
Pustular Eruption following COVID-19 Vaccination: A Narrative Case-Based Review

 ,
,
Abstract
:1. Introduction
2. Case Presentation
3. Methods
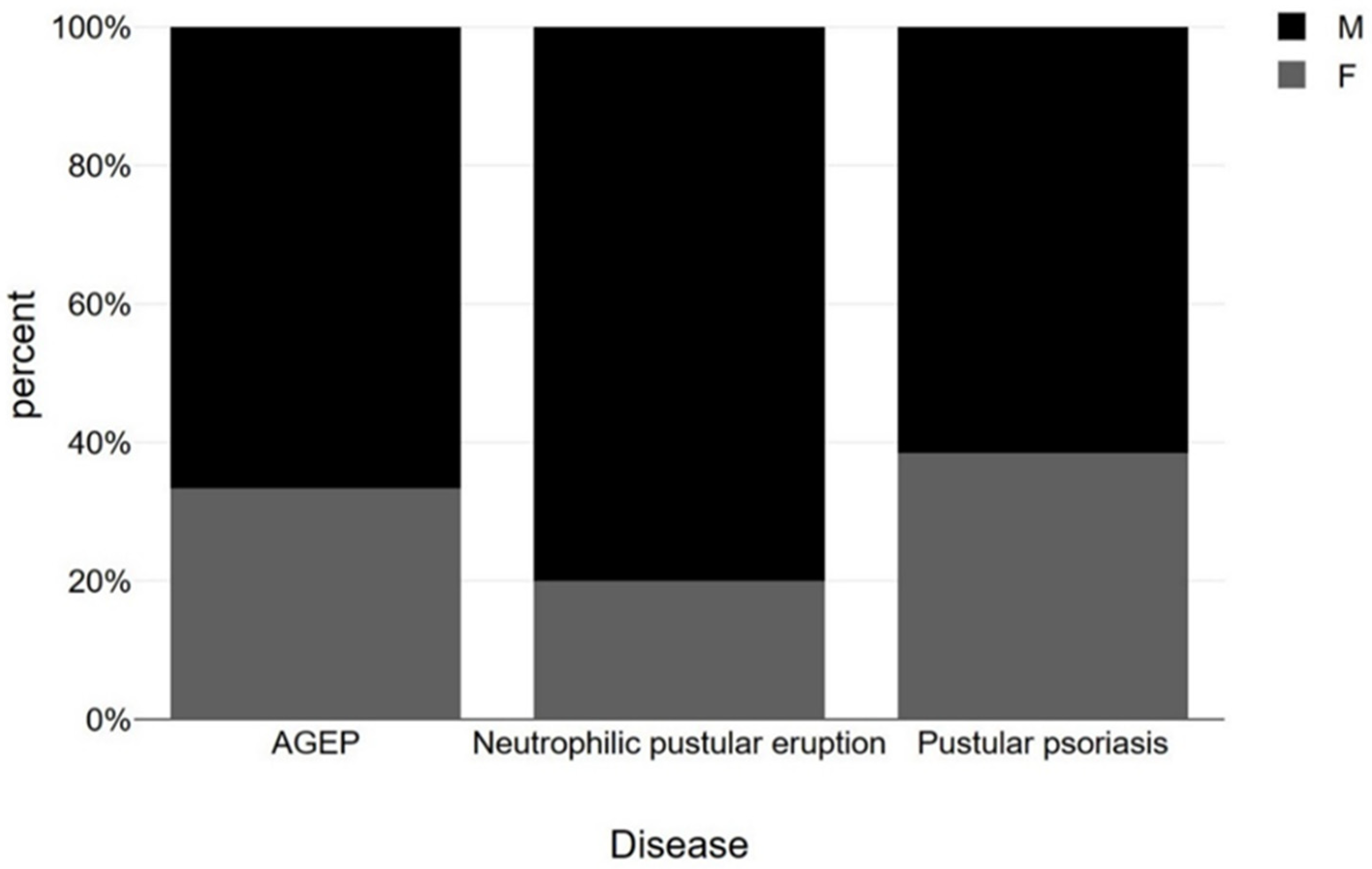
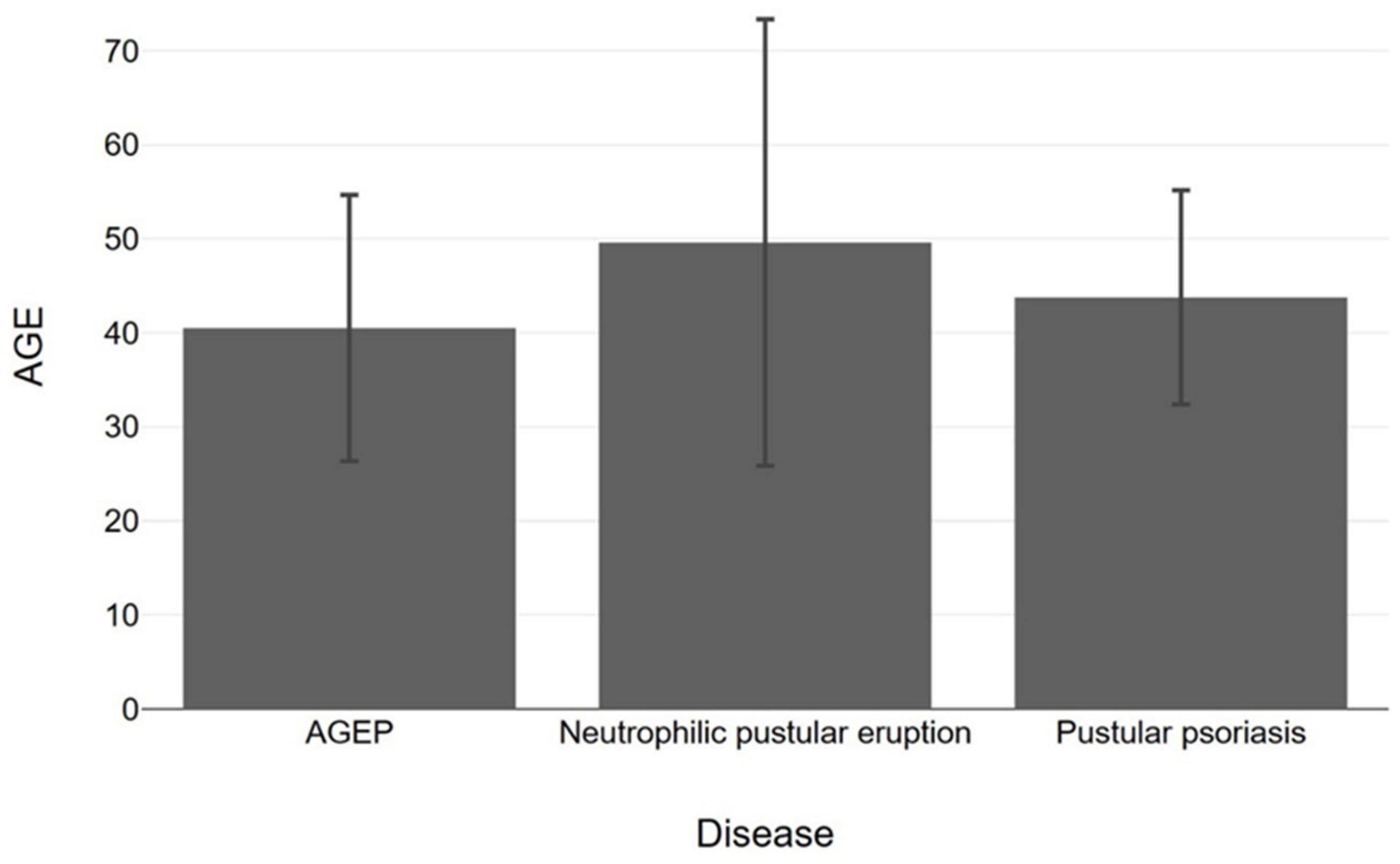
4. Results

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Study | Disease | Sex | Age | Clinical Outcome | Days after Vaccination | Vaccine | Dose of Vaccination | Treatment Strategy |
|---|---|---|---|---|---|---|---|---|
| [19] | Pustular psoriasis (Flare) | M | 72 | Generalized pustular psoriasis | 4 days | Sinovac | First | Acitretin and intravenous Infliximab |
| [20] | Pustular psoriasis (Flare) | F | 22 | Generalized pustular psoriasis | 3 days | Pfizer | First | Not Mentioned |
| [21] | Pustular psoriasis (Flare) | M | 21 | Generalized pustular psoriasis and erythroderma | 4 days | Pfizer | Second | Anti-TNF biologic agent |
| [22] | Pustular psoriasis (Flare) | F | 60 | Generalized pustular psoriasis and erythroderma | 8 days | Pfizer | Second | Oral etretinate |
| [22] | Pustular psoriasis (Flare) | M | 18 | Generalized pustular psoriasis and erythroderma | 7 days | Pfizer | First | Cyclosporine and secukinumab |
| [23] | Pustular psoriasis (Flare) | M | 40 | Generalized pustular psoriasis and erythroderma | 5 days | Pfizer | First | Cyclosporine and infliximab |
| [24] | Pustular psoriasis (Flare) | F | 47 | Generalized pustular psoriasis and erythroderma | 10 days | Pfizer | Second | Risankizumab |
| [25] | Pustular psoriasis (Flare) | M | 65 | Generalized pustular psoriasis and erythroderma with systemic capillary leak syndrome | 12 days | Pfizer | Second | secukinumab |
| [26] | Pustular psoriasis (Flare) | M | 53 | Scales and pustules | 4 days | BBIBP-CorV | First | Neotigason and systemic steroids. |
| [27] | Pustular psoriasis (Flare) | M | 21 | Generalized pustular psoriasis | 4 days | covaxin | First | Acitretin |
| [28] | Pustular psoriasis (New onset) | F | 64 | Erythema, scales, annular pustular psoriasis | NM | Pfizer | First | Methotrexate |
| [29] | Pustular psoriasis (New onset) | F | 66 | Erythema and pustules | 21 days | AstraZeneca | First | Acitretin |
| [30] | Pustular psoriasis (New onset) | M | 20 | Erythema, pustules, crusts | 4 days | Pfizer | First | Acitretin |
| [31] | Sneddon-Wilkinson | M | 21 | Vesiculopustular eruption and crust | 8 days | Moderna | Second | Prednisone |
| [32] | Sweet-syndrome (pustular eruption) | M | 77 | Pustular eruption, encephalitis, myoclonus | 2 days | Moderna | First | Prednisolone |
| [7] | Neutrophilic pustular eruption | M | 32 | Erythematous papulonodules and pustules and aphthous stomatitis with painful genital erosions | 5 days | ChAdOx1 | First | Dapsone and antibiotic treatment |
| Study | Disease Type | Sex | Age | Clinical Outcome | Days after Vaccination | Vaccine Type | Dose of Vaccination | Treatment Strategy |
|---|---|---|---|---|---|---|---|---|
| [15] | AGEP (With DRESS characteristics in follow-up) | F | 40 | Pustules and suberythema | 7 and 11 weeks after first and second dose | First and Second | Pfizer | Prednisolone |
| [16] | AGEP-DRESS | M | 43 | Erythematous edematous papules, plaques and pustules | Hours (1 day) | Second | Moderna | Prednisolone |
| [33] | AGEP | F | 32 | Erythema and pustules | 3 weeks | First | ChAdOx1 | Topical treatment |
| [34] | AGEP | M | 27 | Erythema and pustules | Hours (1 day) | First | Moderna | Not mentioned |
| [17] | AGEP | M | 27 | Erythema and pustules | 8 days | First | Moderna | Prednisolone |
| [18] | AGEP | M | 74 | Erythematous plaques and pustules | 1 day | First | Janssen Ad26.COV2.S | Prednisolone and topical treatment |
5. Discussion
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Graña, C.; Ghosn, L.; Evrenoglou, T.; Jarde, A.; Minozzi, S.; Bergman, H.; Buckley, B.S.; Probyn, K.; Villanueva, G.; Henschke, N.; et al. Efficacy and Safety of COVID-19 Vaccines. Cochrane Database Syst. Rev. 2022, 12, CD015477. [Google Scholar] [CrossRef] [PubMed]
- Mascellino, M.T.; Di Timoteo, F.; De Angelis, M.; Oliva, A. Overview of the Main Anti-SARS-CoV-2 Vaccines: Mechanism of Action, Efficacy and Safety. Infect. Drug Resist. 2021, 14, 3459–3476. [Google Scholar] [CrossRef] [PubMed]
- Martora, F.; Battista, T.; Marasca, C.; Genco, L.; Fabbrocini, G.; Potestio, L. Cutaneous Reactions Following COVID-19 Vaccination: A Review of the Current Literature. Clin. Cosmet. Investig. Dermatol. 2022, 15, 2369–2382. [Google Scholar] [CrossRef] [PubMed]
- Shafie’ei, M.; Jamali, M.; Akbari, Z.; Sarvipour, N.; Ahmadzade, M.; Ahramiyanpour, N. Cutaneous Adverse Reactions Following COVID-19 Vaccinations: A Systematic Review and Meta-Analysis. J. Cosmet. Dermatol. 2022, 21, 3636–3650. [Google Scholar] [CrossRef] [PubMed]
- Wu, P.-C.; Huang, I.-H.; Wang, C.-W.; Tsai, C.-C.; Chung, W.-H.; Chen, C.-B. New Onset and Exacerbations of Psoriasis Following COVID-19 Vaccines: A Systematic Review. Am. J. Clin. Dermatol. 2022, 23, 775–799. [Google Scholar] [CrossRef]
- Parisi, R.; Shah, H.; Navarini, A.A.; Muehleisen, B.; Ziv, M.; Shear, N.H.; Dodiuk-Gad, R.P. Acute Generalized Exanthematous Pustulosis: Clinical Features, Differential Diagnosis, and Management. Am. J. Clin. Dermatol. 2023, 24, 557–575. [Google Scholar] [CrossRef]
- Bhargava, A.; Kharkar, V.; Mahajan, S.; Gole, P. Neutrophilic Pustular Eruption with Behcet’s Like Illness Post Covid-19 Vaccination. Indian. Dermatol. Online J. 2022, 13, 493–496. [Google Scholar] [CrossRef]
- Rikitake, S.; Kokubu, H.; Yamamoto, B.; Manabe, T.; Fujimoto, N. Eosinophilic Pustular Folliculitis Developing at the Site of COVID-19 Vaccination. Clin. Exp. Dermatol. 2022, 47, 2022–2024. [Google Scholar] [CrossRef]
- Mengesha, Y.M.; Bennett, M.L. Pustular Skin Disorders. Am. J. Clin. Dermatol. 2002, 3, 389–400. [Google Scholar] [CrossRef]
- Johnston, A.; Xing, X.; Wolterink, L.; Barnes, D.H.; Yin, Z.; Reingold, L.; Kahlenberg, J.M.; Harms, P.W.; Gudjonsson, J.E. IL-1 and IL-36 Are Dominant Cytokines in Generalized Pustular Psoriasis. J. Allergy Clin. Immunol. 2017, 140, 109–120. [Google Scholar] [CrossRef] [Green Version]
- Tahtinen, S.; Tong, A.-J.; Himmels, P.; Oh, J.; Paler-Martinez, A.; Kim, L.; Wichner, S.; Oei, Y.; McCarron, M.J.; Freund, E.C.; et al. IL-1 and IL-1ra Are Key Regulators of the Inflammatory Response to RNA Vaccines. Nat. Immunol. 2022, 23, 532–542. [Google Scholar] [CrossRef]
- Karampinis, E.; Goudouras, G.; Ntavari, N.; Bogdanos, D.P.; Roussaki-Schulze, A.-V.; Zafiriou, E. Serum Vitamin D Levels Can Be Predictive of Psoriasis Flares up after COVID-19 Vaccination: A Retrospective Case Control Study. Front. Med. 2023, 10, 1203426. [Google Scholar] [CrossRef] [PubMed]
- Mössner, R.; Wilsmann-Theis, D.; Oji, V.; Gkogkolou, P.; Löhr, S.; Schulz, P.; Körber, A.; Prinz, J.C.; Renner, R.; Schäkel, K.; et al. The Genetic Basis for Most Patients with Pustular Skin Disease Remains Elusive. Br. J. Dermatol. 2018, 178, 740–748. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rouai, M.; Slimane, M.B.; Sassi, W.; Alaoui, F.; Chelly, I.; Mokni, M. Pustular Rash Triggered by Pfizer-BioNTech COVID-19 Vaccination: A Case Report. Dermatol. Ther. 2022, 35, e15465. [Google Scholar] [CrossRef]
- Tay, W.C.; Lee, J.S.S.; Chong, W.-S. Tozinameran (Pfizer-BioNTech COVID-19 Vaccine)-Induced AGEP-DRESS Syndrome. Ann. Acad. Med. Singap. 2022, 51, 796–797. [Google Scholar] [CrossRef] [PubMed]
- Ikeda, T.; Yokoyama, K.; Kawakami, T. Overlapping Acute Generalized Exanthematous Pustulosis Drug Reaction with Eosinophilia and Systemic Symptoms Induced by a Second Dose of the Moderna COVID-19 Vaccine. J. Dermatol. 2022, 49, e446–e447. [Google Scholar] [CrossRef] [PubMed]
- Mitri, F.; Toberer, F.; Enk, A.H.; Hartmann, M. Acute Generalized Exanthematous Pustulosis in Close Temporal Association with mRNA-1273 Vaccine. Acta Derm. Venereol. 2021, 101, adv00596. [Google Scholar] [CrossRef]
- Lospinoso, K.; Nichols, C.S.; Malachowski, S.J.; Mochel, M.C.; Nutan, F. A Case of Severe Cutaneous Adverse Reaction Following Administration of the Janssen Ad26.COV2.S COVID-19 Vaccine. JAAD Case Rep. 2021, 13, 134–137. [Google Scholar] [CrossRef]
- Onsun, N.; Kaya, G.; Işık, B.G.; Güneş, B. A Generalized Pustular Psoriasis Flare after CoronaVac COVID-19 Vaccination: Case Report. Health Promot. Perspect. 2021, 11, 261–262. [Google Scholar] [CrossRef]
- Durmaz, I.; Turkmen, D.; Altunisik, N.; Toplu, S.A. Exacerbations of Generalized Pustular Psoriasis, Palmoplantar Psoriasis, and Psoriasis Vulgaris after MRNA COVID-19 Vaccine: A Report of Three Cases. Dermatol. Ther. 2022, 35, e15331. [Google Scholar] [CrossRef]
- Almeida, R.O.; Hanemann, T.; Peres, F.L.X.; Escobar, G.F.; Rangel Bonamigo, R. Reactivation of Pustular Psoriasis Following MRNA Vaccination versus COVID-19 Infection: An Overlap?: Reply to “Generalized Pustular Psoriasis Following COVID-19” by Dadras MS et al.: Reply to “Generalized Pustular Psoriasis Following COVID-19” by Dadras MS et al. Dermatol. Ther. 2022, 35, e15892. [Google Scholar] [CrossRef] [PubMed]
- Tachibana, K.; Kawakami, Y.; Tokuda, M.; Sato, S.; Sugihara, S.; Miyake, T.; Sugiura, K.; Morizane, S. Flare-up of generalized pustular psoriasis following Pfizer-BioNTech BNT162b2 mRNA COVID-19 vaccine: Two cases without mutations of IL36RN and CARD14 genes. J. Dermatol. 2022, 49, e393–e394. [Google Scholar] [CrossRef] [PubMed]
- Perna, D.; Jones, J.; Schadt, C.R. Acute Generalized Pustular Psoriasis Exacerbated by the COVID-19 Vaccine. JAAD Case Rep. 2021, 17, 1–3. [Google Scholar] [CrossRef]
- Pavia, G.; Gargiulo, L.; Spinelli, F.; Avagliano, J.; Valenti, M.; Borroni, R.G.; Costanzo, A.; Narcisi, A. Generalized Pustular Psoriasis Flare in a Patient Affected by Plaque Psoriasis after BNT162b2 mRNA COVID-19 Vaccine, Successfully Treated with Risankizumab. J. Eur. Acad. Dermatol. Venereol. 2022, 36, e502–e505. [Google Scholar] [CrossRef]
- Yatsuzuka, K.; Murakami, M.; Kuroo, Y.; Fukui, M.; Yoshida, S.; Muto, J.; Shiraishi, K.; Sayama, K. Flare-up of Generalized Pustular Psoriasis Combined with Systemic Capillary Leak Syndrome after Coronavirus Disease 2019 MRNA Vaccination. J. Dermatol. 2022, 49, 454–458. [Google Scholar] [CrossRef] [PubMed]
- Dayani, D.; Rokhafrouz, H.; Balighi, K. Generalized Pustular Psoriasis Flare-Up after Both Doses of BBIBP-CorV Vaccination in a Patient under Adalimumab Treatment: A Case Report. Case Rep. Dermatol. 2023, 15, 61–65. [Google Scholar] [CrossRef]
- Infimate, D.L.; Yumnam, D.; Galagali, S.S.; Kabi, A.; Kaeley, N. Psoriasis Flare-Up After COVAXIN BBV152 Whole Virion Inactivated Vaccine. Cureus 2022, 14, e22311. [Google Scholar] [CrossRef]
- Romagnuolo, M.; Pontini, P.; Muratori, S.; Marzano, A.V.; Moltrasio, C. De Novo Annular Pustular Psoriasis Following MRNA COVID-19 Vaccine. J. Eur. Acad. Dermatol. Venereol. 2022, 36, e603–e605. [Google Scholar] [CrossRef]
- Elamin, S.; Hinds, F.; Tolland, J. De Novo Generalized Pustular Psoriasis Following Oxford-AstraZeneca COVID-19 Vaccine. Clin. Exp. Dermatol. 2022, 47, 153–155. [Google Scholar] [CrossRef]
- Frioui, R.; Chamli, A.; Zaouak, A.; Hlel, I.; Khanchel, F.; Fenniche, S.; Hammami, H. A Case of New-Onset Acute Generalized Pustular Psoriasis Following Pfizer-BioNTech COVID-19 Vaccine. Dermatol. Ther. 2022, 35, e15444. [Google Scholar] [CrossRef]
- McCoy, T.; Shamsian, D.; Pan, A.; Sivamani, R.K. Sneddon-Wilkinson Disease Following COVID-19 Vaccination. Dermatol. Online J. 2023, 29, 12. [Google Scholar] [CrossRef]
- Torrealba-Acosta, G.; Martin, J.C.; Huttenbach, Y.; Garcia, C.R.; Sohail, M.R.; Agarwal, S.K.; Wasko, C.; Bershad, E.M.; Hirzallah, M.I. Acute Encephalitis, Myoclonus and Sweet Syndrome after MRNA-1273 Vaccine. BMJ Case Rep. 2021, 14, e243173. [Google Scholar] [CrossRef]
- Kang, S.-Y.; Park, S.-Y.; Kim, J.-H.; Lee, S.M.; Lee, S.P. COVID-19 Vaccine-Induced Acute Generalized Exanthematous Pustulosis. Korean J. Intern. Med. 2021, 36, 1537–1538. [Google Scholar] [CrossRef] [PubMed]
- Agaronov, A.; Makdesi, C.; Hall, C.S. Acute Generalized Exanthematous Pustulosis Induced by Moderna COVID-19 Messenger RNA Vaccine. JAAD Case Rep. 2021, 16, 96–97. [Google Scholar] [CrossRef] [PubMed]
- Katsuie, S.; Nakamura, K.; Ogawa, E.; Arakura, F.; Okuyama, R. Relapse of Palmoplantar Pustulosis Following COVID-19 Vaccination. Cureus 2022, 14, e28604. [Google Scholar] [CrossRef] [PubMed]
- Piccolo, V.; Russo, T.; Mazzatenta, C.; Bassi, A.; Argenziano, G.; Cutrone, M.; Danielsson Darlington, M.E.S.; Grimalt, R. COVID Vaccine-Induced Pustular Psoriasis in Patients with Previous Plaque Type Psoriasis. J. Eur. Acad. Dermatol. Venereol. 2022, 36, e330–e332. [Google Scholar] [CrossRef]
- Ciccarese, G.; Drago, F.; Rebora, A.; Parodi, A. Two Cases of Papulo-Pustular Rosacea-like Eruptions Following COVID-19 Vaccinations. J. Eur. Acad. Dermatol. Venereol. 2021, 35, e868–e870. [Google Scholar] [CrossRef]
- Merrill, E.D.; Kashem, S.W.; Amerson, E.H.; Pincus, L.B.; Lang, U.E.; Shinkai, K.; Chang, A.Y. Association of Facial Pustular Neutrophilic Eruption With Messenger RNA–1273 SARS-CoV-2 Vaccine. JAMA Dermatol. 2021, 157, 1128. [Google Scholar] [CrossRef]
- Wu, R.-W.; Lin, T.-K. Oxford-AstraZeneca COVID-19 Vaccine-Induced Acute Localized Exanthematous Pustulosis. J. Dermatol. 2021, 48, e562–e563. [Google Scholar] [CrossRef] [PubMed]
- McMahon, D.E.; Amerson, E.; Rosenbach, M.; Lipoff, J.B.; Moustafa, D.; Tyagi, A.; Desai, S.R.; French, L.E.; Lim, H.W.; Thiers, B.H.; et al. Cutaneous Reactions Reported after Moderna and Pfizer COVID-19 Vaccination: A Registry-Based Study of 414 Cases. J. Am. Acad. Dermatol. 2021, 85, 46–55. [Google Scholar] [CrossRef]
- Miladi, R.; Janbakhsh, A.; Babazadeh, A.; Aryanian, Z.; Ebrahimpour, S.; Barary, M.; Sio, T.T.; Wollina, U.; Goldust, M.; Mohseni Afshar, Z. Pustular Psoriasis Flare-up in a Patient with COVID-19. J. Cosmet. Dermatol. 2021, 20, 3364–3368. [Google Scholar] [CrossRef]
- Ayatollahi, A.; Robati, R.M.; Kamyab, K.; Firooz, A. Late-onset AGEP-like skin pustular eruption following COVID-19: A possible association. Dermatol. Ther. 2020, 33, e14275. [Google Scholar] [CrossRef] [PubMed]
- Schwartz, R.A.; Janniger, C.K. Generalized Pustular Figurate Erythema: A Newly Delineated Severe Cutaneous Drug Reaction Linked with Hydroxychloroquine. Dermatol. Ther. 2020, 33, e13380. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Megna, M.; Potestio, L.; Gallo, L.; Caiazzo, G.; Ruggiero, A.; Fabbrocini, G. Reply to “Psoriasis Exacerbation after COVID-19 Vaccination: Report of 14 Cases from a Single Centre” by Sotiriou E et al. J. Eur. Acad. Dermatol. Venereol. 2022, 36, e11–e13. [Google Scholar] [CrossRef]
- Heo, J.Y.; Seo, Y.B.; Kim, E.J.; Lee, J.; Kim, Y.R.; Yoon, J.G.; Noh, J.Y.; Cheong, H.J.; Kim, W.J.; Yoon, S.-Y.; et al. COVID-19 Vaccine Type-Dependent Differences in Immunogenicity and Inflammatory Response: BNT162b2 and ChAdOx1 NCoV-19. Front. Immunol. 2022, 13, 975363. [Google Scholar] [CrossRef]
- Wang, L.; Pan, J.; Jin, H. Profiling and Multivariate Analysis of Serum Cytokines in Patients with Generalized Pustular Psoriasis. Eur. J. Inflamm. 2022, 20, 205873922210764. [Google Scholar] [CrossRef]
- Lalevée, S.; Audureau, E.; Riou, A.; Colin, A.; Anquetin, M.; Barau, C.; Valeyrie-Allanore, L.; Delfau-Larue, M.; Chosidow, O.; Wolkenstein, P.; et al. Acute Generalized Exanthematous Pustulosis and Epidermal Necrolysis Differ in Innate Cytokine Patterns. Clin. Exp. Allergy 2019, 49, 1258–1261. [Google Scholar] [CrossRef] [PubMed]
- Marzano, A.V.; Ortega-Loayza, A.G.; Heath, M.; Morse, D.; Genovese, G.; Cugno, M. Mechanisms of Inflammation in Neutrophil-Mediated Skin Diseases. Front. Immunol. 2019, 10, 1059. [Google Scholar] [CrossRef]
- Murata, K.; Nakao, N.; Ishiuchi, N.; Fukui, T.; Katsuya, N.; Fukumoto, W.; Oka, H.; Yoshikawa, N.; Nagao, T.; Namera, A.; et al. Four Cases of Cytokine Storm after COVID-19 Vaccination: Case Report. Front. Immunol. 2022, 13, 967226. [Google Scholar] [CrossRef]
- Cro, S.; Cornelius, V.R.; Pink, A.E.; Wilson, R.; Pushpa-Rajah, A.; Patel, P.; Abdul-Wahab, A.; August, S.; Azad, J.; Becher, G.; et al. Anakinra for Palmoplantar Pustulosis: Results from a Randomized, Double-blind, Multicentre, Two-staged, Adaptive Placebo-controlled Trial (APRICOT)*. Br. J. Dermatol. 2022, 186, 245–256. [Google Scholar] [CrossRef]
- Hüffmeier, U.; Wätzold, M.; Mohr, J.; Schön, M.P.; Mössner, R. Successful Therapy with Anakinra in a Patient with Generalized Pustular Psoriasis Carrying IL36RN Mutations. Br. J. Dermatol. 2014, 170, 202–204. [Google Scholar] [CrossRef] [PubMed]
- Bindoli, S.; Giollo, A.; Galozzi, P.; Doria, A.; Sfriso, P. Hyperinflammation after Anti-SARS-CoV-2 MRNA/DNA Vaccines Successfully Treated with Anakinra: Case Series and Literature Review. Exp. Biol. Med. 2022, 247, 338–344. [Google Scholar] [CrossRef] [PubMed]
- Lazaros, G.; Anastassopoulou, C.; Hatziantoniou, S.; Kalos, T.; Soulaidopoulos, S.; Lazarou, E.; Vlachopoulos, C.; Vassilopoulos, D.; Tsakris, A.; Tsioufis, C. A Case Series of Acute Pericarditis Following COVID-19 Vaccination in the Context of Recent Reports from Europe and the United States. Vaccine 2021, 39, 6585–6590. [Google Scholar] [CrossRef] [PubMed]






| Generalized pustular dermatosis | Generalized Pustular Psoriasis Reiter disease (Keratoderma blennorrhagicum) Subcorneal Pustular Dermatosis Generalized neutrophilic pustular eruptions |
| Pustular drug eruption | AGEP Acneiform eruption |
| Localized pustular eruption | Pustulosis palmaris and plantaris Acrodermatitis continua Acne vulgaris Rosacea Perioral dermatitis Folliculitis Localized neutrophilic pustular eruption Eosinophilic folliculitis |
| Study | Disease Type | Sex | Age | Clinical Outcome | Days after Vaccination | Vaccine Type | Dose of Vaccination | Treatment Strategy |
|---|---|---|---|---|---|---|---|---|
| [36] | Palmoplantar pustulosis (Flare) | M | 57 | NM | One month | Pfizer | NM | Oral acitetrin |
| [36] | Palmoplantar pustulosis (Flare) | F | 63 | NM | One month | Pfizer | NM | Oral acitetrin |
| [35] | Palmoplantar pustulosis (Flare) | M | 60 | Multiple pustules on the palms and soles | One week | Pfizer | Both first and second dose | Topical steroid application for two weeks |
| [37] | Rosacea (New-onset) | F | 60 | Erythema, telangiectasias and papulo-pustular eruption | 4 days | Modena | First dose | Sun protection |
| [37] | Rosacea (NM onset) | F | 47 | Erythema, and papulo-pustular eruption | 5 days | Pfizer | Second dose | Sun protection |
| [38] | Facial pustular neutrophilic eruption (New-onset) | M | 50 | Pustules and crust | 4 days | Moderna | First dose | Antibiotic treatment and cortisol cream |
| [38] | Facial pustular neutrophilic eruption (New-onset) | M | 80 | Pustules, crust and erythema | 5 days | Moderna | Second dose | Antibiotic treatment and calcineurin inhibitor cream |
| [8] | Eosinophilic pustular folliculitis (New-onset) | F | 38 | Pustules and mainly papules | 2 days | Pfizer | First and Second dose | Topical corticosteroids |
| [39] | Acute localized pustulosis | F | 43 | Plaques and pustules | 2 days | AstraZeneca | First | Topical treatment and oral prednisolone |
| Study | Disease | Sex | Age | Clinical Outcome | Days after Vaccination | Vaccine | Dose of Vaccination | Treatment Strategy |
|---|---|---|---|---|---|---|---|---|
| [31] | Sneddon–Wilkinson | M | 21 | Vesiculopustular eruption and crust | 4 days | Moderna | First dose | Antibiotic treatment and cortisol cream |
| [32] | Sweet-syndrome (pustular eruption) | M | 77 | Pustular eruption, encephalitis, myoclonus | 5 days | Moderna | Second dose | Antibiotic treatment and calcineurin inhibitor cream |
| [33] | Neutrophilic pustular eruption | M | 32 | Erythematous papulonodules and pustules and aphthous stomatitis with painful genital erosions | 5 days | ChAdOx1 | First dose | Dapsone and antibiotic treatment |
| [38] | Facial pustular neutrophilic eruption (new-onset) | M | 80 | Pustules, crust and erythema | 5 days | Moderna | Second dose | Antibiotic treatment and calcineurin inhibitor cream |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Karampinis, E.; Gravani, A.; Gidarokosta, P.; Bogdanos, D.P.; Roussaki-Schulze, A.-V.; Zafiriou, E. Pustular Eruption following COVID-19 Vaccination: A Narrative Case-Based Review. Vaccines 2023, 11, 1298. https://doi.org/10.3390/vaccines11081298
Karampinis E, Gravani A, Gidarokosta P, Bogdanos DP, Roussaki-Schulze A-V, Zafiriou E. Pustular Eruption following COVID-19 Vaccination: A Narrative Case-Based Review. Vaccines. 2023; 11(8):1298. https://doi.org/10.3390/vaccines11081298
Chicago/Turabian StyleKarampinis, Emmanouil, Agoritsa Gravani, Polyxeni Gidarokosta, Dimitrios Petros Bogdanos, Angeliki-Viktoria Roussaki-Schulze, and Efterpi Zafiriou. 2023. "Pustular Eruption following COVID-19 Vaccination: A Narrative Case-Based Review" Vaccines 11, no. 8: 1298. https://doi.org/10.3390/vaccines11081298