
Planned Place of Birth—Impact of Psychopathological Risk Factors on the Choice of Birthplace and Its Postpartum Effect on Psychological Adaption: An Exploratory Study

Abstract
:1. Introduction
- Which psychopathological risk factors (current psychopathology, birth anxiety, childhood trauma) were associated with the choice of birthplace?
- Does the choice of birthplace affect the birth experience of women?
- Does the choice of birthplace influence the maternal psychopathological adjustment postpartum (i.e., postpartum depressive symptoms and birth anxiety felt during childbirth)?
2. Materials and Methods
2.1. Study Design
2.2. Study Participants
2.3. Instruments
- Prenatal Distress
- Depressive Symptoms
- Birth Anxiety Symptoms
- Childhood Trauma
- Birth experience
2.4. Statistical Analysis
3. Results
3.1. Study Population and Background Characteristics
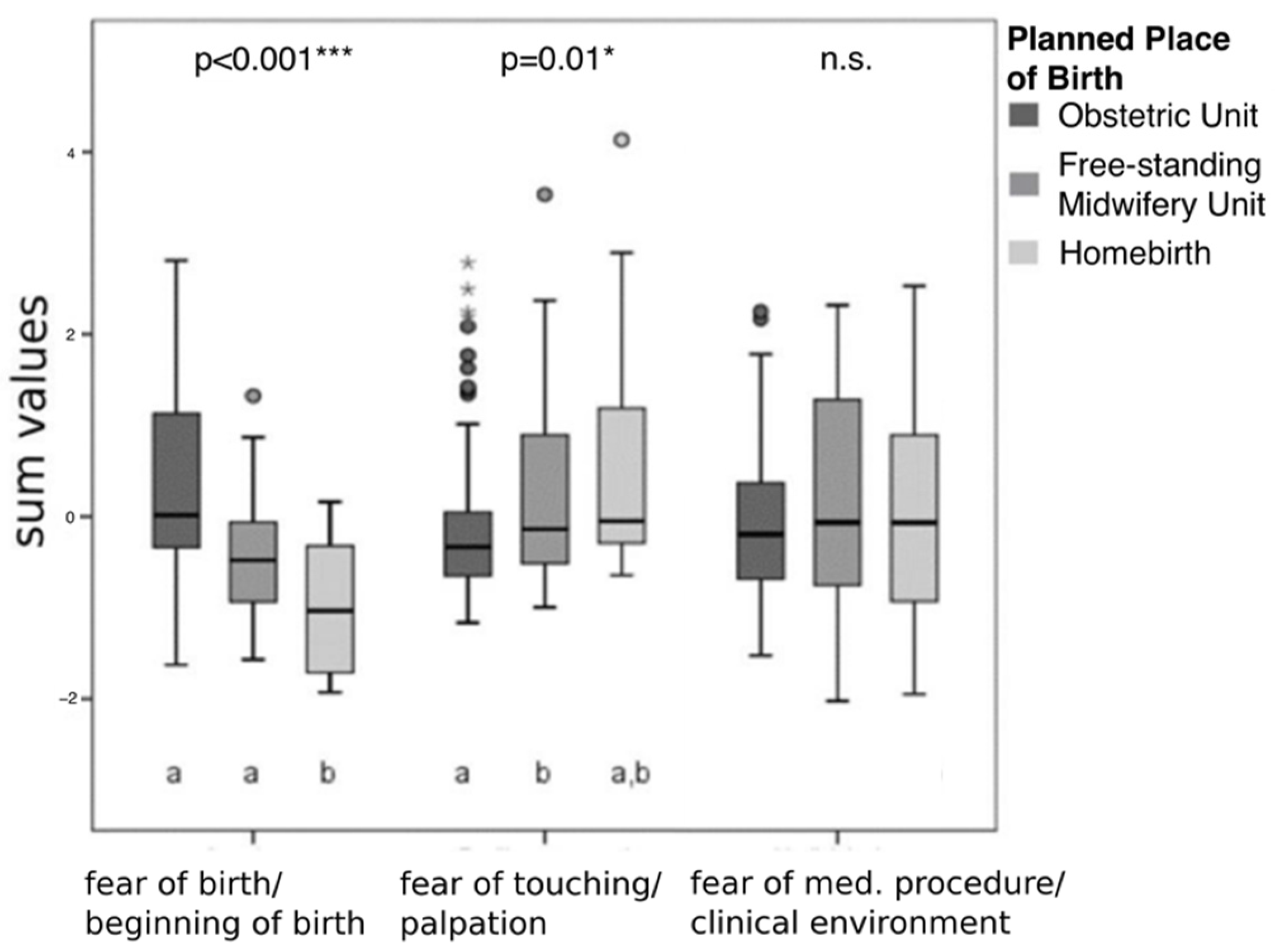
3.2. Psychopathological Risk Factors and Planned Place of Birth
3.3. Confounding Factors
3.4. Birth Experience and Planned Place of Birth
3.5. Postpartum Psychological Adaption and Congruent Birthplace
4. Discussion
4.1. Background Characteristics and Planned Birthplace
4.2. Psychopathological Risk Factors and Planned Place of Birth
4.3. Birth Experience, Postpartal Psychological Adaption and Congruent Birthplace
4.4. Limitations of the Research Design
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Loytved, C. Out-of-Hospital Births in Germany–Quality Report 2019; Auerbach: QUAG e.V.: Storkow, Germany, 2019. [Google Scholar]
- Coxon, K.; Chisholm, A.; Malouf, R.; Rowe, R.; Hollowell, J. What influences birth place preferences, choices and decision-making amongst healthy women with straightforward pregnancies in the UK? A qualitative evidence synthesis using a ‘best fit’ framework approach. BMC Pregnancy Childbirth 2017, 17, 103. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Coxon, K.; Sandall, J.; Fulop, N. To what extent are women free to choose where to give birth? How discourses of risk, blame and responsibility influence birth place decisions. Health Risk Soc. 2014, 16, 51–67. [Google Scholar] [CrossRef] [Green Version]
- Sjöblom, I.; Idvall, E.; Rådestad, I.; Lindgren, H. A provoking choice—Swedish women’s experiences of reactions to their plans to give birth at home. Women Birth 2011, 25, e11–e18. [Google Scholar] [CrossRef]
- Brocklehurst, P.; Puddicombe, D.; Hollowell, J.; Stewart, M.; Linsell, L.; Macfarlane, A.J.; McCourt, C. Birthplace in England Collaborative Group. Perinatal and maternal outcomes by planned place of birth for healthy women with low risk pregnancies: The Birthplace in England national prospective cohort study. BMJ 2011, 343, d7400. [Google Scholar]
- Christiaens, W.; Bracke, P. Place of birth and satisfaction with childbirth in Belgium and the Netherlands. Midwifery 2009, 25, e11–e19. [Google Scholar] [CrossRef]
- Janssen, P.; Henderson, A.; Vedam, S. The experience of planned home birth: Views of the first 500 women. Birth 2009, 36, 297–304. [Google Scholar] [CrossRef]
- Overgaard, C.; Fenger-Grøn, M.; Sandall, J. The impact of birthplace on women’s birth experiences and perceptions of care. Soc. Sci. Med. 2012, 74, 973–981. [Google Scholar] [CrossRef]
- Karlström, A.; Nystedt, A.; Hildingsson, I. The meaning of a very positive birth experience: Focus groups discussions with women. BMC Pregnancy Childbirth 2015, 15, 251. [Google Scholar] [CrossRef] [Green Version]
- Coyle, K.; Hauck, Y.; Percival, P.; Kristjanson, L. Normality and collaboration: Mothers’ perceptions of birth centre versus hospital care. Midwifery 2001, 17, 182–193. [Google Scholar] [CrossRef] [PubMed]
- Montgomery, E. Feeling safe: A metasynthesis of the maternity care needs of women who were sexually abused in childhood. Birth 2013, 40, 88–95. [Google Scholar] [CrossRef] [PubMed]
- Van Haaren-ten Haken, T.; Hendrix, M.; Nieuwenhuijze, M.; Budé, L.; Vries, R.; Nijhuis, J. Preferred place of birth: Characteristics and motives of low-risk nulliparous women in the Netherlands. Midwifery 2012, 28, 609–618. [Google Scholar] [CrossRef]
- Witteveen, A.; Cock, P.; Huizink, A.; de Jonge, A.; Klomp, T.; Westerneng, M.; Geerts, C. Pregnancy related anxiety and general anxious or depressed mood and the choice for birth setting: A secondary data-analysis of the DELIVER study. BMC Pregnancy Childbirth 2016, 16, 363. [Google Scholar] [CrossRef] [Green Version]
- Oberndörfer, K. Angst im Zusammenhang mit Schwangerschaft und Geburt. Hebamme 2005, 18, 75–78. [Google Scholar] [CrossRef] [Green Version]
- Karestan, C.; Koenen, C.; Roberts, A.; Stone, D.; Dunn, E. The epidemiology of early childhood trauma. J. Psychosom. Res. 2006, 61, 139–151. [Google Scholar]
- Lev-Wiesel, R.; Daphna-Tekoah, S.; Hallak, M. Childhood sexual abuse as a predictor of birth-related posttraumatic stress and postpartum posttraumatic stress. Child. Abuse Negl. 2009, 33, 877–887. [Google Scholar] [CrossRef] [PubMed]
- Leeners, B.; Richter-Appelt, H.; Imthurn, B.; Rath, W. Influence of childhood sexual abuse on pregnancy, delivery, and the early postpartum period in adult women. J. Psychosom Res. 2006, 612, 139–151. [Google Scholar] [CrossRef]
- Blackmore, E.R.; Putnam, F.W.; Pressman, E.K.; Rubinow, D.R.; Putnam, K.T.; Matthieu, M.M.; Gilchrist, M.A.; Jones, I.; O’Connor, T.G. The Effects of Trauma History and Prenatal Affective Symptoms on Obstetric Outcomes. J. Trauma Stress 2016, 29, 245–252. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Modarres, M.; Afrasiabi, S.; Rahnama, P.; Montazeri, A. Prevalence and risk factors of childbirth-related post-traumatic stress symptoms. BMC Pregnancy Childbirth. 2012, 12, 88. [Google Scholar] [CrossRef] [Green Version]
- O’Donovan, A.; Alcorn, K.L.; Patrick, J.C.; Creedy, D.K.; Dawe, S.; Devilly, G.J. Predicting posttraumatic stress disorder after childbirth. Midwifery 2014, 308, 935–941. [Google Scholar] [CrossRef] [Green Version]
- Rodríguez-Almagro, J.; Hernández-Martínez, A.; Rodríguez-Almagro, D.; Quirós-García, J.; Martínez-Galiano, J.; Gómez-Salgado, J. Women’s perceptions of living a traumatic childbirth experience and factors related to a birth experience. Int. J. Environ. Res. Public Health 2019, 16, 1654. [Google Scholar] [CrossRef] [Green Version]
- Yali, A.M.; Lobel, M. Coping and distress in pregnancy: An investigation of medically high risk women. J. Psychosom. Obstet. Gynecol. 1999, 20, 39–52. [Google Scholar] [CrossRef] [PubMed]
- Cox, J.L.; Holden, J.M.; Sagovsky, R. Detection of postnatal depression. Development of the 10-item Edinburgh Postnatal Depression Scale. Br. J. Psychiatry 1987, 150, 782–786. [Google Scholar] [CrossRef] [Green Version]
- Bergant, A.M.; Nguyen, T.; Heim, K.; Ulmer, H.; Dapunt, O. Deutschsprachige fassung und validierung der Edinburgh post natal depression scale. Dtsch. Med. Wschr 1998, 123, 35–40. [Google Scholar] [CrossRef]
- Lukesch, H. Geburts-Angst-Skala–Handanweisung; Hogrefe Verlag: Göttingen, Germany, 1983. [Google Scholar]
- Bernstein, D.P.; Stein, J.A.; Newcomb, M.D.; Walker, E.; Pogge, D.; Ahluvalia, T.; Stokes, J.; Handelsman, L.; Medrano, M.; Desmond, D.; et al. Development and validation of a brief screening version of the childhood trauma questionnaire. Child. Abuse Negl. 2003, 27, 169–190. [Google Scholar] [CrossRef]
- Wingenfeld, K.; Spitzer, C.; Mensebach, C.; Grabe, H.J.; Hill, A.; Gast, U.; Schlosser, N.; Hopp, H.; Beblo, T.; Driessen, M. The German version of the Childhood Trauma Questionnaire (CTQ): Preliminary psychometric properties. Psychother. Psychosom. Med. Psychol. 2010, 60, 442–450. [Google Scholar] [CrossRef] [PubMed]
- Stadlmayr, W.; Bitzer, J.; Hösli, I.; Amsler, F.; Leupold, J.; Schwendke-Kliem, A.; Simoni, H.; Bürgin, D. Birth as a multidimensional experience: Comparison of the english- and german-language versions of Salmon’s Item List. J. Psychosom. Obstet. Gynaecol. 2001, 4, 205–214. [Google Scholar] [CrossRef]
- Gordon, A.; Glazko, G.; Qiu, X.; Yakovlev, A. Control of the mean number of false discoveries, bonferroni and stability of multiple testing. Ann. Appl. Stat. 2007, 1, 179–190. [Google Scholar] [CrossRef] [Green Version]
- Anthony, S.; Buitendijk, S.; Offerhaus, P.; Dommelen, P.; Palde Bruin, K. Maternal factors and the probability of a planned home birth. BJOG 2005, 112, 748–753. [Google Scholar] [CrossRef]
- Abou-Dakn, M.; Feige, A.; Franitza, M.; Kühnert, M.; Seelbach-Göbel, B.; Schlembach, D. Position der DGGG zur außerklinischen Geburtshilfe. Frauenarzt 2018, 59, 7. [Google Scholar]
- Hildingsson, I.; Lindgren, H.; Haglund, B.; Rådestad, I. Characteristics of women giving birth at home in Sweden: A national register study. Am. J. Obstet. Gynecol. 2006, 195, 1366–1372. [Google Scholar] [CrossRef]
- Lindgren, H.; Rådestad, I.; Christensson, K.; Hildingsson, I. Outcome of planned home births compared to hospital births in Sweden between 1992 and 2004. A population-based register study. Acta Obst. Gynecol. Scand. 2008, 87, 751–759. [Google Scholar] [CrossRef]
- Waldenström, U.; Nilsson, C.-A. Characteristics of women choosing birth center care. Acta Obstet. Gynecol. Scand. 1993, 72, 181–188. [Google Scholar] [CrossRef] [PubMed]
- Weidner, K.; Garthus-Niegel, S.; Junge-Hoffmeister, J. Traumatic birth: Recognition and prevention. Zeitschr. Geburtsh. Neonat. 2018, 222, 189–196. [Google Scholar]
- World Health Organization (WHO). Violence Against Women: Intimate Partner and Sexual Violence Against Women: Evidence Brief; WHO: Geneva, Switzerland, 2019. [Google Scholar]
- Jundt, K.; Haertl, K.; Knobbe, A.; Kaestner, R.; Friese, K.; Peschers, U. Pregnant women after physical and sexual abuse in Germany. Gynecol. Obstet. Investig. 2009, 68, 82–87. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Beck, C.T.; Casavant, S. Synthesis of mixed research on posttraumatic stress related to traumatic birth. JOGNN 2019, 48, 385–397. [Google Scholar] [CrossRef]
- Deutscher Hebammenverband. Empfehlungen für Traumasensible Begleitung durch Hebammen; DHV e.V.: Karlsruhe, Germany, 2012. [Google Scholar]
- Bohren, M.; Hofmeyr, G.; Sakala, C.; Fukuzawa, R.; Cuthbert, A. Continuous support for women during childbirth. Cochrane Database Syst. Rev. 2017, 7, CD003766. [Google Scholar] [CrossRef] [PubMed]
- Hodnett, E. Pain and women’s satisfaction with the experience of childbirth: A systematic review. Am. J. Obstet. Gynecol. 2002, 186, S160–S172. [Google Scholar]
- Bergink, V.; Kooistra, L.; Lambregtse-van den Berg, M.; Wijnen, H.; Bunevicius, R.; van Baar, A.; Pop, V. Validation of the edinburgh depression scale during pregnancy. J. Psychosom. Res. 2011, 70, 385–389. [Google Scholar] [CrossRef]


{kind=link}
| Variables | Total | OU | FMU | HB | Test Stat. | p |
|---|---|---|---|---|---|---|
| Age (years) 1 | 29.1 ± 4.3 | 29.1 ± 4.0 | 28.9 ± 4.9 | 30.3 ± 4.8 | F = 0.53 | 0.59 |
| Parity | X2 = 16.8 | <0.001 ** | ||||
| Primipara | 116 (65.5%) | 91 (74.4%) | 22(52.4%) | 3 (23.1%) | ||
| Multipara | 61 (34.5%) | 30 (25.6%) | 20 (47.6%) | 11 (76.9%) | ||
| Marital Status | X2 = 11.7 | 0.34 | ||||
| Married | 72 (41.6%) | 42 (35.6%) | 21 (50%) | 9 (69.2%) | ||
| Permanent relationship | 93 (53.8%) | 70 (59.3%) | 19 (45.2%) | 4 (30.8%) | ||
| Single | 5 (2.9%) | 3 (2.5%) | 2 (4.8%) | - | ||
| Living separately | 1 (0.6%) | 1 (0.8%) | - | - | ||
| Other | 1 (0.6%) | 1 (0.8%) | - | - | ||
| Education Level | X2 = 10.7 | 0.33 | ||||
| Middle-school till 9th grade | 2 (1.2%) | - | 1 (2.4%) | 1 (7.7%) | ||
| Middle school till 10th grade | 36 (20.8%) | 27 (22.9%) | 8 (19.0%) | 1 (7.7%) | ||
| High-school diploma | 75 (44.5%) | 50 (42.4%) | 17 (40.5%) | 8 (61.5%) | ||
| University and masters | 60 (33.5%) | 41 (34.7%) | 16 (38.1%) | 3 (23.1%) | ||
| Occupation | X2 = 31.5 | <0.001 *** | ||||
| Employed | 136 (76.8%) | 101 (85.6%) | 26 (61.9%) | 6 (46.2%) | ||
| Housewife | 6 (3.5%) | 1 (.8%) | 1 (2.4%) | 4 (30.8%) | ||
| In education | 17 (9.8%) | 7 (5.9%) | 9 (21.4%) | 1 (7.7%) | ||
| Unemployed | 10 (5.8%) | 5 (4.2%) | 3 (7.1%) | 2 (15.4%) | ||
| Other | 7 (4.0%) | 4 (3.4%) | 3 (7.1%) | - | ||
| Combined Family Income (per annum) | H = 3.0 | 0.22 | ||||
| <6000€ | 5 (2.9%) | 1 (0.9%) | 3 (7.3%) | 1 (7.7%) | ||
| 6000–12,000€ | 19 (11.0%) | 9 (7.7%) | 7 (17.1%) | 3 (23.1%) | ||
| 12,000–18,000€ | 25 (14.5%) | 16 (13.7%) | 8 (19.5%) | 1 (7.7%) | ||
| 18,000–24,000€ | 31 (17.9%) | 26 (22.2%) | 4 (9.8%) | 1 (7.7%) | ||
| 24,000–36,000€ | 54 (31.2%) | 40 (34.2%) | 11 (26.8%) | 3 (23.1%) | ||
| >36,000€ | 37 (21.4%) | 25 (21.4%) | 8 (19.5%) | 4 (30.8%) | ||
| Satisfaction with Financial Situation | X2 = 8.2 | 0.19 | ||||
| Satisfied | 59 (34.1%) | 43 (36.8%) | 9 (21.4%) | 7 (53.8%) | ||
| Rather satisfied | 33 (19.1%) | 21 (17.9%) | 9 (21.4%) | 3 (23.1%) | ||
| Rather unsatisfied | 71 (41.0%) | 45 (38.5%) | 23 (54.8%) | 3 (23.1%) | ||
| Unsatisfied | 9 (5.2%) | 8 (6.8%) | 1 (2.4%) | - | ||
| Childhood Trauma (CTQ) | 42 (24.3%) | 22 (18.6%) | 13 (31.0%) | 7 (53.8%) | X2 = 8.7 | 0.01 * |
| Physical abuse | 18 (10.4%) | 8 (6.8%) | 5 (11.9%) | 5 (38.5%) | X2 = 9.8 | 0.005 ** |
| Sexual abuse | 19 (11.0%) | 10 (8.5%) | 7 (16.7%) | 2 (15.4%) | X2 = 2.8 | 0.19 |
| Emotional neglect | 9 (5.2%) | 6 (5.1%) | 1 (2.4%) | 2 (15.4%) | X2 = 3.1 | 0.19 |
| Physical neglect | 6 (3.5%) | 5 (4.2%) | 1 (2.4%) | - | X2 = 0.27 | >0.99 |
| Emotional abuse | 27 (15.6%) | 20 (16.9%) | 4 (9.5%) | 3 (23.1%) | X2 = 2.0 | 0.39 |
| n | Mean | SD | Min | Max | H | p | ||
|---|---|---|---|---|---|---|---|---|
| (t1) PDQ | OU | 121 | 14.5 | 6.9 | 3 | 31 | 14.24 | 0.001 ** |
| FMU | 42 | 12.1 | 7.9 | 2 | 27 | |||
| HB | 14 | 7.9 | 5.3 | 3 | 20 | |||
| (t1) EPDS | OU | 121 | 5.8 | 3.8 | 0 | 18 | 3.7 | 0.16 |
| FMU | 42 | 6.7 | 4.5 | 0 | 17 | |||
| HB | 14 | 4.4 | 4.7 | 0 | 17 | |||
| (t1) BAS | OU | 121 | 75.3 | 34.7 | 9 | 178 | 1.35 | 0.51 |
| FMU | 42 | 77.9 | 38.8 | 15 | 170 | |||
| HB | 14 | 61.7 | 36.5 | 0 | 139 | |||
| (t1) CTQ | OU | 121 | 11.43 | 2.99 | 10 | 25 | 8.09 | 0.02 * |
| FMU | 42 | 12.37 | 4.80 | 10 | 32 | |||
| HB | 14 | 15.15 | 5.58 | 10 | 27 | |||
| Physical abuse | OU | 121 | 5.97 | 2.42 | 5 | 20 | 13.17 | 0.001 ** |
| FMU | 42 | 5.74 | 1.85 | 5 | 13 | |||
| HB | 14 | 9.62 | 5.32 | 5 | 22 | |||
| Sexual abuse | OU | 121 | 5.47 | 1.39 | 5 | 11 | 3.39 | 0.18 |
| FMU | 42 | 6.22 | 3.12 | 5 | 20 | |||
| HB | 14 | 6.54 | 3.46 | 5 | 16 | |||
| Emotional abuse | OU | 121 | 8.49 | 4.19 | 5 | 21 | 8.01 | 0.02 * |
| FMU | 42 | 8.12 | 3.05 | 5 | 19 | |||
| HB | 14 | 11.46 | 4.27 | 5 | 19 | |||
| Physical neglect | OU | 121 | 5.83 | 1.48 | 4 | 10 | 1.14 | 0.57 |
| FMU | 42 | 5.89 | 1.61 | 4 | 11 | |||
| HB | 14 | 6.23 | 1.59 | 5 | 9 | |||
| Emotional neglect | OU | 121 | 6.92 | 3.14 | 5 | 20 | 2.77 | 0.25 |
| FMU | 42 | 6.76 | 2.66 | 4 | 16 | |||
| HB | 14 | 8.23 | 4.02 | 5 | 18 |
| SIL | Group | n | Mean | SD | Min | Max | H | p |
|---|---|---|---|---|---|---|---|---|
| Total score | OUt1=t2 | 119 | 82.8 | 20.5 | 23 | 114 | 3.47 | 0.18 |
| FMt1=t2 | 30 | 87.7 | 20.5 | 34 | 112 | |||
| HBt1=t2 | 12 | 93.3 | 8.4 | 78 | 105 | |||
| Fulfilment | OUt1=t2 | 119 | 33.4 | 8.8 | 6 | 42 | 0.68 | 0.71 |
| FMt1=t2 | 30 | 34.4 | 8.6 | 7 | 42 | |||
| HBt1=t2 | 12 | 35.0 | 3.9 | 27 | 40 | |||
| Good emotional adaption | OUt1=t2 | 119 | 26.0 | 7.0 | 6 | 35 | 10.52 | 0.005 ** |
| FMt1=t2 | 30 | 28.2 | 7.7 | 8 | 35 | |||
| HBt1=t2 | 12 | 30.7 | 3.4 | 24 | 35 | |||
| Negative emotional experience 1 | OUt1=t2 | 119 | 18.8 | 3.6 | 6 | 21 | 9.06 | 0.01 * |
| FMt1=t2 | 30 | 19.3 | 3.4 | 10 | 21 | |||
| HBt1=t2 | 12 | 20.9 | 0.3 | 20 | 21 | |||
| Physical discomfort 1 | OUt1=t2 | 119 | 11.3 | 3.8 | 3 | 21 | 0.75 | 0.69 |
| FMt1=t2 | 30 | 11.7 | 4.1 | 4 | 20 | |||
| HBt1=t2 | 12 | 12.2 | 2.9 | 8 | 18 |
| n | Mean | SD | Min | Max | H | p | ||
|---|---|---|---|---|---|---|---|---|
| (t1) EPDS | OUt1=t2 | 119 | 5.85 | 3.92 | 0 | 18 | 5.37 | 0.07 |
| FMt1=t2 | 30 | 6.57 | 4.69 | 0 | 17 | |||
| HBt1=t2 | 12 | 4.50 | 4.90 | 0 | 17 | |||
| (t2) EPDS | OUt1=t2 | 119 | 11.01 | 3.26 | 7 | 23 | 1.28 | 0.53 |
| FMt1=t2 | 30 | 11.53 | 3.34 | 7 | 19 | |||
| HBt1=t2 | 12 | 11.70 | 4.52 | 7 | 19 | |||
| (t1) BAS | OUt1=t2 | 119 | 75.50 | 34.34 | 9 | 178 | 0.29 | 0.86 |
| FMt1=t2 | 30 | 77.67 | 39.83 | 15 | 170 | |||
| HBt1=t2 | 12 | 78.50 | 32.59 | 26 | 139 | |||
| (t2) BAS 1 | OUt1=t2 | 119 | 66.40 | 32.49 | 4 | 176 | 19.36 | <0.001 *** |
| FMt1=t2 | 30 | 44,43 | 20.47 | 12 | 99 | |||
| HBt1=t2 | 12 | 36.90 | 23.12 | 6 | 66 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Winter, C.; Junge-Hoffmeister, J.; Bittner, A.; Gerstner, I.; Weidner, K. Planned Place of Birth—Impact of Psychopathological Risk Factors on the Choice of Birthplace and Its Postpartum Effect on Psychological Adaption: An Exploratory Study. J. Clin. Med. 2022, 11, 292. https://doi.org/10.3390/jcm11020292
Winter C, Junge-Hoffmeister J, Bittner A, Gerstner I, Weidner K. Planned Place of Birth—Impact of Psychopathological Risk Factors on the Choice of Birthplace and Its Postpartum Effect on Psychological Adaption: An Exploratory Study. Journal of Clinical Medicine. 2022; 11(2):292. https://doi.org/10.3390/jcm11020292
Chicago/Turabian StyleWinter, Clara, Juliane Junge-Hoffmeister, Antje Bittner, Irene Gerstner, and Kerstin Weidner. 2022. "Planned Place of Birth—Impact of Psychopathological Risk Factors on the Choice of Birthplace and Its Postpartum Effect on Psychological Adaption: An Exploratory Study" Journal of Clinical Medicine 11, no. 2: 292. https://doi.org/10.3390/jcm11020292