


Novel Parameter in Pre-Surgical Orthodontic Preparation: A Retrospective Study on the Role of the Upper Incisor Position and a Morphological Evaluation of the Anterior Nasal Spine


Abstract
:1. Introduction
2. Materials and Methods
- -
- -
- (1)
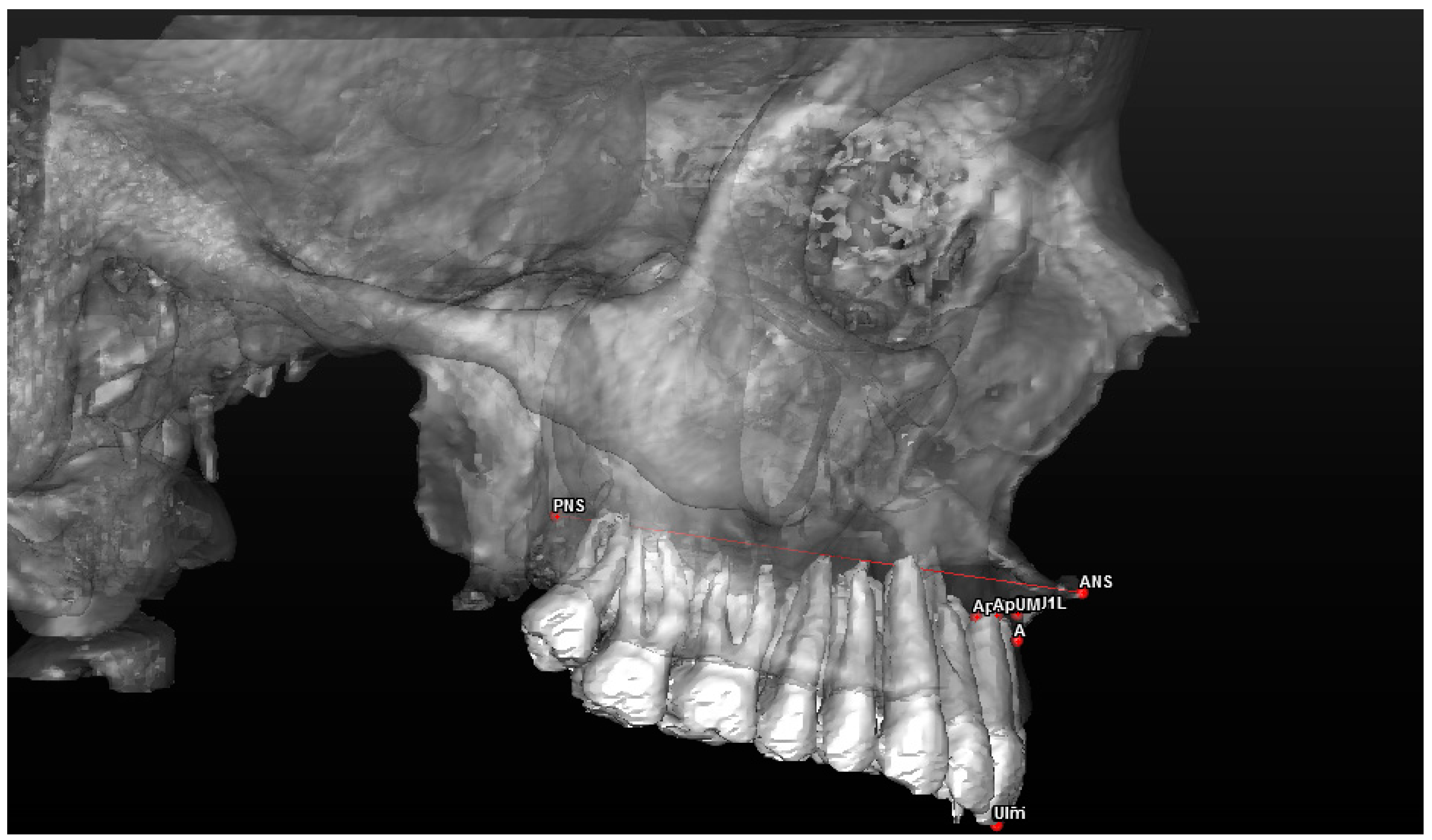
- Maxillary sagittal position (MX) and anterior nasal spine length (A-ATP) (distance) (Figure 5);
- (2)
- Spino-incisal angle (ANS–PNS to ApUM–Ulm) (angle) (Figure 6);
- (3)
- Position of the upper incisal margin (Ulm–ATP) (distance);
- (4)
- Nasolabial angle (Col–Sn–Ls) (angle) (Figure 7);
- (5)
- Upper lip height (Sn–Ls) (distance) (Figure 8);
- (6)
- Coronal lip thickness (BLs–Ulm) (distance) (Figure 9);
- (7)
- Apical lip thickness (A–A’p) (distance).
3. Results
3.1. Evaluation of the Position of the Upper Incisal Margin
3.2. Morphological Evaluation of the Anterior Nasal Spine
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Larson, B.E. Orthodontic preparation for orthognathic surgery. Oral Maxillofac. Surg. Clin. N. Am. 2014, 26, 441–458. [Google Scholar] [CrossRef] [PubMed]
- Sangalli, L.; Dalessandri, D.; Bonetti, S.; Mandelli, G.; Visconti, L.; Savoldi, F. Proposed parameters of optimal central incisor positioning in orthodontic treatment planning: A systematic review. Korean J. Orthod. 2022, 52, 53–65. [Google Scholar] [CrossRef]
- Wirthlin, J.O.; Shetye, P.R. Orthodontist’s Role in Orthognathic Surgery. Semin. Plast. Surg. 2013, 27, 137–144. [Google Scholar] [CrossRef] [PubMed]
- Quast, A.; Santander, P.; Leding, J.; Klenke, D.; Moser, N.; Schliephake, H.; Meyer-Marcotty, P. Orthodontic incisor decompensation in orthognathic therapy—Success and efficiency in three dimensions. Clin. Oral Investig. 2021, 25, 4001–4010. [Google Scholar] [CrossRef]
- McNeil, C.; McIntyre, G.T.; Laverick, S. How much incisor decompensation is achieved prior to orthognathic surgery? J. Clin. Exp. Dent. 2014, 6, e225–e229. [Google Scholar] [CrossRef] [PubMed]
- Troy, B.A.; Shanker, S.; Fields, H.W.; Vig, K.; Johnston, W. Comparison of incisor inclination in patients with Class III malocclusion treated with orthognathic surgery or orthodontic camouflage. Am. J. Orthod. Dentofac. Orthop. 2009, 135, 146.e1–149; discussion 146–147. [Google Scholar] [CrossRef]
- Gorbunkova, A.; Pagni, G.; Brizhak, A.; Farronato, G.; Rasperini, G. Impact of Orthodontic Treatment on Periodontal Tissues: A Narrative Review of Multidisciplinary Literature. Int. J. Dent. 2016, 2016, 4723589. [Google Scholar] [CrossRef] [PubMed]
- Park, J.H.; Hong, J.Y.; Ahn, H.W.; Kim, S.J. Correlation between periodontal soft tissue and hard tissue surrounding incisors in skeletal Class III patients. Angle Orthod. 2018, 88, 91–99. [Google Scholar] [CrossRef]
- Gotte, P.; Bertelè, G.P. Modulability of the surgical intervention to correct maxillofacial dysmorphism in light of new interpretive concepts of profile esthetics. Minerva Stomatol. 1984, 33, 703–721. [Google Scholar]
- Perrotti, G.; Testori, T.; Politi, M. 3D Imaging and Dentistry: From Multiplane Cephalometry to Guided Navigation in Implantology; Quintessenza Edizioni: Rho, Italy, 2016. [Google Scholar]
- Arnett, G.W.; Gunson, M.J. Facial planning for orthodontists and oral surgeons. Am. J. Orthod. Dentofac. Orthop. 2004, 126, 290–295. [Google Scholar] [CrossRef]
- Andrews, W.A. AP relationship of the maxillary central incisors to the forehead in adult white females. Angle Orthod. 2008, 78, 662–669. [Google Scholar] [CrossRef] [PubMed]
- Işiksal, E.; Hazar, S.; Akyalçin, S. Smile esthetics: Perception and comparison of treated and untreated smiles. Am. J. Orthod. Dentofac. Orthop. 2006, 129, 8–16. [Google Scholar] [CrossRef] [PubMed]
- Schabel, B.J.; McNamara, J.A.; Baccetti, T.; Franchi, L.; Jamieson, S.A. The relationship between posttreatment smile esthetics and the ABO Objective Grading System. Angle Orthod. 2008, 78, 579–584. [Google Scholar] [CrossRef] [PubMed]
- Singh, A.V.; Mahamuni, A.; Gaharwar, J.S.; Rai, R.; Yadav, K.; Sirishkusum, C. Evaluation of Change in the Facial Profile and Aesthetics in Relation to Incisor Position in Both Maxillary and Mandibular Arches. Cureus 2023, 15, e34403. [Google Scholar] [CrossRef] [PubMed]
- Fastuca, R.; Beccarini, T.; Rossi, O.; Zecca, P.A.; Caprioglio, A. Influence of facial components in class III malocclusion esthetic perception of orthodontists, patients, and laypersons. J. Orofac. Orthop. 2022, 83, 48–58. [Google Scholar] [CrossRef] [PubMed]
- Quinzi, V.; D’Andrea, N.; Albani, A.; Monaco, A.; Saccomanno, S. Evaluation of the Nasolabial Angle in Orthodontic Diagnosis: A Systematic Review. Appl. Sci. 2021, 11, 2531. [Google Scholar] [CrossRef]
- Naini, F.B.; Cobourne, M.T.; Garagiola, U.; McDonald, F.; Wertheim, D. Mentolabial angle and aesthetics: A quantitative investigation of idealized and normative values. Maxillofac. Plast. Reconstr. Surg. 2017, 39, 4. [Google Scholar] [CrossRef] [PubMed]
- Cao, L.; Zhang, K.; Bai, D.; Jing, Y.; Tian, Y.; Guo, Y. Effect of maxillary incisor labiolingual inclination and anteroposterior position on smiling profile esthetics. Angle Orthod. 2011, 81, 121–129. [Google Scholar] [CrossRef] [PubMed]
- Gioka, C.; Eliades, T. Materials-induced variation in the torque expression of preadjusted appliances. Am. J. Orthod. Dentofac. Orthop. 2004, 125, 323–328. [Google Scholar] [CrossRef]
- Cordato, M. Variation in torque expression. Am. J. Orthod. Dentofac. Orthop. 2004, 126, 18A, author reply 19A. [Google Scholar] [CrossRef]
- Patel, J.R.; Prajapati, P.; Sethuraman, R.; Naveen, Y.G. A comparative evaluation of effect of upper lip length, age and sex on amount of exposure of maxillary anterior teeth. J. Contemp. Dent. Pract. 2011, 12, 24–29. [Google Scholar] [CrossRef] [PubMed]
- Hussels, W.; Nanda, R.S. Analysis of factors affecting angle ANB. Am. J. Orthod. 1984, 85, 411–423. [Google Scholar] [CrossRef] [PubMed]
- Binder, R.E. The geometry of cephalometrics. J. Clin. Orthod. 1979, 13, 258–263. [Google Scholar] [PubMed]
- Jacobson, A. The “Wits” appraisal of jaw disharmony. Am. J. Orthod. 1975, 67, 125–138. [Google Scholar] [CrossRef] [PubMed]
- Enlow, D.H. Facial growth and development. Int. J. Orofac. Myol. 1979, 5, 7–10. [Google Scholar] [CrossRef]
- Schlosser, J.B.; Preston, C.B.; Lampasso, J. The effects of computer-aided anteroposterior maxillary incisor movement on ratings of facial attractiveness. Am. J. Orthod. Dentofac. Orthop. 2005, 127, 17–24. [Google Scholar] [CrossRef] [PubMed]
- Arnett, G.W.; Jelic, J.S.; Kim, J.; Cummings, D.R.; Beress, A.; Worley, C.M.; Chung, B.; Bergman, R. Soft tissue cephalometric analysis: Diagnosis and treatment planning of dentofacial deformity. Am. J. Orthod. Dentofac. Orthop. 1999, 116, 239–253. [Google Scholar] [CrossRef]
- Cevidanes, L.; Oliveira, A.E.; Motta, A.; Phillips, C.; Burke, B.; Tyndall, D. Head orientation in CBCT-generated cephalograms. Angle Orthod. 2009, 79, 971–977. [Google Scholar] [CrossRef]










{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Point | Definition | |
|---|---|---|
| Dental | U11 | Midpoint of the incisal margin of the right central incisor |
| ApU1R | Apex of the right central incisor | |
| U21 | Midpoint of the incisal margin of the left central incisor | |
| ApU1L | Apex of the left central incisor | |
| Skeletal | Point A | Backward point in the concavity of the upper maxilla between the ANS and the alveolar crest |
| ANS (Anterior Nasal Spine) | Most advanced point in the profile of the upper maxilla at the level of the median palatine suture | |
| PNS (Posterior Nasal Spine) | Posterior and median point in the upper maxilla |
| Point | Definition |
|---|---|
| Ls (Upper Labial) | Midpoint protruding more anteriorly than the upper labial vermilion |
| Sn (Subnasal) | Cutaneous midpoint of the encounter between the columella and the upper lip |
| Col (Columella) | Highest cutaneous midpoint of the columella at the meeting level between the nostrils |
| BLs (Back Edge of the Upper Lip) | Posterior–inferior point in the upper lip at the level of the incisal margin |
| A* | Cutaneous point of the corresponding subspinal point A |
| Measurement | Unit | Values Considered the “Norm” | Description | |
|---|---|---|---|---|
| Skeletal | A–ATP (maxillary sagittal position = anterior nasal spine length) | Mm | 3.2–6 | Distance between the anterior facial plane and point A |
| Dental | ANS–PNS/ApUM–Ulm (spino-incisal angle) | Degrees | 110 ± 5 | Angle between the spinal axis and incisal axis |
| Ulm–ATP (position of the upper incisal margin) | Mm | To search | Distance between the Ulm and the anterior facial plane | |
| Soft tissue | Col–Sn–Ls (nasolabial angle) | Degrees | U 98.7–114.1 F 96.7–110.3 | Angle between points columella–subnasal–upper labial |
| Sn–Ls (lip height) | Mm | 19–22 | Distance between point Sn and Ls | |
| BLs–Ulm (coronal lip thickness) | Mm | U13.4–16.2 D10.8–14.4 | Distance between BLs and Ulm | |
| A–A’p (apical lip thickness) | Mm | 14–16 | Distance between A and A*p |
| Measurement | Values Obtained | Standard Values |
|---|---|---|
| Maxillary position | M 4.69 ± 0.55 mm F 4.73 ± 0.82 mm | Intermediate 3.2–4 mm Mixed 4–6 mm |
| Spino-incisal angle | M 109.9° ± 3.55° F 109.26° ± 3.37° | 110° ± 5° |
| Position of the upper incisal margin | M 0.16 ± 0.65 mm F 0.1 ± 0.5 mm | - |
| Nasolabial angle | M 104.94° ± 3.64° F 105.32° ± 3.6° | M 98.7°–114.1° F 96.7°–110.3° |
| Upper lip height | M 14.98 ± 2.53 mm F 14.71 ± 2.67 mm | 19–22 mm |
| Coronal lip thickness | M 10.99 ± 2.24 mm F 9.34 ± 2.07 mm | M 13.4–16.2 mm F 10.8–14.4 mm |
| Apical lip thickness | M 14.53 ± 1.75 mm F 13.21 ± 2.02 mm | 14–16 mm |
| Patient (Male Sample) | 1 | 2 | 3 | 4 | 5 | 6 | 7 |
|---|---|---|---|---|---|---|---|
| MX o A–ATP | ANSPNS su ApUM–Ulm | Ulm–ATP | Col–Sn–Ls | Sn–Ls | Bls–Ulm | A–A’p | |
| 1 | 5.06 | 113.62 | 0.16 | 102.15 | 14.14 | 12.23 | 16.34 |
| 2 | 4.59 | 107.59 | 0.75 | 104.33 | 20.44 | 9.92 | 15.46 |
| 3 | 5.67 | 104.62 | 1.6 | 98.47 | 10.07 | 10 | 13.28 |
| 4 | 4.16 | 111.1 | 0.32 | 110.81 | 15.7 | 10.15 | 12.23 |
| 5 | 4.33 | 105.81 | 0.43 | 109.94 | 11.97 | 9.93 | 13.75 |
| 6 | 4.23 | 107.65 | −0.41 | 107.81 | 14.92 | 11.15 | 13.53 |
| 7 | 4.23 | 108.7 | 0.11 | 103.55 | 16.04 | 14.81 | 16.16 |
| 8 | 4.13 | 105.65 | 0.28 | 101.37 | 13.94 | 12.88 | 14.58 |
| 9 | 4.1 | 113.35 | 0.06 | 106.7 | 12.37 | 13.74 | 16.24 |
| 10 | 4.22 | 107.89 | 0.6 | 101.37 | 20.89 | 14.46 | 16.27 |
| 11 | 4.9 | 114.73 | 0.34 | 99.95 | 14.3 | 9.17 | 14.87 |
| 12 | 5.24 | 112.26 | 0.15 | 111.15 | 15.19 | 7.57 | 13.97 |
| 13 | 4.9 | 111.32 | 0.5 | 103.1 | 17.1 | 6 | 10.64 |
| 14 | 5.24 | 110.73 | 0.16 | 108.71 | 17.03 | 12.75 | 14.4 |
| 15 | 4.91 | 107.03 | 0.95 | 103.24 | 17.7 | 15.45 | 15.09 |
| 16 | 5.07 | 111.22 | 0.06 | 107.7 | 12.09 | 9.98 | 17.58 |
| 17 | 4.01 | 112.32 | 0.14 | 102.58 | 12.59 | 10.5 | 13.09 |
| 18 | 5.34 | 105.31 | −1.75 | 105.17 | 12.48 | 11.93 | 17.65 |
| 19 | 4.15 | 113.41 | 0.23 | 108.3 | 16.52 | 12.1 | 15.13 |
| 20 | 3.96 | 114.9 | −0.47 | 101.48 | 12.94 | 9.9 | 14.25 |
| 21 | 5.2 | 112.31 | −0.89 | 101.24 | 12.29 | 9.91 | 14.9 |
| 22 | 4.77 | 104 | 0.4 | 107.6 | 9.01 | 11.66 | 14.65 |
| 23 | 5.79 | 100.07 | 0.36 | 103.4 | 11.57 | 13.5 | 12.11 |
| 24 | 4.85 | 109.87 | 0.84 | 115 | 9.09 | 12.72 | 13.3 |
| 25 | 4.43 | 103.47 | −0.58 | 104.73 | 10.49 | 15.85 | 16.85 |
| Patient (Female Sample) | 1 | 2 | 3 | 4 | 5 | 6 | 7 |
|---|---|---|---|---|---|---|---|
| MX o A–ATP | ANSPNS su ApUM–Ulm | Ulm–ATP | Col–Sn–Ls | Sn–Ls | Bls–Ulm | A–A’p | |
| 1 | 4.85 | 110.67 | 0.64 | 109.3 | 15.69 | 9.75 | 14.18 |
| 2 | 5.15 | 105 | 0.01 | 104.03 | 14.96 | 13.31 | 13.44 |
| 3 | 4.11 | 106.13 | −0.11 | 108.03 | 17.46 | 7.9 | 13.19 |
| 4 | 5.83 | 109.6 | 0.18 | 104.72 | 15.73 | 7.59 | 11.92 |
| 5 | 4.66 | 111.95 | −0.8 | 104.59 | 11.17 | 9.18 | 8.48 |
| 6 | 4.01 | 110.05 | 0.32 | 103.69 | 14.07 | 11.19 | 14.68 |
| 7 | 4.02 | 105.81 | 0.78 | 100.7 | 14.98 | 11.31 | 14.13 |
| 8 | 4.44 | 106.65 | 0.19 | 109 | 16.65 | 8.57 | 13.35 |
| 9 | 4.05 | 114.96 | −0.55 | 100.51 | 16.09 | 11 | 14.14 |
| 10 | 6 | 112.06 | 0.71 | 106.47 | 21.55 | 12.25 | 16.61 |
| 11 | 4.22 | 105.97 | −0.66 | 107.6 | 15.6 | 6.51 | 13 |
| 12 | 4.66 | 113.26 | 0.4 | 109.53 | 14.12 | 10.84 | 13.39 |
| 13 | 6 | 110.7 | 0.07 | 102.67 | 14.42 | 8.82 | 14 |
| 14 | 4.99 | 109.78 | 0.33 | 110 | 14.01 | 9.01 | 12.8 |
| 15 | 3.29 | 108.82 | 0.03 | 103.44 | 9.54 | 9.54 | 14.64 |
| 16 | 3.82 | 108.28 | 0.22 | 103.52 | 15.99 | 7.62 | 10.95 |
| 17 | 5.98 | 107.77 | −0.22 | 102.63 | 10.89 | 7.76 | 11.51 |
| 18 | 3.71 | 105.7 | 0.4 | 110.2 | 12.03 | 7.66 | 10.98 |
| 19 | 4.9 | 107.62 | −0.79 | 107.88 | 11.47 | 5.18 | 12.03 |
| 20 | 4.13 | 113.93 | −0.6 | 97.59 | 16.69 | 13.63 | 17.54 |
| 21 | 4.37 | 105.78 | 0.68 | 102.53 | 13.97 | 10.1 | 12.28 |
| 22 | 4.07 | 109.92 | 0.89 | 106 | 10.79 | 11.5 | 15 |
| 23 | 5.32 | 104.02 | −0.38 | 115 | 7.15 | 12.18 | 12.76 |
| 24 | 5.9 | 110.02 | 0.19 | 105 | 12.68 | 15.92 | 19.57 |
| 25 | 5.76 | 100.93 | 0.52 | 114.95 | 10.19 | 14.47 | 13.34 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rossi, O.; Perrotti, G.; Del Fabbro, M.; Testori, T. Novel Parameter in Pre-Surgical Orthodontic Preparation: A Retrospective Study on the Role of the Upper Incisor Position and a Morphological Evaluation of the Anterior Nasal Spine. J. Clin. Med. 2024, 13, 2346. https://doi.org/10.3390/jcm13082346
Rossi O, Perrotti G, Del Fabbro M, Testori T. Novel Parameter in Pre-Surgical Orthodontic Preparation: A Retrospective Study on the Role of the Upper Incisor Position and a Morphological Evaluation of the Anterior Nasal Spine. Journal of Clinical Medicine. 2024; 13(8):2346. https://doi.org/10.3390/jcm13082346
Chicago/Turabian StyleRossi, Ornella, Giovanna Perrotti, Massimo Del Fabbro, and Tiziano Testori. 2024. "Novel Parameter in Pre-Surgical Orthodontic Preparation: A Retrospective Study on the Role of the Upper Incisor Position and a Morphological Evaluation of the Anterior Nasal Spine" Journal of Clinical Medicine 13, no. 8: 2346. https://doi.org/10.3390/jcm13082346