
PEACE: Perception and Expectations toward Artificial Intelligence in Capsule Endoscopy

 , , , , ,
, , , , ,  ,
, {kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Materials and Methods
2.1. Agreement to Statements
2.2. Statistical Analysis
3. Results
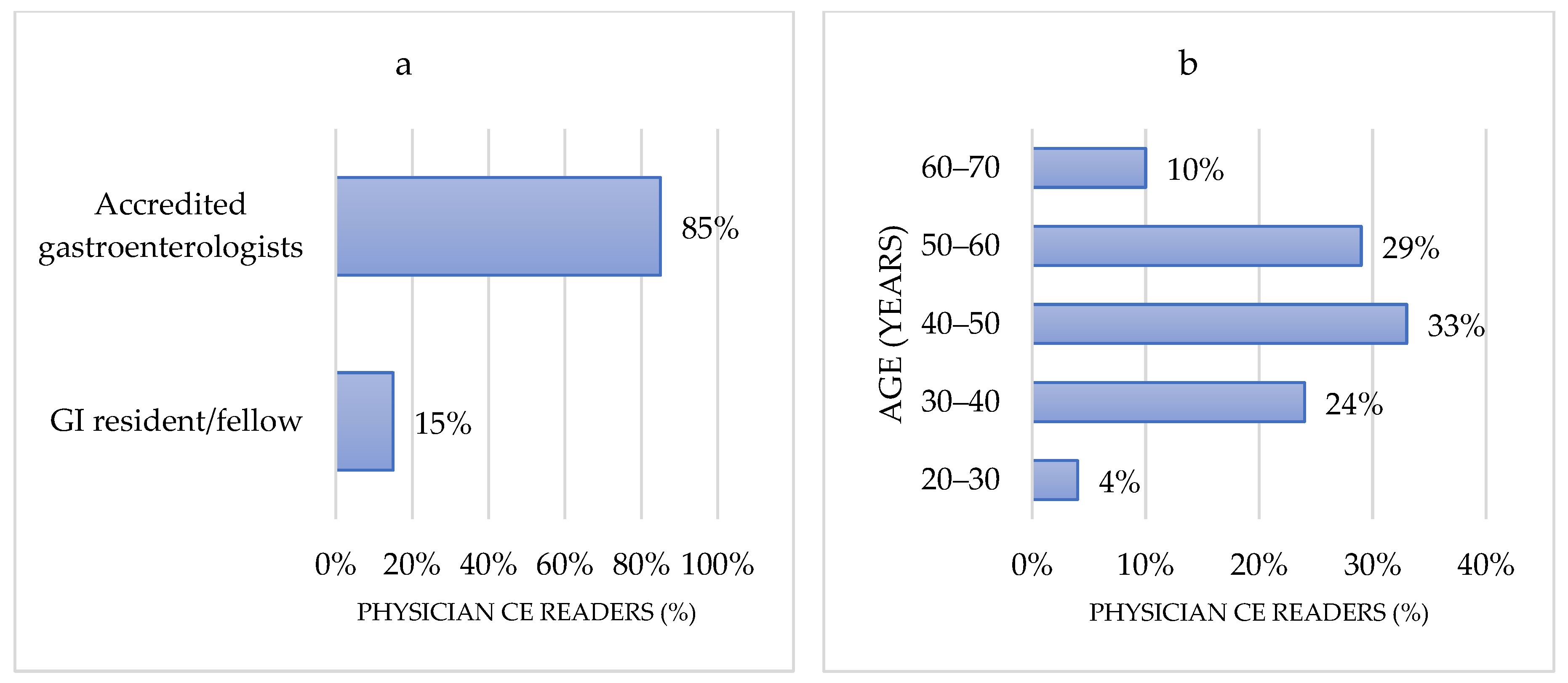
3.1. Physicians’ Characteristics
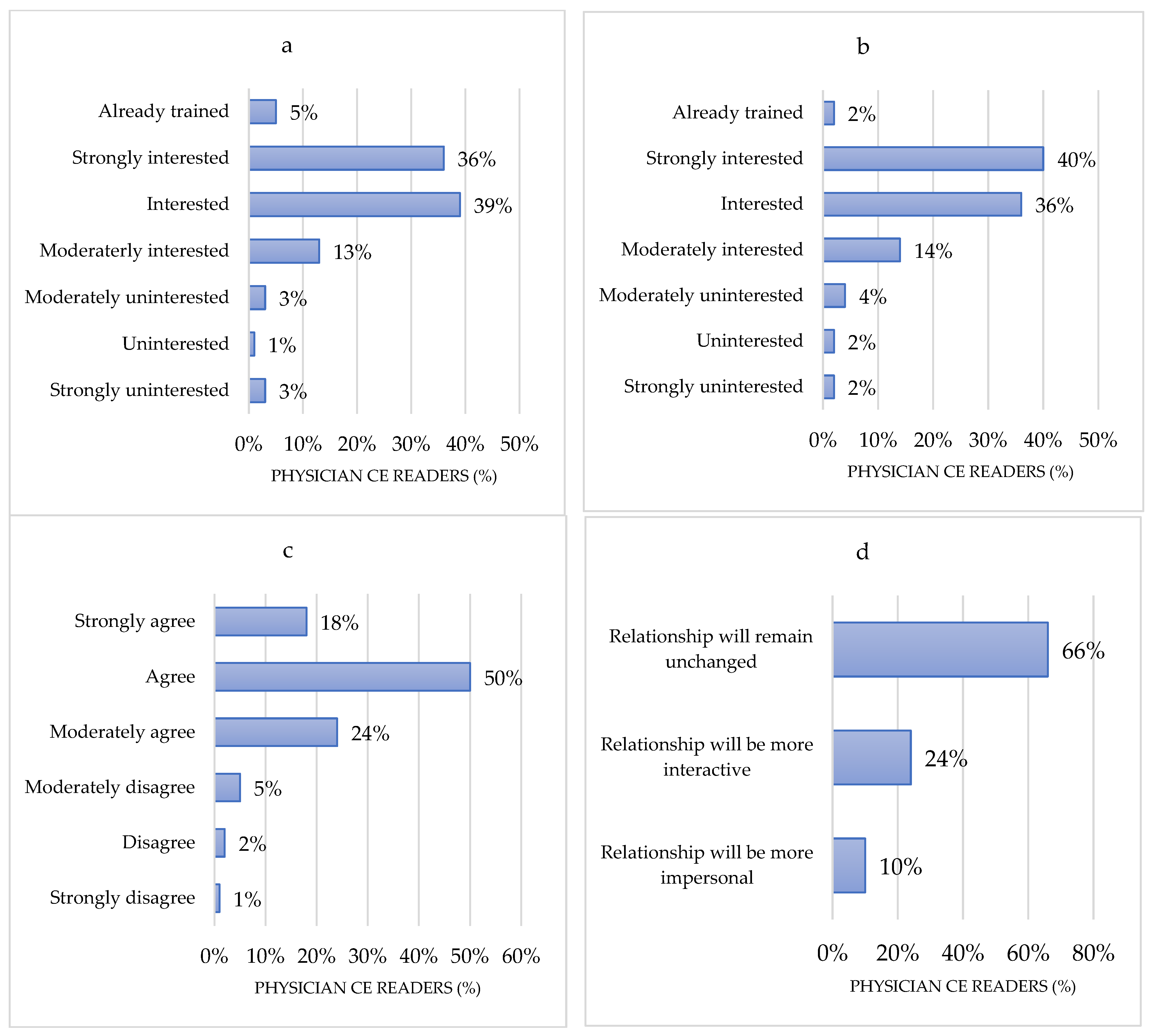
3.2. Level of Information on AI
3.3. Perceptions of AI toward Capsule Endoscopy
3.4. Perceptions Regarding the Barriers for AI Implementation
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Appendix A
- Are you a capsule endoscopy reader?
- Your age?
- Your country (where you practice)?
- Your professional level?
- What is your main practice setting?
- Years of CE reading experience?
- Current average number of CE read by yourself per year.
- Are you already using any AI applications (e.g., speech recognition, spam filters, recommendation algorithms, etc.) in your everyday life?
- Do you use any endoscopy AI solution in your regular practice already?
- AI will revolutionize endoscopy.
- How interested are you in receiving a generic/baseline training on AI?
- How interested are you in receiving technically advanced training on AI?
- How will the relationship between the endoscopist and the patient change with the introduction of AI?
- AI should be part of endoscopy training.
- Are you already using quick CE reading modes?
- What will be the role(s) of endoscopists in developing/validating AI applications into CE practice?
- What MEAN reading time should AI-based applications provide before implementation in small bowel CE practice is considered? (Minutes)
- AI will have a positive impact on CE.
- AI will increase the diagnostic yield in CE.
- AI will allow automated reporting of CE without validation by the gastroenterologist.
- AI will shorten the reading time in CE.
- AI will help characterizing lesions seen in CE.
- AI will help standardizing reporting in CE.
- Patients should be aware about the use of AI in CE reading.
- Patients should specifically consent to the use of AI in CE reading?
- Cost is important in implementing AI in CE reading.
- A normal small bowel CE encompasses a mean number of 12,500 frames. What maximal number of AI false positive frames would you accept to review?
- What should be a reasonable time limit to get the results from an AI-based CE reading?
- AI in CE will lead to operator dependence on the technology.
- AI will increase the number of requests for CE examinations.
- In the foreseeable future, all capsule readers will be replaced by AI.
- Who should take the responsibility of AI-based reporting in CE?
References
- Rajkomar, A.; Dean, J.; Kohane, I. Machine Learning in Medicine. N. Engl. J. Med. 2019, 380, 1347–1358. [Google Scholar] [CrossRef] [PubMed]
- Schmitz, R.; Werner, R.; Repici, A.; Bisschops, R.; Meining, A.; Zornow, M.; Messmann, H.; Hassan, C.; Sharma, P.; Rösch, T. Artificial intelligence in GI endoscopy: Stumbling blocks, gold standards and the role of endoscopy societies. Gut 2021. [Google Scholar] [CrossRef] [PubMed]
- Wang, P.; Berzin, T.M.; Glissen Brown, J.R.; Bharadwaj, S.; Becq, A.; Xiao, X.; Liu, P.; Li, L.; Song, Y.; Zhang, D.; et al. Real-time automatic detection system increases colonoscopic polyp and adenoma detection rates: A prospective randomised controlled study. Gut 2019, 68, 1813–1819. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ding, Z.; Shi, H.; Zhang, H.; Meng, L.; Fan, M.; Han, C.; Zhang, K.; Ming, F.; Xie, X.; Liu, H.; et al. Gastroenterologist-Level Identification of Small-Bowel Diseases and Normal Variants by Capsule Endoscopy Using a Deep-Learning Model. Gastroenterology 2019, 157, 1044–1054.e5. [Google Scholar] [CrossRef] [PubMed]
- Repici, A.; Spadaccini, M.; Antonelli, G.; Correale, L.; Maselli, R.; Galtieri, P.A.; Pellegatta, G.; Capogreco, A.; Milluzzo, S.M.; Lollo, G.; et al. Artificial intelligence and colonoscopy experience: Lessons from two randomised trials. Gut 2021. [Google Scholar] [CrossRef] [PubMed]
- Bisschops, R.; East, J.E.; Hassan, C.; Hazewinkel, Y.; Kamiński, M.F.; Neumann, H.; Pellisé, M.; Antonelli, G.; Balen, M.B.; Coron, E.; et al. Advanced imaging for detection and differentiation of colorectal neoplasia: European Society of Gastrointestinal Endoscopy (ESGE) Guideline—Update 2019. Endoscopy 2019, 51, 1155–1179. [Google Scholar] [PubMed] [Green Version]
- Leenhardt, R.; Vasseur, P.; Philippe, M.; Saurin, J.C.; Rahmi, G.; Cholet, F.; Becq, A.; Marteau, P.; Histace, A.; Dray, X.; et al. A neural network algorithm for detection of GI angiectasia during small-bowel capsule endoscopy. Gastrointest. Endosc. 2019, 89, 189–194. [Google Scholar] [CrossRef] [PubMed]
- Aoki, T.; Yamada, A.; Aoyama, K.; Saito, H.; Tsuboi, A.; Nakada, A.; Niikura, R.; Fujishiro, M.; Oka, S.; Ishihara, S.; et al. Automatic detection of erosions and ulcerations in wireless capsule endoscopy images based on a deep convolutional neural network. Gastrointest. Endosc. 2019, 89, 357–363.e2. [Google Scholar] [CrossRef] [PubMed]
- Dray, X.; Iakovidis, D.; Houdeville, C.; Jover, R.; Diamantis, D.; Histace, A.; Koulaouzidis, A. Artificial intelligence in small bowel capsule endoscopy—Current status, challenges and future promise. J. Gastroenterol. Hepatol. 2021, 36, 12–19. [Google Scholar] [CrossRef] [PubMed]
- Wadhwa, V.; Alagappan, M.; Gonzalez, A.; Gupta, K.; Brown, J.R.G.; Cohen, J.; Sawhney, M.; Pleskow, D.; Berzin, T.M. Physician sentiment toward artificial intelligence (AI) in colonoscopic practice: A survey of US gastroenterologists. Endosc. Int. Open 2020, 8, E1379–E1384. [Google Scholar] [CrossRef] [PubMed]
- Waymel, Q.; Badr, S.; Demondion, X.; Cotten, A.; Jacques, T. Impact of the rise of artificial intelligence in radiology: What do radiologists think? Diagn. Interv. Imaging 2019, 100, 327–336. [Google Scholar] [CrossRef] [PubMed]
- Pinto Dos Santos, D.; Giese, D.; Brodehl, S.; Chon, S.H.; Staab, W.; Kleinert, R.; Maintz, D.; Baeßler, B. Medical students’ attitude towards artificial intelligence: A multicentre survey. Eur. Radiol. 2019, 29, 1640–1646. [Google Scholar] [CrossRef] [PubMed]
- ASGE Technology Committee; Wang, A.; Banerjee, S.; Barth, B.A.; Bhat, Y.M.; Chauhan, S.; Gottlieb, K.T.; Konda, V.; Maple, J.T.; Murad, F. Wireless capsule endoscopy. Gastrointest. Endosc. 2013, 78, 805–815. [Google Scholar] [CrossRef] [PubMed]
- Beg, S.; Card, T.; Sidhu, R.; Wronska, E.; Ragunath, K.; Ching, H.-L.; Koulaouzidis, A.; Yung, D.; Panter, S.; Mcalindon, M.; et al. The impact of reader fatigue on the accuracy of capsule endoscopy interpretation. Dig. Liver Dis. 2021, 53, 1028–1033. [Google Scholar] [CrossRef] [PubMed]
- Rondonotti, E.; Spada, C.; Adler, S.; May, A.; Despott, E.J.; Koulaouzidis, A.; Panter, S.; Domagk, D.; Fernandez-Urien, I.; Rahmi, G.; et al. Small-bowel capsule endoscopy and device-assisted enteroscopy for diagnosis and treatment of small-bowel disorders: European Society of Gastrointestinal Endoscopy (ESGE) Technical Review. Endoscopy 2018, 50, 423–446. [Google Scholar] [CrossRef] [Green Version]
- Piccirelli, S.; Milluzzo, S.M.; Bizzotto, A.; Cesaro, P.; Pecere, S.; Spada, C. Small Bowel Capsule Endoscopy and artificial intelligence: First or second reader? Best Pract. Res. Clin. Gastroenterol. 2021, 52–53, 101742. [Google Scholar] [CrossRef] [PubMed]
- Vinsard, D.G.; Mori, Y.; Misawa, M.; Kudo, S.-E.; Rastogi, A.; Bagci, U.; Rex, D.K.; Wallace, M.B. Quality assurance of computer-aided detection and diagnosis in colonoscopy. Gastrointest. Endosc. 2019, 90, 55–63. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ahmad, O.F.; Mori, Y.; Misawa, M.; Kudo, S.-E.; Anderson, J.T.; Bernal, J.; Berzin, T.M.; Bisschops, R.; Byrne, M.F.; Chen, P.-J.; et al. Establishing key research questions for the implementation of artificial intelligence in colonoscopy: A modified Delphi method. Endoscopy 2021, 53, 893–901. [Google Scholar] [CrossRef]
- Cabitza, F.; Zeitoun, J.-D. The proof of the pudding: In praise of a culture of real-world validation for medical artificial intelligence. Ann. Transl. Med. 2019, 7, 161. [Google Scholar] [CrossRef]




Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Leenhardt, R.; Fernandez-Urien Sainz, I.; Rondonotti, E.; Toth, E.; Van de Bruaene, C.; Baltes, P.; Rosa, B.J.; Triantafyllou, K.; Histace, A.; Koulaouzidis, A.; et al. PEACE: Perception and Expectations toward Artificial Intelligence in Capsule Endoscopy. J. Clin. Med. 2021, 10, 5708. https://doi.org/10.3390/jcm10235708
Leenhardt R, Fernandez-Urien Sainz I, Rondonotti E, Toth E, Van de Bruaene C, Baltes P, Rosa BJ, Triantafyllou K, Histace A, Koulaouzidis A, et al. PEACE: Perception and Expectations toward Artificial Intelligence in Capsule Endoscopy. Journal of Clinical Medicine. 2021; 10(23):5708. https://doi.org/10.3390/jcm10235708
Chicago/Turabian StyleLeenhardt, Romain, Ignacio Fernandez-Urien Sainz, Emanuele Rondonotti, Ervin Toth, Cedric Van de Bruaene, Peter Baltes, Bruno Joel Rosa, Konstantinos Triantafyllou, Aymeric Histace, Anastasios Koulaouzidis, and et al. 2021. "PEACE: Perception and Expectations toward Artificial Intelligence in Capsule Endoscopy" Journal of Clinical Medicine 10, no. 23: 5708. https://doi.org/10.3390/jcm10235708