
Pharmacokinetics and Metabolomic Profiling of Metformin and Andrographis paniculata: A Protocol for a Crossover Randomised Controlled Trial

 , ,
, , 
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
Objectives
2. Materials and Methods
2.1. Study Design
2.2. Ethics Committee and Clinical Trial Registry
2.3. Conduct of Study
2.3.1. Trial Site
2.3.2. Inclusion and Exclusion Criteria
2.3.3. Informed Consent and Patient Withdrawal Criteria
2.3.4. Assignment of Intervention, Randomisation, and Blinding
2.3.5. Investigational Products Intervention
2.3.6. Sample Size Calculation
2.3.7. Screening and Data Collection
2.4. Safety Assessment
3. Data Collection, Management, and Statistical Analyses
3.1. Clinical Data
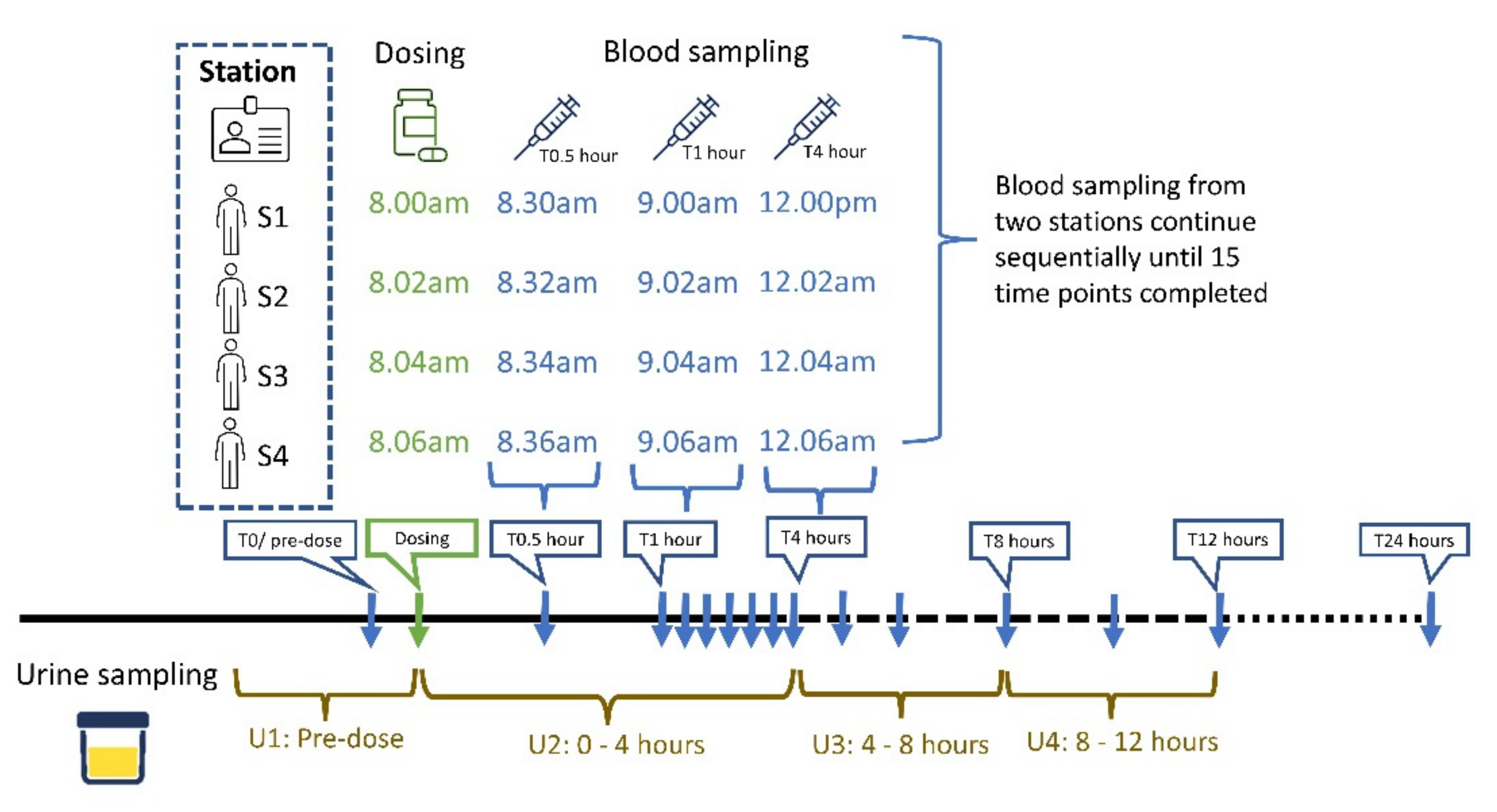
3.2. Pharmacokinetics Analysis
3.3. Untargeted Metabolomics and Multivariate Data Analysis
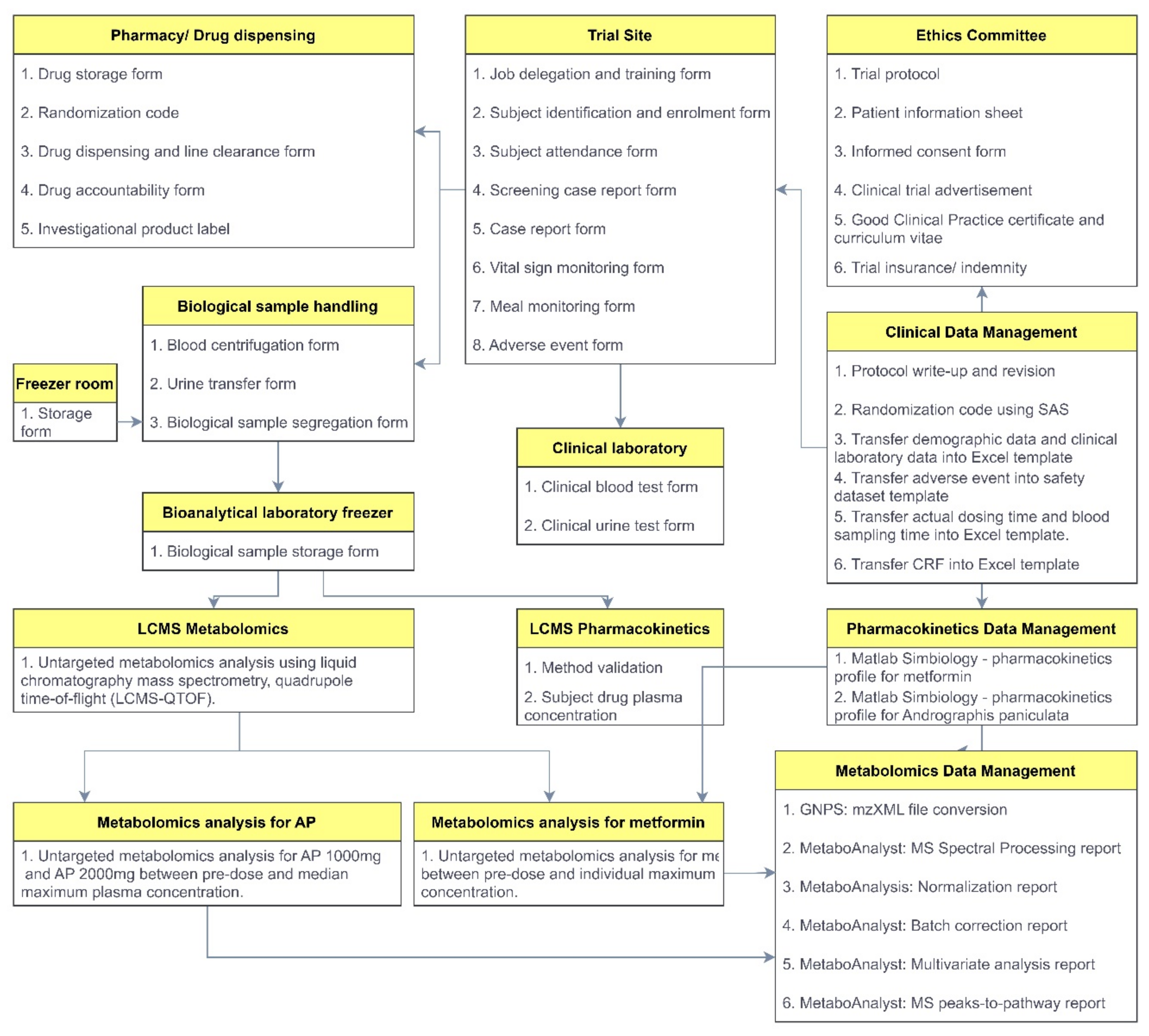
3.4. Reporting Framework
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- International Conference of Harmonization. Guidance on General Consideration for Clinical Trials. Available online: http://www.ich.org/fileadmin/Public_Web_Site/ICH_Products/Guidelines/Efficacy/E8/Step4/E8_Guideline.pdf (accessed on 20 March 2022).
- Burt, T.; Nandal, S. Pharmacometabolomics in Early-Phase Clinical Development. Clin. Transl. Sci. 2016, 9, 128–138. [Google Scholar] [CrossRef] [PubMed]
- Wishart, D.S. Emerging Applications of Metabolomics in Drug Discovery and Precision Medicine. Nat. Rev. Drug Discov. 2016, 15, 473–484. [Google Scholar] [CrossRef]
- van der Greef, J.; Hankemeier, T.; McBurney, R.N. Metabolomics-Based Systems Biology and Personalized Medicine: Moving Towards n = 1 Clinical Trials? Pharmacogenomics 2006, 7, 1087–1094. [Google Scholar] [CrossRef] [Green Version]
- Yang, Z.; Marotta, F. Pharmacometabolomics in Drug Discovery & Development: Applications and Challenges. Metabolomics 2012, 2, e122. [Google Scholar]
- Chan, K. Progress in Traditional Chinese Medicine. Trends Pharmacol. Sci. 1995, 16, 182–187. [Google Scholar] [CrossRef]
- Lan, K.; Jia, W. An integrated metabolomics and pharmacokinetics strategy for multi-component drugs evaluation. Curr. Drug Metab. 2010, 11, 105–114. [Google Scholar] [CrossRef]
- Lan, K.; Xie, G.; Jia, W. Towards Polypharmacokinetics: Pharmacokinetics of Multicomponent Drugs and Herbal Medicines Using a Metabolomics Approach. Evid. Based Complement. Altern. Med. 2013, 2013, 819147. [Google Scholar] [CrossRef] [Green Version]
- Diabetes Prevention Program Research Group. Long-Term Safety, Tolerability, and Weight Loss Associated with Metformin in the Diabetes Prevention Program Outcomes Study. Diabetes Care 2012, 35, 731–737. [Google Scholar] [CrossRef] [Green Version]
- Friedrich, C.; Br, T.; Ring, A.; Meinicke, T. Bioequivalence of Glucophage® (Metformin) Tablets from Europe and the United States Tested in Healthy Volunteers. J. Bioequiv. Bioavailab. 2014, 6, 61–66. [Google Scholar]
- Hossain, S.; Urbi, Z.; Karuniawati, H.; Mohiuddin, R.B.; Moh Qrimida, A.; Allzrag, A.M.M.; Ming, L.C.; Pagano, E.; Capasso, R. Andrographis paniculata (Burm. f.) Wall. ex Nees: An Updated Review of Phytochemistry, Antimicrobial Pharmacology, and Clinical Safety and Efficacy. Life 2021, 11, 348. [Google Scholar] [CrossRef] [PubMed]
- Jayakumar, T.; Hsieh, C.-Y.; Lee, J.-J.; Sheu, J.-R. Experimental and Clinical Pharmacology of Andrographis paniculata and Its Major Bioactive Phytoconstituent Andrographolide. Evid.-Based Complementary Altern. Med. 2013, 2013, 846740. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chao, W.-W.; Lin, B.-F. Isolation and identification of bioactive compounds in Andrographis paniculata (Chuanxinlian). Chin. Med. 2010, 5, 17. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Worakunphanich, W.; Thavorncharoensap, M.; Youngkong, S.; Thadanipon, K.; Thakkinstian, A. Safety of Andrographis paniculata: A Systematic Review and Meta-Analysis. Pharmacoepidemiol. Drug Saf. 2021, 30, 727–739. [Google Scholar] [CrossRef]
- Mkrtchyan, A.; Panosyan, V.; Panossian, A.; Wikman, G.; Wagner, H. A Phase I Clinical Study of Andrographis paniculata Fixed Combination Kan Jang Versus Ginseng and Valerian on the Semen Quality of Healthy Male Subjects. Phytomedicine 2005, 12, 403–409. [Google Scholar] [CrossRef] [PubMed]
- Panossian, A.; Hovhannisyan, A.; Mamikonyan, G.; Abrahamian, H.; Hambardzumyan, E.; Gabrielian, E.; Goukasova, G.; Wikman, G.; Wagner, H. Pharmacokinetic and oral bioavailability of Andrographolide from Andrographis paniculata Fixed Combination Kan Jang in Rats and Human. Phytomedicine 2000, 7, 351–364. [Google Scholar] [CrossRef]
- Calabrese, C.; Berman, S.H.; Babish, J.G.; Ma, X.; Shinto, L.; Dorr, M.; Wells, K.; Wenner, C.A.; Standish, L.J. A Phase I Trial of Andrographolide in HIV Positive Patients and Normal Volunteers. Phytother Res. 2000, 14, 333–338. [Google Scholar] [CrossRef]
- Pholphana, N.; Panomvana, D.; Rangkadilok, N.; Suriyo, T.; Puranajoti, P.; Ungtrakul, T.; Pongpun, W.; Thaeopattha, S.; Songvut, P.; Satayavivad, J. Andrographis paniculata: Dissolution Investigation and Pharmacokinetic Studies of Four Major Active Diterpenoids after Multiple Oral Dose Administration in Healthy Thai Volunteers. J. Ethnopharmacol. 2016, 194, 513–521. [Google Scholar] [CrossRef]
- Agarwal, R.; Sulaiman, S.A.; Mohamed, M. Open Label Clinical Trial to Study Adverse Effects and Tolerance to Dry Powder of the Aerial Part of Andrographis paniculata in Patients Type 2 with Diabetes Mellitus. Malays. J. Med. Sci. 2005, 12, 13–19. [Google Scholar]
- Yan, F.; Thall, P.F.; Lu, K.H.; Gilbert, M.R.; Yuan, Y. Phase I–II Clinical Trial Design: A State-of-the-Art Paradigm for Dose Finding. Ann. Oncol. 2017, 29, 694–699. [Google Scholar] [CrossRef]
- Beger, R.D.; Schmidt, M.A.; Kaddurah-Daouk, R. Current Concepts in Pharmacometabolomics, Biomarker Discovery, and Precision Medicine. Metabolites 2020, 10, 129. [Google Scholar] [CrossRef] [Green Version]
- Gu, Y.L.; Ma, J.Y.; Liu, Y.L.; Chen, B.; Yao, S.Z. Determination of Andrographolide in Human Plasma by High-Performance Liquid Chromatography/Mass Spectrometry. J. Chromatogr. B 2007, 854, 328–331. [Google Scholar] [CrossRef] [PubMed]
- Yuan, H.C.; Feng, J.F.; Zhang, D.; Zhang, J.; Wang, Y.J.; Qiu, X.J. Development and Validation of UPLC-MS/MS Method for the Determination of Andrographolide in Human Plasma. Lat. Am. J. Pharm. 2015, 34, 1205–1210. [Google Scholar]
- Merck Sante, S.A.S. Glucophage® (Metformin Hydrochloride) Tablets. Package Insert from Internet 2017. Available online: https://www.accessdata.fda.gov/drugsatfda_docs/label/2017/020357s037s039,021202s021s023lbl.pdf (accessed on 20 March 2022).
- European Medicine Agency. Guideline on the Investigation of Bioequivalence. Available online: https://www.ema.europa.eu/en/documents/scientific-guideline/guideline-investigation-bioequivalence-rev1_en.pdf (accessed on 21 February 2022).
- Union, E. Pharmacokinetics Study in Man. Available online: https://www.ema.europa.eu/en/documents/scientific-guideline/pharmacokinetic-studies-man_en.pdf (accessed on 12 February 2022).
- U.S. Food and Drug Administration. Bioavailability and Bioequivalence Studies for Orally Administered Drug Products-General Considerations. Available online: http://www.fda.gov/downloads/Drugs/.../Guidances/ucm070124.pdf (accessed on 11 November 2021).
- Senn, S. Cross-over Trials in Clinical Research: Introduction; Wiley Online Library: New York, NY, USA, 2002; pp. 1–16. [Google Scholar]
- Kim, H.W. Metabolomic Approaches to Investigate the Effect of Metformin: An Overview. Int. J. Mol. Sci. 2021, 22, 10275. [Google Scholar] [CrossRef] [PubMed]
- Malaysian Herbal Monograph Committee. Malaysian Herbal Monograph 2015; National Institutes of Health: Kuala Lumpur, Malayisa, 2015. [Google Scholar]
- Sandborn, W.J.; Targan, S.R.; Byers, V.S.; Rutty, D.A.; Mu, H.; Zhang, X.; Tang, T. Andrographis paniculata Extract (HMPL-004) for Active Ulcerative Colitis. Am. J. Gastroenterol. 2013, 108, 90–98. [Google Scholar] [CrossRef] [Green Version]
- Melchior, J.; Spasov, A.A.; Ostrovskij, O.V.; Bulanov, A.E.; Wikman, G. Double-Blind, Placebo-Controlled Pilot and Phase III Study of Activity of Standardized Andrographis paniculata Herba Nees Extract Fixed Combination (Kan jang) in the Treatment of Uncomplicated Upper-Respiratory Tract Infection. Phytomedicine 2000, 7, 341–350. [Google Scholar] [CrossRef]
- Kantae, V.; Krekels, E.H.J.; Esdonk, M.J.V.; Lindenburg, P.; Harms, A.C.; Knibbe, C.A.J.; Van der Graaf, P.H.; Hankemeier, T. Integration of Pharmacometabolomics with Pharmacokinetics and Pharmacodynamics: Towards Personalized Drug Therapy. Metabolomics 2017, 13, 9. [Google Scholar] [CrossRef] [Green Version]
- Committee, S.-F.F. Recognized ECs/IRBs. Available online: https://www.sidcer-fercap.org/pages/recognized-ecs-irbs.html (accessed on 5 April 2021).
- ClinicalTrials.gov. Pharmacometabolomics of Andrographis paniculata and Metformin in Healthy Volunteers under Fasting Condition. 2019. Available online: https://clinicaltrials.gov/ct2/show/NCT04161404 (accessed on 12 January 2022).
- National Committee Clinical Research. Malaysian Guideline for Good Clinical Practice. Available online: https://www.npra.gov.my/images/Guidelines_Central/Guidelines_on_Clinical_Trial/MalaysianGuidelineforGoodClinicalPractice.pdf (accessed on 20 February 2022).
- World Medical Association. Declaration of Helsinki-Ethical Principles for Medical Research Involving Human Subjects. 2018. Available online: https://www.wma.net/policies-post/wma-declaration-of-helsinki-ethical-principles-for-medical-research-involving-human-subjects/ (accessed on 12 January 2022).
- Peace, K.; Chen, D.-G. Clinical Trial Methodology; CRC Press: Boca Raton, FL, USA, 2010. [Google Scholar]
- US Department of Health and Human Services, Food and Drug Administration. Guidance for Industry: Statistical Approaches to Establishing Bioequivalence; US Department of Health and Human Services, Food and Drug Administration: Rockville, MD, USA, 2001; p. 48. [Google Scholar]
- Nyamundanda, G.; Gormley, I.C.; Fan, Y.; Gallagher, W.M.; Brennan, L. MetSizeR: Selecting the optimal sample size for metabolomic studies using an analysis based approach. BMC Bioinform. 2013, 14, 338. [Google Scholar] [CrossRef] [Green Version]
- International Council of Harmonization. Clinical Safety Data Mangement: Definitions and Standards for Expedited Reporting. Available online: https://database.ich.org/sites/default/files/E2A_Guideline.pdf (accessed on 20 April 2021).
- Piantadosi, S.; Fisher, J.D.; Grossman, S. Practical Implementation of a Modified Continual Reassessment Method for Dose-Finding Trials. Cancer Chemother. Pharmacol. 1998, 41, 429–436. [Google Scholar] [CrossRef]
- Ivy, S.P.; Siu, L.L.; Garrett-Mayer, E.; Rubinstein, L. Approaches to Phase 1 Clinical Trial Design Focused on Safety, Efficiency, and Selected Patient Populations: A Report from the Clinical Trial Design Task Force of the National Cancer Institute Investigational Drug Steering Committee. Clin. Cancer Res. 2010, 16, 1726–1736. [Google Scholar] [CrossRef] [Green Version]
- Ishizuka, N.; Ohashi, Y. The Continual Reassessment Method and its Applications: A Bayesian Methodology for Phase I Cancer Clinical Trials. Stat. Med. 2001, 20, 2661–2681. [Google Scholar] [CrossRef]
- Song, R. Mechanism of Metformin: A Tale of Two Sites. Diabetes Care 2016, 39, 187–189. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- European Medicine Agency. Guideline on Bioanalytical Method Validation. Available online: http://www.ema.europa.eu/docs/en_GB/document_library/Scientific_guideline/2011/08/WC500109686.pdf (accessed on 9 September 2021).
- Contrepois, K.; Jiang, L.; Snyder, M. Optimized Analytical Procedures for the Untargeted Metabolomic Profiling of Human Urine and Plasma by Combining Hydrophilic Interaction (HILIC) and Reverse-Phase Liquid Chromatography (RPLC)-Mass Spectrometry. Mol. Cell. Proteom. 2015, 14, 1684–1695. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Agilent Technologies. MassHunter METLIN Metabolite PCD/PCDL Quick Start Guide. Available online: https://www.agilent.com/cs/library/usermanuals/Public/G6825-90008_MetlinPCDL_QuickStart.pdf (accessed on 18 February 2022).
- Wang, M.; Carver, J.J.; Phelan, V.V.; Sanchez, L.M.; Garg, N.; Peng, Y.; Nguyen, D.D.; Watrous, J.; Kapono, C.A.; Luzzatto-Knaan, T.; et al. Sharing and community curation of mass spectrometry data with Global Natural Products Social Molecular Networking. Nat. Biotechnol. 2016, 34, 828–837. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chong, J.; Wishart, D.S.; Xia, J. Using MetaboAnalyst 4.0 for Comprehensive and Integrative Metabolomics Data Analysis. Curr. Protoc. Bioinform. 2019, 68, e86. [Google Scholar] [CrossRef] [PubMed]
- Tee, K.B.; Ibrahim, L.; Hashim, N.M.; Saiman, M.Z.; Zakaria, Z.H.; Huri, H.Z. Pharmacokinetic -Pharmacometabolomic Approach in Early-Phase Clinical Trials: A Way Forward for Targeted Therapy in Type 2 Diabetes. Pharmaceutics 2022, 14, 1268. [Google Scholar] [CrossRef]




Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tee, K.B.; Ibrahim, L.; Hashim, N.M.; Saiman, M.Z.; Zakaria, Z.H.; Huri, H.Z. Pharmacokinetics and Metabolomic Profiling of Metformin and Andrographis paniculata: A Protocol for a Crossover Randomised Controlled Trial. J. Clin. Med. 2022, 11, 3931. https://doi.org/10.3390/jcm11143931
Tee KB, Ibrahim L, Hashim NM, Saiman MZ, Zakaria ZH, Huri HZ. Pharmacokinetics and Metabolomic Profiling of Metformin and Andrographis paniculata: A Protocol for a Crossover Randomised Controlled Trial. Journal of Clinical Medicine. 2022; 11(14):3931. https://doi.org/10.3390/jcm11143931
Chicago/Turabian StyleTee, Khim Boon, Luqman Ibrahim, Najihah Mohd Hashim, Mohd Zuwairi Saiman, Zaril Harza Zakaria, and Hasniza Zaman Huri. 2022. "Pharmacokinetics and Metabolomic Profiling of Metformin and Andrographis paniculata: A Protocol for a Crossover Randomised Controlled Trial" Journal of Clinical Medicine 11, no. 14: 3931. https://doi.org/10.3390/jcm11143931