
Prevalence and Determinants of COVID-19 Vaccination Uptake Were Different between Chinese Diabetic Inpatients with and without Chronic Complications: A Cross-Sectional Survey

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
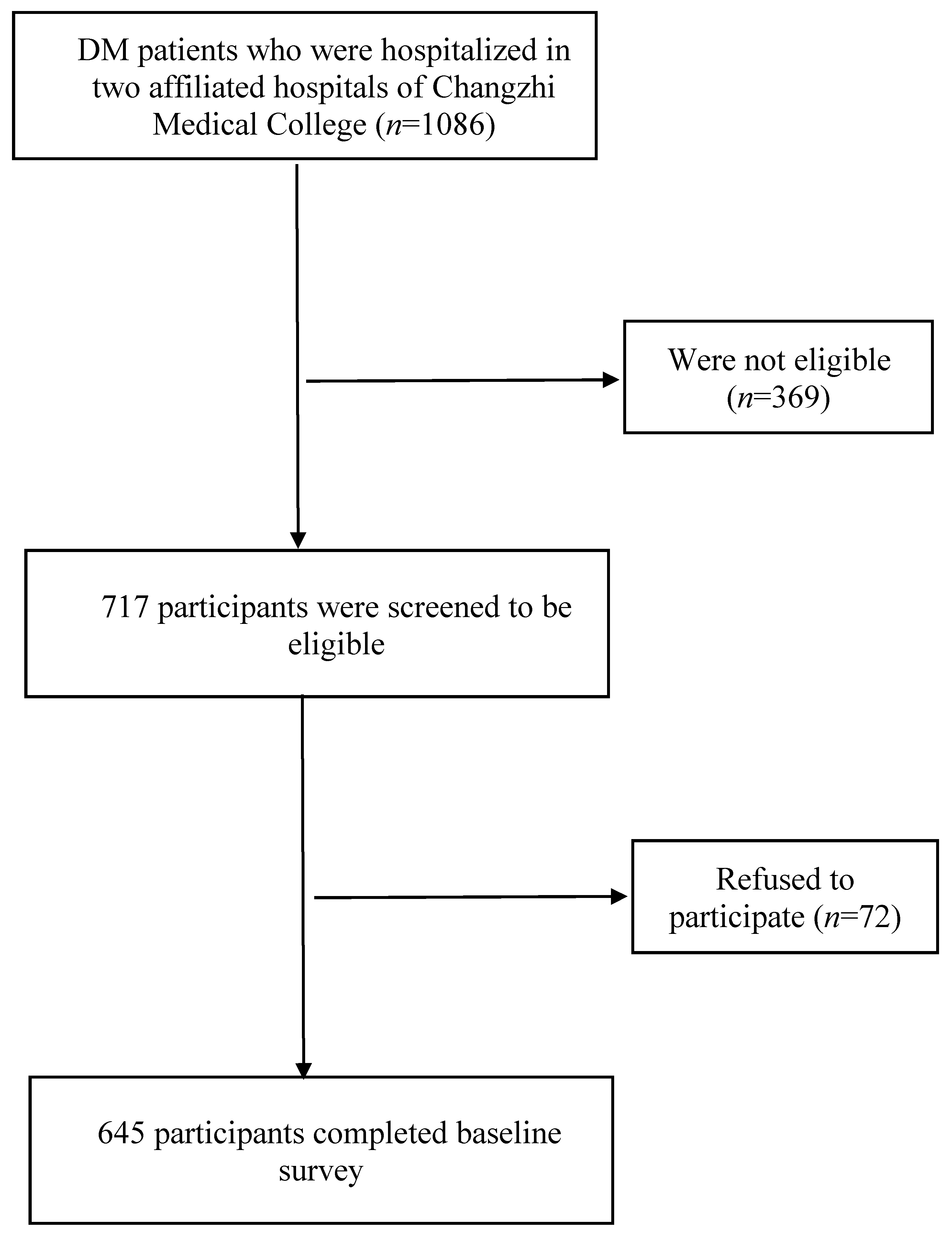
2.2. Participants
2.3. Recruitment and Data Collection
2.4. Measures
2.4.1. Development of the Questionnaire
2.4.2. Background Characteristics
2.4.3. COVID-19 Vaccination Uptake
2.4.4. Presence of Chronic DM Complications
2.4.5. Perceptions Related to COVID-19 Vaccination Based on the HBM
2.5. Sample Size Planning
2.6. Statistical Analysis
3. Results
3.1. Background Characteristics
3.2. Comparing COVID-19 Vaccination Uptake and Perceptions Related to COVID-19 Vaccination between DM Patients with and without Complications
3.3. Factors Associated with COVID-19 Vaccination Uptake among Participants with Chronic DM Complications
3.4. Factors Associated with COVID-19 Vaccination Uptake among Participants without any Chronic DM Complications
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
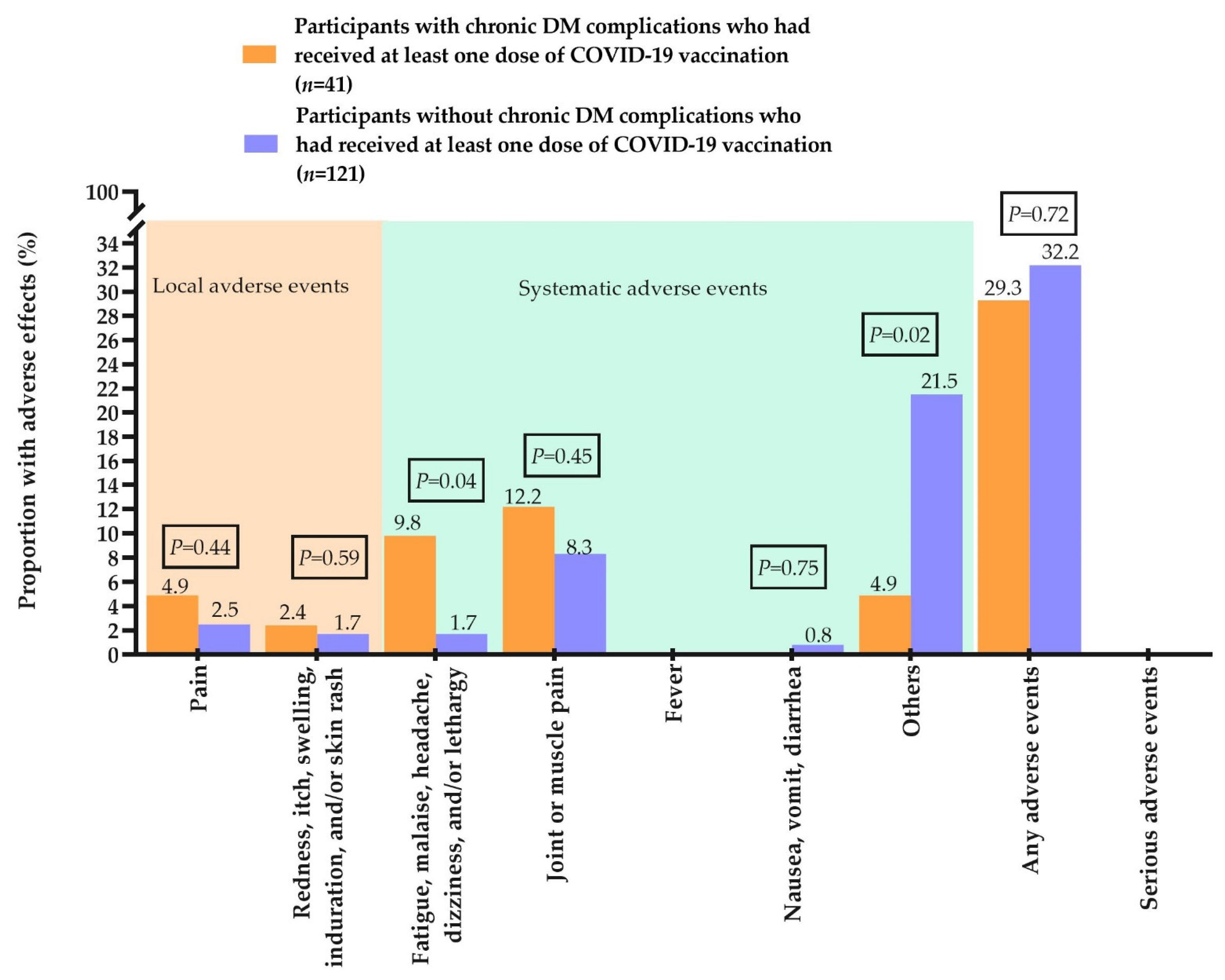
| Self-Reported Adverse Events of COVID-19 Vaccination | With Complications (n = 41) | Without Complications (n = 121) | p Values |
|---|---|---|---|
| Local adverse events (% Yes) | |||
| Pain | 4.9 | 2.5 | 0.44 |
| Redness, itch, swelling, induration, and/or skin rash | 2.4 | 1.7 | 0.59 |
| Systematic adverse events (% Yes) | |||
| Fatigue, malaise, headache, dizziness, and/or lethargy | 9.8 | 1.7 | 0.04 |
| Joint or muscle pain | 12.2 | 8.3 | 0.45 |
| Fever | 0.0 | 0.0 | N.A. |
| Nausea, vomiting, diarrhea | 0.0 | 0.8 | 0.75 |
| Others | 4.9 | 21.5 | 0.02 |
| Any adverse events (% Yes) | 29.3 | 32.2 | 0.72 |
| Serious adverse events (% Yes) | 0.0 | 0.0 | N.A. |
References
- GBD 2019 Diabetes Mortality Collaborators. Diabetes mortality and trends before 25 years of age: An analysis of the Global Burden of Disease Study 2019. Lancet Diabetes Endocrinol. 2022, 10, 177–192. [Google Scholar] [CrossRef]
- Ma, R.C.W. Epidemiology of diabetes and diabetic complications in China. Diabetologia 2018, 61, 1249–1260. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chee, Y.J.; Tan, S.K.; Yeoh, E. Dissecting the interaction between COVID-19 and diabetes mellitus. J. Diabetes Investig. 2020, 11, 1104–1114. [Google Scholar] [CrossRef] [PubMed]
- Aldossari, K.K.; Alharbi, M.B.; Alkahtani, S.M.; Alrowaily, T.Z.; Alshaikhi, A.M.; Twair, A.A. COVID-19 vaccine hesitancy among patients with diabetes in Saudi Arabia. Diabetes Metab. Syndr. 2021, 15, 102271. [Google Scholar] [CrossRef] [PubMed]
- Kreuzer, D.; Nikoopour, E.; Au, B.C.; Krougly, O.; Lee-Chan, E.; Summers, K.L.; Haeryfar, S.M.M.; Singh, B. Reduced interferon-α production by dendritic cells in type 1 diabetes does not impair immunity to influenza virus. Clin. Exp. Immunol. 2015, 179, 245–255. [Google Scholar] [CrossRef] [Green Version]
- Muniyappa, R.; Gubbi, S. COVID-19 pandemic, coronaviruses, and diabetes mellitus. Am. J. Physiol. Endocrinol. Metab. 2020, 318, E736–E741. [Google Scholar] [CrossRef] [Green Version]
- Huang, C.; Wang, Y.; Li, X.; Ren, L.; Zhao, J.; Hu, Y.; Zhang, L.; Fan, G.; Xu, J.; Gu, X.; et al. Clinical features of patients infected with 2019 novel coronavirus in Wuhan, China. Lancet 2020, 395, 497–506. [Google Scholar] [CrossRef] [Green Version]
- Mao, L.; Jin, H.; Wang, M.; Hu, Y.; Chen, S.; He, Q.; Chang, J.; Hong, C.; Zhou, Y.; Wang, D.; et al. Neurologic Manifestations of Hospitalized Patients With Coronavirus Disease 2019 in Wuhan, China. JAMA Neurol. 2020, 77, 683–690. [Google Scholar] [CrossRef] [Green Version]
- Albulescu, R.; Dima, S.O.; Florea, I.R.; Lixandru, D.; Serban, A.M.; Aspritoiu, V.M.; Tanase, C.; Popescu, I.; Ferber, S. COVID-19 and diabetes mellitus: Unraveling the hypotheses that worsen the prognosis (Review). Exp. Ther. Med. 2020, 20, 194. [Google Scholar] [CrossRef]
- World Health Organization. Episode #46—Diabetes & COVID-19. 2022. Available online: https://www.who.int/emergencies/diseases/novel-coronavirus-2019/media-resources/science-in-5/episode-46---diabetes-covid-19 (accessed on 23 January 2022).
- Centers for Disease Control and Prevention. The Advisory Committee on Immunization Practices’ Updated Interim Recommendation for Allocation of COVID-19 Vaccine—United States, December 2020. Available online: https://www.cdc.gov/mmwr/volumes/69/wr/mm695152e2.htm (accessed on 16 February 2022).
- European Centre for Disease Prevention and Control. COVID-19 Vaccination and Prioritisation Strategies in the EU/EEA. 2020. Available online: https://www.ecdc.europa.eu/en/publications-data/covid-19-vaccination-and-prioritisation-strategies-eueea (accessed on 29 January 2022).
- American Diabetes Association. What You Need to Know: Getting a COVID-19 Vaccine. 2022. Available online: https://www.diabetes.org/coronavirus-covid-19/vaccination-guide (accessed on 20 January 2021).
- National Health Commission of the People’s Republic of China. The Guidelines for COVID-19 vaccination (first edition). 2021. Available online: http://www.nhc.gov.cn/xcs/yqfkdt/202103/c2febfd04fc5498f916b1be080905771.shtml (accessed on 19 December 2021).
- Liu, Z.; Fu, C.; Wang, W.; Xu, B. Prevalence of chronic complications of type 2 diabetes mellitus in outpatients–A cross-sectional hospital based survey in urban China. Health Qual. Life Outcomes 2010, 8, 62. [Google Scholar] [CrossRef] [Green Version]
- Jia, W.; Gao, X.; Pang, C.; Hou, X.; Bao, Y.; Liu, W.; Wang, W.; Zuo, Y.; Gu, H.; Xiang, K. Prevalence and risk factors of albuminuria and chronic kidney disease in Chinese population with type 2 diabetes and impaired glucose regulation: Shanghai diabetic complications study (SHDCS). Nephrol. Dial. Transplant. Off. Publ. Eur. Dial. Transpl. Assoc.—Eur. Ren. Assoc. 2009, 24, 3724–3731. [Google Scholar] [CrossRef] [Green Version]
- McGurnaghan, S.J.; Weir, A.; Bishop, J.; Kennedy, S.; Blackbourn, L.A.K.; A McAllister, D.; Hutchinson, S.; Caparrotta, T.M.; Mellor, J.; Jeyam, A.; et al. Risks of and risk factors for COVID-19 disease in people with diabetes: A cohort study of the total population of Scotland. Lancet Diabetes Endocrinol. 2021, 9, 82–93. [Google Scholar] [CrossRef]
- Tamura, R.E.; Said, S.M.; de Freitas, L.M.; Rubio, I.G.S. Outcome and death risk of diabetes patients with Covid-19 receiving pre-hospital and in-hospital metformin therapies. Diabetol. Metab. Syndr. 2021, 13, 76. [Google Scholar] [CrossRef]
- PPal, R.; Bhadada, S.K.; Misra, A. COVID-19 vaccination in patients with diabetes mellitus: Current concepts, uncertainties and challenges. Diabetes Metab. Syndr. 2021, 15, 505–508. [Google Scholar] [CrossRef] [PubMed]
- Guaraldi, F.; Montalti, M.; Di Valerio, Z.; Mannucci, E.; Nreu, B.; Monami, M.; Gori, D. Rate and Predictors of Hesitancy toward SARS-CoV-2 Vaccine among Type 2 Diabetic Patients: Results from an Italian Survey. Vaccines 2021, 9, 460. [Google Scholar] [CrossRef]
- Syed Alwi, S.A.R.; Rafidah, E.; Zurraini, A.; Juslina, O.; Brohi, I.B.; Lukas, S. A survey on COVID-19 vaccine acceptance and concern among Malaysians. BMC Public Health 2021, 21, 1129. [Google Scholar] [CrossRef]
- Wang, Y.; Duan, L.; Li, M.; Wang, J.; Yang, J.; Song, C.; Li, J.; Wang, J.; Jia, J.; Xu, J. COVID-19 Vaccine Hesitancy and Associated Factors among Diabetes Patients: A Cross-Sectional Survey in Changzhi, Shanxi, China. Vaccines 2022, 10, 129. [Google Scholar] [CrossRef]
- Nachimuthu, S.; Viswanathan, V. Trend in COVID-19 vaccination among people with diabetes: A short study from India. Diabetes Metab. Syndr. 2021, 15, 102190. [Google Scholar] [CrossRef]
- Duan, L.; Wang, Y.; Dong, H.; Song, C.; Zheng, J.; Li, J.; Li, M.; Wang, J.; Yang, J.; Xu, J. The COVID-19 Vaccination Behavior and Correlates in Diabetic Patients: A Health Belief Model Theory-Based Cross-Sectional Study in China, 2021. Vaccines 2022, 10, 659. [Google Scholar] [CrossRef]
- Tourkmani, A.M.; Bin Rsheed, A.M.; AlEissa, M.S.; Alqahtani, S.M.; AlOtaibi, A.F.; Almujil, M.S.; Alkhashan, I.H.; Alnassar, T.N.; Alotaibi, M.N.; Alrasheedy, A.A. Prevalence of COVID-19 Infection among Patients with Diabetes and Their Vaccination Coverage Status in Saudi Arabia: A Cross-Sectional Analysis from a Hospital-Based Diabetes Registry. Vaccines 2022, 10, 310. [Google Scholar] [CrossRef]
- Lee, D.; Rundle-Thiele, S.; Li, G. Motivating Seasonal Influenza Vaccination and Cross-Promoting COVID-19 Vaccination: An Audience Segmentation Study among University Students. Vaccines 2021, 9, 1397. [Google Scholar] [CrossRef] [PubMed]
- Carico, R.R., Jr.; Sheppard, J.; Thomas, C.B. Community pharmacists and communication in the time of COVID-19: Applying the health belief model. Res. Soc. Adm. Pharm. 2021, 17, 1984–1987. [Google Scholar] [CrossRef] [PubMed]
- Huang, X.; Yan, Y.; Su, B.; Xiao, D.; Yu, M.; Jin, X.; Duan, J.; Zhang, X.; Zheng, S.; Fang, Y.; et al. Comparing Immune Responses to Inactivated Vaccines against SARS-CoV-2 between People Living with HIV and HIV-Negative Individuals: A Cross-Sectional Study in China. Viruses 2022, 14, 277. [Google Scholar] [CrossRef]
- Our World in Data. Coronavirus (COVID-19) Vaccinations. 2022. Available online: https://ourworldindata.org/covid-vaccinations?country=OWID_WRL (accessed on 19 February 2022).
- Lau, J.T.F.; Lee, A.L.; Tse, W.S.; Mo, P.K.H.; Fong, F.; Wang, Z.; Cameron, L.D.; Sheer, V. A Randomized Control Trial for Evaluating Efficacies of Two Online Cognitive Interventions With and Without Fear-Appeal Imagery Approaches in Preventing Unprotected Anal Sex Among Chinese Men Who Have Sex with Men. AIDS Behav. 2016, 20, 1851–1862. [Google Scholar] [CrossRef] [PubMed]
- Stolow, J.A.; Moses, L.M.; Lederer, A.M.; Carter, R. How Fear Appeal Approaches in COVID-19 Health Communication May Be Harming the Global Community. Health Educ. Behav. 2020, 47, 531–535. [Google Scholar] [CrossRef]
- Jahangiry, L.; Bakhtari, F.; Sohrabi, Z.; Reihani, P.; Samei, S.; Ponnet, K.; Montazeri, A. Correction to: Risk perception related to COVID-19 among the Iranian general population: An application of the extended parallel process model. BMC Public Health 2021, 21, 1993. [Google Scholar] [CrossRef]
- Ashworth, M.; Thunström, L.; Cherry, T.L.; Newbold, S.C.; Finnoff, D.C. Emphasize personal health benefits to boost COVID-19 vaccination rates. Proc. Natl. Acad. Sci. USA 2021, 118, e2108225118. [Google Scholar] [CrossRef]
- Cheng, S.-W.; Wang, C.-Y.; Ko, Y. Costs and Length of Stay of Hospitalizations due to Diabetes-Related Complications. J. Diabetes Res. 2019, 2019, 2363292. [Google Scholar] [CrossRef]


| All (n = 645) | With Complications (n = 365) | Without Complications (n = 280) | p Values | |
|---|---|---|---|---|
| n (%) | n (%) | n (%) | ||
| Sociodemographic | ||||
| Gender | ||||
| Male | 361 (56.0) | 212 (58.1) | 149 (53.2) | 0.22 |
| Female | 284 (44.0) | 153 (41.9) | 131 (46.8) | |
| Age group, years | ||||
| 18–39 | 68 (10.5) | 39 (10.7) | 29 (10.4) | 0.72 |
| 40–49 | 115 (17.8) | 65 (17.8) | 50 (17.9) | |
| 50–59 | 187 (29.0) | 113 (31.0) | 74 (26.4) | |
| 60–69 | 163 (25.3) | 89 (24.4) | 74 (26.4) | |
| ≥70 | 112 (17.4) | 59 (16.1) | 53 (18.9) | |
| Ethnicity | ||||
| Han majority | 633 (98.1) | 357 (97.8) | 276 (98.6) | 0.48 |
| Other ethnic minorities | 12 (1.9) | 8 (2.2) | 4 (1.4) | |
| The highest educational level attained | ||||
| Primary | 379 (58.8) | 198 (54.2) | 181 (64.6) | 0.008 |
| Secondary | 122 (18.9) | 70 (19.2) | 52 (18.6) | |
| Tertiary or above | 144 (22.3) | 97 (26.6) | 47 (16.8) | |
| Relationship status | ||||
| Currently single | 76 (11.8) | 35 (9.6) | 41 (14.6) | 0.048 |
| Married or cohabiting with a partner | 569 (88.2) | 330 (90.4) | 239 (85.4) | |
| Employment status | ||||
| Fulltime | 179 (27.8) | 100 (27.4) | 79 (28.2) | 0.82 |
| Part-time/unemployed /retired/students | 466 (72.2) | 265 (72.6) | 201 (71.8) | |
| Monthly personal income, China Yuan (USD) | ||||
| <2000 (317.5) | 263 (40.8) | 147 (40.3) | 116 (41.4) | 0.83 |
| 2000–3499 (317.5–555.4) | 178 (27.6) | 100 (27.4) | 78 (27.9) | |
| 3500–4999 (555.5–793.5) | 131 (20.3) | 73 (20.0) | 58 (20.7) | |
| ≥5000 (793.6) | 73 (11.3) | 45 (12.3) | 28 (10.0) | |
| Type of medical insurance | ||||
| Urban workers’ medical insurance | 297 (46.0) | 202 (55.3) | 95 (33.9) | <0.001 |
| Urban residents’ medical insurance | 152 (23.6) | 115 (31.5) | 37 (13.2) | |
| New Rural Cooperative Medical Scheme | 196 (30.4) | 48 (13.2) | 148 (52.9) | |
| Lifestyles | ||||
| Current smoker | ||||
| No | 248 (38.4) | 134 (36.7) | 114 (40.7) | 0.30 |
| Yes | 397 (61.6) | 231 (63.3) | 166 (59.3) | |
| Current drinker | ||||
| No | 228 (35.3) | 118 (32.3) | 110 (39.3) | 0.07 |
| Yes | 417 (64.7) | 247 (67.7) | 170 (60.7) | |
| Characteristics related to DM | ||||
| Type of DM | ||||
| Type 2 | 613 (95.0) | 344 (94.2) | 269 (96.1) | |
| Type 1 | 32 (5.0) | 21 (5.8) | 11 (3.9) | 0.29 |
| Family history of DM | ||||
| No | 281 (43.6) | 146 (40.0) | 135 (48.2) | 0.04 |
| Yes | 364 (56.4) | 219 (60.0) | 145 (51.8) | |
| Time since receiving the diagnosis of DM, years | ||||
| ≤1 | 180 (27.9) | 99 (27.2) | 81 (28.9) | 0.002 |
| 2–10 | 265 (41.1) | 133 (36.4) | 132 (47.1) | |
| >10 | 200 (31.0) | 133 (36.4) | 67 (24.0) | |
| Fasting blood glucose level in the most recent episode of testing, mmol/L | ||||
| <7 | 236 (36.6) | 134 (36.7) | 102 (36.4) | 0.37 |
| 7–13.9 | 367 (56.9) | 203 (55.6) | 164 (58.6) | |
| >13.9 | 42 (6.5) | 28 (7.7) | 14 (5.0) | |
| The postprandial blood glucose level in the most recent episode of testing, mmol/L | ||||
| <10 | 221 (34.3) | 118 (32.3) | 103 (36.8) | 0.01 |
| 10–11.1 | 117 (18.1) | 56 (15.3) | 61 (21.8) | |
| >11.1 | 307 (47.6) | 191 (52.4) | 116 (41.4) | |
| Presence of chronic conditions that were not considered as chronic DM complications | ||||
| No | 162 (25.1) | 33 (9.0) | 129 (46.1) | <0.001 |
| Yes | 483 (74.9) | 332 (91.0) | 151 (53.9) |
| With Complications (n = 365) | Without Complications (n = 280) | Unadjusted p Values 1 | Adjusted p Values 2 | |
|---|---|---|---|---|
| COVID-19 vaccination uptake | ||||
| Uptake of at least one dose of COVID-19 vaccination, n (%) | ||||
| No | 324 (88.8) | 159 (56.8) | ||
| Yes | 41 (11.2) | 121 (43.2) | <0.001 | <0.001 |
| Perceived susceptibility | ||||
| You have a high risk of contracting COVID-19, n (%) agree/strongly agree | 277 (75.9) | 237 (84.6) | 0.006 | 0.001 |
| Item score, mean (SD) | 3.8 (0.8) | 4.1 (0.9) | <0.001 | <0.001 |
| Perceived severity | ||||
| The consequences of contracting COVID-19 are severe; n (%) agree/strongly agree | 127 (34.8) | 127 (45.3) | 0.007 | 0.04 |
| Item score, mean (SD) | 2.9 (1.3) | 3.5 (0.7) | <0.001 | <0.001 |
| Perceived benefits | ||||
| Receiving COVID-19 vaccination could reduce your risk of contracting COVID-19; n (%) agree/strongly agree | 131 (35.9) | 141 (50.4) | <0.001 | 0.03 |
| Item score, mean (SD) | 3.3 (0.8) | 3.6 (0.8) | <0.001 | <0.001 |
| Receiving COVID-19 vaccination could reduce your risk of transmitting COVID-19 to others; n (%) agree/strongly agree | 149 (40.8) | 96 (34.3) | 0.09 | 0.50 |
| Item score, mean (SD) | 3.3 (0.9) | 3.3 (0.7) | 0.43 | 0.71 |
| Receiving COVID-19 vaccination is beneficial for you and others; n (%) agree/strongly agree | 20 (5.5) | 37 (13.2) | 0.001 | 0.01 |
| Item score, mean (SD) | 2.8 (0.6) | 3.0 (0.7) | 0.001 | 0.006 |
| Perceived barriers | ||||
| You are worried about the safety of COVID-19 vaccination for DM patients, n (%) agree/strongly agree | 241 (66.0) | 154 (55.0) | 0.004 | 0.22 |
| Item score, mean (SD) | 3.8 (0.9) | 3.5 (0.7) | <0.001 | 0.002 |
| You are concerned about the side effects of COVID-19 vaccination; n (%) agree/strongly agree | 186 (51.0) | 124 (44.3) | 0.09 | 0.28 |
| Item score, mean (SD) | 3.5 (0.8) | 3.6 (0.9) | 0.06 | 0.10 |
| Cues to action | ||||
| Doctors will suggest you receive COVID-19 vaccination to reduce the risk of infection; n (%) agree/strongly agree | 233 (63.8) | 171 (61.1) | 0.47 | 0.99 |
| Item score, mean (SD) | 3.5 (1.1) | 3.6 (0.7) | 0.10 | 0.10 |
| Mass media suggest DM patients receive COVID-19 vaccination; n) agree/strongly agree | 172 (47.1) | 152 (54.3) | 0.07 | 0.07 |
| Item score, mean (SD) | 3.2 (1.1) | 3.5 (0.7) | <0.001 | 0.001 |
| Uptake of COVID-19 vaccination among your relatives would influence your decision to receive the vaccine; n (%) agree/strongly agree | 79 (21.6) | 94 (33.6) | 0.001 | 0.001 |
| Item score, mean (SD) | 2.3 (1.1) | 3.2 (0.9) | <0.001 | <0.001 |
| With Complications (n = 365) | Without Complications (n = 280) | |||
|---|---|---|---|---|
| OR (95%CI) | p Values | OR (95%CI) | p Values | |
| Sociodemographic | ||||
| Gender | ||||
| Male | 1.0 | 1.0 | ||
| Female | 0.54 (0.27, 1.09) | 0.09 | 0.39 (0.24, 0.64) | <0.001 |
| Age group, years | ||||
| 18–39 | 1.0 | 1.0 | ||
| 40–49 | 4.57 (0.54, 38.78) | 0.16 | 1.06 (0.42, 2.69) | 0.90 |
| 50–59 | 4.10 (0.51, 32.85) | 0.18 | 0.57 (0.24, 1.36) | 0.20 |
| 60–69 | 4.28 (0.52, 34.97) | 0.18 | 0.30 (0.12, 0.73) | 0.008 |
| ≥70 | 10.74 (1.34, 85.86) | 0.03 | 0.39 (0.16, 1.00) | 0.049 |
| Ethnicity | ||||
| Han majority | 1.0 | 1.0 | ||
| Other ethnic minorities | 1.13 (0.14, 9.44) | 0.91 | 4.02 (0.41, 39.10) | 0.23 |
| The highest educational level attained | ||||
| Primary | 1.0 | 1.0 | ||
| Secondary | 0.53 (0.20, 1.45) | 0.22 | 1.28 (0.68, 2.39) | 0.44 |
| Tertiary or above | 0.89 (0.42, 1.88) | 0.75 | 4.11 (2.05, 8.23) | <0.001 |
| Relationship status | ||||
| Currently single | 1.0 | 1.0 | ||
| Married or cohabiting with a partner | 2.21 (0.51, 9.58) | 0.29 | 1.38 (0.70, 2.74) | 0.36 |
| Employment status | ||||
| Full-time | 1.0 | 1.0 | ||
| Part-time/unemployed /retired/students | 1.96 (0.84, 4.57) | 0.12 | 0.61 (0.36, 1.04) | 0.07 |
| Monthly personal income, China Yuan (USD) | ||||
| <2000 (317.5) | 1.0 | 1.0 | ||
| 2000–3499 (317.5–555.4) | 0.43 (0.18, 1.04) | 0.06 | 1.32 (0.72, 2.41) | 0.37 |
| 3500–4999 (555.5–793.5) | 0.42 (0.15, 1.15) | 0.09 | 2.93 (1.53, 5.63) | 0.001 |
| ≥5000 (793.6) | 1.05 (0.42, 2.64) | 0.92 | 10.22 (3.60, 29.04) | <0.001 |
| Type of medical insurance | ||||
| Urban workers’ medical insurance | 1.0 | 1.0 | ||
| Urban residents’ medical insurance | 2.17 (1.02, 4.63) | 0.05 | 1.20 (0.55, 2.61) | 0.65 |
| New Rural Cooperative Medical Scheme | 3.99 (1.68, 9.48) | 0.002 | 0.30 (0.17, 0.51) | <0.001 |
| Lifestyles | ||||
| Current smoker | ||||
| No | 1.0 | 1.0 | ||
| Yes | 0.15 (0.07, 0.32) | <0.001 | 0.24 (0.15, 0.41) | <0.001 |
| Current drinker | ||||
| No | 1.0 | 1.0 | ||
| Yes | 0.16 (0.08, 0.32) | <0.001 | 0.14 (0.08, 0.24) | <0.001 |
| Characteristics related to DM | ||||
| Type of DM | ||||
| Type 2 | 1.0 | 1.0 | ||
| Type 1 | 0.38 (0.05, 2.91) | 0.35 | 2.38 (0.68, 8.32) | 0.18 |
| Family history of DM | ||||
| No | 1.0 | 1.0 | ||
| Yes | 0.23 (0.12, 0.48) | <0.001 | 0.29 (0.18, 0.48) | <0.001 |
| Time since receiving the diagnosis of DM, years | ||||
| ≤1 | 1.0 | 1.0 | ||
| 2–10 | 5.25 (1.16, 23.85) | 0.03 | 0.88 (0.50, 1.53) | 0.64 |
| >10 | 11.79 (2.73, 50.96) | 0.001 | 0.85 (0.44, 1.64) | 0.64 |
| Fasting blood glucose level in the most recent episode of testing, mmol/L | ||||
| <7 | 1.0 | 1.0 | ||
| 7–13.9 | 0.92 (0.48, 1.79) | 0.81 | 0.72 (0.44, 1.18) | 0.19 |
| >13.9 | N.A. | N.A. | 0.42 (0.12, 1.41) | 0.16 |
| The postprandial blood glucose level in the most recent episode of testing, mmol/L | ||||
| <10 | 1.0 | 1.0 | ||
| 10–11.1 | 1.15 (0.43, 3.07) | 0.78 | 0.67 (0.35, 1.27) | 0.22 |
| >11.1 | 1.00 (0.48, 2.08) | 1.00 | 0.81 (0.47, 1.38) | 0.43 |
| Presence of chronic conditions that were not considered as chronic DM complications | ||||
| No | 1.0 | 1.0 | ||
| Yes | 0.12 (0.05, 0.27) | <0.001 | 0.21 (0.13, 0.36) | <0.001 |
| With Complications (n = 365) | Without Complications (n = 280) | |||
|---|---|---|---|---|
| AOR (95%CI) | p Values | AOR (95%CI) | p Values | |
| Perceived susceptibility | ||||
| You have a high risk of contracting COVID-19 | 2.01 (1.03, 3.91) | 0.04 | 0.88 (0.60, 1.28) | 0.50 |
| Perceived severity | ||||
| The consequences of contracting COVID-19 are severe | 1.73 (1.17, 2.56) | 0.01 | 2.74 (1.68, 4.47) | <0.001 |
| Perceived benefits | ||||
| Receiving COVID-19 vaccination could reduce your risk of contracting COVID-19 | 1.21 (0.75, 1.95) | 0.45 | 1.91 (1.28, 2.84) | 0.001 |
| Receiving COVID-19 vaccination could reduce your risk of transmitting COVID-19 to others | 1.06 (0.67, 1.69) | 0.81 | 0.89 (0.57, 1.41) | 0.62 |
| Receiving COVID-19 vaccination is beneficial for you and others | 0.80 (0.45, 1.42) | 0.45 | 0.63 (0.38, 1.05) | 0.08 |
| Perceived barriers | ||||
| You are worried about the safety of COVID-19 vaccination for DM patients | 0.37 (0.22, 0.62) | <0.001 | 0.31 (0.18, 0.52) | <0.001 |
| You are concerned about the side effects of COVID-19 vaccination | 0.50 (0.31, 0.83) | 0.008 | 0.58 (0.38, 0.89) | 0.01 |
| Cues to action | ||||
| Doctors will suggest you receive COVID-19 vaccination to reduce the risk of infection | 1.99 (1.19, 3.35) | 0.009 | 1.38 (0.89, 2.16) | 0.16 |
| Mass media suggest DM patients receive COVID-19 vaccination | 1.08 (0.73, 1.59) | 0.71 | 1.09 (0.70, 1.69) | 0.72 |
| Uptake of COVID-19 vaccination among your relatives would influence your decision to receive the vaccination | 2.80 (1.83, 4.30) | <0.001 | 2.09 (1.47, 2.96) | <0.001 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Xu, J.; Chen, S.; Wang, Y.; Duan, L.; Li, J.; Shan, Y.; Lan, X.; Song, M.; Yang, J.; Wang, Z. Prevalence and Determinants of COVID-19 Vaccination Uptake Were Different between Chinese Diabetic Inpatients with and without Chronic Complications: A Cross-Sectional Survey. Vaccines 2022, 10, 994. https://doi.org/10.3390/vaccines10070994
Xu J, Chen S, Wang Y, Duan L, Li J, Shan Y, Lan X, Song M, Yang J, Wang Z. Prevalence and Determinants of COVID-19 Vaccination Uptake Were Different between Chinese Diabetic Inpatients with and without Chronic Complications: A Cross-Sectional Survey. Vaccines. 2022; 10(7):994. https://doi.org/10.3390/vaccines10070994
Chicago/Turabian StyleXu, Junjie, Siyu Chen, Ying Wang, Lingrui Duan, Jing Li, Ying Shan, Xinquan Lan, Moxin Song, Jianzhou Yang, and Zixin Wang. 2022. "Prevalence and Determinants of COVID-19 Vaccination Uptake Were Different between Chinese Diabetic Inpatients with and without Chronic Complications: A Cross-Sectional Survey" Vaccines 10, no. 7: 994. https://doi.org/10.3390/vaccines10070994