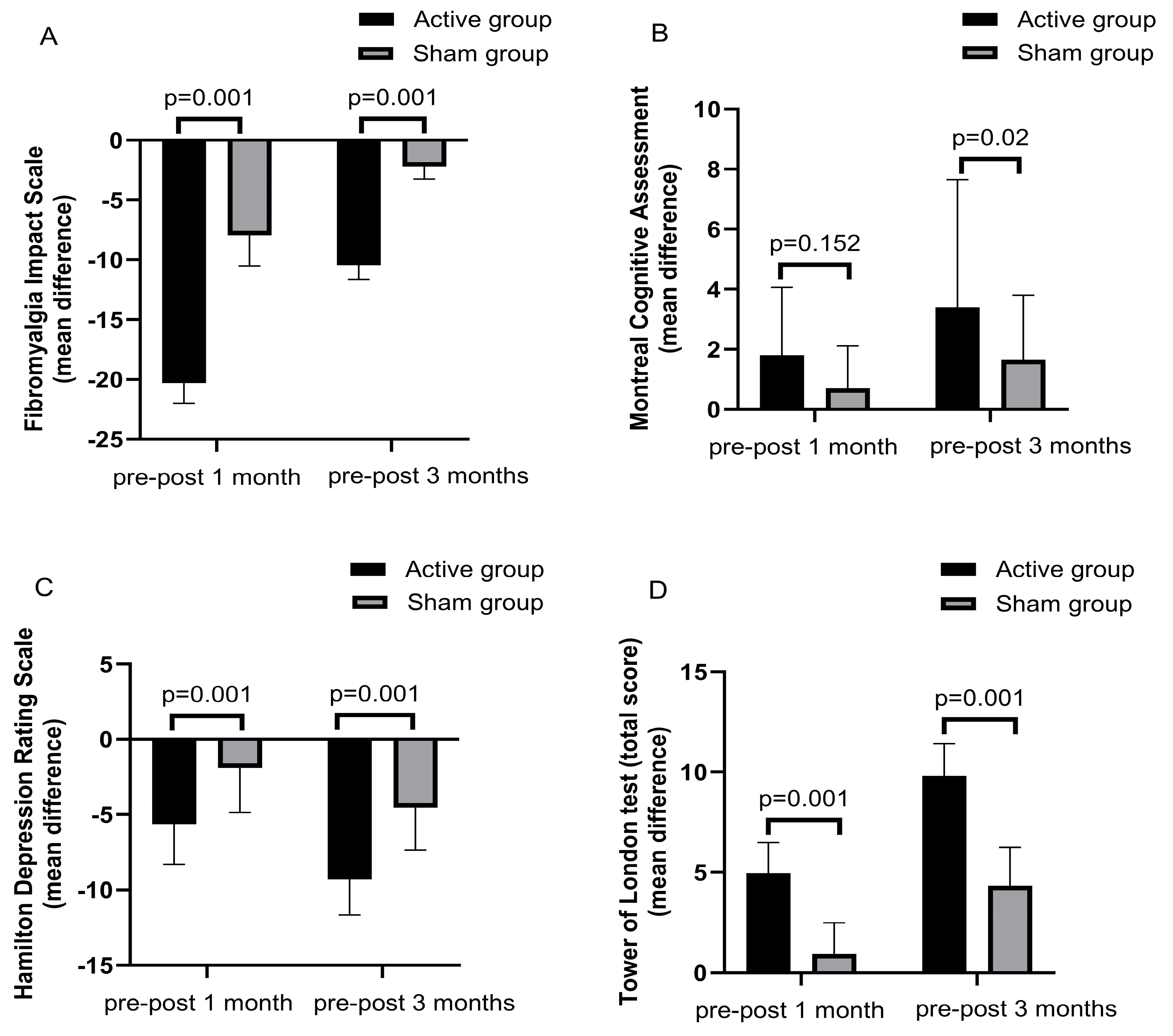
| Fibromyalgia Impact Questionnaire Median (IQR) | −20.30 ± 1.71 20(2.5) | −7.95 ± 2.56 8(2) | Z = −5.44, p = 0.001 | −10.45 ± 1.19 10.5(1) | −2.2 ± 1.05 2(1) | Z = −5.47, p = 0.001 |
| Hamilton Depression Rating Scale (HDRS) Median (IQR) | −5.65 ± 2.66 −6(1.75) | −1.9 ± 2.97 0(4) | Z = −3.228, p = 0.001 | −9.30 ± 2.36 −10(4) | −4.55 ± 2.81 −6(3) | Z = −4.616, p = 0.001 |
| Hamilton Anxiety Rating Scale (HARS) Median (IQR) | −5.05 ± 2.87 −6(4) | −0.80 ± 2.3 0(1.5) | Z = −4.086, p = 0.001 | −6.35 ± 2.81 −7(5.75) | −2.95 ± 2.32 −2.5(4.5) | Z = −3.498, p = 0.001 |
| Variable Assessment | Group I (Active rTMS) n = 20 | Group II (Sham rTMS) n = 20 | p-Value | Group I (Active rTMS) n = 20 | Group II (Sham rTMS) n = 20 | p-Value |
|---|---|---|---|---|---|---|
| Mean Difference ± SD (Pre–Post 1 Month) | Mean Difference ± SD (Pre–Post 1 Month) | Mean Difference ± SD (Pre–Post 3 Month) | Mean Difference ± SD (Pre–Post 3 Months) | |||
| Montreal Cognitive Assessment (MoCA) Median (IQR) | 1.8 ± 2.26 0(4.5) | 0.7 ± 1.41 0(1) | Z = −1.43, p = 0.152 | 3.4 ± 4.25 4(4.25) | 1.65 ± 2.15 0(3.5) | z = −2.27, p = 0.023 |
| Rey Auditory Verbal Learning Test (RAVLT) (sum of trials1–5 immediate real) Median (IQR) | 7.3 ± 3.09 6(3.25) | 1.95 ± 3.88 0(2) | Z = −4.46, p = 0.001 | 12.15 ± 2.85 11(2) | 4.9 ± 4.74 6(2.75) | Z = −4.50, p = 0.001 |
| Rey Auditory Verbal Learning Test (RAVLT) (delayed recall) Median (IQR) | 2.7 ± 0.80 3(0) | 0.4 ± 0.94 0(0) | Z = −5.08, p = 0.001 | 5.7 ± 0.80 6(0) | 1.55 ± 1.46 2(3) | Z = −5.62, p = 0.001 |
| Tower of London test (TOL) (total score) Median (IQR) | 4.95 ± 1.53 5(1.75) | 0.95 ± 1.54 0(2) | Z = −5.04, p = 0.001 | 9.8 ± 1.6 10(2.5) | 4.35 ± 1.89 5(2.42) | Z =−5.40, p = 0.001 |
| Tower of London test (TOL) (solution time in seconds) Median (IQR) | −16.75 ± 6.11 −14.5(11.13) | −15.68 ± 5.46 −14.5(4.45) | Z = −0.286, p = 0.775 | −10.8 ± 5.81 −12.5(7.5) | −3.5 ± 7.27 0(5) | Z = −2.60, p = 0.009 |
| Tower of London test (TOL) (execution time in seconds) Median (IQR) | −3.57 ± 4.52 0(8) | −2.41 ± 4.34 0(4.38) | Z = −1.008, p = 0.314 | −5.22 ± 4.36 −6.5(8) | −3.41 ± 4.61 0(8) | Z = −1.306, p = 0.192 |
| Trail Making Test (TMT) part A Median (IQR) | −8.05 ± 9.02 −2.5(20) | −1.45 ± 2.78 0(2) | Z = −2.09, p = 0.037 | −17.2 ± 6.03 −19(4) | −5.05 ± 7.33 −2(13.25) | Z = −4.11, p = 0.001 |
| Trail Making Test (TMT) part B Median (IQR) | −6.6 ± 8.77 0(16) | −0.6 ± 1.42 −0(0) | Z = −2.146, p = 0.032 | −12.35 ± 10.2 −15.5(20.5) | −4.3 ± 6.64 −1.5(4) | Z = −2.098, p = 0.036 |
| Digit Span Test (DST) forward. Median (IQR) | 2.13 ± 0.41 2(0) | 1.1 ± 0.52 1(0) | Z = −4.98, =0.001 | 4.26 ± 0.54 4.2(0.75) | 2.08 ± 0.46 2(0) | Z = −5.50, p = 0.001 |
| Digit Span Test (DST) Backward Median (IQR) | 2.57 ± 0.58 2.75(1) | 0.45 ± 0.48 0.25(1) | Z = 5.52, p = 0.001 | 4.57 ± 0.58 4.75(1) | 1.35 ± 0.46 1(1) | Z = −5.54, p = 0.001 |
| Changes in FIQ (Pre and Post Sessions) | Changes in FIQ (Pre and Post 3 Months) | |||
|---|---|---|---|---|
| Hamilton Depression Rating Scale (HDRS) | r | −0.270 | r | 0.170 |
| p-value | 0.250 | p-value | 0.474 | |
| Hamilton Anxiety Rating Scale (HARS) | r | 0.235 | r | 0.214 |
| p-value | 0.319 | p-value | 0.366 | |
| Montreal Cognitive Assessment (MoCA) | r | −0.436 | r | 0.089 |
| p-value | 0.055 | p-value | 0.708 | |
| Rey Auditory Verbal Learning Test (RAVLT) (sum of trials 1–5 immediate recall) | r | 0.536 | r | 0.315 |
| p-value | 0.015 | p-value | 0.177 | |
| Rey Auditory Verbal Learning Test (RAVLT) (delayed recall) | r | −0.257 | r | −0.062 |
| p-value | 0.274 | p-value | 0.796 | |
| Tower of London test (TOL) (total score) | r | 0.445 | r | 0.425 |
| p-value | 0.049 | p-value | 0.062 | |
| Tower of London test (TOL) (solution time in seconds) | r | −0.283 | r | −0.258 |
| p-value | 0.227 | p-value | 0.273 | |
| Tower of London test (TOL) (execution time in seconds) | r | −0.149 | r | −0.340 |
| p-value | 0.530 | p-value | 0.142 | |
| Trail Making Test (TMT) part A | r | −0.011 | r | −0.021 |
| p-value | 0.963 | p-value | 0.930 | |
| Trail Making Test (TMT) part B | r | 0.059 | r | −0.220 |
| p-value | 0.805 | p-value | 0.352 | |
| Digit Span Test (DST) forward | r | 0.236 | r | 0.441 |
| p-value | 0.317 | p-value | 0.052 | |
| Digit Span Test (DST) backward | r | −0.213 | r | −0.067 |
| p-value | 0.367 | p-value | 0.779 | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Badr, M.Y.; Ahmed, G.K.; Amer, R.A.; Aref, H.M.; Salem, R.M.; Elmokadem, H.A.; Khedr, E.M. Impact of Repetitive Transcranial Magnetic Stimulation on Cognitive and Psychiatric Dysfunction in Patients with Fibromyalgia: A Double-Blinded, Randomized Clinical Trial. Brain Sci. 2024, 14, 416. https://doi.org/10.3390/brainsci14050416
Badr MY, Ahmed GK, Amer RA, Aref HM, Salem RM, Elmokadem HA, Khedr EM. Impact of Repetitive Transcranial Magnetic Stimulation on Cognitive and Psychiatric Dysfunction in Patients with Fibromyalgia: A Double-Blinded, Randomized Clinical Trial. Brain Sciences. 2024; 14(5):416. https://doi.org/10.3390/brainsci14050416
Chicago/Turabian StyleBadr, Marwa Y., Gellan K. Ahmed, Reham A. Amer, Hend M. Aref, Rehab M. Salem, Heba A. Elmokadem, and Eman M. Khedr. 2024. "Impact of Repetitive Transcranial Magnetic Stimulation on Cognitive and Psychiatric Dysfunction in Patients with Fibromyalgia: A Double-Blinded, Randomized Clinical Trial" Brain Sciences 14, no. 5: 416. https://doi.org/10.3390/brainsci14050416