

Efficacy of a Soft Robotic Exoskeleton to Improve Lower Limb Motor Function in Children with Spastic Cerebral Palsy: A Single-Blinded Randomized Controlled Trial
 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Subjects and Inclusion Criteria
2.2. Study Design
2.3. Sample Size and Randomization
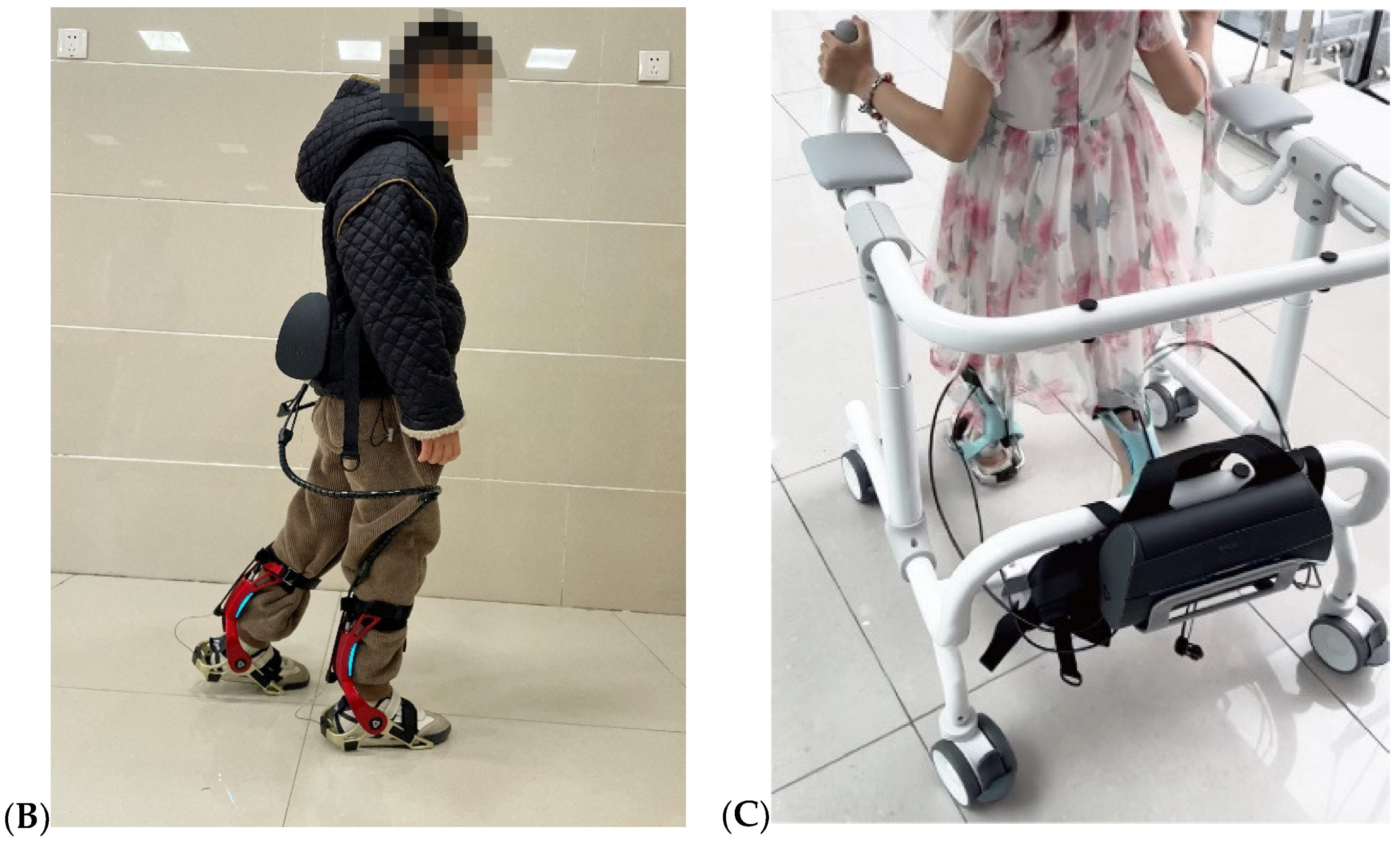
2.4. Soft Robotic Exoskeleton
2.5. Intervention
2.6. Assessment and Outcome Measures
2.6.1. 10-Meter Walk Test [26]
2.6.2. 6-Minute Walk Test
2.6.3. Gross Motor Function Measure [28]
2.6.4. Pediatric Balance Scale
2.6.5. Modified Ashworth Scale
2.6.6. Physiological Cost Index [29]
2.7. Statistical Analysis and Minimal Clinically Important Difference
3. Results
3.1. Participants
3.2. Primary Outcome Measures
3.3. Secondary Outcome Measures
3.4. Correlation Analysis
3.5. Minimal Clinically Important Difference
4. Discussion
5. Limitations
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Nahm, N.J.; Graham, H.K.; Gormley, M.E.; Georgiadis, A.G. Management of hypertonia in cerebral palsy. Curr. Opin. Pediatr. 2018, 30, 57–64. [Google Scholar] [CrossRef] [PubMed]
- Hanssen, B.; Peeters, N.; Vandekerckhove, I.; De Beukelaer, N.; Bar-On, L.; Molenaers, G.; Van Campenhout, A.; Degelaen, M.; Broeck, C.V.D.; Calders, P.; et al. The Contribution of Decreased Muscle Size to Muscle Weakness in Children with Spastic Cerebral Palsy. Front. Neurol. 2021, 12, 692582. [Google Scholar] [CrossRef] [PubMed]
- Palisano, R.; Rosenbaum, P.; Walter, S.; Russell, D.; Wood, E.; Galuppi, B. Development and reliability of a system to classify gross motor function in children with cerebral palsy. Dev. Med. Child Neurol. 1997, 39, 214–223. [Google Scholar] [CrossRef] [PubMed]
- Wu, M.; Kim, J.; Gaebler-Spira, D.J.; Schmit, B.D.; Arora, P. Robotic Resistance Treadmill Training Improves Locomotor Function in Children With Cerebral Palsy: A Randomized Controlled Pilot Study. Arch. Phys. Med. Rehabil. 2017, 98, 2126–2133. [Google Scholar] [CrossRef] [PubMed]
- Rosenbaum, P.; Paneth, N.; Leviton, A.; Goldstein, M.; Bax, M.; Damiano, D.; Dan, B.; Jacobsson, B. A report: The definition and classification of cerebral palsy April 2006. Dev. Med. Child Neurol. Suppl. 2007, 109, 8–14. [Google Scholar] [PubMed]
- Aiello, E.; Gates, D.H.; Patritti, B.L.; Cairns, K.D.; Meister, M.; Clancy, E.A.; Bonato, P. Visual EMG Biofeedback to Improve Ankle Function in Hemiparetic Gait. In Proceedings of the 2005 IEEE Engineering in Medicine and Biology 27th Annual Conference, Shanghai, China, 1–4 September 2005; pp. 7703–7706. [Google Scholar] [CrossRef]
- Raja, K.; Joseph, B.; Benjamin, S.; Minocha, V.; Rana, B. Physiological cost index in cerebral palsy: Its role in evaluating the efficiency of ambulation. J. Pediatr. Orthop. 2007, 27, 130–136. [Google Scholar] [CrossRef] [PubMed]
- Carvalho, I.; Pinto, S.M.; das Virgens Chagas, D.; dos Santos, J.L.P.; de Sousa Oliveira, T.; Batista, L.A. Robotic Gait Training for Individuals with Cerebral Palsy: A Systematic Review and Meta-Analysis. Arch. Phys. Med. Rehabil. 2017, 98, 2332–2344. [Google Scholar] [CrossRef] [PubMed]
- Pool, D.; Valentine, J.; Taylor, N.F.; Bear, N.; Elliott, C. Locomotor and robotic assistive gait training for children with cerebral palsy. Dev. Med. Child Neurol. 2021, 63, 328–335. [Google Scholar] [CrossRef]
- Yu, H.; Zheng, S.; Wu, J.; Sun, L.; Chen, Y.; Zhang, S.; Qin, Z. A New Single-Leg Lower-Limb Rehabilitation Robot: Design, Analysis and Experimental Evaluation. Machines 2023, 11, 447. [Google Scholar] [CrossRef]
- Yandell, M.B.; Quinlivan, B.T.; Popov, D.; Walsh, C.; Zelik, K.E. Physical interface dynamics alter how robotic exosuits augment human movement: Implications for optimizing wearable assistive devices. J. Neuroeng. Rehabil. 2017, 14, 40. [Google Scholar] [CrossRef] [PubMed]
- Awad, L.N.; Bae, J.; O’donnell, K.; De Rossi, S.M.M.; Hendron, K.; Sloot, L.H.; Kudzia, P.; Allen, S.; Holt, K.G.; Ellis, T.D.; et al. A soft robotic exosuit improves walking in patients after stroke. Sci. Transl. Med. 2017, 9, eaai9084. [Google Scholar] [CrossRef] [PubMed]
- Sloot, L.H.; Baker, L.M.; Bae, J.; Porciuncula, F.; Clément, B.F.; Siviy, C.; Nuckols, R.W.; Baker, T.; Sloutsky, R.; Choe, D.K.; et al. Effects of a soft robotic exosuit on the quality and speed of overground walking depends on walking ability after stroke. J. Neuroeng. Rehabil. 2023, 20, 113. [Google Scholar] [CrossRef] [PubMed]
- Ammann-Reiffer, C.; Bastiaenen, C.H.G.; Meyer-Heim, A.D.; van Hedel, H.J.A. Effectiveness of robot-assisted gait training in children with cerebral palsy: A bicenter, pragmatic, randomized, cross-over trial (PeLoGAIT). BMC Pediatr. 2017, 17, 64. [Google Scholar] [CrossRef] [PubMed]
- Esquenazi, A.; Talaty, M. Robotics for Lower Limb Rehabilitation. Phys. Med. Rehabil. Clin. N. Am. 2019, 30, 385–397. [Google Scholar] [CrossRef] [PubMed]
- Panizzolo, F.A.; Galiana, I.; Asbeck, A.T.; Siviy, C.; Schmidt, K.; Holt, K.G.; Walsh, C.J. A biologically-inspired multi-joint soft exosuit that can reduce the energy cost of loaded walking. J. Neuroeng. Rehabil. 2016, 13, 43. [Google Scholar] [CrossRef]
- Conner, B.; Orekhov, G.; Lerner, Z. Ankle Exoskeleton Assistance Increases Six-Minute Walk Test Performance in Cerebral Palsy. IEEE Open J. Eng. Med. Biol. 2021, 2, 320–323. [Google Scholar] [CrossRef] [PubMed]
- Shin, S.Y.; Hohl, K.; Giffhorn, M.; Awad, L.N.; Walsh, C.J.; Jayaraman, A. Correction to: Soft robotic exosuit augmented high intensity gait training on stroke survivors: A pilot study. J. Neuroeng. Rehabil. 2022, 19, 100. [Google Scholar] [CrossRef] [PubMed]
- Bae, J.; Awad, L.N.; Long, A.; O’Donnell, K.; Hendron, K.; Holt, K.G.; Ellis, T.D.; Walsh, C.J. Biomechanical mechanisms underlying exosuit-induced improvements in walking economy after stroke. J. Exp. Biol. 2018, 221, jeb168815. [Google Scholar] [CrossRef]
- Awad, L.N.; Esquenazi, A.; Francisco, G.E.; Nolan, K.J.; Jayaraman, A. The ReWalk ReStoreTM soft robotic exosuit: A multi-site clinical trial of the safety, reliability, and feasibility of exosuit-augmented post-stroke gait rehabilitation. J. Neuroeng. Rehabil. 2020, 17, 80. [Google Scholar] [CrossRef] [PubMed]
- Xie, R.; Zhang, Y.; Jin, H.; Yang, F.; Feng, Y.; Pan, Y. Effects of soft robotic exoskeleton for gait training on clinical and biomechanical gait outcomes in patients with sub-acute stroke: A randomized controlled pilot study. Front. Neurol. 2023, 14, 1296102. [Google Scholar] [CrossRef] [PubMed]
- Wu, M.; Kim, J.; Arora, P.; Gaebler-Spira, D.J.; Zhang, Y. Effects of the Integration of Dynamic Weight Shifting Training Into Treadmill Training on Walking Function of Children with Cerebral Palsy: A Randomized Controlled Study. Am. J. Phys. Med. Rehabil. 2017, 96, 765–772. [Google Scholar] [CrossRef] [PubMed]
- Aras, B.; Yaşar, E.; Kesikburun, S.; Türker, D.; Tok, F.; Yılmaz, B. Comparison of the effectiveness of partial body weight-supported treadmill exercises, robotic-assisted treadmill exercises, and anti-gravity treadmill exercises in spastic cerebral palsy. Turk. J. Phys. Med. Rehabil. 2019, 65, 361–370. [Google Scholar] [CrossRef] [PubMed]
- Peri, E.; Turconi, A.C.; Biffi, E.; Maghini, C.; Panzeri, D.; Morganti, R.; Pedrocchi, A.; Gagliardi, C. Effects of dose and duration of Robot-Assisted Gait Training on walking ability of children affected by cerebral palsy. Technol. Health Care 2017, 25, 671–681. [Google Scholar] [CrossRef] [PubMed]
- Cherni, Y.; Ballaz, L.; Lemaire, J.; Dal Maso, F.; Begon, M. Effect of low dose robotic-gait training on walking capacity in children and adolescents with cerebral palsy. Neurophysiol. Clin. 2020, 50, 507–519. [Google Scholar] [CrossRef] [PubMed]
- Chrysagis, N.; Skordilis, E.K.; Koutsouki, D. Validity and clinical utility of functional assessments in children with cerebral palsy. Arch. Phys. Med. Rehabil. 2014, 95, 369–374. [Google Scholar] [CrossRef] [PubMed]
- Nsenga Leunkeu, A.; Shephard, R.J.; Ahmaidi, S. Six-minute walk test in children with cerebral palsy gross motor function classification system levels I and II: Reproducibility, validity, and training effects. Arch. Phys. Med. Rehabil. 2012, 93, 2333–2339. [Google Scholar] [CrossRef] [PubMed]
- Russell, D.J.; Rosenbaum, P.L.; Cadman, D.T.; Gowland, C.; Hardy, S.; Jarvis, S. The gross motor function measure: A means to evaluate the effects of physical therapy. Dev. Med. Child Neurol. 1989, 31, 341–352. [Google Scholar] [CrossRef] [PubMed]
- Bratteby Tollerz, L.U.; Olsson, R.M.; Forslund, A.H.; Norrlin, S.E. Reliability of energy cost calculations in children with cerebral palsy, cystic fibrosis and healthy controls. Acta Paediatr. 2011, 100, 1616–1620. [Google Scholar] [CrossRef] [PubMed]
- Akerstedt, A.; Risto, O.; Odman, P.; Oberg, B. Evaluation of single event multilevel surgery and rehabilitation in children and youth with cerebral palsy—A 2-year follow-up study. Disabil. Rehabil. 2010, 32, 530–539. [Google Scholar] [CrossRef] [PubMed]
- Hayashi, S.; Miyata, K.; Takeda, R.; Iizuka, T.; Igarashi, T.; Usuda, S. Minimal clinically important difference of the Berg Balance Scale and comfortable walking speed in patients with acute stroke: A multicenter, prospective, longitudinal study. Clin. Rehabil. 2022, 36, 1512–1523. [Google Scholar] [CrossRef] [PubMed]
- Storm, F.A.; Petrarca, M.; Beretta, E.; Strazzer, S.; Piccinini, L.; Maghini, C.; Panzeri, D.; Corbetta, C.; Morganti, R.; Reni, G.; et al. Minimum Clinically Important Difference of Gross Motor Function and Gait Endurance in Children with Motor Impairment: A Comparison of Distribution-Based Approaches. BioMed Res. Int. 2020, 2020, 2794036. [Google Scholar] [CrossRef] [PubMed]
- Oeffinger, D.; Bagley, A.; Rogers, S.; Gorton, G.; Kryscio, R.; Abel, M.; Damiano, D.; Barnes, D.; Tylkowski, C. Outcome tools used for ambulatory children with cerebral palsy: Responsiveness and minimum clinically important differences. Dev. Med. Child Neurol. 2008, 50, 918–925. [Google Scholar] [CrossRef] [PubMed]
- Noten, S.; Pettersson, K.; Czuba, T.; Cloodt, E.; Casey, J.; Rodby-Bousquet, E. Probability of independent walking and wheeled mobility in individuals with cerebral palsy. Dev. Med. Child Neurol. 2024, 66, 326–332. [Google Scholar] [CrossRef] [PubMed]
- Damiano, D.L. Activity, activity, activity: Rethinking our physical therapy approach to cerebral palsy. Phys. Ther. 2006, 86, 1534–1540. [Google Scholar] [CrossRef] [PubMed]
- Krakauer, J.W.; Hadjiosif, A.M.; Xu, J.; Wong, A.L.; Haith, A.M. Motor Learning. Compr. Physiol. 2019, 9, 613–663. [Google Scholar] [CrossRef] [PubMed]
- Haith, A.M.; Krakauer, J.W. The multiple effects of practice: Skill, habit and reduced cognitive load. Curr. Opin. Behav. Sci. 2018, 20, 196–201. [Google Scholar] [CrossRef] [PubMed]
- Patel, D.R.; Neelakantan, M.; Pandher, K.; Merrick, J. Cerebral palsy in children: A clinical overview. Transl. Pediatr. 2020, 9, S125–S135. [Google Scholar] [CrossRef] [PubMed]
- Wallard, L.; Dietrich, G.; Kerlirzin, Y.; Bredin, J. Robotic-assisted gait training improves walking abilities in diplegic children with cerebral palsy. Eur. J. Paediatr. Neurol. 2017, 21, 557–564. [Google Scholar] [CrossRef]
- Hussain, S.; Xie, S.Q.; Liu, G. Robot assisted treadmill training: Mechanisms and training strategies. Med. Eng. Phys. 2011, 33, 527–533. [Google Scholar] [CrossRef] [PubMed]
- Lotze, M.; Braun, C.; Birbaumer, N.; Anders, S.; Cohen, L.G. Motor learning elicited by voluntary drive. Brain 2003, 126, 866–872. [Google Scholar] [CrossRef] [PubMed]
- Shideler, B.L.; Bulea, T.C.; Chen, J.; Stanley, C.J.; Gravunder, A.J.; Damiano, D.L. Toward a hybrid exoskeleton for crouch gait in children with cerebral palsy: Neuromuscular electrical stimulation for improved knee extension. J. Neuroeng. Rehabil. 2020, 17, 121. [Google Scholar] [CrossRef] [PubMed]
- Wu, Y.-N.; Hwang, M.; Ren, Y.; Gaebler-Spira, D.; Zhang, L.-Q. Combined passive stretching and active movement rehabilitation of lower-limb impairments in children with cerebral palsy using a portable robot. Neurorehabil. Neural Repair 2011, 25, 378–385. [Google Scholar] [CrossRef] [PubMed]
- Chen, K.; Wu, Y.-N.; Ren, Y.; Liu, L.; Gaebler-Spira, D.; Tankard, K.; Lee, J.; Song, W.; Wang, M.; Zhang, L.-Q. Home-Based Versus Laboratory-Based Robotic Ankle Training for Children With Cerebral Palsy: A Pilot Randomized Comparative Trial. Arch. Phys. Med. Rehabil. 2016, 97, 1237–1243. [Google Scholar] [CrossRef] [PubMed]
- Al-Quraishi, M.S.; Ishak, A.J.; Ahmad, S.A.; Hasan, M.K.; Al-Qurishi, M.; Ghapanchizadeh, H.; Alamri, A. Classification of ankle joint movements based on surface electromyography signals for rehabilitation robot applications. Med. Biol. Eng. Comput. 2017, 55, 747–758. [Google Scholar] [CrossRef] [PubMed]
- Piccinini, L.; Cimolin, V.; Galli, M.; Berti, M.; Crivellini, M.; Turconi, A.C. Quantification of energy expenditure during gait in children affected by cerebral palsy. Eur. Medicophys. 2007, 43, 7–12. [Google Scholar]
- Orekhov, G.; Fang, Y.; Luque, J.; Lerner, Z.F. Ankle Exoskeleton Assistance Can Improve Over-Ground Walking Economy in Individuals With Cerebral Palsy. IEEE Trans. Neural Syst. Rehabil. Eng. 2020, 28, 461–467. [Google Scholar] [CrossRef] [PubMed]
- Lerner, Z.F.; Harvey, T.A.; Lawson, J.L. A Battery-Powered Ankle Exoskeleton Improves Gait Mechanics in a Feasibility Study of Individuals with Cerebral Palsy. Ann. Biomed. Eng. 2019, 47, 1345–1356. [Google Scholar] [CrossRef]
- Farris, R.J.; Quintero, H.A.; Murray, S.A.; Ha, K.H.; Hartigan, C.; Goldfarb, M. A preliminary assessment of legged mobility provided by a lower limb exoskeleton for persons with paraplegia. IEEE Trans. Neural Syst. Rehabil. Eng. 2014, 22, 482–490. [Google Scholar] [CrossRef]
- Kamp, F.A.; Lennon, N.; Holmes, L.; Dallmeijer, A.J.; Henley, J.; Miller, F. Energy cost of walking in children with spastic cerebral palsy: Relationship with age, body composition and mobility capacity. Gait Posture 2014, 40, 209–214. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| RR Group (n = 18) | SRE Group (n = 17) | p-Value | |
|---|---|---|---|
| Male, n (%) | 9 (50) | 11 (64.7) | 0.38 |
| Age, (year) * | 5.4 (2.0) | 5.8 (1.8) | 0.45 |
| Height (cm) * | 113.4 (13.9) | 116.7 (12.7) | 0.41 |
| Weight (kg) * | 22.5 (6.1) | 23.1 (5.0) | 0.33 |
| Use of a walking aid, n (%) | 4 (22) | 3 (18) | 0.74 |
| SCP | |||
| unilateral | 10 | 9 | 0.88 |
| bilateral | 8 | 8 | |
| GMFCS | |||
| Level I | 5 | 6 | 0.54 |
| Level II | 9 | 7 | |
| Level III | 4 | 4 |
| Variables | RR Group (n = 18) | SRE Group (n = 17) |
|---|---|---|
| 10MWT (m/min) | ||
| Pre | 24.7 (5.8) | 24.9 (5.9) |
| Post | 27.9 (6.5) ** | 34.9 (5.0) ** |
| % Post-pre > MCID (0.14 m/s) | - | 20% |
| 6MWT (m) | ||
| Pre | 138.6 (35.2) | 144.5 (35.1) |
| Post | 160.3 (35.1) ** | 201.3 (44.1) ** |
| % Post-pre > MCID (46 m) | - | 23% |
| GMFM-D | ||
| Pre | 20.6 (10.4) | 25.7 (9.4) |
| Post | 24.3 (10.3) ** | 31.7 (6.9) ** |
| % Post-pre > MCID (1.8) | 107% | 233% |
| GMFM-E | ||
| Pre | 28.5 (16.7) | 33.9 (19.2) |
| Post | 32.5 (16.8) ** | 41.1 (18.2) ** |
| % Post-pre > MCID (2.6) | 54% | 169% |
| PBS | ||
| Pre | 35.0 (23.3) | 34.0 (21.5) |
| Post | 37.0 (24.3) * | 39.0 (16.5) ** |
| MAS | ||
| Pre | 2.1 (1.1) | 2.1 (1.1) |
| Post | 1.4 (1.1) ** | 1.3 (0.8) ** |
| PCI (beats/m) | ||
| Pre | 1.0 (0.2) | 1.0 (0.2) |
| Post | 0.6 (0.1) ** | 0.3 (0.1) ** |
| Outcome Measures | SRE Group vs. RR Group |
|---|---|
| 10MWT (m/min) | +6.78 (5.74–7.83) ** [0.845] |
| 6MWT (m) | +34.42 (28.84–39.99) ** [0.832] |
| GMFM-D | +2.98 (1.45–4.51) ** [0.330] |
| GMFM-E | +3.35 (2.14–4.57) ** [0.497] |
| PBS | +4.80 (3.17–6.43) ** [0.530] |
| MAS | −1.26 (0.84–1.68) ** [0.537] |
| PCI (beats/m) | −0.31 (−0.32–−0.25) ** [0.733] |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hui, Z.; Qi, W.; Zhang, Y.; Wang, M.; Zhang, J.; Li, D.; Zhu, D. Efficacy of a Soft Robotic Exoskeleton to Improve Lower Limb Motor Function in Children with Spastic Cerebral Palsy: A Single-Blinded Randomized Controlled Trial. Brain Sci. 2024, 14, 425. https://doi.org/10.3390/brainsci14050425
Hui Z, Qi W, Zhang Y, Wang M, Zhang J, Li D, Zhu D. Efficacy of a Soft Robotic Exoskeleton to Improve Lower Limb Motor Function in Children with Spastic Cerebral Palsy: A Single-Blinded Randomized Controlled Trial. Brain Sciences. 2024; 14(5):425. https://doi.org/10.3390/brainsci14050425
Chicago/Turabian StyleHui, Zhichong, Weihang Qi, Yi Zhang, Mingmei Wang, Jiamei Zhang, Dong Li, and Dengna Zhu. 2024. "Efficacy of a Soft Robotic Exoskeleton to Improve Lower Limb Motor Function in Children with Spastic Cerebral Palsy: A Single-Blinded Randomized Controlled Trial" Brain Sciences 14, no. 5: 425. https://doi.org/10.3390/brainsci14050425