
Surgical Treatment for Simple Isolated and Displaced Olecranon Fractures: Comparison between Plate and Tension Band Wire Fixation
 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Surgical Technique
2.2. Clinical and Radiographic Evaluation
2.3. Statistical Analysis
3. Results
3.1. Patient Demographics
3.2. Hospitalization and Surgery Duration
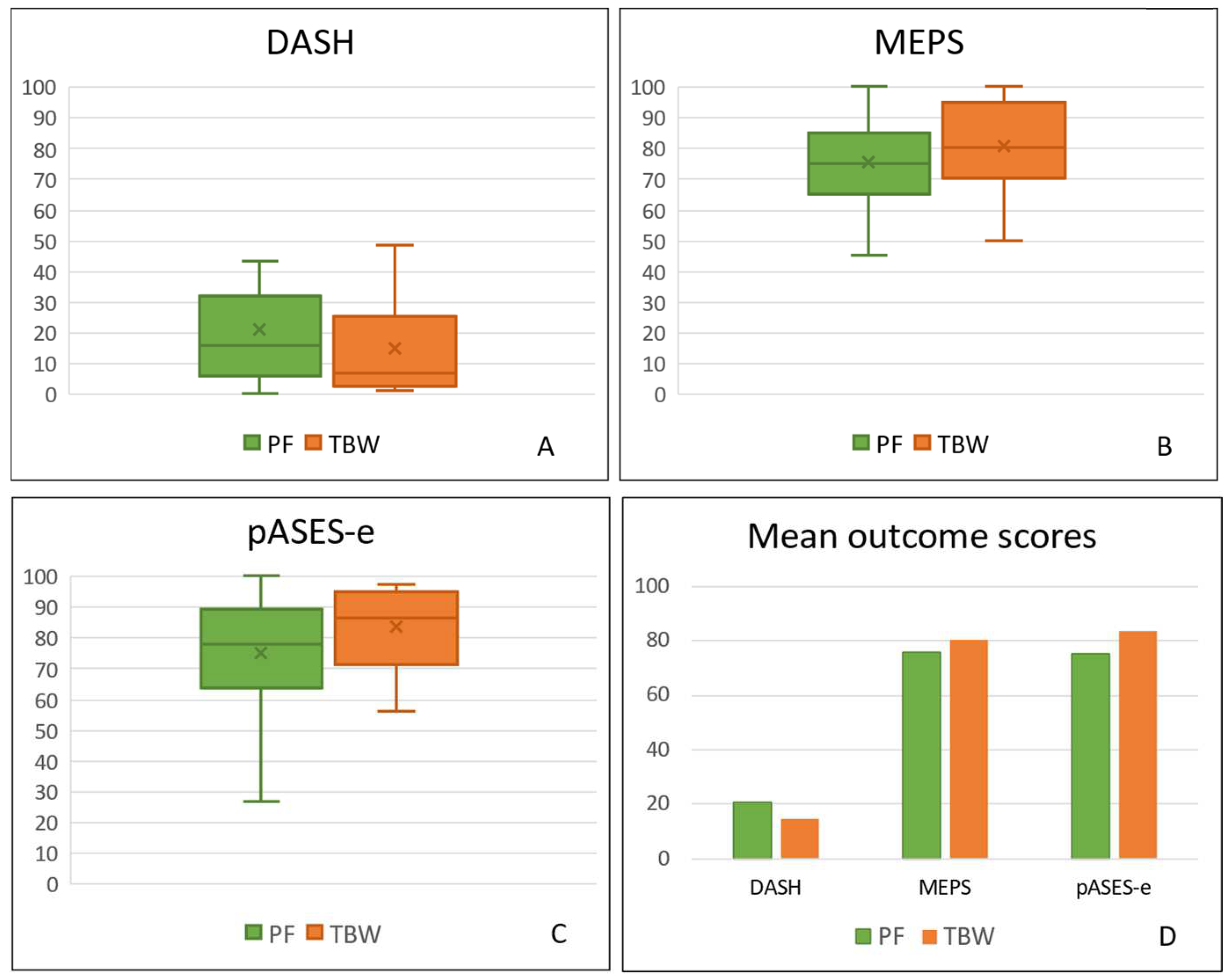
3.3. Patient Outcomes
3.4. Surgical Complications
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Appendix A
- Attachment A1

- Attachment A2

- Attachment A3

References
- Duckworth, A.D.; Clement, N.D.; Aitken, S.A.; Court-Brown, C.M.; McQueen, M.M. The Epidemiology of Fractures of the Proximal Ulna. Injury 2012, 43, 343–346. [Google Scholar] [CrossRef] [PubMed]
- Rommens, P.M.; Schneider, R.U.; Reuter, M. Functional Results after Operative Treatment of Olecranon Fractures. Acta Chir. Belg. 2004, 104, 191–197. [Google Scholar] [CrossRef] [PubMed]
- Karlsson, M.K.; Hasserius, R.; Karlsson, C.; Besjakov, J.; Josefsson, P.O. Fractures of the Olecranon: A 15- to 25-Year Followup of 73 Patients. Clin. Orthop. Relat. Res. 2002, 403, 205–212. [Google Scholar] [CrossRef]
- Hotchkiss, R.N. Fractures of the Olecranon. In Rockwood and Green’s Fractures in Adults; Rockwood, C.A., Jr., Green, D.P., Bucholz, R.W., Heckman, J.D., Eds.; JB Lippincott: Philadelphia, PA, USA, 1996; pp. 984–996. [Google Scholar]
- Brüggemann, A.; Mukka, S.; Wolf, O. Epidemiology, Classification and Treatment of Olecranon Fractures in Adults: An Observational Study on 2462 Fractures from the Swedish Fracture Register. Eur. J. Trauma Emerg. Surg. 2022, 48, 2255–2263. [Google Scholar] [CrossRef] [PubMed]
- Hak, D.J.; Golladay, G.J. Olecranon Fractures: Treatment Options. J. Am. Acad. Orthop. Surg. 2000, 8, 266–275. [Google Scholar] [CrossRef] [PubMed]
- Wood, T.; Thomas, K.; Farrokhyar, F.; Ristevski, B.; Bhandari, M.; Petrisor, B. A Survey of Current Practices and Preferences for Internal Fixation of Displaced Olecranon Fractures. Can. J. Surg. 2015, 58, 250–256. [Google Scholar] [CrossRef] [PubMed]
- Duckworth, A.D.; Court-Brown, C.M.; McQueen, M.M. Isolated Displaced Olecranon Fracture. J. Hand Surg. Am. 2012, 37, 341–345. [Google Scholar] [CrossRef]
- Veillette, C.J.H.; Steinmann, S.P. Olecranon Fractures. Orthop. Clin. N. Am. 2008, 39, 229–236. [Google Scholar] [CrossRef]
- Newman, S.D.S.; Mauffrey, C.; Krikler, S. Olecranon Fractures. Injury 2009, 40, 575–581. [Google Scholar] [CrossRef]
- Wolfgang, G.; Burke, F.; Bush, D.; Parenti, J.; Perry, J.; LaFollette, B.; Lillmars, S. Surgical Treatment of Displaced Olecranon Fractures by Tension Band Wiring Technique. Clin. Orthop. 1987, 224, 192–204. [Google Scholar] [CrossRef]
- Paremain, G.P.; Novak, V.P.; Jinnah, R.H.; Belkoff, S.M. Biomechanical Evaluation of Tension Band Placement for the Repair of Olecranon Fractures. Clin. Orthop. Relat. Res. 1997, 335, 325–330. [Google Scholar] [CrossRef]
- Villanueva, P.; Osorio, F.; Commessatti, M.; Sanchez-Sotelo, J. Tension-Band Wiring for Olecranon Fractures: Analysis of Risk Factors for Failure. J. Shoulder Elb. Surg. 2006, 15, 351–356. [Google Scholar] [CrossRef] [PubMed]
- Erturer, R.E.; Sever, C.; Sonmez, M.M.; Ozcelik, I.B.; Akman, S.; Ozturk, I. Results of Open Reduction and Plate Osteosynthesis in Comminuted Fracture of the Olecranon. J. Shoulder Elb. Surg. 2011, 20, 449–454. [Google Scholar] [CrossRef]
- Bailey, C.S.; MacDermid, J.; Patterson, S.D.; King, G.J.W. Outcome of Plate Fixation of Olecranon Fractures. J. Orthop. Trauma. 2001, 15, 542–548. [Google Scholar] [CrossRef] [PubMed]
- Weber, B.G.; Vasey, H. Osteosynthesis in Olecranon Fractures. Z. Unfallmed Berufskr. 1963, 56, 90–96. [Google Scholar] [PubMed]
- Deliyannis, S.N. Comminuted Fractures of the Olecranon Treated by the Weber-Vasey Technique. Injury 1973, 5, 19–24. [Google Scholar] [CrossRef] [PubMed]
- Quintero, J.; Varecka, T. Olecranon, Radial Head and Complex Elbow Injuries. In AO Principles of Fracture Management-Specific Fractures—Volume 2, 2nd ed.; Ruedi, T.P., Buckley, R.E., Moran, C.G., Eds.; Thieme: Stuttgart, Germany, 2007; pp. 628–633. [Google Scholar]
- Fyfe, I.; Mossad, M.; Holdsworth, B. Methods of Fixation of Olecranon Fractures. An Experimental Mechanical Study. J. Bone Jt. Surg. Br. 1985, 67-B, 367–372. [Google Scholar] [CrossRef]
- Murphy, D.F.; Greene, W.B.; Dameron, T.B. Displaced Olecranon Fractures in Adults: Clinical Evaluation. Clin. Orthop. 1987, 224, 215–223. [Google Scholar] [CrossRef]
- Çağlar, C.; Akçaalan, S.; Özaslan, H.I.; Yağar, H.; Uğurlu, M. Comparison of Tension Band Wiring and Plate Fixation in Mayo Type 2A Olecranon Fractures. Jt. Dis. Relat. Surg. 2021, 32, 85–92. [Google Scholar] [CrossRef]
- Morrey, B.F. Current Concepts in the Treatment of Fractures of the Radial Head, the Olecranon, and the Coronoid. Instr. Course Lect. 1995, 44, 175–185. [Google Scholar] [CrossRef]
- Lavigne, G.; Baratz, M. Fractures of the Olecranon. J. Am. Soc. Surg. Hand 2004, 4, 94–102. [Google Scholar] [CrossRef]
- Baecher, N.; Edwards, S. Olecranon Fractures. J. Hand Surg. 2013, 38, 593–604. [Google Scholar] [CrossRef] [PubMed]
- Hoelscher-Doht, S.; Kladny, A.-M.; Paul, M.M.; Eden, L.; Buesse, M.; Meffert, R.H. Low-Profile Double Plating versus Dorsal LCP in Stabilization of the Olecranon Fractures. Arch. Orthop. Trauma. Surg. 2021, 141, 245–251. [Google Scholar] [CrossRef] [PubMed]
- Moritomo, H.; Murase, T.; Arimitsu, S.; Oka, K.; Yoshikawa, H.; Sugamoto, K. The in Vivo Isometric Point of the Lateral Ligament of the Elbow. J. Bone Jt. Surg. 2007, 89, 2011–2017. [Google Scholar] [CrossRef]
- Nuttall, D.; Birch, A.; Trail, I.I.; Espag, M.P.; Clark, D.I.; Stanley, J.K. Assessing Elbow Assessment, Past, Present and Future. Shoulder Elb. 2010, 2, 43–54. [Google Scholar] [CrossRef]
- Longo, U.G.; Franceschi, F.; Loppini, M.; Maffulli, N.; Denaro, V. Rating Systems for Evaluation of the Elbow. Br. Med. Bull. 2008, 87, 131–161. [Google Scholar] [CrossRef] [PubMed]
- Hudak, P.L.; Amadio, P.C.; Bombardier, C.; Beaton, D.; Cole, D.; Davis, A.; Hawker, G.; Katz, J.N.; Makela, M.; Marx, R.G.; et al. Development of an Upper Extremity Outcome Measure: The DASH (Disabilities of the Arm, Shoulder, and Head). Am. J. Ind. Med. 1996, 29, 602–608. [Google Scholar] [CrossRef]
- Beaton, D.E.; Katz, J.N.; Fossel, A.H.; Wright, J.G.; Tarasuk, V.; Bombardier, C. Measuring the Whole or the Parts? J. Hand Ther. 2001, 14, 128–142. [Google Scholar] [CrossRef]
- Cusick, M.C.; Bonnaig, N.S.; Azar, F.M.; Mauck, B.M.; Smith, R.A.; Throckmorton, T.W. Accuracy and Reliability of the Mayo Elbow Performance Score. J. Hand Surg. Am. 2014, 39, 1146–1150. [Google Scholar] [CrossRef]
- Schneeberger, A.G.; Kösters, M.C.; Steens, W. Comparison of the Subjective Elbow Value and the Mayo Elbow Performance Score. J. Shoulder Elb. Surg. 2014, 23, 308–312. [Google Scholar] [CrossRef]
- Morrey, B.F.; An, K. Functional Evaluation of the Elbow. In The Elbow and Its Disorders; Morrey, B.F., Sanchez-Sotelo, J., Eds.; Saunders Elsevier: Philadelphia, PA, USA, 2008; pp. 80–89. [Google Scholar]
- Vincent, J.I.; MacDermid, J.C.; King, G.J.W.; Grewal, R. Validity and Sensitivity to Change of Patient-Reported Pain and Disability Measures for Elbow Pathologies. J. Orthop. Sports Phys. Ther. 2013, 43, 263–274. [Google Scholar] [CrossRef] [PubMed]
- Research Committee American Shoulder and Elbow Surgeons; King, G.J.W.; Richards, R.R.; Murnahan, J.P.; Mow, V.C.; Woo, S.L.Y. A Standardized Method for Assessment of Elbow Function. J. Shoulder Elb. Surg. 1999, 8, 351–354. [Google Scholar] [CrossRef]
- Chalidis, B.E.; Sachinis, N.C.; Samoladas, E.P.; Dimitriou, C.G.; Pournaras, J.D. Is Tension Band Wiring Technique the “Gold Standard” for the Treatment of Olecranon Fractures? A Long Term Functional Outcome Study. J. Orthop. Surg. Res. 2008, 3, 9. [Google Scholar] [CrossRef] [PubMed]
- Gordon, M.J.; Budoff, J.E.; Yeh, M.L.; Luo, Z.-P.; Noble, P.C. Comminuted Olecranon Fractures: A Comparison of Plating Methods. J. Shoulder Elb. Surg. 2006, 15, 94–99. [Google Scholar] [CrossRef]
- Hutchinson, D.T.; Horwitz, D.S.; Ha, G.; Thomas, C.W.; Bachus, K.N. Cyclic Loading of Olecranon Fracture Fixation Constructs. J. Bone Jt. Surg. Am. 2003, 85, 831–837. [Google Scholar] [CrossRef] [PubMed]
- Brink, P.R.G.; Windolf, M.; de Boer, P.; Brianza, S.; Braunstein, V.; Schwieger, K. Tension Band Wiring of the Olecranon: Is It Really a Dynamic Principle of Osteosynthesis? Injury 2013, 44, 518–522. [Google Scholar] [CrossRef] [PubMed]
- Schneider, M.M.; Nowak, T.E.; Bastian, L.; Katthagen, J.C.; Isenberg, J.; Rommens, P.M.; Müller, L.P.; Burkhart, K.J. Tension Band Wiring in Olecranon Fractures: The Myth of Technical Simplicity and Osteosynthetical Perfection. Int. Orthop. 2014, 38, 847–855. [Google Scholar] [CrossRef]
- Wilson, J.; Bajwa, A.; Kamath, V.; Rangan, A. Biomechanical Comparison of Interfragmentary Compression in Transverse Fractures of the Olecranon. J. Bone Jt. Surg. Br. 2011, 93-B, 245–250. [Google Scholar] [CrossRef]
- Matar, H.E.; Ali, A.A.; Buckley, S.; Garlick, N.I.; Atkinson, H.D. Surgical Interventions for Treating Fractures of the Olecranon in Adults. Cochrane Database Syst. Rev. 2014, CD010144. [Google Scholar] [CrossRef]
- Rantalaiho, I.K.; Miikkulainen, A.E.; Laaksonen, I.E.; Äärimaa, V.O.; Laimi, K.A. Treatment of Displaced Olecranon Fractures: A Systematic Review. Scand. J. Surg. 2021, 110, 13–21. [Google Scholar] [CrossRef]
- Hume, M.C.; Wiss, D.A. Olecranon Fractures. A Clinical and Radiographic Comparison of Tension Band Wiring and Plate Fixation. Clin. Orthop. Relat. Res. 1992, 285, 229–235. [Google Scholar] [CrossRef]
- Duckworth, A.D.; Clement, N.D.; White, T.O.; Court-Brown, C.M.; McQueen, M.M. Plate Versus Tension-Band Wire Fixation for Olecranon Fractures. J. Bone Jt. Surg. 2017, 99, 1261–1273. [Google Scholar] [CrossRef] [PubMed]
- Tarallo, L.; Mugnai, R.; Adani, R.; Capra, F.; Zambianchi, F.; Catani, F. Simple and Comminuted Displaced Olecranon Fractures: A Clinical Comparison between Tension Band Wiring and Plate Fixation Techniques. Arch. Orthop. Trauma. Surg. 2014, 134, 1107–1114. [Google Scholar] [CrossRef] [PubMed]
- DelSole, E.M.; Pean, C.A.; Tejwani, N.C.; Egol, K.A. Outcome after Olecranon Fracture Repair: Does Construct Type Matter? Eur. J. Orthop. Surg. Traumatol. 2016, 26, 153–159. [Google Scholar] [CrossRef] [PubMed]
- Claessen, F.M.A.P.; Braun, Y.; Peters, R.M.; Dyer, G.; Doornberg, J.N.; Ring, D. Factors Associated with Reoperation after Fixation of Displaced Olecranon Fractures. Clin. Orthop. Relat. Res. 2016, 474, 193–200. [Google Scholar] [CrossRef]
- Schliemann, B.; Raschke, M.J.; Groene, P.; Weimann, A.; Wähnert, D.; Lenschow, S.; Kösters, C. Comparison of Tension Band Wiring and Precontoured Locking Compression Plate Fixation in Mayo Type IIA Olecranon Fractures. Acta Orthop. Belg. 2014, 80, 106–111. [Google Scholar]
- Powell, A.J.; Farhan-Alanie, O.M.; McGraw, I.W.W. Tension Band Wiring versus Locking Plate Fixation for Simple, Two-Part Mayo 2A Olecranon Fractures: A Comparison of Post-Operative Outcomes, Complications, Reoperations and Economics. Musculoskelet. Surg. 2019, 103, 155–160. [Google Scholar] [CrossRef] [PubMed]
- Gathen, M.; Jaenisch, M.; Peez, C.; Weinhold, L.; Schmid, M.; Welle, K.; Burger, C.; Kabir, K. Plate Fixation and Tension Band Wiring after Isolated Olecranon Fracture Comparison of Outcome and Complications. J. Orthop. 2020, 18, 69–75. [Google Scholar] [CrossRef]
- Rantalaiho, I.K.; Laaksonen, I.E.; Ryösä, A.J.; Perkonoja, K.; Isotalo, K.J.; Äärimaa, V.O. Complications and Reoperations Related to Tension Band Wiring and Plate Osteosynthesis of Olecranon Fractures. J. Shoulder Elb. Surg. 2021, 30, 2412–2417. [Google Scholar] [CrossRef]
- Oputa, T.J.; Plastow, R.; Kennedy, J.; Jain, N.; Konarski, A.; Jump, C.; Manning, C.; Caruana, E.; Hodhody, G.; Riley, J.; et al. There Is No Difference in the Complication or Re-Operation Rates between Tension Band Wiring and Locking Plate Fixation for Olecranon Fractures. The Findings of a Multicentre Study. Arch. Orthop. Trauma. Surg. 2021, 142, 3341–3345. [Google Scholar] [CrossRef]
- Edwards, S.G.; Cohen, M.S.; Lattanza, L.L.; Iorio, M.L.; Daniels, C.; Lodha, S.; Smucny, M. Surgeon Perceptions and Patient Outcomes Regarding Proximal Ulna Fixation: A Multicenter Experience. J. Shoulder Elb. Surg. 2012, 21, 1637–1643. [Google Scholar] [CrossRef] [PubMed]
- Karlsson, M.K.; Hasserius, R.; Besjakov, J.; Karlsson, C.; Josefsson, P.O. Comparison of Tension-Band and Figure-of-Eight Wiring Techniques for Treatment of Olecranon Fractures. J. Shoulder Elb. Surg. 2002, 11, 377–382. [Google Scholar] [CrossRef] [PubMed]
- Macko, D.; Szabo, R.M. Complications of Tension-Band Wiring of Olecranon Fractures. J. Bone Joint Surg. Am. 1985, 67, 1396–1401. [Google Scholar] [CrossRef] [PubMed]
- Terstappen, A.L.E.; Joosse, P.; van Dijke, C.F.; Mirck, B.; van den Brand, J.G.H. Tension Band Wiring Provides Excellent Patient-Reported Long-Term Results for Both Comminuted and Simple Displaced Olecranon Fractures. J. Orthop. Trauma. 2020, 34, e239–e244. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Hospitalization (days) | Surgery Duration (min) | |||
|---|---|---|---|---|
| Mean ± 1 SD | Range | Mean ± 1 SD | Range | |
| TBW group | 8.6 ± 4.0 | 3–18 | 86.6 ± 30.9 | 40–165 |
| PF group | 9.5 ± 3.2 | 4–18 | 143.3 ± 61.3 | 60–260 |
| p value | 0.37 | 0.002 | ||
| Overall population | 9.3 ± 3.7 | 3–18 | 117.9 ± 59.1 | 40–260 |
| DASH | MEPS | pASES-e | ||||
|---|---|---|---|---|---|---|
| Mean ± 1 SD | Range | Mean ± 1 SD | Range | Mean ± 1 SD | Range | |
| TBW group | 14.5 ±17.2 | 0–22 | 80.5 ± 4.7 | 50–100 | 83.6 ± 12.4 | 55.8–97.2 |
| PF group | 21.0 ± 21.7 | 0–84.2 | 75.6 ± 5.3 | 45–100 | 75.1 ± 19.2 | 26.7–100 |
| p value | 0.16 | 0.17 | 0.003 | |||
| Overall population | 17.6 ± 9.6 | 0–84.2 | 78.2 ± 5.1 | 45–100 | 79.6 ± 16.4 | 26.7–100 |
| Range of Motion (°) | ||||
|---|---|---|---|---|
| Flexion | Extension | Pronation | Supination | |
| Mean ± 1 SD | Mean ± 1 SD | Mean ± 1 SD | Mean ± 1 SD | |
| TBW group | 138.02 ± 4.92 | 5.26 ± 22.3 | 67.89 ± 6.20 | 82.97 ± 5.60 |
| PF group | 138.2 ± 2.34 | 4.57 ± 21.13 | 68 ± 6.52 | 83.25 ± 5.02 |
| p value | 0.34 | 0.26 | 0.43 | 0.3 |
| Overall population | 138.10 ± 3.75 | 4.93 ± 21.75 | 67.94 ± 6.35 | 83.10 ± 5.32 |
| Metalwork Irritation | Nonunion | Implant Migration | Infection | Ulnar Neuropathy | Total Complications | |
|---|---|---|---|---|---|---|
| N (%) | N (%) | N (%) | N (%) | N (%) | N (%) | |
| TBW group | 6 (15.8) | 1 (2.6) | 1 (2.6) | 0 (0) | 0 (0) | 8 (21.2) |
| PF group | 1 (2.9) | 0 (0) | 0 (0) | 1 (2.9) | 1 (2.9) | 3 (8.8) |
| p value | 0.15 | |||||
| Overall population | 7 (9.8) | 1 (1.4) | 1 (1.4) | 1 (1.4) | 1 (1.4) | 11 (15.3) |
| Reoperations | Time Interval (months) | ||
|---|---|---|---|
| N (%) | Mean ± 1 SD | Range | |
| TBW group | 7 (18.4) | 11.4 ± 6.2 | 4–20 |
| PF group | 3 (8.8) | 14 ± 4.0 | 9–20 |
| p value | 0.24 | 0.57 | |
| Overall population | 10 (13.9) | 12.4 ± 5.7 | 4–20 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Giardina, S.M.C.; Testa, G.; Cuffaro, E.R.; Castiglione, M.D.; Sapienza, M.; Caldaci, A.; Cosentino, P.; Raffa, A.; Pavone, V. Surgical Treatment for Simple Isolated and Displaced Olecranon Fractures: Comparison between Plate and Tension Band Wire Fixation. J. Clin. Med. 2024, 13, 1815. https://doi.org/10.3390/jcm13061815
Giardina SMC, Testa G, Cuffaro ER, Castiglione MD, Sapienza M, Caldaci A, Cosentino P, Raffa A, Pavone V. Surgical Treatment for Simple Isolated and Displaced Olecranon Fractures: Comparison between Plate and Tension Band Wire Fixation. Journal of Clinical Medicine. 2024; 13(6):1815. https://doi.org/10.3390/jcm13061815
Chicago/Turabian StyleGiardina, Serena Maria Chiara, Gianluca Testa, Enrica Rosalia Cuffaro, Mirko Domenico Castiglione, Marco Sapienza, Alessia Caldaci, Pierluigi Cosentino, Angelo Raffa, and Vito Pavone. 2024. "Surgical Treatment for Simple Isolated and Displaced Olecranon Fractures: Comparison between Plate and Tension Band Wire Fixation" Journal of Clinical Medicine 13, no. 6: 1815. https://doi.org/10.3390/jcm13061815