
Why Parents Say No to Having Their Children Vaccinated against Measles: A Systematic Review of the Social Determinants of Parental Perceptions on MMR Vaccine Hesitancy
 , , ,
, , ,
Abstract
:1. Introduction
1.1. Vaccine Hesitancy
1.2. Social Determinants of MMR Vaccination
- Why do parents delay, refuse, or oppose to having their children vaccinated against measles and other vaccine preventable diseases?
- What are the parental perceptions, attitudes, and practices on measles vaccination?
- Where do parents/caregivers obtain measles vaccine information? Which source do parents/caregivers trust on measles immunization?
- Which social factors impact parental perceptions, attitudes, and practices promote or hinder measles vaccine hesitancy?
- How can families, primary care, health care, public health, and government address measles vaccine hesitancy?
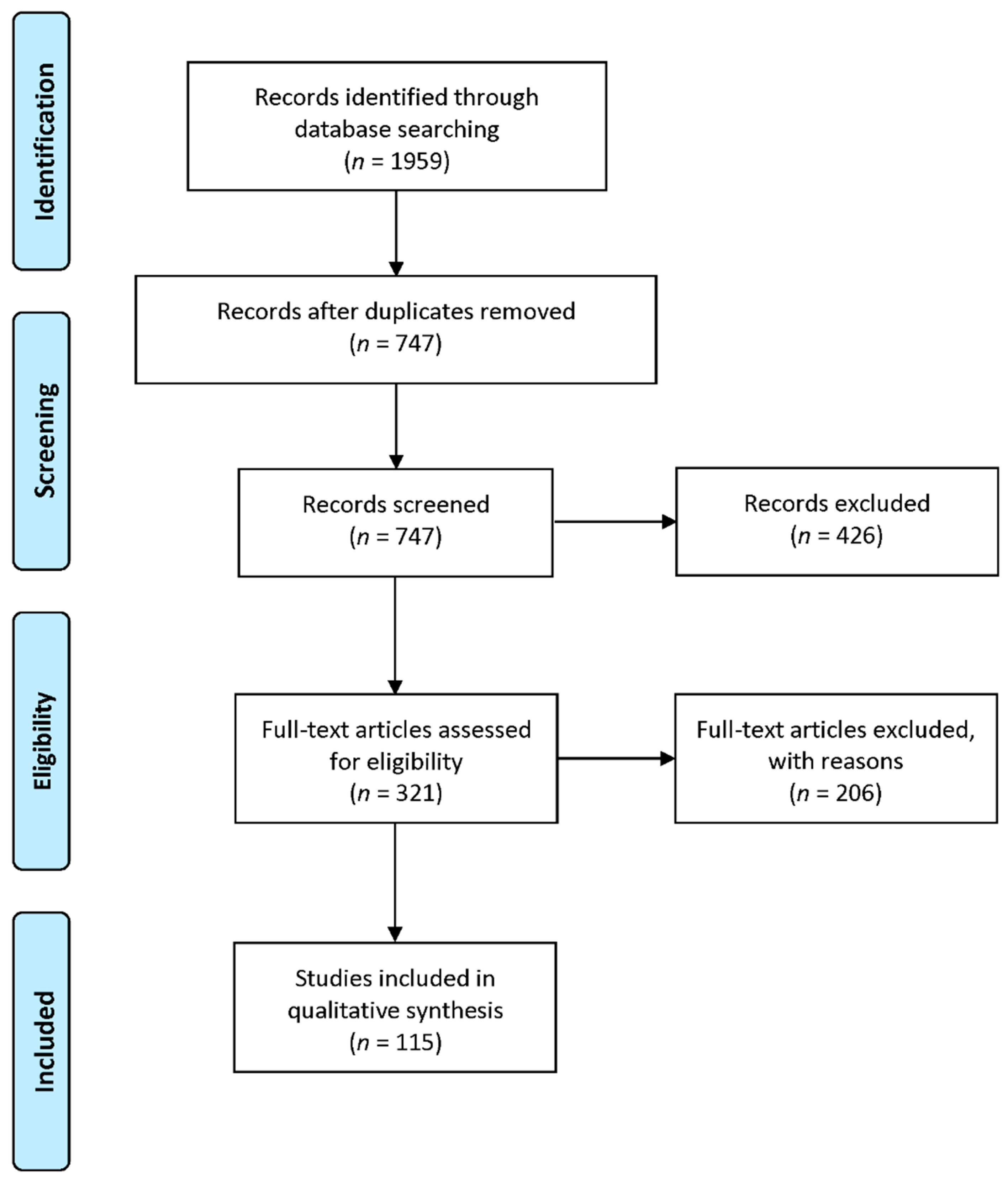
2. Materials and Methods
2.1. Search Strategy
2.2. Eligibility Criteria
- Written in English;
- Published during the years from 2000 to 2022 to capture patterns in vaccine hesitancy and vaccine perspectives, attitudes, and behavior within the context of the social determinants of health to help explain the resurgence in measles during the post-measles elimination era in the United States;
- Involved empirical research studies and/or literature reviews (journal articles, dissertations, theses);
- Focused on the United States;
- Addressed measles/MMR vaccine hesitancy;
- Discussed/mentioned parent/caregiver demographics, vaccine beliefs, attitudes, practices toward measles/MMR, sources of vaccine information, and social factors facilitating or hindering vaccine compliance.
2.3. Data Extraction and Management
- Economy (annual household income and community poverty levels);
- Employment (job status, work–life balance);
- Education (attainment of formal education, access to health education materials);
- Political (legislation, political involvement);
- Environmental (neighborhood physical characteristics, environmental influences);
- Housing (home ownership, housing condition);
- Medical (physical distance to healthcare facilities, positive relationship with healthcare providers, access to health insurance);
- Governmental (funding, policy/legislation, services, local governments, civic participation, political structure, community organizations);
- Public health (health policy, intervention strategies);
- Psychosocial (influence of friends, extended family, other social networks);
- Behavioral (smoking, physical activity, diet/obesity, fresh fruit and vegetable consumption, alcohol/illicit drug use, violence);
- Transport (public transportation, personal vehicle ownership).
2.4. Data Analysis
3. Results
3.1. Study Design and Vaccine Focus
3.2. Sociodemographics
3.3. Vaccine Hesitancy Themes
3.4. Vaccine Information Sources
3.5. SDH Facilitating and Hindering Vaccine Compliance
3.6. Approaches to Vaccine Hesitancy
3.6.1. Primary Care/Healthcare-Level Strategies
3.6.2. Public-Health-Level Strategies
3.6.3. Government-Level Strategies
4. Discussion
4.1. Themes on MMR Vaccine Hesitancy
4.2. Themes on Vaccine Information Sources
4.3. Themes on the Social Determinants of Vaccine Hesitancy and Vaccine Compliance
4.4. Themes on Primary Care/Healthcare Strategies
4.5. Themes on Public Health and Government-Level Strategies
4.6. Strengths and Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Centers for Disease Control and Prevention. Ten great public health achievements—United States, 1900–1999. Morb. Mortal. Wkly. Rep. 1999, 48, 241–243. [Google Scholar]
- McSeveney, M. FDA Reiterates the Importance of Vaccines Such as the Measles, Mumps, and Rubella (MMR) Vaccine. Available online: https://www.fda.gov/news-events/fda-brief/fda-brief-fda-reiterates-importance-vaccines-such-measles-mumps-and-rubella-mmr-vaccine (accessed on 27 May 2021).
- World Health Organization. Measles Cases Spike Globally Due to Gaps in Vaccination Coverage. Available online: https://www.who.int/news/item/29-11-2018-measles-cases-spike-globally-due-to-gaps-in-vaccination-coverage (accessed on 1 November 2021).
- Centers for Disease Control and Prevention. Transmission of Measles. Available online: https://www.cdc.gov/measles/transmission.html (accessed on 2 September 2021).
- Tesini, B.L. Merck Manual—Measles. Available online: https://www.merckmanuals.com/professional/pediatrics/miscellaneous-viral-infections-in-infants-and-children/measles (accessed on 2 September 2021).
- Centers for Disease Control and Prevention. About Measles Vaccination. Available online: https://www.cdc.gov/vaccines/vpd/measles/index.html (accessed on 27 May 2021).
- The College of Physicians of Philadelphia. History of Vaccines. Available online: https://www.historyofvaccines.org/timeline/all (accessed on 27 May 2021).
- Centers for Disease Control and Prevention. Measles Cases and Outbreaks: Measles Cases in 2019. Available online: https://www.cdc.gov/measles/cases-outbreaks.html (accessed on 27 May 2021).
- MacDonald, N.E.; Eskola, J.; Liang, X.; Chaudhuri, M.; Dube, E.; Gellin, B.; Goldstein, S.; Larson, H.; Manzo, M.L.; Reingold, A.; et al. Vaccine Hesitancy: Definition, Scope and Determinants. Vaccine 2015, 33, 4161–4164. [Google Scholar] [CrossRef]
- World Health Organization. Report of the SAGE Working Group on Vaccine Hesitancy. Available online: https://www.who.int/immunization/sage/meetings/2014/october/1_Report_WORKING_GROUP_vaccine_hesitancy_final.pdf (accessed on 27 May 2021).
- Gowda, C.; Dempsey, A.F. The rise (and fall?) of parental vaccine hesitancy. Hum. Vaccines Immunother. 2013, 9, 1755–1762. [Google Scholar] [CrossRef] [PubMed]
- Salmon, D.A.; Dudley, M.Z.; Glanz, J.M.; Omer, S.B. Vaccine hesitancy: Causes, consequences, and a call to action. Vaccine 2015, 33, D66–D71. [Google Scholar] [CrossRef] [PubMed]
- Centers for Disease Control and Prevention. Global Measles Outbreaks. Available online: https://www.cdc.gov/globalhealth/measles/data/global-measles-outbreaks.html (accessed on 27 February 2023).
- Dabbagh, A.; Laws, R.L.; Steulet, C.; Dumolard, L.; Gacic-Dobo, M.; Mulders, M.N.; Kretsinger, K.; Alexander, J.P.; Rota, P.A.; Goodson, J.L. Progress towards Regional measles elimination—Worldwide, 2000–2017. Wkly. Epidemiol. Rec. 2018, 93, 649–659. [Google Scholar] [CrossRef]
- World Health Organization. Nearly 40 Million Children Are Dangerously Susceptible to Growing Measles Threat. Available online: https://www.who.int/news/item/23-11-2022-nearly-40-million-children-are-dangerously-susceptible-to-growing-measles-threat (accessed on 29 March 2023).
- Shen, S.C.; Dubey, V. Addressing vaccine hesitancy: Clinical guidance for primary care physicians working with parents. Can. Fam. Physician 2019, 65, 175–181. [Google Scholar]
- Quinn, S.C.; Jamison, A.M.; Freimuth, V.S. Measles outbreaks and public attitudes towards vaccine exemptions: Some cautions and strategies for addressing vaccine hesitancy. Hum. Vaccines Immunother. 2020, 16, 1050–1054. [Google Scholar] [CrossRef]
- Gatwood, J.; Chiu, C.-Y.; Shuvo, S.; Ramachandran, S.; Jadhav, S.; Hohmeier, K.C.; Hagemann, T. Role of social determinants of health in pneumococcal vaccination among high-risk adults. Vaccine 2021, 39, 1951–1962. [Google Scholar] [CrossRef]
- Larson, H.J.; Clarke, R.M.; Jarrett, C.; Eckersberger, E.; Levine, Z.; Schulz, W.S.; Paterson, P. Measuring trust in vaccination: A systematic review. Hum. Vaccines Immunother. 2018, 14, 1599–1609. [Google Scholar] [CrossRef] [PubMed]
- Goodson, B.; Larson, H. How to Build Trust in Vaccines: Understanding the Drivers of Vaccine Confidence. Available online: https://www.weforum.org/reports/how-to-build-trust-in-vaccines-understanding-the-drivers-of-vaccine-confidence/ (accessed on 25 May 2021).
- Olive, J.K.; Hotez, P.J.; Damania, A.; Nolan, M.S. Correction: The state of the antivaccine movement in the United States: A focused examination of nonmedical exemptions in states and counties. PLoS Med. 2018, 15, e1002616. [Google Scholar] [CrossRef]
- Kim, H.B. Socio-Demographic Variables That Correlate with the Percentages of Personal Belief Exemption among Kindergartens in Orange County, California. Master’s Thesis, California State University Long Beach, Long Beach, CA, USA, 2016. [Google Scholar]
- Sugerman, D.E.; Barskey, A.E.; Delea, M.G.; Ortega-Sanchez, I.R.; Bi, D.; Ralston, K.J.; Rota, P.A.; Waters-Montijo, K.; LeBaron, C.W. Measles Outbreak in a Highly Vaccinated Population, San Diego, 2008: Role of the Intentionally Undervaccinated. Pediatrics 2010, 125, 747–755. [Google Scholar] [CrossRef]
- Seither, R.; Loretan, C.; Driver, K.; Mellerson, J.L.; Knighton, C.L.; Black, C.L. Vaccination Coverage with Selected Vaccines and Exemption Rates among Children in Kindergarten—United States, 2018–2019 School Year. Morb. Mortal. Wkly. Rep. 2019, 68, 905–912. [Google Scholar] [CrossRef]
- World Health Organization. Closing the Gap in a Generation: Health Equity through Action on the Social Determinants of Health. Available online: http://www.who.int/social_determinants/thecommission/finalreport/en/ (accessed on 27 May 2021).
- Brewer, N.T.; Chapman, G.B.; Rothman, A.J.; Leask, J.; Kempe, A. Increasing Vaccination: Putting Psychological Science into Action. Psychol. Sci. Public Interest 2017, 18, 149–207. [Google Scholar] [CrossRef]
- Larson, H.J.; Jarrett, C.; Schulz, W.S.; Chaudhuri, M.; Zhou, Y.; Dubé, E.; Schuster, M.; MacDonald, N.E.; Wilson, R.; The SAGE Working Group on Vaccine Hesitancy. Measuring vaccine hesitancy: The development of a survey tool. Vaccine 2015, 33, 4165–4175. [Google Scholar] [CrossRef] [PubMed]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; PRISMA Group. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. PLoS Med. 2009, 6, e1000097. [Google Scholar] [CrossRef]
- Hillemeier, M.; Lynch, J.; Harper, S.; Casper, M. Data Set Directory of Social Determinants of Health at the Local Level; US Department of Health and Human Services, Centers for Disease Control and Prevention: Atlanta, GA, USA, 2004. Available online: https://www.cdc.gov/dhdsp/docs/data_set_directory.pdf (accessed on 9 July 2021).
- Hong, Q.N.; Pluye, P.; Fàbregues, S.; Bartlett, G.; Boardman, F.; Cargo, M.; Dagenais, P.; Gagnon, M.-P.; Griffiths, F.; Nicolau, B.; et al. Mixed Methods Appraisal Tool (MMAT), Version 2018; Registration of Copyright (#1148552); Canadian Intellectual Property Office, Industry Canada: Gatineau, QC, Canada. Available online: http://mixedmethodsappraisaltoolpublic.pbworks.com/ (accessed on 30 March 2023).
- Bardenheier, B.; Yusuf, H.; Schwartz, B.; Gust, D.; Barker, L.; Rodewald, L. Are Parental Vaccine Safety Concerns Associated with Receipt of Measles-Mumps-Rubella, Diphtheria and Tetanus Toxoids with Acellular Pertussis, or Hepatitis B Vaccines by Children? Arch. Pediatr. Adolesc. Med. 2004, 158, 569–575. [Google Scholar] [CrossRef] [PubMed]
- Baumgaertner, B.; Carlisle, J.E.; Justwan, F. The influence of political ideology and trust on willingness to vaccinate. PLoS ONE 2018, 13, e0191728. [Google Scholar] [CrossRef]
- Blackshire, L.C.; Iyiegbuniwe, E. Impact of governmental regulations on compliance with MMR immunizations in Northern California. Public Health Nurs. 2021, 38, 279–287. [Google Scholar] [CrossRef]
- Blakeslee, L. The Social Context of Vaccine Resistance: How Culture Influences the Timing and Prevalence of Vaccination. Ph.D. Thesis, The University of Wisconsin—Madison, Madison, WI, USA, 2014. [Google Scholar]
- Bonsu, N.E.M.; Mire, S.S.; Sahni, L.C.; Berry, L.N.; Dowell, L.R.; Minard, C.G.; Cunningham, R.M.; Boom, J.A.; Voigt, R.G.; Goin-Kochel, R.P. Understanding Vaccine Hesitancy among Parents of Children with Autism Spectrum Disorder and Parents of Children with Non-Autism Developmental Delays. J. Child Neurol. 2021, 36, 911–918. [Google Scholar] [CrossRef] [PubMed]
- Buckman, C.; Liu, I.C.; Cortright, L.; Tumin, D.; Syed, S. The influence of local political trends on childhood vaccine completion in North Carolina. Soc. Sci. Med. 2020, 260, 113187. [Google Scholar] [CrossRef]
- Cacciatore, M.A.; Nowak, G.; Evans, N.J. Exploring the Impact of the US Measles Outbreak on Parental Awareness of and Support for Vaccination. Health Aff. 2016, 35, 334–340. [Google Scholar] [CrossRef]
- Cataldi, J.R.; Dempsey, A.F.; O’Leary, S.T. Measles, the media, and MMR: Impact of the 2014-15 measles outbreak. Vaccine 2016, 34, 6375–6380. [Google Scholar] [CrossRef] [PubMed]
- Christianson, B.; Sharif-Mohamed, F.; Heath, J.; Roddy, M.; Bahta, L.; Omar, H.; Rockwood, T.; Kenyon, C. Parental attitudes and decisions regarding MMR vaccination during an outbreak of measles among an undervaccinated Somali community in Minnesota. Vaccine 2020, 38, 6979–6984. [Google Scholar] [CrossRef]
- Cole, J.W.; Chen, A.M.; McGuire, K.; Berman, S.; Gardner, J.; Teegala, Y. Motivational interviewing and vaccine acceptance in children: The MOTIVE study. Vaccine 2022, 40, 1846–1854. [Google Scholar] [CrossRef]
- Dempsey, A.F.; Schaffer, S.; Singer, D.; Butchart, A.; Davis, M.; Freed, G.L. Alternative Vaccination Schedule Preferences among Parents of Young Children. Pediatrics 2011, 128, 848–856. [Google Scholar] [CrossRef] [PubMed]
- Doll, M.K.; Weitzen, S.D.; Morrison, K.T. Trends in the uptake of pediatric measles-containing vaccine in the United States: A Disneyland effect? Vaccine 2021, 39, 357–363. [Google Scholar] [CrossRef]
- Flanagan-Klygis, E.A.; Sharp, L.; Frader, J.E. Dismissing the family who refuses vaccines: A study of pediatrician attitudes. Arch. Pediatr. Adolesc. Med. 2005, 159, 929–934. [Google Scholar] [CrossRef]
- Freed, G.L.; Clark, S.J.; Butchart, A.T.; Singer, D.C.; Davis, M.M. Parental Vaccine Safety Concerns in 2009. Pediatrics 2010, 125, 654–659. [Google Scholar] [CrossRef]
- Freeman, R.E.; Thaker, J.; Daley, M.F.; Glanz, J.M.; Newcomer, S.R. Vaccine timeliness and prevalence of undervaccination patterns in children ages 0–19 months, US, National Immunization Survey-Child 2017. Vaccine 2022, 40, 765–773. [Google Scholar] [CrossRef] [PubMed]
- Frew, P.M.; Fisher, A.K.; Basket, M.M.; Chung, Y.; Schamel, J.; Weiner, J.L.; Mullen, J.; Omer, S.B.; Orenstein, W.A. Changes in childhood immunization decisions in the United States: Results from 2012 & 2014 National Parental Surveys. Vaccine 2016, 34, 5689–5696. [Google Scholar] [CrossRef]
- Fuchs, E.L. Self-reported prenatal influenza vaccination and early childhood vaccine series completion. Prev. Med. 2016, 88, 8–12. [Google Scholar] [CrossRef] [PubMed]
- Gennaro, E.; Caleb, S.; Torres, R.; Alexander-Parrish, R.; Thoburn, E.; McLaughlin, J.M.; Fu, L.Y. Parental Beliefs, Logistical Challenges, and Improvement Opportunities for Vaccination among Children Ages 19–35 Months Experiencing Homelessness. J. Pediatr. 2021, 236, 246–252. [Google Scholar] [CrossRef] [PubMed]
- Gilkey, M.B.; McRee, A.-L.; Magnus, B.E.; Reiter, P.L.; Dempsey, A.F.; Brewer, N.T. Vaccination Confidence and Parental Refusal/Delay of Early Childhood Vaccines. PLoS ONE 2016, 11, e0159087. [Google Scholar] [CrossRef] [PubMed]
- Glanz, J.M.; Wagner, N.M.; Narwaney, K.J.; Pyrzanowski, J.; Kwan, B.M.; Sevick, C.; Resnicow, K.; Dempsey, A.F. Web-Based Tailored Messaging to Increase Vaccination: A Randomized Clinical Trial. Pediatrics 2020, 146, e20200669. [Google Scholar] [CrossRef]
- Gowda, C.; Schaffer, S.E.; Kopec, K.; Markel, A.; Dempsey, A.F. Does the relative importance of MMR vaccine concerns differ by degree of parental vaccine hesitancy? An exploratory study. Hum. Vaccines Immunother. 2013, 9, 430–436. [Google Scholar] [CrossRef]
- Gowda, C.; Schaffer, S.E.; Kopec, K.; Markel, A.; Dempsey, A.F. A pilot study on the effects of individually tailored education for MMR vaccine-hesitant parents on MMR vaccination intention. Hum. Vaccines Immunother. 2013, 9, 437–445. [Google Scholar] [CrossRef]
- Gromis, A.; Liu, K.-Y. The Emergence of Spatial Clustering in Medical Vaccine Exemptions Following California Senate Bill 277, 2015–2018. Am. J. Public Health 2020, 110, 1084–1091. [Google Scholar] [CrossRef]
- Holroyd, T.A.; Howa, A.C.; Delamater, P.L.; Klein, N.P.; Buttenheim, A.M.; Limaye, R.J.; Proveaux, T.M.; Omer, S.B.; Salmon, D.A. Parental vaccine attitudes, beliefs, and practices: Initial evidence in California after a vaccine policy change. Hum. Vaccines Immunother. 2021, 17, 1675–1680. [Google Scholar] [CrossRef]
- Kempe, A.; Saville, A.W.; Albertin, C.; Zimet, G.; Breck, A.; Helmkamp, L.; Vangala, S.; Dickinson, L.M.; Rand, C.; Humiston, S.; et al. Parental Hesitancy about Routine Childhood and Influenza Vaccinations: A National Survey. Pediatrics 2020, 146, e20193852. [Google Scholar] [CrossRef]
- Kettunen, C.; Nemecek, J.; Wenger, O. Evaluation of low immunization coverage among the Amish population in rural Ohio. Am. J. Infect. Control 2017, 45, 630–634. [Google Scholar] [CrossRef]
- Langkamp, D.L.; Dusseau, A.; Brown, M.F. Vaccine Hesitancy and Low Immunization Rates in Children with Down Syndrome. J. Pediatr. 2020, 223, 64–67.e2. [Google Scholar] [CrossRef] [PubMed]
- Lee, C.; Whetten, K.; Omer, S.; Pan, W.; Salmon, D. Hurdles to herd immunity: Distrust of government and vaccine refusal in the US, 2002–2003. Vaccine 2016, 34, 3972–3978. [Google Scholar] [CrossRef] [PubMed]
- Leonard, W.L. Parental Confidence in US Government and Medical Authorities, Measles (Rubeloa) Knowledge, and MMR Vaccine Compliance. Ph.D. Thesis, Walden University, Minneapolis, MN, USA, 2015. [Google Scholar]
- Lieu, T.A.; Ray, G.T.; Klein, N.P.; Chung, C.; Kulldorff, M. Geographic Clusters in Underimmunization and Vaccine Refusal. Pediatrics 2015, 135, 280–289. [Google Scholar] [CrossRef] [PubMed]
- McNutt, L.-A.; Desemone, C.; DeNicola, E.; El Chebib, H.; Nadeau, J.A.; Bednarczyk, R.A.; Shaw, J. Affluence as a predictor of vaccine refusal and underimmunization in California private kindergartens. Vaccine 2016, 34, 1733–1738. [Google Scholar] [CrossRef]
- Mergler, M.J.; Omer, S.B.; Pan, W.K.; Navar-Boggan, A.M.; Orenstein, W.; Marcuse, E.K.; Taylor, J.; Dehart, M.P.; Carter, T.C.; Damico, A.; et al. Association of vaccine-related attitudes and beliefs between parents and health care providers. Vaccine 2013, 31, 4591–4595. [Google Scholar] [CrossRef]
- Mills, K.; Nilsen, K. Kansas Family Physicians Perceptions of Parental Vaccination Hesitancy. Kans. J. Med. 2020, 13, 248–259. [Google Scholar] [CrossRef]
- Moyer-Gusé, E.; Robinson, M.J.; Mcknight, J. The Role of Humor in Messaging about the MMR Vaccine. J. Health Commun. 2018, 23, 514–522. [Google Scholar] [CrossRef]
- Navin, M.C.; Wasserman, J.A.; Ahmad, M.; Bies, S. Vaccine Education, Reasons for Refusal, and Vaccination Behavior. Am. J. Prev. Med. 2019, 56, 359–367. [Google Scholar] [CrossRef]
- Newcomer, S.R.; Freeman, R.E.; Wehner, B.K.; Anderson, S.L.; Daley, M.F. Timeliness of Early Childhood Vaccinations and Undervaccination Patterns in Montana. Am. J. Prev. Med. 2021, 61, e21–e29. [Google Scholar] [CrossRef]
- Nguyen, K.H.; Srivastav, A.; Lindley, M.C.; Fisher, A.; Kim, D.; Greby, S.M.; Lee, J.; Singleton, J.A. Parental Vaccine Hesitancy and Association with Childhood Diphtheria, Tetanus Toxoid, and Acellular Pertussis; Measles, Mumps, and Rubella; Rotavirus; and Combined 7-Series Vaccination. Am. J. Prev. Med. 2022, 62, 367–376. [Google Scholar] [CrossRef]
- Nyathi, S.; Karpel, H.C.; Sainani, K.L.; Maldonado, Y.; Hotez, P.J.; Bendavid, E.; Lo, N.C. The 2016 California policy to eliminate nonmedical vaccine exemptions and changes in vaccine coverage: An empirical policy analysis. PLoS Med. 2019, 16, e1002994. [Google Scholar] [CrossRef] [PubMed]
- Nyhan, B.; Reifler, J.; Richey, S.; Freed, G.L. Effective Messages in Vaccine Promotion: A Randomized Trial. Pediatrics 2014, 133, e835–e842. [Google Scholar] [CrossRef]
- Opel, D.J.; Taylor, J.A.; Mangione-Smith, R.; Solomon, C.; Zhao, C.; Catz, S.; Martin, D. Validity and reliability of a survey to identify vaccine-hesitant parents. Vaccine 2011, 29, 6598–6605. [Google Scholar] [CrossRef] [PubMed]
- Opel, D.J.; Taylor, J.A.; Zhou, C.; Catz, S.; Myaing, M.; Mangione-Smith, R. The Relationship between Parent Attitudes about Childhood Vaccines Survey Scores and Future Child Immunization Status. JAMA Pediatr. 2013, 167, 1065–1071. [Google Scholar] [CrossRef]
- Philpot, A.M. Predicting the Compliance of Children to DTaP and MMR within the United States. Ph.D. Thesis, Capella University, Minneapolis, MN, USA, 2015. [Google Scholar]
- Qian, M.; Chou, S.-Y.; Lai, E.K. Confirmatory bias in health decisions: Evidence from the MMR-autism controversy. J. Health Econ. 2020, 70, 102284. [Google Scholar] [CrossRef] [PubMed]
- Reuben, R.; Aitken, D.; Freedman, J.L.; Einstein, G. Mistrust of the medical profession and higher disgust sensitivity predict parental vaccine hesitancy. PLoS ONE 2020, 15, e0237755. [Google Scholar] [CrossRef]
- Rodriguez-Nava, G.; Trelles-Garcia, D.P.; Yanez-Bello, M.A.; Imani-Ramos, T.; Trelles-Garcia, V.P.; Bustamante-Soliz, D.S.; Patiño-Salamea, E. MMR Vaccine Adverse Drug Reactions Reports in the CDC WONDER System, 1989–2019. Open Forum Infect. Dis. 2020, 7, ofaa211. [Google Scholar] [CrossRef]
- Sahni, L.C.; Boom, J.A.; Mire, S.S.; Berry, L.N.; Dowell, L.R.; Minard, C.G.; Cunningham, R.M.; Goin-Kochel, R.P. Vaccine hesitancy and illness perceptions: Comparing parents of children with autism spectrum disorder to other parent groups. Child. Health Care 2020, 49, 385–402. [Google Scholar] [CrossRef] [PubMed]
- Salazar, T.L. Vaccine Hesitancy among Parents in North Metro Denver in Colorado. Master’s Thesis, University of Colorado Colorado Springs, Colorado Spring, CO, USA, 2021. [Google Scholar]
- Salmon, D.A.; Moulton, L.; Omer, S.B.; Dehart, M.P.; Stokley, S.; Halsey, N.A. Factors Associated with Refusal of Childhood Vaccines among Parents of School-Aged Children: A case-control study. Arch. Pediatr. Adolesc. Med. 2005, 159, 470–476. [Google Scholar] [CrossRef]
- Salmon, D.A.; Sotir, M.J.; Pan, W.K.; Berg, J.L.; Omer, S.B.; Stokley, S.; Hopfensperger, D.J.; Davis, J.P.; Halsey, N.A. Parental vaccine refusal in Wisconsin: A case-control study. Wis. Med. J. 2009, 108, 17–23. [Google Scholar]
- Smith, P.J.; Humiston, S.G.; Parnell, T.; Vannice, K.S.; Salmon, D.A. The Association between Intentional Delay of Vaccine Administration and Timely Childhood Vaccination Coverage. Public Health Rep. 2010, 125, 534–541. [Google Scholar] [CrossRef] [PubMed]
- Smith, P.J.; Humiston, S.G.; Marcuse, E.K.; Zhao, Z.; Dorell, C.G.; Howes, C.; Hibbs, B. Parental Delay or Refusal of Vaccine Doses, Childhood Vaccination Coverage at 24 Months of Age, and the Health Belief Model. Public Health Rep. 2011, 126, 135–146. [Google Scholar] [CrossRef]
- Williams, S.E.; Morgan, A.; Opel, D.; Edwards, K.; Weinberg, S.; Rothman, R. Screening Tool Predicts Future Underimmunization among a Pediatric Practice in Tennessee. Clin. Pediatr. 2016, 55, 537–542. [Google Scholar] [CrossRef] [PubMed]
- Wolf, E.; Rowhani-Rahbar, A.; Tasslimi, A.; Matheson, J.; DeBolt, C. Parental Country of Birth and Childhood Vaccination Uptake in Washington State. Pediatrics 2016, 138, e20154544. [Google Scholar] [CrossRef]
- Xu, Y.; Margolin, D.; Niederdeppe, J. Testing Strategies to Increase Source Credibility through Strategic Message Design in the Context of Vaccination and Vaccine Hesitancy. Health Commun. 2021, 36, 1354–1367. [Google Scholar] [CrossRef] [PubMed]
- Bahta, L.; Ashkir, A. Addressing MMR vaccine resistance in Minnesota’s Somali community. Minn. Med. 2015, 98, 33–36. [Google Scholar]
- Campeau, K.L. The Rhetorical Making of an Illness: Medical Refusal, Trope, and Improvisation in a Somali Women’s Health Center. Ph.D. Thesis, University of Minnesota, Minneapolis, MN, USA, 2020. [Google Scholar]
- Danso-Odei, L. Addressing Immunization Challenges in Rural Florida: A Qualitative Case Study Research. Ph.D. Thesis, Capella University, Minneapolis, MN, USA, 2017. [Google Scholar]
- Duchsherer, A.; Jason, M.; Platt, C.A.; Majdik, Z.P. Immunized against science: Narrative community building among vaccine refusing/hesitant parents. Public Underst. Sci. 2020, 29, 419–435. [Google Scholar] [CrossRef] [PubMed]
- Kadono, M. “It’s Been a Huge Stress”: An In-Depth, Exploratory Study of Vaccine Hesitant Parents in Southern California. Ph.D. Thesis, University of South Florida, Tampa, FL, USA, 2020. [Google Scholar]
- Kang, G.J.; Ewing-Nelson, S.R.; Mackey, L.; Schlitt, J.T.; Marathe, A.; Abbas, K.M.; Swarup, S. Semantic network analysis of vaccine sentiment in online social media. Vaccine 2017, 35, 3621–3638. [Google Scholar] [CrossRef]
- McDonald, P.; Limaye, R.J.; Omer, S.B.; Buttenheim, A.M.; Mohanty, S.; Klein, N.P.; Salmon, D.A. Exploring California’s new law eliminating personal belief exemptions to childhood vaccines and vaccine decision-making among homeschooling mothers in California. Vaccine 2019, 37, 742–750. [Google Scholar] [CrossRef]
- Steiner, R.J. Who Calls the Shots? A Rhetorical Investigation into Vaccine-Hesitant Discourse. Ph.D. Thesis, University of Georgia, Athens, GA, USA, 2020. [Google Scholar]
- Ugale, J.L.; Spielvogle, H.; Spina, C.; Perreira, C.; Katz, B.; Pahud, B.; Dempsey, A.F.; Robinson, J.D.; Garrett, K.; O’leary, S.T.; et al. “It’s Like 1998 again”: Why Parents Still Refuse and Delay Vaccines. Glob. Pediatr. Health 2021, 8, 2333794X211042331. [Google Scholar] [CrossRef]
- Wharton-Michael, P.; Wharton-Clark, A. What is in a Google search? A qualitative examination of non-vaxxers’ online search practices. Qual. Res. Rep. Commun. 2020, 21, 10–20. [Google Scholar] [CrossRef]
- Downs, J.S.; DE Bruin, W.B.; Fischhoff, B. Parents’ vaccination comprehension and decisions. Vaccine 2008, 26, 1595–1607. [Google Scholar] [CrossRef]
- Estep, K.; Greenberg, P. Opting Out: Individualism and Vaccine Refusal in Pockets of Socioeconomic Homogeneity. Am. Sociol. Rev. 2020, 85, 957–991. [Google Scholar] [CrossRef]
- Gahr, P.; DeVries, A.S.; Wallace, G.; Miller, C.; Kenyon, C.; Sweet, K.; Martin, K.; White, K.; Bagstad, E.; Hooker, C.; et al. An Outbreak of Measles in an Undervaccinated Community. Pediatrics 2014, 134, e220–e228. [Google Scholar] [CrossRef]
- Kennedy, A.M.; Gust, D.A. Measles Outbreak Associated with a Church Congregation: A Study of Immunization Attitudes of Congregation Members. Public Health Rep. 2008, 123, 126–134. [Google Scholar] [CrossRef]
- Parker, A.A.; Staggs, W.; Dayan, G.H.; Ortega-Sánchez, I.R.; Rota, P.A.; Lowe, L.; Boardman, P.; Teclaw, R.; Graves, C.; LeBaron, C.W. Implications of a 2005 Measles Outbreak in Indiana for Sustained Elimination of Measles in the United States. N. Engl. J. Med. 2006, 355, 447–455. [Google Scholar] [CrossRef]
- Smith, M.J.; Woods, C.R.; Marshall, G.S. Parental vaccine concerns in Kentucky. J. Ky. Med. Assoc. 2009, 107, 342–349. [Google Scholar] [PubMed]
- Ackerman, L.K.; Serrano, J.L. Update on Routine Childhood and Adolescent Immunizations. Am. Fam. Physician 2015, 92, 460–468. [Google Scholar] [PubMed]
- Akojie, H. Strategies for Teaching New Mothers the Importance of Vaccination. Ph.D. Thesis, Walden University, Minneapolis, MN, USA, 2021. [Google Scholar]
- Anderson, P.M.; Bryson, J.M. Confronting vaccine hesitancy: What nurses need to know. Nursing 2020, 50, 43–46. [Google Scholar] [CrossRef] [PubMed]
- Blendell, R.L.; Fehr, J.L. Discussing vaccination with concerned patients: An evidence-based resource for healthcare providers. J. Périnat. Neonatal Nurs. 2012, 26, 230–241. [Google Scholar] [CrossRef] [PubMed]
- Braun, C.; O’Leary, S.T. Recent advances in addressing vaccine hesitancy. Curr. Opin. Pediatr. 2020, 32, 601–609. [Google Scholar] [CrossRef]
- Cawkwell, P.B.; Oshinsky, D. Storytelling in the context of vaccine refusal: A strategy to improve communication and immunisation. Med. Humanit. 2016, 42, 31–35. [Google Scholar] [CrossRef] [PubMed]
- Chatterjee, A.; O’keefe, C. Current controversies in the USA regarding vaccine safety. Expert Rev. Vaccines 2010, 9, 497–502. [Google Scholar] [CrossRef]
- Colgrove, J.; Bayer, R. Could it happen here? Vaccine risk controversies and the specter of derailment: A successful immunization system depends mostly on people’s willingness to have themselves and their children vaccinated. Health Aff. 2005, 24, 729–739. [Google Scholar] [CrossRef]
- de St. Maurice, A.; Edwards, K.M.; Hackell, J. Addressing Vaccine Hesitancy in Clinical Practice. Pediatr. Ann. 2018, 47, e366–e370. [Google Scholar] [CrossRef]
- DeStefano, F.; Shimabukuro, T.T. The MMR Vaccine and Autism. Annu. Rev. Virol. 2019, 6, 585–600. [Google Scholar] [CrossRef] [PubMed]
- Dubé, E.; Laberge, C.; Guay, M.; Bramadat, P.; Roy, R.; Bettinger, J.A. Vaccine hesitancy: An overview. Hum. Vaccines Immunother. 2013, 9, 1763–1773. [Google Scholar] [CrossRef] [PubMed]
- Dubé, E.; Vivion, M.; MacDonald, N.E. Vaccine hesitancy, vaccine refusal and the anti-vaccine movement: Influence, impact and implications. Expert Rev. Vaccines 2014, 14, 99–117. [Google Scholar] [CrossRef] [PubMed]
- Gilmour, J.; Harrison, C.; Asadi, L.; Cohen, M.H.; Vohra, S. Childhood Immunization: When Physicians and Parents Disagree. Pediatrics 2011, 128, S167–S174. [Google Scholar] [CrossRef]
- Glanz, J.M.; Kraus, C.R.; Daley, M.F. Addressing Parental Vaccine Concerns: Engagement, Balance, and Timing. PLoS Biol. 2015, 13, e1002227. [Google Scholar] [CrossRef]
- Glanz, J.M.; Newcomer, S.R.; Jackson, M.L.; Omer, S.B.; Bednarczyk, R.A.; Shoup, J.A.; DeStefano, F.; Daley, M.F.; Goddard, K.; Panneton, M.; et al. White Paper on studying the safety of the childhood immunization schedule in the Vaccine Safety Datalink. Vaccine 2016, 34, A1–A29. [Google Scholar] [CrossRef]
- Gupta, K.; Chen, M.; Rocker, J. Measles: Taking steps forward to prevent going backwards. Curr. Opin. Pediatr. 2020, 32, 436–445. [Google Scholar] [CrossRef] [PubMed]
- Healy, C.M.; Pickering, L.K. How to communicate with vaccine-hesitant parents. Pediatrics 2011, 127, S127–S133. [Google Scholar] [CrossRef]
- Hulsey, E.; Bland, T. Immune overload: Parental attitudes toward combination and single antigen vaccines. Vaccine 2015, 33, 2546–2550. [Google Scholar] [CrossRef] [PubMed]
- Jacobson, R. Vaccinations: A public health triumph and a public relations tragedy. Minn. Med. 2012, 95, 36–40. [Google Scholar]
- Jacobson, R.M.; St Sauver, J.L.; Finney Rutten, L.J. Vaccine Hesitancy. Mayo Clin. Proc. 2015, 90, 1562–1568. [Google Scholar] [CrossRef]
- Johnson, M. Motivational Interviewing for Vaccine Hesitant Parents. Master’s Thesis, Boston University, Boston, MA, USA, 2017. [Google Scholar]
- Keeton, V.F.; Chen, A.K. Immunization updates and challenges. Curr. Opin. Pediatr. 2010, 22, 234–240. [Google Scholar] [CrossRef] [PubMed]
- Kubin, L. Is There a Resurgence of Vaccine Preventable Diseases in the US? J. Pediatr. Nurs. 2019, 44, 115–118. [Google Scholar] [CrossRef]
- Lantos, J.D.; Jackson, M.A.; Opel, D.J.; Marcuse, E.K.; Myers, A.L.; Connelly, B.L. Controversies in Vaccine Mandates. Curr. Probl. Pediatr. Adolesc. Health Care 2010, 40, 38–58. [Google Scholar] [CrossRef]
- Loehr, J. Communicating about Immunizations. Prim. Care Clin. Off. Pract. 2020, 47, 419–430. [Google Scholar] [CrossRef] [PubMed]
- Luthy, K.E.; Burningham, J.; Eden, L.M.; MacIntosh, J.L.B.; Beckstrand, R.L. Addressing Parental Vaccination Questions in the School Setting. J. Sch. Nurs. 2016, 32, 47–57. [Google Scholar] [CrossRef]
- Marcus, B. A Nursing Approach to the Largest Measles Outbreak in Recent US History: Lessons Learned Battling Homegrown Vaccine Hesitancy. Online J. Issues Nurs. 2020, 25, 3. [Google Scholar] [CrossRef]
- Olusanya, O.A.; Bednarczyk, R.A.; Davis, R.L.; Shaban-Nejad, A. Addressing Parental Vaccine Hesitancy and Other Barriers to Childhood/Adolescent Vaccination Uptake during the Coronavirus (COVID-19) Pandemic. Front. Immunol. 2021, 12, 663074. [Google Scholar] [CrossRef] [PubMed]
- Omer, S.B.; Salmon, D.A.; Orenstein, W.A.; Dehart, M.P.; Halsey, N. Vaccine Refusal, Mandatory Immunization, and the Risks of Vaccine-Preventable Diseases. N. Engl. J. Med. 2009, 360, 1981–1988. [Google Scholar] [CrossRef]
- Papachrisanthou, M.M.; Davis, R.L. The Resurgence of Measles, Mumps, and Pertussis. J. Nurse Pract. 2019, 15, 391–395. [Google Scholar] [CrossRef]
- Paquette, E.T. In the Wake of a Pandemic: Revisiting School Approaches to Nonmedical Exemptions to Mandatory Vaccination in the US. J. Pediatr. 2021, 231, 17–23. [Google Scholar] [CrossRef]
- Pierik, R. On religious and secular exemptions: A case study of childhood vaccination waivers. Ethnicities 2017, 17, 220–241. [Google Scholar] [CrossRef] [PubMed]
- Schmidt, K. Measles and Vaccination: A Resurrected Disease, A Conflicted Response. J. Christ. Nurs. 2019, 36, 214–221. [Google Scholar] [CrossRef]
- Siddiqui, M.; Salmon, D.A.; Omer, S.B. Epidemiology of vaccine hesitancy in the United States. Hum. Vaccines Immunother. 2013, 9, 2643–2648. [Google Scholar] [CrossRef]
- Smith, M.J. Promoting Vaccine Confidence. Infect. Dis. Clin. N. Am. 2015, 29, 759–769. [Google Scholar] [CrossRef]
- Smith, T.C. Vaccine Rejection and Hesitancy: A Review and Call to Action. Open Forum Infect. Dis. 2017, 4, ofx146. [Google Scholar] [CrossRef]
- Tankwanchi, A.S.; Bowman, B.; Garrison, M.; Larson, H.; Wiysonge, C.S. Vaccine hesitancy in migrant communities: A rapid review of latest evidence. Curr. Opin. Immunol. 2021, 71, 62–68. [Google Scholar] [CrossRef]
- Tokish, H.; Solanto, M.V. The problem of vaccination refusal. Curr. Opin. Pediatr. 2020, 32, 683–693. [Google Scholar] [CrossRef]
- Williams, S.E. What are the factors that contribute to parental vaccine-hesitancy and what can we do about it? Hum. Vaccines Immunother. 2014, 10, 2584–2596. [Google Scholar] [CrossRef]
- Wilson, K.; Atkinson, K.; Deeks, S. Opportunities for utilizing new technologies to increase vaccine confidence. Expert Rev. Vaccines 2014, 13, 969–977. [Google Scholar] [CrossRef]
- Wood, D.L.; American Academy of Pediatrics Committee on Community Health Services; American Academy of Pediatrics Committee on Practice and Ambulatory Medicine. Increasing immunization coverage. Pediatrics 2003, 112, 993–996. [Google Scholar] [CrossRef]
- International Conference on Primary Health Care. Declaration of Alma-Ata. Available online: https://www.who.int/teams/social-determinants-of-health/declaration-of-alma-ata (accessed on 10 November 2021).
- Jarrett, C.; Wilson, R.; O’Leary, M.; Eckersberger, E.; Larson, H.J.; Eskola, J.; Liang, X.; Chaudhuri, M.; Dube, E.; Gellin, B.; et al. Strategies for Addressing Vaccine Hesitancy: A Systematic Review. Vaccine 2015, 33, 4180–4190. [Google Scholar] [CrossRef]
- The Lancet Child & Adolescent Health. Vaccine hesitancy: A generation at risk. Lancet Child Adolesc. Health 2019, 3, 281. [Google Scholar] [CrossRef]
- US Health Resources & Services Administration. “Vaccine Hesitancy” Fuels Outbreaks. Available online: https://www.hrsa.gov/enews/past-issues/2019/september-19/vaccine-hesitancy-fuels-outbreaks (accessed on 27 May 2021).
- Puri, N.; Coomes, E.A.; Haghbayan, H.; Gunaratne, K. Social media and vaccine hesitancy: New updates for the era of COVID-19 and globalized infectious diseases. Hum. Vaccines Immunother. 2020, 16, 2586–2593. [Google Scholar] [CrossRef]
- McKee, C.; Bohannon, K. Exploring the Reasons behind Parental Refusal of Vaccines. J. Pediatr. Pharmacol. Ther. 2016, 21, 104–109. [Google Scholar] [CrossRef]
- Gust, D.; Brown, C.; Sheedy, K.; Hibbs, B.; Weaver, D.; Nowak, G. Immunization attitudes and beliefs among parents: Beyond a dichotomous perspective. Am. J. Health Behav. 2005, 29, 81–92. [Google Scholar] [CrossRef]
- Leask, J.; Kinnersley, P.; Jackson, C.; Cheater, F.; Bedford, H.; Rowles, G. Communicating with parents about vaccination: A framework for health professionals. BMC Pediatr. 2012, 12, 154. [Google Scholar] [CrossRef]
- Smith, P.J.; Chu, S.Y.; Barker, L.E. Children Who Have Received No Vaccines: Who Are They and Where Do They Live? Pediatrics 2004, 114, 187–195. [Google Scholar] [CrossRef]
- Kennedy, A.M.; Brown, C.J.; Gust, D.A. Vaccine Beliefs of Parents Who Oppose Compulsory Vaccination. Public Health Rep. 2005, 120, 252–258. [Google Scholar] [CrossRef]
- Adler, R.S.; Pittle, R.D. Cajolery or command: Are education campaigns an adequate substitute for regulation? Yale J. Regul. 1984, 1, 159–193. [Google Scholar]
- Nagata, J.M.; Hernández-Ramos, I.; Kurup, A.S.; Albrecht, D.; Vivas-Torrealba, C.; Franco-Paredes, C. Social determinants of health and seasonal influenza vaccination in adults ≥65 years: A systematic review of qualitative and quantitative data. BMC Public Health 2013, 13, 388. [Google Scholar] [CrossRef]
- Goldlust, S.; Lee, E.C.; Haran, M.; Rohani, P.; Bansal, S. Assessing the distribution and determinants of vaccine underutilization in the United States. bioRxiv 2017, 113043. [Google Scholar] [CrossRef]
- Wood, D.; Donald-Sherbourne, C.; Halfon, N.; Tucker, M.B.; Ortiz, V.; Hamlin, J.S.; Duan, N.; Mazel, R.M.; Grabowsky, M.; Brunell, P.; et al. Factors Related to Immunization Status among Inner-City Latino and African-American Preschoolers. Pediatrics 1995, 96, 295–301. [Google Scholar] [CrossRef]
- Luman, E.T.; McCauley, M.M.M.; Shefer, A.; Chu, S.Y. Maternal Characteristics Associated with Vaccination of Young Children. Pediatrics 2003, 111, 1215–1218. [Google Scholar] [CrossRef]
- Gardner, L.; Dong, E.; Khan, K.; Sarkar, S. Persistence of US measles risk due to vaccine hesitancy and outbreaks abroad. Lancet Infect. Dis. 2020, 20, 1114–1115. [Google Scholar] [CrossRef]
- Garnier, R.; Nedell, E.R.; Omer, S.B.; Bansal, S. Getting Personal: How Childhood Vaccination Policies Shape the Landscape of Vaccine Exemptions. Open Forum Infect. Dis. 2020, 7, ofaa088. [Google Scholar] [CrossRef]
- Colgrove, J.; Lowin, A. A Tale of Two States: Mississippi, West Virginia, and Exemptions to Compulsory School Vaccination Laws. Health Aff. 2016, 35, 348–355. [Google Scholar] [CrossRef]
- Opel, D.J.; Kronman, M.P.; Diekema, D.S.; Marcuse, E.K.; Duchin, J.S.; Kodish, E. Childhood Vaccine Exemption Policy: The Case for a Less Restrictive Alternative. Pediatrics 2016, 137, e20154230. [Google Scholar] [CrossRef]
- California Legislative Information. SB-277 Public Health: Vaccinations. Available online: https://leginfo.legislature.ca.gov/faces/billTextClient.xhtml?bill_id=201520160SB277 (accessed on 11 November 2021).
- Delamater, P.; Leslie, T.; Yang, Y.T. Change in Medical Exemptions from Immunization in California after Elimination of Personal Belief Exemptions. JAMA 2017, 318, 863–864. [Google Scholar] [CrossRef]
- California Department of Public Health Immunization Branch. 2018–2019 Kindergarten Immunization Assessment—Executive Summary. Available online: https://eziz.org/assets/docs/shotsforschool/2018-19CAKindergartenSummaryReport.pdf (accessed on 11 November 2021).
- Karlamangla, S.; Poindexter, S. Despite California’s Strict New Law, Hundreds of Schools Still Don’t Have Enough Vaccinated Kids. Los Angeles Times, 13 August 2017. [Google Scholar]
- California Legislative Information. SB-276 Immunizations: Medical Exemptions. Available online: https://leginfo.legislature.ca.gov/faces/billTextClient.xhtml?bill_id=201920200SB276 (accessed on 11 November 2021).
- Lo, N.C.; Hotez, P.J. Public Health and Economic Consequences of Vaccine Hesitancy for Measles in the United States. JAMA Pediatr. 2017, 171, 887–892. [Google Scholar] [CrossRef]
- Centers for Disease Control and Prevention. The Journey of Your Child’s Vaccine. Available online: https://www.cdc.gov/vaccines/parents/infographics/journey-of-child-vaccine.html (accessed on 27 May 2021).


{kind=link}
| Demographic Variable and Total Number of Articles per Variable | Relationships Mentioned or Observed in Articles | Number of Articles | Summary |
|---|---|---|---|
| Parental Age (15 articles) | Older parental age and higher vaccine hesitancy | 7 | Several articles included in the review noted higher vaccine hesitancy among older parents (≥30 years of age) in association with education, income, marital status, and number of children. |
| Younger parental age and higher vaccine hesitancy | 4 | ||
| No relationship observed between parental age and vaccine hesitancy | 4 | ||
| Parental Race/Ethnicity (30 articles) | Non-Hispanic White race and higher vaccine hesitancy | 15 | Several articles included in the review cited higher vaccine hesitancy and vaccine refusal among non-Hispanic White parents. Unvaccinated or undervaccinated children were more likely to be White and/or have parents with NMEs *. |
| Non-White race and higher vaccine hesitancy | 11 | ||
| Other race/ethnicity findings | 4 | ||
| Education (39 articles) | Higher level of parental education and higher vaccine hesitancy | 17 | Contrasting patterns were noted as to level of education. Several articles included in the review noted higher vaccine hesitancy among parents with college education or higher. Almost the same number of articles mentioned higher vaccine hesitancy among parents with lower education. Vaccine hesitant parents were more likely to enroll their children in private, charter, or home-based schools. |
| Lower level of parental education and higher vaccine hesitancy | 15 | ||
| No relationship observed between level of parental education and vaccine hesitancy | 4 | ||
| Higher level of parental education and lower vaccine hesitancy | 1 | ||
| Private, charter, or home-based schools and higher vaccine hesitancy | 2 | ||
| Income/Socioeconomic Status (SES) (26 articles) | Higher SES/income and higher vaccine hesitancy | 12 | Contrasting patterns were noted as to income/socio-economic status. An equal number of articles included in the review noted vaccine hesitancy in association with both higher and lower income/SES. |
| Lower SES/income and higher vaccine hesitancy | 11 | ||
| No relationship observed between SES/income and vaccine hesitancy | 3 | ||
| Health Insurance (5 articles) | Health or private insurance and vaccine hesitancy | 3 | Having health insurance and/or the type of health insurance influenced vaccine hesitancy. |
| Public/lack of health insurance and vaccine hesitancy | 2 | ||
| Social Influences/Social Network (2 articles) | Place-based ideological sorting as to socio-economic status, political affiliations, or religious beliefs and higher vaccine hesitancy | 1 | Social networks and geographical patterns in ideological clustering of NMEs influenced vaccine hesitancy. |
| Local spread of vaccine beliefs via parental social networks and higher vaccine hesitancy | 1 | ||
| Policies/Political Affiliation (10 articles) | Policies (ex. SB277, NMEs, vaccine policies) Parents who identified as Democrat and higher vaccine hesitancy | 8 | Policies (NMEs and vaccine-specific policies) influenced vaccine hesitancy. Higher vaccine hesitancy was noted among parents who filed for NMEs. |
| Parents who identified as Republican/Conservatives and vaccine hesitancy | 1 | ||
| Parents who identified as neither Democrat nor Republican and vaccine hesitancy | 1 | ||
| Religion/Religiosity (5 articles) | Higher religiosity/religious objections and higher vaccine hesitancy | 3 | Religious beliefs and objections influenced vaccine hesitancy and outbreaks in measles cases. |
| Ultra-Orthodox Jewish communities in New York and higher vaccine hesitancy | 2 | ||
| Urban/Rural Areas (2 articles) | Residing in non-metropolitan statistical areas (MSA) or rural areas and vaccine hesitancy | 1 | Residing in rural vs. urban areas influenced vaccine hesitancy. Residing in rural areas and lack of insurance were associated with undervaccination. |
| Residing in certain MSA and in rural areas and vaccine hesitancy | 1 | ||
| Chronic Conditions (3 articles) | Parents of children with Autism Spectrum Disorder (ASD) or Down Syndrome and higher vaccine hesitancy | 3 | Being a parent with a child diagnosed with Autism Spectrum Disorder or Down Syndrome influenced vaccine hesitancy. |
| Marital Status (9 articles) | Married parents and higher vaccine hesitancy | 7 | Higher vaccine hesitancy was noted among married vs. single parents. |
| Single parents and higher vaccine hesitancy | 2 |
| Theme | Belief | General Vaccines f (%) | MMR † Specific f (%) |
|---|---|---|---|
| Danger/risk | Vaccine adverse reactions/hypersensitivity reactions | 86 (75) | 36 (31) |
| General/other safety concerns | 54 (47) | 18 (16) | |
| Risk of autism | 49 (43) | 62 (54) | |
| Overwhelms immune system | 37 (32) | 1 (1) | |
| Concerns with vaccine components | 33 (29) | 13 (11) | |
| Pain on injection site | 26 (23) | 6 (5) | |
| Personal concern | Too many vaccines/concerns with vaccine schedule | 49 (43) | 9 (8) |
| Mistrust of government and health officials | 45 (39) | 9 (8) | |
| Preference for natural immunity | 31 (27) | 3 (3) | |
| Philosophical/moral objection | 27 (23) | 5 (4) | |
| Cost or access to vaccines | 26 (23) | 6 (5) | |
| Religious opposition | 24 (21) | 8 (7) | |
| Perceived benefits | Low perceived benefit/susceptibility | 45 (39) | 14 (12) |
| Vaccine efficacy concerns | 26 (23) | 8 (7) | |
| Not recommended by healthcare provider | 7 (6) | 0 (0) |
| Source | Parent Category | ||
|---|---|---|---|
| Hesitant f (%) | Compliant f (%) | Not Specified f (%) | |
| Healthcare sources | 44 (38) | 56 (49) | 68 (59) |
| Internet/social media | 52 (45) | 25 (22) | 52 (45) |
| Word of mouth | 37 (32) | 18 (16) | 40 (35) |
| Print/broadcast media | 21 (18) | 15 (13) | 25 (22) |
| Source | Parent Category | ||
|---|---|---|---|
| Hesitant f (%) | Compliant f (%) | Not Specified f (%) | |
| Healthcare sources | 31 (27) | 46 (40) | 45 (39) |
| Internet/social media | 16 (14) | 6 (5) | 9 (8) |
| Word of mouth | 15 (13) | 5 (4) | 6 (5) |
| Print/broadcast media | 4 (3) | 2 (2) | 4 (3) |
| Social Determinant | Facilitating f (%) | Hindering f (%) |
|---|---|---|
| Primary care/healthcare | 46 (40) | 38 (33) |
| Education | 30 (26) | 38 (33) |
| Government/political | 21 (18) | 26 (23) |
| Psychosocial/behavioral | 20 (17) | 47 (41) |
| Public health | 19 (17) | 17 (15) |
| Economy/income | 18 (16) | 30 (26) |
| Environment/built environment | 4 (3) | 9 (8) |
| Housing | 4 (3) | 6 (5) |
| Employment | 2 (2) | 3 (3) |
| Transportation | 2 (2) | 4 (3) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Novilla, M.L.B.; Goates, M.C.; Redelfs, A.H.; Quenzer, M.; Novilla, L.K.B.; Leffler, T.; Holt, C.A.; Doria, R.B.; Dang, M.T.; Hewitt, M.; et al. Why Parents Say No to Having Their Children Vaccinated against Measles: A Systematic Review of the Social Determinants of Parental Perceptions on MMR Vaccine Hesitancy. Vaccines 2023, 11, 926. https://doi.org/10.3390/vaccines11050926
Novilla MLB, Goates MC, Redelfs AH, Quenzer M, Novilla LKB, Leffler T, Holt CA, Doria RB, Dang MT, Hewitt M, et al. Why Parents Say No to Having Their Children Vaccinated against Measles: A Systematic Review of the Social Determinants of Parental Perceptions on MMR Vaccine Hesitancy. Vaccines. 2023; 11(5):926. https://doi.org/10.3390/vaccines11050926
Chicago/Turabian StyleNovilla, M. Lelinneth B., Michael C. Goates, Alisha H. Redelfs, Mallory Quenzer, Lynneth Kirsten B. Novilla, Tyler Leffler, Christian A. Holt, Russell B. Doria, Michael T. Dang, Melissa Hewitt, and et al. 2023. "Why Parents Say No to Having Their Children Vaccinated against Measles: A Systematic Review of the Social Determinants of Parental Perceptions on MMR Vaccine Hesitancy" Vaccines 11, no. 5: 926. https://doi.org/10.3390/vaccines11050926