
Safety and Immunogenicity of the Monovalent Omicron XBB.1.5-Adapted BNT162b2 COVID-19 Vaccine in Individuals ≥12 Years Old: A Phase 2/3 Trial
 ,
on behalf of the C4591054 Study Groupadd
Show full author list
,
on behalf of the C4591054 Study Groupadd
Show full author list
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Participants
2.2. Objectives, Endpoints, and Assessments
2.3. Statistical Analysis
3. Results
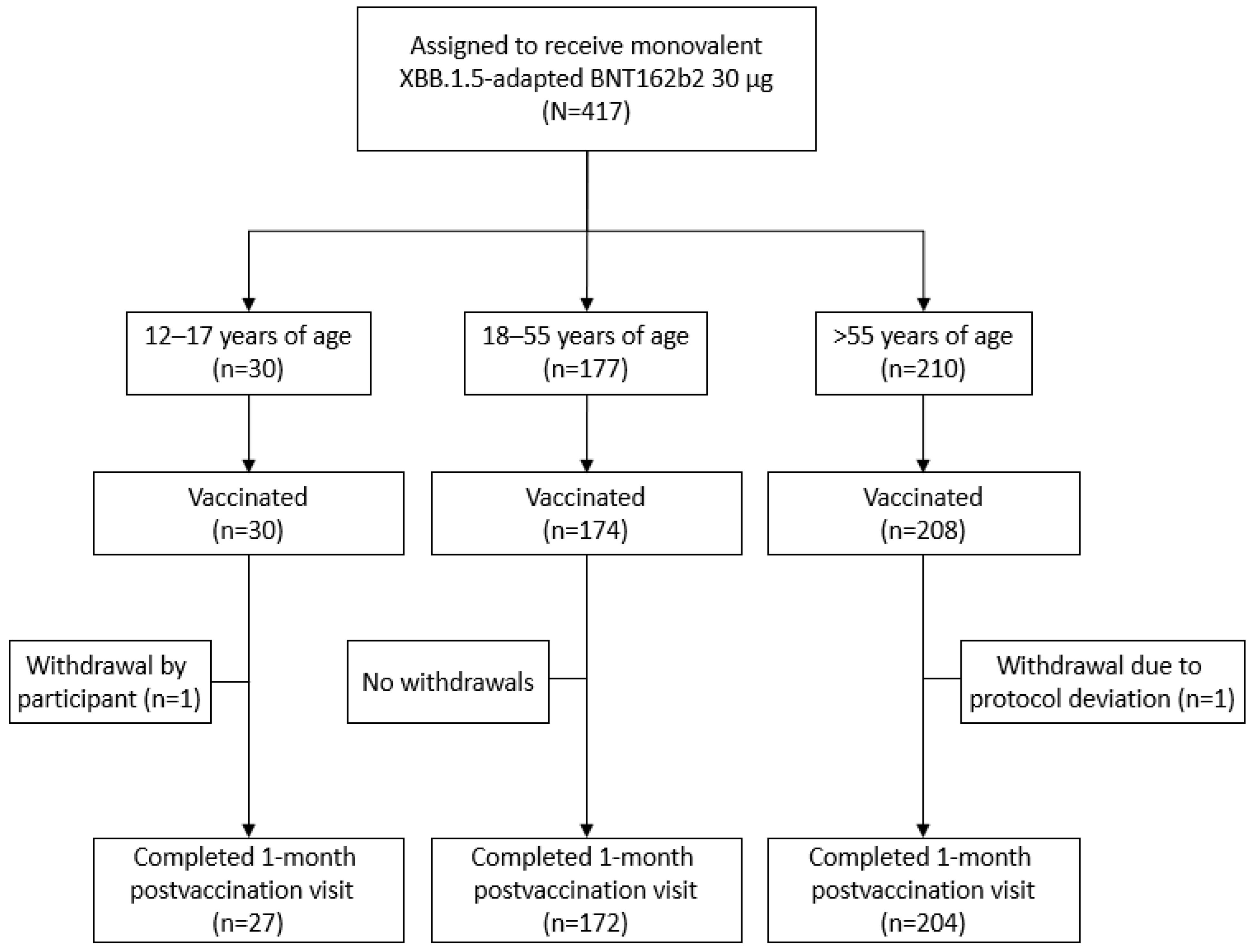
3.1. Participants
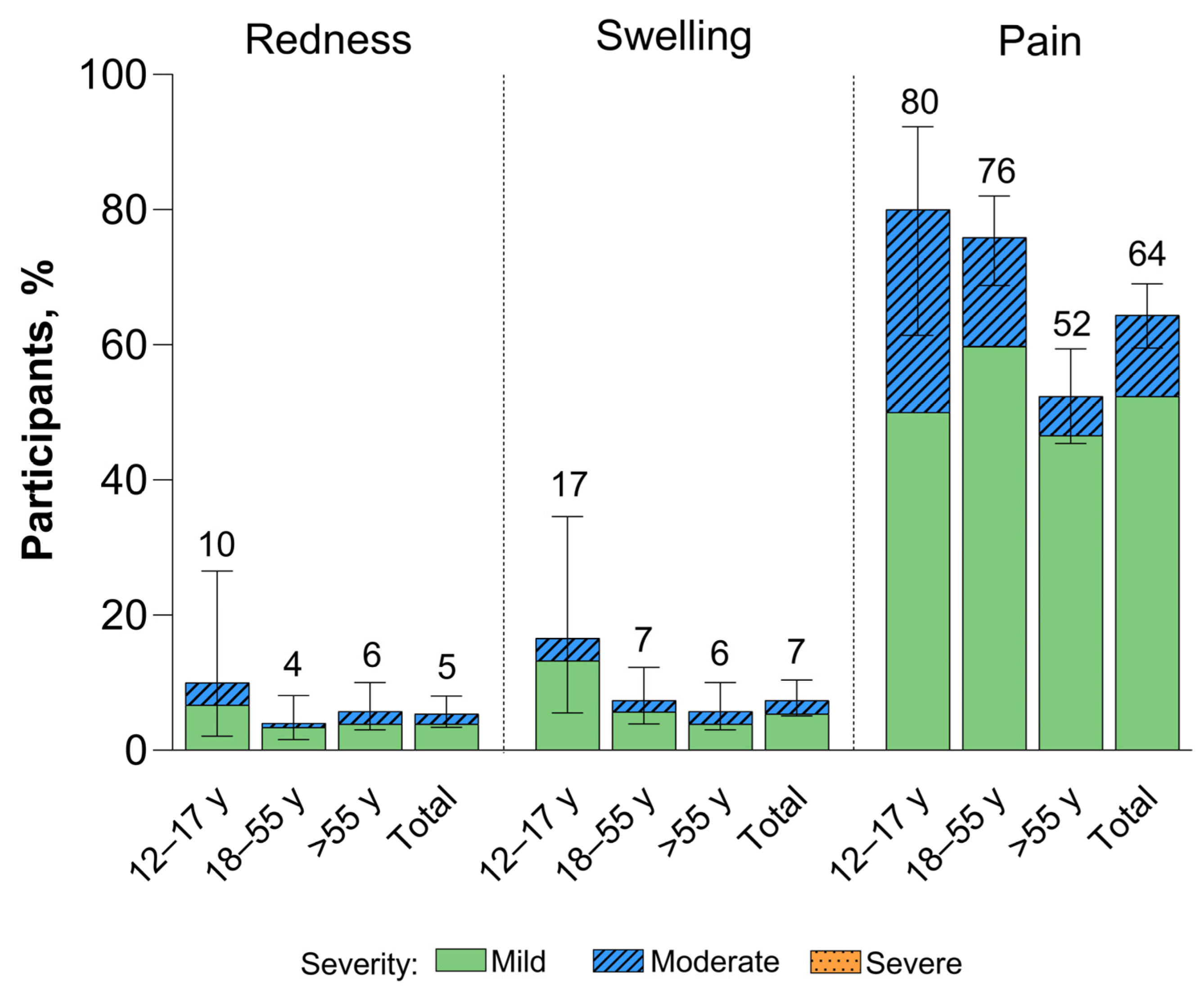
3.2. Safety
3.3. Immunogenicity
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Velavan, T.P.; Ntoumi, F.; Kremsner, P.G.; Lee, S.S.; Meyer, C.G. Emergence and geographic dominance of Omicron subvariants XBB/XBB.1.5 and BF.7—The public health challenges. Int. J. Infect. Dis. 2023, 128, 307–309. [Google Scholar] [CrossRef] [PubMed]
- Carabelli, A.M.; Peacock, T.P.; Thorne, L.G.; Harvey, W.T.; Hughes, J.; Peacock, S.J.; Barclay, W.S.; de Silva, T.I.; Towers, G.J.; Robertson, D.L. SARS-CoV-2 variant biology: Immune escape, transmission and fitness. Nat. Rev. Microbiol. 2023, 21, 162–177. [Google Scholar] [CrossRef] [PubMed]
- Chakraborty, C.; Bhattacharya, M.; Chopra, H.; Islam, M.A.; Saikumar, G.; Dhama, K. The SARS-CoV-2 Omicron recombinant subvariants XBB, XBB.1, and XBB.1.5 are expanding rapidly with unique mutations, antibody evasion, and immune escape properties—An alarming global threat of a surge in COVID-19 cases again? Int. J. Surg. 2023, 109, 1041–1043. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. XBB.1.5 Updated Risk Assessment, 20 June 2023. Available online: https://www.who.int/docs/default-source/coronaviruse/20230620xbb.1.5.pdf?sfvrsn=fff6f686_3 (accessed on 19 November 2023).
- Lassaunière, R.; Polacek, C.; Utko, M.; Sørensen, K.M.; Baig, S.; Ellegaard, K.; Escobar-Herrera, L.A.; Fomsgaard, A.; Spiess, K.; Gunalan, V.; et al. Virus isolation and neutralisation of SARS-CoV-2 variants BA.2.86 and EG.5.1. Lancet Infect. Dis. 2023, 23, e509–e510. [Google Scholar] [CrossRef] [PubMed]
- GISAID. Tracking of hCoV-19 Variants. Available online: https://gisaid.org/hcov19-variants/ (accessed on 24 November 2023).
- Yang, S.; Yu, Y.; Xu, Y.; Jian, F.; Song, W.; Yisimayi, A.; Wang, P.; Wang, J.; Liu, J.; Yu, L.; et al. Fast evolution of SARS-CoV-2 BA.2.86 to JN.1 under heavy immune pressure. bioRxiv 2023. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Vulnerable? Vaccinate. Protecting the Unprotected from COVID-19 and Influenza. Available online: https://www.who.int/europe/news/item/09-10-2023-vulnerable--vaccinate.-protecting-the-unprotected-from-covid-19-and-influenza (accessed on 10 November 2023).
- Pather, S.; Muik, A.; Rizzi, R.; Mensa, F. Clinical development of variant-adapted BNT162b2 COVID-19 vaccines: The early Omicron era. Expert Rev. Vaccines 2023, 22, 650–661. [Google Scholar] [CrossRef]
- COVID-19 Vaccine Tracker. Pfizer/BioNTech: Comirnaty. Available online: https://covid19.trackvaccines.org/vaccines/6/ (accessed on 10 November 2023).
- US Food and Drug Administration. Fact Sheet for Healthcare Providers Administering Vaccine: Emergency Use Authorization of Pfizer-BioNTech COVID-19 Vaccine (2023–2024 Formula), for 6 Months through 11 Years of Age. Available online: https://www.fda.gov/media/167211/download (accessed on 14 November 2023).
- COMIRNATY® (COVID-19 Vaccine mRNA) Highlights of Prescribing Information; Pfizer Inc.: New York, NY, USA, 2023.
- Liu, Y.; Liu, J.; Xia, H.; Zhang, X.; Zou, J.; Fontes-Garfias, C.R.; Weaver, S.C.; Swanson, K.A.; Cai, H.; Sarkar, R.; et al. BNT162b2-elicited neutralization against new SARS-CoV-2 spike variants. N. Engl. J. Med. 2021, 385, 472–474. [Google Scholar] [CrossRef]
- Singer, S.R.; Angulo, F.J.; Swerdlow, D.L.; McLaughlin, J.M.; Hazan, I.; Ginish, N.; Anis, E.; Mendelson, E.; Mor, O.; Zuckerman, N.S.; et al. Effectiveness of BNT162b2 mRNA COVID-19 vaccine against SARS-CoV-2 variant Beta (B.1.351) among persons identified through contact tracing in Israel: A prospective cohort study. EClinicalMedicine 2021, 42, 101190. [Google Scholar] [CrossRef]
- Bernal, J.L.; Andrews, N.; Gower, C.; Gallagher, E.; Simmons, R.; Thelwall, S.; Stowe, J.; Tessier, E.; Groves, N.; Dabrera, G.; et al. Effectiveness of COVID-19 vaccines against the B.1.617.2 (Delta) variant. N. Engl. J. Med. 2021, 385, 585–594. [Google Scholar] [CrossRef]
- Barda, N.; Dagan, N.; Cohen, C.; Hernan, M.A.; Lipsitch, M.; Kohane, I.S.; Reis, B.Y.; Balicer, R.D. Effectiveness of a third dose of the BNT162b2 mRNA COVID-19 vaccine for preventing severe outcomes in Israel: An observational study. Lancet 2021, 398, 2093–2100. [Google Scholar] [CrossRef]
- Collie, S.; Nayager, J.; Bamford, L.; Bekker, L.G.; Zylstra, M.; Gray, G. Effectiveness and durability of the BNT162b2 vaccine against Omicron sublineages in South Africa. N. Engl. J. Med. 2022, 387, 1332–1333. [Google Scholar] [CrossRef]
- Bar-On, Y.M.; Goldberg, Y.; Mandel, M.; Bodenheimer, O.; Amir, O.; Freedman, L.; Alroy-Preis, S.; Ash, N.; Huppert, A.; Milo, R. Protection by a fourth dose of BNT162b2 against Omicron in Israel. N. Engl. J. Med. 2022, 386, 1712–1720. [Google Scholar] [CrossRef]
- US Food and Drug Administration. Coronavirus (COVID-19) Update: FDA Authorizes Moderna and Pfizer-BioNTech Bivalent COVID-19 Vaccines for Use as a Booster Dose in Younger Age Groups. Available online: https://www.fda.gov/news-events/press-announcements/coronavirus-covid-19-update-fda-authorizes-moderna-and-pfizer-biontech-bivalent-covid-19-vaccines (accessed on 5 December 2022).
- Link-Gelles, R.; Ciesla, A.A.; Roper, L.E.; Scobie, H.M.; Ali, A.R.; Miller, J.D.; Wiegand, R.E.; Accorsi, E.K.; Verani, J.R.; Shang, N.; et al. Early estimates of bivalent mRNA booster dose vaccine effectiveness in preventing symptomatic SARS-CoV-2 infection attributable to Omicron BA.5- and XBB/XBB.1.5-related sublineages among immunocompetent adults: Increasing community access to testing program, United States, December 2022–January 2023. MMWR Morb. Mortal. Wkly. Rep. 2023, 72, 119–124. [Google Scholar] [PubMed]
- Tenforde, M.W.; Weber, Z.A.; Natarajan, K.; Klein, N.P.; Kharbanda, A.B.; Stenehjem, E.; Embi, P.J.; Reese, S.E.; Naleway, A.L.; Grannis, S.J.; et al. Early estimates of bivalent mRNA vaccine effectiveness in preventing COVID-19-associated emergency department or urgent care encounters and hospitalizations among immunocompetent adults—VISION Network, nine states, September–November 2022. MMWR Morb. Mortal. Wkly. Rep. 2023, 71, 1637–1646. [Google Scholar] [CrossRef] [PubMed]
- Lin, D.Y.; Xu, Y.; Gu, Y.; Zeng, D.; Wheeler, B.; Young, H.; Sunny, S.K.; Moore, Z. Effectiveness of bivalent boosters against severe Omicron infection. N. Engl. J. Med. 2023, 388, 764–766. [Google Scholar] [CrossRef]
- Poukka, E.; Nohynek, H.; Goebeler, S.; Leino, T.; Baum, U. Bivalent booster effectiveness against severe COVID-19 outcomes in Finland, September 2022–March 2023. medRxiv 2023. [Google Scholar] [CrossRef]
- Link-Gelles, R. COVID-19 Vaccine Effectiveness Updates, 19 April 2023. Available online: https://www.cdc.gov/vaccines/acip/meetings/downloads/slides-2023-04-19/05-COVID-Link-Gelles-508.pdf (accessed on 19 June 2023).
- US Food and Drug Administration. FDA Briefing Document: Vaccines and Related Biological Products Advisory Committee Meeting, 15 June 2023. Available online: https://www.fda.gov/media/169378/download (accessed on 19 July 2023).
- World Health Organization. Statement on the Antigen Composition of COVID-19 Vaccines. Available online: https://www.who.int/news/item/18-05-2023-statement-on-the-antigen-composition-of-covid-19-vaccines (accessed on 19 June 2023).
- US Food and Drug Administration. FDA Takes Action on Updated mRNA COVID-19 Vaccines to Better Protect against Currently Circulating Variants. Available online: https://www.fda.gov/news-events/press-announcements/fda-takes-action-updated-mrna-covid-19-vaccines-better-protect-against-currently-circulating (accessed on 9 November 2023).
- Polack, F.P.; Thomas, S.J.; Kitchin, N.; Absalon, J.; Gurtman, A.; Lockhart, S.; Perez, J.L.; Perez Marc, G.; Moreira, E.D.; Zerbini, C.; et al. Safety and efficacy of the BNT162b2 mRNA Covid-19 vaccine. N. Engl. J. Med. 2020, 383, 2603–2615. [Google Scholar] [CrossRef]
- Winokur, P.; Gayed, J.; Fitz-Patrick, D.; Thomas, S.J.; Diya, O.; Lockhart, S.; Xu, X.; Zhang, Y.; Bangad, V.; Schwartz, H.I.; et al. Bivalent Omicron BA.1-adapted BNT162b2 booster in adults older than 55 years. N. Engl. J. Med. 2023, 388, 214–227. [Google Scholar] [CrossRef]
- Hause, A.M.; Baggs, J.; Marquez, P.; Myers, T.R.; Su, J.R.; Blanc, P.G.; Gwira Baumblatt, J.A.; Woo, E.J.; Gee, J.; Shimabukuro, T.T.; et al. Safety monitoring of COVID-19 vaccine booster doses among adults—United States, September 22, 2021–February 6, 2022. MMWR Morb. Mortal. Wkly. Rep. 2022, 71, 249–254. [Google Scholar] [CrossRef]
- Hause, A.M.; Baggs, J.; Marquez, P.; Abara, W.E.; Baumblatt, J.; Blanc, P.G.; Su, J.R.; Hugueley, B.; Parker, C.; Myers, T.R.; et al. Safety monitoring of COVID-19 mRNA vaccine second booster doses among adults aged ≥50 years—United States, 29 March 2022–10 July 2022. MMWR Morb. Mortal. Wkly. Rep. 2022, 71, 971–976. [Google Scholar] [CrossRef]
- Uriu, K.; Ito, J.; Zahradnik, J.; Fujita, S.; Kosugi, Y.; Schreiber, G.; Sato, K. Enhanced transmissibility, infectivity, and immune resistance of the SARS-CoV-2 omicron XBB.1.5 variant. Lancet Infect. Dis. 2023, 23, 280–281. [Google Scholar] [CrossRef] [PubMed]
- Qu, P.; Xu, K.; Faraone, J.N.; Goodarzi, N.; Zheng, Y.-M.; Carlin, C.; Bednash, J.S.; Horowitz, J.C.; Mallampalli, R.K.; Saif, L.J.; et al. Immune evasion, infectivity, and fusogenicity of SARS-CoV-2 Omicron BA.2.86 and FLip variants. bioRxiv 2023. [Google Scholar] [CrossRef]
- Parums, D.V. Editorial: A rapid global increase in COVID-19 is due to the emergence of the EG.5 (Eris) subvariant of Omicron SARS-CoV-2. Med. Sci. Monit. 2023, 29, e942244. [Google Scholar] [CrossRef] [PubMed]
- Wang, Q.; Guo, Y.; Liu, L.; Schwanz, L.T.; Li, Z.; Nair, M.S.; Ho, J.; Zhang, R.M.; Iketani, S.; Yu, J.; et al. Antigenicity and receptor affinity of SARS-CoV-2 BA.2.86 spike. Nature 2023, 624, 639–644. [Google Scholar] [CrossRef] [PubMed]
- Attar Cohen, H.; Mesfin, S.; Ikejezie, J.; Kassamali, Z.; Campbell, F.; Adele, S.; Guinko, N.; Idoko, F.; Mirembe, B.B.; Mitri, M.E.; et al. Surveillance for variants of SARS-CoV-2 to inform risk assessments. Bull. World Health Organ. 2023, 101, 707–716. [Google Scholar] [CrossRef] [PubMed]
- Jones, J.M.; Manrique, I.M.; Stone, M.S.; Grebe, E.; Saa, P.; Germanio, C.D.; Spencer, B.R.; Notari, E.; Bravo, M.; Lanteri, M.C.; et al. Estimates of SARS-CoV-2 seroprevalence and incidence of primary SARS-CoV-2 infections among blood donors, by COVID-19 vaccination status—United States, April 2021–September 2022. MMWR Morb. Mortal. Wkly. Rep. 2023, 72, 601–605. [Google Scholar] [CrossRef]
- Modjarrad, K.; Che, Y.; Chen, W.; Wu, H.; Cadima, C.I.; Muik, A.; Maddur, M.S.; Tompkins, K.R.; Martinez, L.T.; Cai, H.; et al. Preclinical characterization of the Omicron XBB.1.5-adapted BNT162b2 COVID-19 vaccine. bioRxiv 2023. [Google Scholar] [CrossRef]
- Muñoz, F.M.; Sher, L.D.; Sabharwal, C.; Gurtman, A.; Xu, X.; Kitchin, N.; Lockhart, S.; Riesenberg, R.; Sexter, J.M.; Czajka, H.; et al. Evaluation of BNT162b2 COVID-19 vaccine in children younger than 5 years of age. N. Engl. J. Med. 2023, 388, 621–634. [Google Scholar] [CrossRef]
- US Food and Drug Administration, Emergency Use Authorization (EUA) Amendment for an Unapproved Product Review Memorandum (Application EUA27034, Amendment 719). 28 February 2023. Available online: https://www.fda.gov/media/166240/download (accessed on 22 January 2024).







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristic | 12–17 Years Old (N a = 30) | 18–55 Years Old (N a = 174) | >55 Years Old (N a = 208) | Total (N a = 412) |
|---|---|---|---|---|
| Sex, n b (%) | ||||
| Male | 11 (36.7) | 74 (42.5) | 85 (40.9) | 170 (41.3) |
| Female | 19 (63.3) | 100 (57.5) | 123 (59.1) | 242 (58.7) |
| Race, n b (%) | ||||
| White | 26 (86.7) | 135 (77.6) | 165 (79.3) | 326 (79.1) |
| Black | 3 (10.0) | 23 (13.2) | 26 (12.5) | 52 (12.6) |
| American Indian or Alaska Native | 0 | 0 | 1 (0.5) | 1 (0.2) |
| Asian | 1 (3.3) | 11 (6.3) | 10 (4.8) | 22 (5.3) |
| Native Hawaiian or other Pacific Islander | 0 | 0 | 2 (1.0) | 2 (0.5) |
| Multiracial or unknown | 0 | 5 (2.9) | 4 (1.9) | 9 (2.1) |
| Ethnicity, n b (%) | ||||
| Hispanic/Latino | 6 (20.0) | 35 (20.1) | 34 (16.3) | 75 (18.2) |
| Age at vaccination, years | ||||
| Mean (SD) | 14.0 (1.74) | 40.4 (9.82) | 68.6 (6.74) | 52.7 (19.12) |
| Median (range) | 14.0 (12–17) | 42.0 (18–55) | 68.5 (56–88) | 56.0 (12–88) |
| Baseline SARS-CoV-2 status, n b (%) | ||||
| Positive c | 23 (76.7) | 144 (82.8) | 155 (74.5) | 322 (78.2) |
| Negative d | 7 (23.3) | 30 (17.2) | 53 (25.5) | 90 (21.8) |
| Prior COVID-19 vaccine doses, e n b (%) | ||||
| 3 doses | 30 (100.0) | 174 (100.0) | 208 (100.0) | 412 (100.0) |
| 4 doses | 26 (86.7) | 154 (88.5) | 199 (95.7) | 379 (92.0) |
| 5 doses | 1 (3.3) | 19 (10.9) | 104 (50.0) | 124 (30.1) |
| 6 doses | 0 | 1 (0.6) | 4 (1.9) | 5 (1.2) |
| 7 doses | 0 | 0 | 1 (0.5) | 1 (0.2) |
| Time from last dose of mRNA COVID-19 vaccine e to the study vaccination, months f | ||||
| Mean (SD) | 10.2 (1.95) | 10.4 (2.33) | 10.4 (1.82) | 10.4 (2.05) |
| Median (range) | 10.3 (6.7–12.6) | 10.9 (5.5–24.1) | 10.8 (5.8–22.6) | 10.8 (5.5–24.1) |
| 5 to <7, n b (%) | 1 (3.3) | 12 (6.9) | 11 (5.3) | 24 (5.8) |
| 7 to <9, n b (%) | 8 (26.7) | 31 (17.8) | 31 (14.9) | 70 (17.0) |
| 9 to 12, n b (%) | 10 (33.3) | 108 (62.1) | 155 (74.5) | 273 (66.3) |
| >12, n b (%) | 11 (36.7) | 23 (13.2) | 11 (5.3) | 45 (10.9) |
| Time from last dose of mRNA COVID-19 vaccine e to the study vaccination, days | ||||
| Mean (SD) | 286.4 (54.50) | 292.1 (65.24) | 290.2 (50.95) | 290.8 (57.54) |
| Median (range) | 289.0 (188–352) | 305.0 (154–675) | 303.0 (162–634) | 303.0 (154–675) |
| BMI, ≥16 years of age, n b (%) | ||||
| Number of participants g | 5 | 174 | 208 | 387 |
| Underweight (<18.5 kg/m2) | 0 | 4 (2.3) | 2 (1.0) | 6 (1.6) |
| Normal weight (≥18.5–24.9 kg/m2) | 4 (80.0) | 52 (29.9) | 53 (25.5) | 109 (28.2) |
| Overweight (≥25.0–29.9 kg/m2) | 0 | 56 (32.2) | 78 (37.5) | 134 (34.6) |
| Obese (≥30.0 kg/m2) | 1 (20.0) | 62 (35.6) | 75 (36.1) | 138 (35.7) |
| BMI, 12–15 years of age/obese, h n b (%) | ||||
| Number of participants g | 25 | - | - | 25 |
| Not obese | 22 (88.0) | - | - | 22 (88.0) |
| Obese | 3 (12.0) | - | - | 3 (12.0) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gayed, J.; Diya, O.; Lowry, F.S.; Xu, X.; Bangad, V.; Mensa, F.; Zou, J.; Xie, X.; Hu, Y.; Lu, C.; et al. Safety and Immunogenicity of the Monovalent Omicron XBB.1.5-Adapted BNT162b2 COVID-19 Vaccine in Individuals ≥12 Years Old: A Phase 2/3 Trial. Vaccines 2024, 12, 118. https://doi.org/10.3390/vaccines12020118
Gayed J, Diya O, Lowry FS, Xu X, Bangad V, Mensa F, Zou J, Xie X, Hu Y, Lu C, et al. Safety and Immunogenicity of the Monovalent Omicron XBB.1.5-Adapted BNT162b2 COVID-19 Vaccine in Individuals ≥12 Years Old: A Phase 2/3 Trial. Vaccines. 2024; 12(2):118. https://doi.org/10.3390/vaccines12020118
Chicago/Turabian StyleGayed, Juleen, Oyeniyi Diya, Francine S. Lowry, Xia Xu, Vishva Bangad, Federico Mensa, Jing Zou, Xuping Xie, Yanping Hu, Claire Lu, and et al. 2024. "Safety and Immunogenicity of the Monovalent Omicron XBB.1.5-Adapted BNT162b2 COVID-19 Vaccine in Individuals ≥12 Years Old: A Phase 2/3 Trial" Vaccines 12, no. 2: 118. https://doi.org/10.3390/vaccines12020118