No Reported Renal Stones with Intravenous Vitamin C Administration: A Prospective Case Series Study



Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design, Setting and Participants
2.2. Study Size
2.3. Baseline Data
2.4. Treatment
2.5. Follow-Up
2.6. Data Sources and Measurement
2.7. Statistical Analysis
3. Results
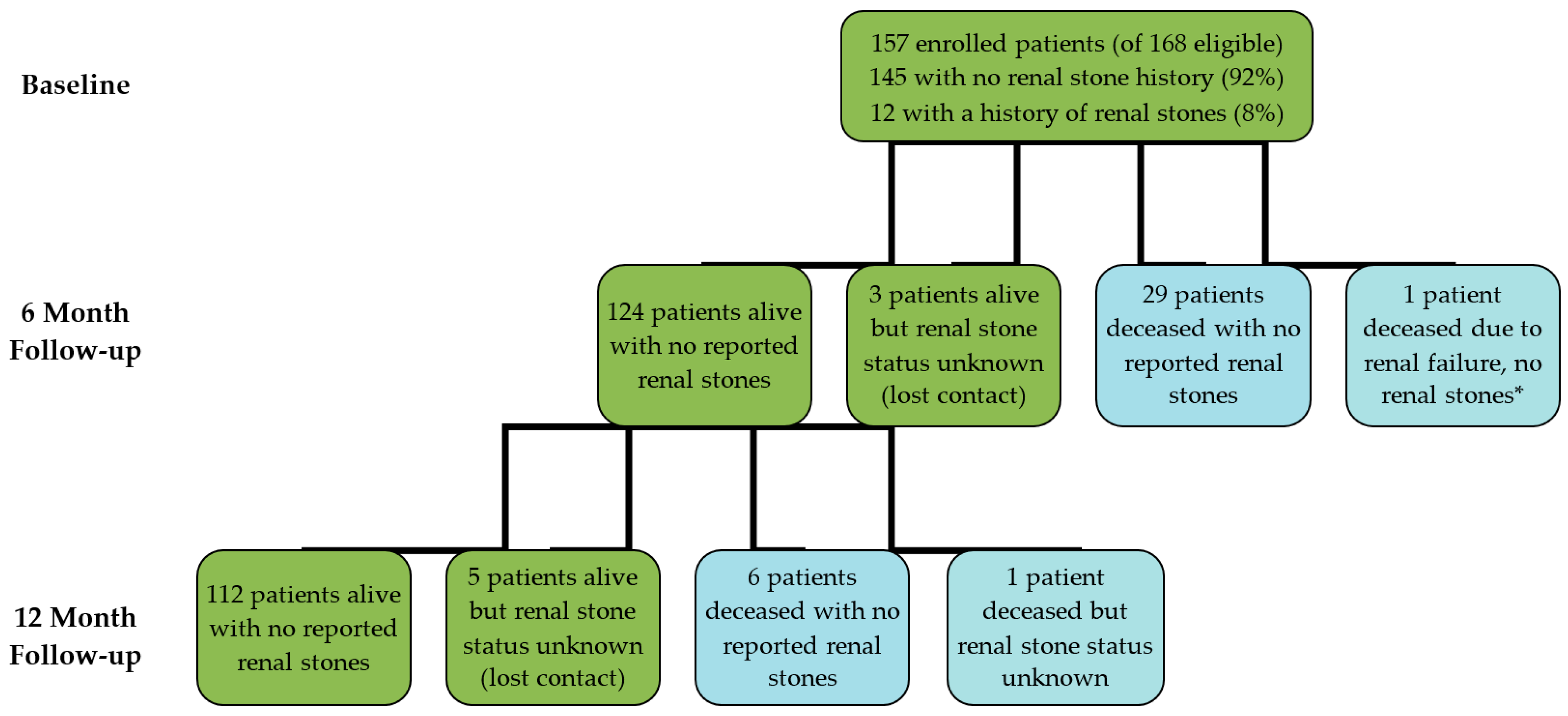
3.1. Participants
3.2. Outcome Data
3.2.1. Reported Renal Stones
3.2.2. Renal function tests
3.3. Patient A Case Report
4. Discussion
5. Conclusions
Author Contributions
Acknowledgments
Conflicts of Interest
References
- Padayatty, S.J.; Sun, A.Y.; Chen, Q.; Espey, M.G.; Drisko, J.; Levine, M. Vitamin C: Intravenous use by complementary and alternative medicine practitioners and adverse effects. PLoS ONE 2010, 5, e11414. [Google Scholar] [CrossRef] [PubMed]
- Parrow, N.L.; Leshin, J.A.; Levine, M. Parenteral ascorbate as a cancer therapeutic: A reassessment based on pharmacokinetics. Antioxid. Redox Signal 2013, 19, 2141–2156. [Google Scholar] [CrossRef] [PubMed]
- Mikirova, N.A.; Casciari, J.J.; Hunninghake, R.E.; Riordan, N.H. Intravenous ascorbic acid protocol for cancer patients: Scientific rationale, pharmacology, and clinical experience. Funct. Foods Health Dis. 2013, 3, 344–366. [Google Scholar]
- Carr, A.C.; Vissers, M.C.M.; Cook, J.S. The effect of intravenous vitamin C on cancer- and chemotherapy-related fatigue and quality of life. Front. Oncol. 2014, 4, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Carr, A.C.; Shaw, G.M.; Fowler, A.A.; Natarajan, R. Ascorbate-dependent vasopressor synthesis: A rationale for vitamin C administration in severe sepsis and septic shock? Crit. Care 2015, 19, e418. [Google Scholar] [CrossRef] [PubMed]
- Fukushima, R.; Yamazaki, E. Vitamin C requirement in surgical patients. Curr. Opin. Clin. Nutr. Metab. Care 2010, 13, 669–676. [Google Scholar] [CrossRef] [PubMed]
- Padayatty, S.J.; Sun, H.; Wang, Y.; Riordan, H.D.; Hewitt, S.M.; Katz, A.; Wesley, R.A.; Levine, M. Vitamin C pharmacokinetics: Implications for oral and intravenous use. Ann. Intern. Med. 2004, 140, 533–537. [Google Scholar] [CrossRef] [PubMed]
- Mastrangelo, D.; Pelosi, E.; Castelli, G.; Lo-Coco, F.; Testa, U. Mechanisms of anti-cancer effects of ascorbate: Cytotoxic activity and epigenetic modulation. Blood Cells Mol. Dis. 2017, 69, 57–64. [Google Scholar] [CrossRef] [PubMed]
- Kuiper, C.; Vissers, M.C.; Hicks, K.O. Pharmacokinetic modeling of ascorbate diffusion through normal and tumor tissue. Free Radic. Biol Med. 2014, 77, 340–352. [Google Scholar] [CrossRef] [PubMed]
- Kuiper, C.; Vissers, M.C. Ascorbate as a co-factor for Fe- and 2-oxoglutarate dependent dioxygenases: Physiological activity in tumor growth and progression. Front. Oncol. 2014, 4, 359. [Google Scholar] [CrossRef] [PubMed]
- Carr, A.C.; Maggini, S. Vitamin C and immune function. Nutrients 2017, 9, 1211. [Google Scholar] [CrossRef] [PubMed]
- McAllister, C.J.; Scowden, E.B.; Dewberry, F.L.; Richman, A. Renal failure secondary to massive infusion of vitamin C. JAMA 1984, 252, 1684. [Google Scholar] [CrossRef] [PubMed]
- Lawton, J.M.; Conway, L.T.; Crosson, J.T.; Smith, C.L.; Abraham, P.A. Acute oxalate nephropathy after massive ascorbic acid administration. Arch. Intern. Med. 1985, 145, 950–951. [Google Scholar] [CrossRef] [PubMed]
- Wong, K.; Thomson, C.; Bailey, R.R.; McDiarmid, S.; Gardner, J. Acute oxalate nephropathy after a massive intravenous dose of vitamin C. Aust. N. Z. J. Med. 1994, 24, 410–411. [Google Scholar] [CrossRef] [PubMed]
- Cossey, L.N.; Rahim, F.; Larsen, C.P. Oxalate nephropathy and intravenous vitamin C. Am. J. Kidney Dis. 2013, 61, 1032–1035. [Google Scholar] [CrossRef] [PubMed]
- Story, D.A.; Ronco, C.; Bellomo, R. Trace element and vitamin concentrations and losses in critically ill patients treated with continuous venovenous hemofiltration. Crit. Care Med. 1999, 27, 220–223. [Google Scholar] [CrossRef] [PubMed]
- Marik, P.E.; Khangoora, V.; Rivera, R.; Hooper, M.H.; Catravas, J. Hydrocortisone, vitamin C, and thiamine for the treatment of severe sepsis and septic shock: A retrospective before-after study. Chest 2017, 151, 1229–1238. [Google Scholar] [CrossRef] [PubMed]
- Dennis, J.M.; Witting, P.K. Protective role for antioxidants in acute kidney disease. Nutrients 2017, 9, 718. [Google Scholar] [CrossRef] [PubMed]
- Ma, Y.; Chapman, J.; Levine, M.; Polireddy, K.; Drisko, J.; Chen, Q. High-dose parenteral ascorbate enhanced chemosensitivity of ovarian cancer and reduced toxicity of chemotherapy. Sci. Transl. Med. 2014, 6, 222ra18. [Google Scholar] [CrossRef] [PubMed]
- Massey, L.K.; Liebman, M.; Kynast-Gales, S.A. Ascorbate increases human oxaluria and kidney stone risk. J. Nutr. 2005, 135, 1673–1677. [Google Scholar] [CrossRef] [PubMed]
- Traxer, O.; Huet, B.; Poindexter, J.; Pak, C.Y.; Pearle, M.S. Effect of ascorbic acid consumption on urinary stone risk factors. J. Urol. 2003, 170 Pt 1, 397–401. [Google Scholar] [CrossRef] [PubMed]
- Robitaille, L.; Mamer, O.A.; Miller, W.H., Jr.; Levine, M.; Assouline, S.; Melnychuk, D.; Rousseau, C.; Hoffer, L.J. Oxalic acid excretion after intravenous ascorbic acid administration. Metabolism 2009, 58, 263–269. [Google Scholar] [CrossRef] [PubMed]
- Riordan, H.D.; Casciari, J.J.; Gonzalez, M.J.; Riordan, N.H.; Miranda-Massari, J.R.; Taylor, P.; Jackson, J.A. A pilot clinical study of continuous intravenous ascorbate in terminal cancer patients. P. R. Health Sci. J. 2005, 24, 269–276. [Google Scholar] [PubMed]
- Evans, K.; Costabile, R.A. Time to development of symptomatic urinary calculi in a high risk environment. J. Urol. 2005, 173, 858–861. [Google Scholar] [CrossRef] [PubMed]
- Shepard, C.L.; Wang, G.; Hopson, B.D.; Bunt, E.B.; Assimos, D.G. Urinary tract stone development in patients with myelodysplasia subjected to augmentation cystoplasty. Rev. Urol. 2017, 19, 11–15. [Google Scholar] [PubMed]
- Kok, D.J.; Boellaard, W.; Ridwan, Y.; Levchenko, V.A. Timelines of the “free-particle” and “fixed-particle” models of stone-formation: Theoretical and experimental investigations. Urolithiasis 2017, 45, 33–41. [Google Scholar] [CrossRef] [PubMed]
- Stephenson, C.M.; Levin, R.D.; Spector, T.; Lis, C.G. Phase I clinical trial to evaluate the safety, tolerability, and pharmacokinetics of high-dose intravenous ascorbic acid in patients with advanced cancer. Cancer Chemother. Pharmacol. 2013, 72, 139–146. [Google Scholar] [CrossRef] [PubMed]
- Ministry of Health. Managing Chronic Kidney Disease in Primary Care: A National Consensus Statement; Ministry of Health: Wellington, New Zealand, 2015.
- Chronic Kidney Disease (CKD): Management in General Practice. 2014. Available online: https://www.kidneys.co.nz/resources/file/ckd_management_in_general_practice._2014_version.pdf (accessed on 16 March 2018).
- Reinhard, M.; Erlandsen, E.J.; Randers, E. Biological variation of cystatin C and creatinine. Scand. J. Clin. Lab. Investig. 2009, 69, 831–836. [Google Scholar] [CrossRef] [PubMed]
- Auer, B.L.; Auer, D.; Rodgers, A.L. Relative hyperoxaluria, crystalluria and haematuria after megadose ingestion of vitamin C. Eur. J. Clin. Investig. 1998, 28, 695–700. [Google Scholar] [CrossRef]
- Gerster, H. No contribution of ascorbic acid to renal calcium oxalate stones. Ann. Nutr. Metab. 1997, 41, 269–282. [Google Scholar] [CrossRef] [PubMed]
- Simon, J.A.; Hudes, E.S. Relation of serum ascorbic acid to serum vitamin B12, serum ferritin, and kidney stones in US adults. Arch. Intern. Med. 1999, 159, 619–624. [Google Scholar] [CrossRef] [PubMed]
- Curhan, G.C.; Willett, W.C.; Rimm, E.B.; Stampfer, M.J. A prospective study of the intake of vitamins C and B6, and the risk of kidney stones in men. J. Urol. 1996, 155, 1847–1851. [Google Scholar] [CrossRef]
- Curhan, G.C.; Willett, W.C.; Speizer, F.E.; Stampfer, M.J. Intake of vitamins B6 and C and the risk of kidney stones in women. J. Am. Soc. Nephrol. 1999, 10, 840–845. [Google Scholar] [PubMed]
- Ferraro, P.M.; Curhan, G.C.; Gambaro, G.; Taylor, E.N. Total, dietary, and supplemental vitamin C intake and risk of incident kidney stones. Am. J. Kidney Dis. 2016, 67, 400–407. [Google Scholar] [CrossRef] [PubMed]
- Thomas, L.D.; Elinder, C.G.; Tiselius, H.G.; Wolk, A.; Akesson, A. Ascorbic acid supplements and kidney stone incidence among men: A prospective study. JAMA Intern. Med. 2013, 173, 386–388. [Google Scholar] [CrossRef] [PubMed]
- Taylor, E.N.; Stampfer, M.J.; Curhan, G.C. Dietary factors and the risk of incident kidney stones in men: New insights after 14 years of follow-up. J. Am. Soc. Nephrol. 2004, 15, 3225–3232. [Google Scholar] [CrossRef] [PubMed]
- Pullar, J.M.; Carr, A.C.; Vissers, M.C. Vitamin C supplementation and kidney stone risk. N. Z. Med. J. 2013, 126, 133–134. [Google Scholar] [PubMed]
- Lamarche, J.; Nair, R.; Peguero, A.; Courville, C. Vitamin C-induced oxalate nephropathy. Int. J. Nephrol. 2011, 2011, 146927. [Google Scholar] [CrossRef] [PubMed]
- McHugh, G.J.; Graber, M.L.; Freebairn, R.C. Fatal vitamin C-associated acute renal failure. Anaesth Intensive Care 2008, 36, 585–588. [Google Scholar] [PubMed]
- Rathi, S.; Kern, W.; Lau, K. Vitamin C-induced hyperoxaluria causing reversible tubulointerstitial nephritis and chronic renal failure: A case report. J. Med. Case Rep. 2007, 1, 155. [Google Scholar] [CrossRef] [PubMed]
- Nasr, S.H.; Kashtanova, Y.; Levchuk, V.; Markowitz, G.S. Secondary oxalosis due to excess vitamin C intake. Kidney Int. 2006, 70, 1672. [Google Scholar] [CrossRef] [PubMed]
- Poulin, L.D.; Riopel, J.; Castonguay, V.; Mac-Way, F. Acute oxalate nephropathy induced by oral high-dose vitamin C alternative treatment. Clin. Kidney J. 2014, 7, 218. [Google Scholar] [CrossRef] [PubMed]
- Gurm, H.; Sheta, M.A.; Nivera, N.; Tunkel, A. Vitamin C-induced oxalate nephropathy: A case report. J. Community Hosp. Intern. Med. Perspect. 2012, 2. [Google Scholar] [CrossRef] [PubMed]
- Nankivell, B.J.; Murali, K.M. Images in clinical medicine. Renal failure from vitamin C after transplantation. N. Engl. J. Med. 2008, 358, e4. [Google Scholar] [CrossRef] [PubMed]
- Yaich, S.; Chaabouni, Y.; Charfeddine, K.; Zaghdane, S.; Kharrat, M.; Kammoun, K.; Makni, S.; Boudawara, T.; Hachicha, J. Secondary oxalosis due to excess vitamin C intake: A cause of graft loss in a renal transplant recipient. Saudi J. Kidney Dis. Transpl. 2014, 25, 113–116. [Google Scholar] [CrossRef] [PubMed]
- Colliou, E.; Mari, A.; Delas, A.; Delarche, A.; Faguer, S. Oxalate nephropathy following vitamin C intake within intensive care unit. Clin. Nephrol. 2017, 88, 354–358. [Google Scholar] [CrossRef] [PubMed]
- Mashour, S.; Turner, J.F., Jr.; Merrell, R. Acute renal failure, oxalosis, and vitamin C supplementation: A case report and review of the literature. Chest 2000, 118, 561–563. [Google Scholar] [CrossRef] [PubMed]
- Morgan, S.H.; Maher, E.R.; Purkiss, P.; Watts, R.W.; Curtis, J.R. Oxalate metabolism in end-stage renal disease: The effect of ascorbic acid and pyridoxine. Nephrol. Dial Transplant. 1988, 3, 28–32. [Google Scholar] [PubMed]
- Canavese, C.; Petrarulo, M.; Massarenti, P.; Berutti, S.; Fenoglio, R.; Pauletto, D.; Lanfranco, G.; Bergamo, D.; Sandri, L.; Marangella, M. Long-term, low-dose, intravenous vitamin C leads to plasma calcium oxalate supersaturation in hemodialysis patients. Am. J. Kidney Dis. 2005, 45, 540–549. [Google Scholar] [CrossRef] [PubMed]
- Costello, J.F.; Sadovnic, M.J.; Cottington, E.M. Plasma oxalate levels rise in hemodialysis patients despite increased oxalate removal. J. Am. Soc. Nephrol. 1991, 1, 1289–1298. [Google Scholar] [PubMed]
- Curhan, G.C. Epidemiology of stone disease. Urol. Clin. N. Am. 2007, 34, 287–293. [Google Scholar] [CrossRef] [PubMed]
- Lee, Y.H.; Huang, W.C.; Lu, C.M.; Tsai, J.Y.; Huang, J.K. Stone recurrence predictive score (SRPS) for patients with calcium oxalate stones. J. Urol. 2003, 170 Pt 1, 404–407. [Google Scholar] [CrossRef] [PubMed]
- Ljunghall, S.; Danielson, B.G. A prospective study of renal stone recurrences. Br. J. Urol. 1984, 56, 122–124. [Google Scholar] [CrossRef] [PubMed]
- Curhan, G.C.; Willett, W.C.; Rimm, E.B.; Stampfer, M.J. A prospective study of dietary calcium and other nutrients and the risk of symptomatic kidney stones. N. Engl. J. Med. 1993, 328, 833–838. [Google Scholar] [CrossRef] [PubMed]
- Curhan, G.C.; Willett, W.C.; Speizer, F.E.; Spiegelman, D.; Stampfer, M.J. Comparison of dietary calcium with supplemental calcium and other nutrients as factors affecting the risk for kidney stones in women. Ann. Intern. Med. 1997, 126, 497–504. [Google Scholar] [CrossRef] [PubMed]
- Bansal, A.D.; Hui, J.; Goldfarb, D.S. Asymptomatic nephrolithiasis detected by ultrasound. Clin. J. Am. Soc. Nephrol. 2009, 4, 680–684. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Characteristic | Total Cohort 1 | No History of Renal Stones | History of Renal Stones | p Value 2 |
|---|---|---|---|---|
| N (%) | 157 (100) 3 | 141 (90) | 12 (8) | |
| Mean age, years (range) | 54 (17–86) | 54 (17) | 58 (12) | 0.332 |
| Male/female, n | 62/95 | 53/88 | 9/3 | 0.038 |
| Mean number of IVC treatments, n (range) | 15 (1–119) | 14 (19) | 16 (13) | 0.799 |
| Mean IVC dose per session, g (range) | 50 (15–125) | 49 (23) | 59 (24) | 0.159 |
| Mean creatinine pre-IVC, µmol/L (SD) | 70 (20) | 70 (21) | 76 (18) | 0.323 |
| Mean eGFR pre-IVC, mL/min/1.73 m2 (SD) | 82 (12) | 82 (14) | 81 (14) | 0.932 |
| Presenting Condition | Total Cohort N (%) | No History of Renal Stones | History of Renal Stones |
|---|---|---|---|
| Cancer | 76 (48) | 66 (47) | 6 (50) |
| Infectious diseases and/or immune support | 54 (34) | 50 (35) | 4 (33) |
| Neurological, musculoskeletal, and skin disorders | 13 (8) | 11 (8) | 2 (17) |
| Fatigue | 6 (4) | 6 (4) | 0 |
| Other (e.g., pre-surgery, Crohn’s disease, dental, fracture, haemorrhoids) | 8 (5) | 8 (6) | 0 |
| Observation | Patient N (%) |
|---|---|
| Creatinine Increased 1 | 45/79 (57) |
| Low to Normal | 2/45 (4) |
| Normal to Normal | 40/45 (89) |
| Normal to High | 3/45 (7) |
| eGFR Decreased ≥ 15% 2 | 6/71 (8) |
| Normal to Low | 2/6 (33) |
| Low to Lower | 4/6 (66) |
| Creatinine Increased + eGFR Decreased ≥ 15% | 6/79 (9) |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Prier, M.; Carr, A.C.; Baillie, N. No Reported Renal Stones with Intravenous Vitamin C Administration: A Prospective Case Series Study. Antioxidants 2018, 7, 68. https://doi.org/10.3390/antiox7050068
Prier M, Carr AC, Baillie N. No Reported Renal Stones with Intravenous Vitamin C Administration: A Prospective Case Series Study. Antioxidants. 2018; 7(5):68. https://doi.org/10.3390/antiox7050068
Chicago/Turabian StylePrier, Melissa, Anitra C. Carr, and Nicola Baillie. 2018. "No Reported Renal Stones with Intravenous Vitamin C Administration: A Prospective Case Series Study" Antioxidants 7, no. 5: 68. https://doi.org/10.3390/antiox7050068
APA StylePrier, M., Carr, A. C., & Baillie, N. (2018). No Reported Renal Stones with Intravenous Vitamin C Administration: A Prospective Case Series Study. Antioxidants, 7(5), 68. https://doi.org/10.3390/antiox7050068