Social Cognition and Oxytocin in Huntington’s Disease: New Insights

 ,
,
Abstract
:1. Introduction
2. Material and Methods
2.1. Study Population
2.2. Measurement of Oxytocin Plasma Levels
Chemicals
2.3. Blood Collection and Plasma Extraction
2.4. Plasma Oxytocin Enzyme-Immunoassay (EIA)
2.5. Cognitive and Neuropsychological Evaluation
2.6. Statistical Analysis
3. Results
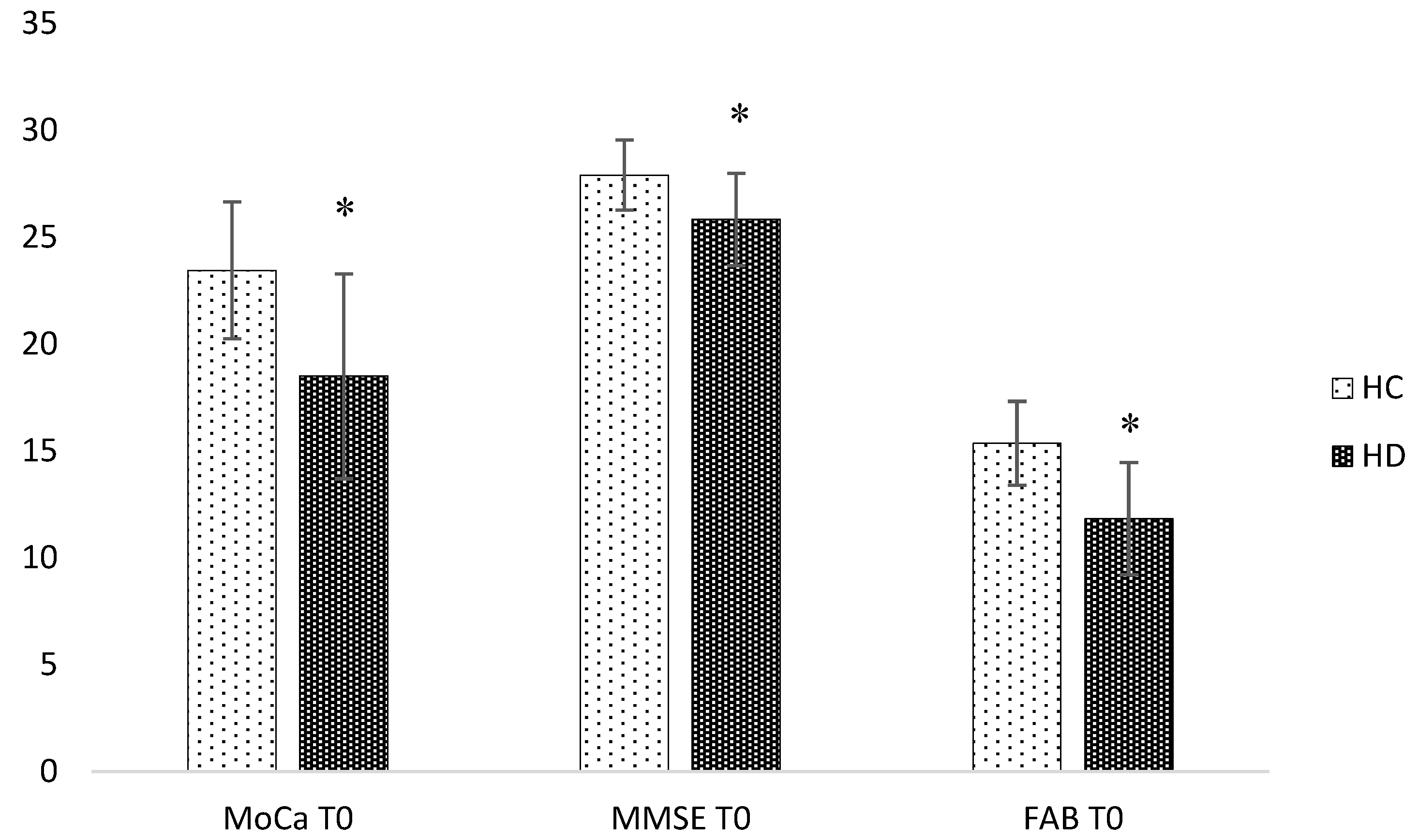
3.1. Baseline Analysis
3.2. Longitudinal Analysis
4. Discussion
Author Contributions
Funding
Conflicts of Interest
References
- Ross, C.A.; Tabrizi, S.J. Huntington’s disease: From molecular pathogenesis to clinical treatment. Lancet Neurol. 2011, 10, 83–98. [Google Scholar] [CrossRef]
- Craufurd, D.; Snowden, J.S. Neuropsychological and neuropsychiatric aspects of Huntington’s disease. In Huntington’s Disease; Bates, G., Harper, P.S., Jones, L., Eds.; Oxfor University Press: Oxford, UK, 2002; pp. 62–91. [Google Scholar]
- Montoya, A.; Pelletier, M.; Menear, M.; Duplessis, E.; Richer, F.; Lepage, M. Episodic memory impairment in Huntington’s disease: A meta-analysis. Neuropsychologia 2006, 44, 1984–1994. [Google Scholar] [CrossRef] [PubMed]
- Henley, S.M.; Novak, M.J.; Frost, C.; King, J.; Tabrizi, S.J.; Warren, J.D. Emotion recognition in Huntington’s disease: A systematic review. Neurosci. Biobehav. Rev. 2012, 36, 237–253. [Google Scholar] [CrossRef] [PubMed]
- Kordsachia, C.C.; Labuschagne, I.; Stout, J.C. Beyond emotion recognition deficits: A theory guided analysis of emotion processing in Huntington’s disease. Neurosci. Biobehav. Rev. 2017, 73, 276–292. [Google Scholar] [CrossRef] [PubMed]
- Labuschagne, I.; Jones, R.; Callaghan, J.; Whitehead, D.; Dumas, E.M.; Say, M.J.; Hart, E.P.; Justo, D.; Coleman, A.; Dar Santos, R.C.; et al. Emotional face recognition deficits and medication effects in pre-manifest through stage-II Huntington’s disease. Psychiatry Res. 2013, 207, 118–126. [Google Scholar] [CrossRef] [PubMed]
- Calder, A.J.; Keane, J.; Young, A.W.; Lawrence, A.D.; Mason, S.; Barker, R.A. The relation between anger and different forms of disgust: Implications for emotion recognition impairments in Huntington’s disease. Neuropsychologia 2010, 48, 2719–2729. [Google Scholar] [CrossRef] [PubMed]
- De Gelder, B.; Van den Stock, J.; Balaguer Rde, D.; Bachoud-Lévi, A.C. Huntington’s disease impairs recognition of angry and instrumental body language. Neuropsychologia 2008, 46, 369–373. [Google Scholar] [CrossRef] [PubMed]
- Frith, C.D.; Frith, U. Mechanisms of social cognition. Ann. Rev. Psychol. 2012, 63, 287–313. [Google Scholar] [CrossRef] [PubMed]
- Adjeroud, N.; Besnard, J.; El Massioui, N.; Verny, C.; Prudean, A.; Scherer, C.; Gohier, B.; Bonneau, D.; Allain, P. Theory of mind and empathy in preclinical and clinical Huntington’s disease. Soc. Cogn. Affect. Neurosci. 2016, 11, 89–99. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vonsattel, J.P.; Myers, R.H.; Stevens, T.J.; Ferrante, R.J.; Bird, E.D.; Richardson, E.P., Jr. Neuropathological classification of Huntington’s disease. J. Neuropathol. Exp. Neurol. 1985, 44, 559–577. [Google Scholar] [CrossRef] [PubMed]
- Gabery, S.; Murphy, K.; Schultz, K.; Loy, C.T.; McCusker, E.; Kirik, D.; Halliday, G.; Petersén, A. Changes in key hypothalamic neuropeptide populations in Huntington disease revealed by neuropathological analyses. Acta Neuropathol. 2010, 120, 777–788. [Google Scholar] [CrossRef] [PubMed]
- Heinrichs, M.; Von Dawans, B.; Domes, G. Oxytocin, vasopressin, and human social behavior. Front. Neuroendocrinol. 2009, 30, 548–557. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Veening, J.G.; De Jonget, T.; Barendregt, H.P. Oxytocin-messages via the cerebrospinal fluid: Behavioural effects; a review. Physiol. Behav. 2010, 101, 193–210. [Google Scholar] [CrossRef] [PubMed]
- Galbally, M.; Lewis, A.J.; Van Ijzendoorn, M.; Permezel, M. The role of oxytocin in mother-infant relations: A systematic review of human studies. Harv. Rev. Psychiatry 2011, 19, 1–14. [Google Scholar] [CrossRef] [PubMed]
- Insel, T.R. The challenge of translation in social neuroscience: A review of oxytocin, vasopressin, and affiliative behaviour. Neuron 2010, 65, 768–779. [Google Scholar] [CrossRef] [PubMed]
- Kendrick, K.M. Oxytocin, motherhood and bonding. Exp. Physiol. 2000, 85, 111s–124s. [Google Scholar] [CrossRef] [PubMed]
- Sue Carter, C. Neuroendocrine perspectives on social attachment and love. Psychoneuroendocrinology 1998, 23, 779–818. [Google Scholar] [CrossRef]
- Guastella, A.J.; MacLeod, C. A critical review of the influence of oxytocin nasal spray on social cognition in humans: Evidence and future directions. Horm. Behav. 2012, 61, 410–418. [Google Scholar] [CrossRef] [PubMed]
- Hurlemann, R.; Scheele, D. Dissecting the role of oxytocin in the formation and loss of social relationships. Biol. Psychiatry 2015, 79, 185–193. [Google Scholar] [CrossRef] [PubMed]
- Nave, G.; Camerer, C.; McCullough, M. Does oxytocin increase trust in humans? A critical review of research. Perspect. Psychol. Sci. 2015, 10, 772–789. [Google Scholar] [CrossRef] [PubMed]
- Kavaliers, M.; Colwell, D.D.; Choleris, E.; Agmo, A.; Muglia, L.J.; Ogawa, S.; Pfaff, D.W. Impaired discrimination of and aversion to parasitized male odors by female oxytocin knockout mice. Gene Brain Behav. 2003, 2, 220–230. [Google Scholar] [CrossRef] [Green Version]
- Ferguson, J.N.; Aldag, J.M.; Insel, T.R.; Young, L.J. Oxytocin in the medial amygdale is essential for social recognition in the mouse. J. Neurosci. 2001, 21, 8278–8285. [Google Scholar] [CrossRef] [PubMed]
- Labuschagne, I.; Poudel, G.; Kordsachia, C.; Wu, Q.; Thomson, H.; Georgiou-Karistianis, N.; Stout, J.C. Oxytocin selectively modulates brain processing of disgust in Huntington’s disease gene carriers. Prog. Neuro-Psychoph. 2018, 81, 11–16. [Google Scholar] [CrossRef] [PubMed]
- Betti, L.; Palego, L.; Unti, E.; Mazzucchi, S.; Kiferle, L.; Palermo, G.; Bonuccelli, U.; Giannaccini, G.; Ceravolo, R. Brain-Derived Neurotrophic Factor (BDNF) and Serotonin Transporter (SERT) in Platelets of Patients with Mild Huntington’s Disease: Relationships with Social Cognition Symptoms. Arch. Ital Biol. 2018, 156, 27–39. [Google Scholar] [PubMed]
- Huntington Study Group. Unified Huntington’s Disease Rating Scale: reliability and consistency. Mov. Disord. 1996, 11, 136–142. [Google Scholar] [CrossRef] [PubMed]
- Blazer, D. Neurocognitive disorders in DSM-5. Am. J. Psychiatry 2013, 170, 585–587. [Google Scholar] [CrossRef] [PubMed]
- Shoulson, I.F.; Fahn, S. Huntington disease: Clinical care and evaluation. Neurology 1979, 29, 1–3. [Google Scholar] [CrossRef] [PubMed]
- Bazzichi, L.; Da Valle, Y.; Rossi, A.; Giacomelli, C.; Sernissi, F.; Giannaccini, G.; Betti, L.; Ciregia, F.; Giusti, L.; Scarpellini, P.; et al. A multidisciplinary approach to study the effects of balneotherapy and mud-bath therapy treatments on fibromyalgia. Clin. Exp. Rheumatol. 2013, 31, S111–S120. [Google Scholar] [PubMed]
- Folstein, M.F.; Folstein, S.E.; McHugh, P.R. “Mini-mental state”: A practical method for grading the cognitive state of patients for the clinician. J. Psychiatry Res. 1975, 12, 189–198. [Google Scholar] [CrossRef]
- Nasreddine, Z.S.; Phillips, N.A.; Bédirian, V.; Charbonneau, S.; Whitehead, V.; Collin, I.; Cummings, J.L.; Chertkow, H. The Montreal Cognitive Assessment, MoCA: A brief screening tool for mild cognitive impairment. J. Am. Geriatr. Soc. 2005, 53, 695–699. [Google Scholar] [CrossRef] [PubMed]
- Dubois, B.; Slachevsky, A.; Litvan, I.; Pillon, B. Frontal Assessment Battery (FAB). Neurology 2000, 55, 1621–1626. [Google Scholar] [CrossRef]
- Sartori, G.; Colombo, L.; Vallar, G.; Rusconi, M.L.; Pinarello, A. TIB Test di Intelligenza Breve per la Valutazione del Quoziente Intellettivo Attuale e Premorboso; Giornale dell’Ordine Nazionale degli Psicologi: Rome, Italy, 1997. [Google Scholar]
- Stone, V.E.; Baron-Cohen, S.; Knight, R.T. Frontal lobe contributions to theory of mind. Faux-pas task. J. Cogn. Neurosci. 1998, 10, 640–656. [Google Scholar] [CrossRef] [PubMed]
- Lundqvist, D.; Flykt, A.; Öhman, A. Karolinska Directed Emotional Faces—KDEF (CD ROM); Department of Clinical Neuroscience, Psychology section, Karolinska Institutet: Stockholm, Sweden, 1998. [Google Scholar]
- Prior, M.; Sartori, G.; Marchi, S. Cognizione Sociale E Comportamento: Uno Strumento Per La Misurazione; Domeneghini Editore: Padova, Italy, 2003. [Google Scholar]
- Happè, F.G.E. An Advanced test of theory of mind: understanding the story characters thoughts and feeling by able autistic, mentally handicapped and normal children and adults. J. Autism Dev. Disord. 1994, 24, 129–154. [Google Scholar] [CrossRef] [PubMed]
- Inoue, Y.; Tonooka, Y.; Yamada, K.; Kanba, S. Deficiency of theory of mind in patients with remitted mood disorder. J. Affect. Disord. 2004, 82, 403–409. [Google Scholar] [CrossRef] [PubMed]
- Allain, P.; Havet-Thomassin, V.; Verny, C.; Gohier, B.; Lancelot, C.; Besnard, J.; Fasotti, L.; Le Gall, D. Evidence for Deficits on Different Components of Theory of Mind in Huntington’s Disease. Neuropsychology 2011, 25, 741–751. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sprengelmeyer, R.; Young, A.W.; Calder, A.J.; Karnat, A.; Lange, H.; Hömberg, V.; Perrett, D.I.; Rowland, D. Loss of Disgust-perception of faces and emotions in Huntingon’s disease. Brain 1996, 119, 1647–1665. [Google Scholar] [CrossRef] [PubMed]
- Mitchell, I.J.; Heims, H.; Neville, E.A.; Rickards, H. Huntingtons disease patients show impaired perception of disgust in the gustatory and olfactory modalities. J. Neuropsychiatry Clin. Neurosci. 2005, 17, 119–121. [Google Scholar] [CrossRef] [PubMed]
- Hayes, C.J.; Stevenson, R.J.; Coltheart, M. Disgust and Huntington’s disease. Neuropsychologia 2007, 45, 1135–1151. [Google Scholar] [CrossRef] [PubMed]
- Soneson, C.; Fontes, M.; Zhou, Y.; Denisov, V.; Paulsen, J.S.; Kirik, D.; Petersén, A.; Huntington Study Group PREDICT-HD investigators. Early changes in the hypothalamic region in prodromal Huntington’s disease revealed by MRI analysis. Neurobiol. Dis. 2010, 40, 531–543. [Google Scholar] [CrossRef] [PubMed]
- Gabery, S.; Halliday, G.; Kirik, D.; Englund, E.; Petersén, Å. Selective loss of oxytocin and vasopressin in the hypothalamus in early Huntington disease: A case study. Neuropathol. Appl. Neurol. 2015, 41, 843–848. [Google Scholar] [CrossRef] [PubMed]
- Guyton, A.C.; Hall, J.E. Fisiologia Medica; Piccin: Padua, Italy, 2001. [Google Scholar]
- McCarthy, M.M.; Altemus, M. Central nervous system actions of oxytocin and modulation of behavior in humans. Mol. Med. Today 1997, 3, 269–275. [Google Scholar] [CrossRef]
- Mens, W.B.; Witter, A.; Van Wimersma Greidanus, T.B. Penetration of neurohypophyseal hormones from plasma into cerebrospinal fluid (CSF): Half-times of disappearance of these neuropeptides from CSF. Brain Res. 1983, 262, 143–149. [Google Scholar] [CrossRef]
- Kagerbauer, S.M.; Martin, J.; Schuster, T.; Blobner, M.; Kochs, E.F.; Landgraf, R. Plasma oxytocin and vasopressin do not predict neuropeptide concentrations in human cerebrospinal fluid. J. Neuroendocronol. 2013, 25, 668–673. [Google Scholar] [CrossRef] [PubMed]
- Cochran, D.; Fallon, D.; Hill, M.; Frazier, J.A. The role of oxytocin in psychiatric disorders: A review of biological and therapeutic research findings. Harvard Rev. Psychiatry 2013, 21, 219–247. [Google Scholar] [CrossRef] [PubMed]
- Modahl, C.; Green, L.; Fein, D.; Morris, M.; Waterhouse, L.; Feinstein, C.; Levin, H. Plasma oxytocin levels in autistic children. Biol. Psychiatry 1998, 43, 270–277. [Google Scholar] [CrossRef]
- Goldman, M.; Marlow-O’Connor, M.; Torres, I.; Carter, C.S. Diminished plasma oxytocin in schizophrenic patients with neuroendocrine dysfunction and emotional deficits. Schizophr. Res. 2008, 98, 247–255. [Google Scholar] [CrossRef] [PubMed]
- Marazziti, D.; Dell’Osso, B.; Baroni, S.; Mungai, F.; Catena, M.; Rucci, P.; Albanese, F.; Giannaccini, G.; Betti, L.; Fabbrini, L.; et al. A relationship between oxytocin and anxiety of romantic attachment. Clin. Pract. Epidemiol. Ment. Health 2006, 2, 28. [Google Scholar]
- Savaskan, E.; Ehrhardt, R.; Schulz, A.; Walter, M.; Schächinger, H. Post-learning intranasal oxytocin modulates human memory for facial identity. Psychoneuroendocrinology 2008, 33, 368–374. [Google Scholar] [CrossRef] [PubMed]
- Boccia, M.L.; Petrusz, P.; Suzuki, K.; Marson, L.; Pedersen, C.A. Immunohistochemical localization of oxytocin receptors in human brain. Neuroscience 2013, 253, 155–164. [Google Scholar] [CrossRef] [PubMed]
- Kirsch, P.; Esslinger, C.; Chen, Q.; Mier, D.; Lis, S.; Siddhanti, S.; Gruppe, H.; Mattay, V.S.; Gallhofer, B.; Meyer-Lindenberg, A. Oxytocin modulates neural circuitry for social cognition and fear in humans. J. Neurosci. 2005, 25, 11489–11493. [Google Scholar] [CrossRef] [PubMed]
- Bruene, M.; Blank, K.; Witthaus, H.; Saft, C. “Theory of Mind” is impaired in Huntington’s Disease? Mov. Disord. 2011, 26, 671–678. [Google Scholar] [CrossRef] [PubMed]
- Larsen, I.U.; Vinther-Jensen, T.; Nielsen, J.E.; Gade, A.; Vogel, A. Social Cognition, Executive Functions and Self-Report of Psychological Distress in Huntington’s Disease. PLoS Curr. 2016, 8, 1–20. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Demographic Characteristics | HD(n13) | HC(n11) |
|---|---|---|
| Sex | 4F,9M | 3F,8M |
| Age(years) | 61.08 ± 11.90 (45–78 years) | 65.45 ± 10.34 (45–78 years) |
| Educational level(years) | 8.66 ± 3.44 (5–13 years) | 8.18 ± 3.91 (5–13 years) |
| FP/N_T1 | Str-Stor_T1 | KDEF_Tot_T1 | Disg_KDED_T1 | Neutr_KDEF_T1 | |
|---|---|---|---|---|---|
| OT_T0 | p = 0.03 * | - | - | - | - |
| MOCa_T0 | - | p = 0.001 ** | p = 0.007 ** | p = 0.003 ** | |
| MMSE_T0 | - | p = 0.01 * | p = 0.03 * | - | p = 0.04 * |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Unti, E.; Mazzucchi, S.; Frosini, D.; Pagni, C.; Tognoni, G.; Palego, L.; Betti, L.; Miraglia, F.; Giannaccini, G.; Ceravolo, R. Social Cognition and Oxytocin in Huntington’s Disease: New Insights. Brain Sci. 2018, 8, 161. https://doi.org/10.3390/brainsci8090161
Unti E, Mazzucchi S, Frosini D, Pagni C, Tognoni G, Palego L, Betti L, Miraglia F, Giannaccini G, Ceravolo R. Social Cognition and Oxytocin in Huntington’s Disease: New Insights. Brain Sciences. 2018; 8(9):161. https://doi.org/10.3390/brainsci8090161
Chicago/Turabian StyleUnti, Elisa, Sonia Mazzucchi, Daniela Frosini, Cristina Pagni, Gloria Tognoni, Lionella Palego, Laura Betti, Fabiana Miraglia, Gino Giannaccini, and Roberto Ceravolo. 2018. "Social Cognition and Oxytocin in Huntington’s Disease: New Insights" Brain Sciences 8, no. 9: 161. https://doi.org/10.3390/brainsci8090161