
Elevated Colon Cancer Rates Linked to Prior Appendicitis: A Retrospective Cohort Study Based on Data from German General Practices

 , , and
, , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Database
2.2. Study Population
3. Results
3.1. Basic Characteristics of the Study Sample
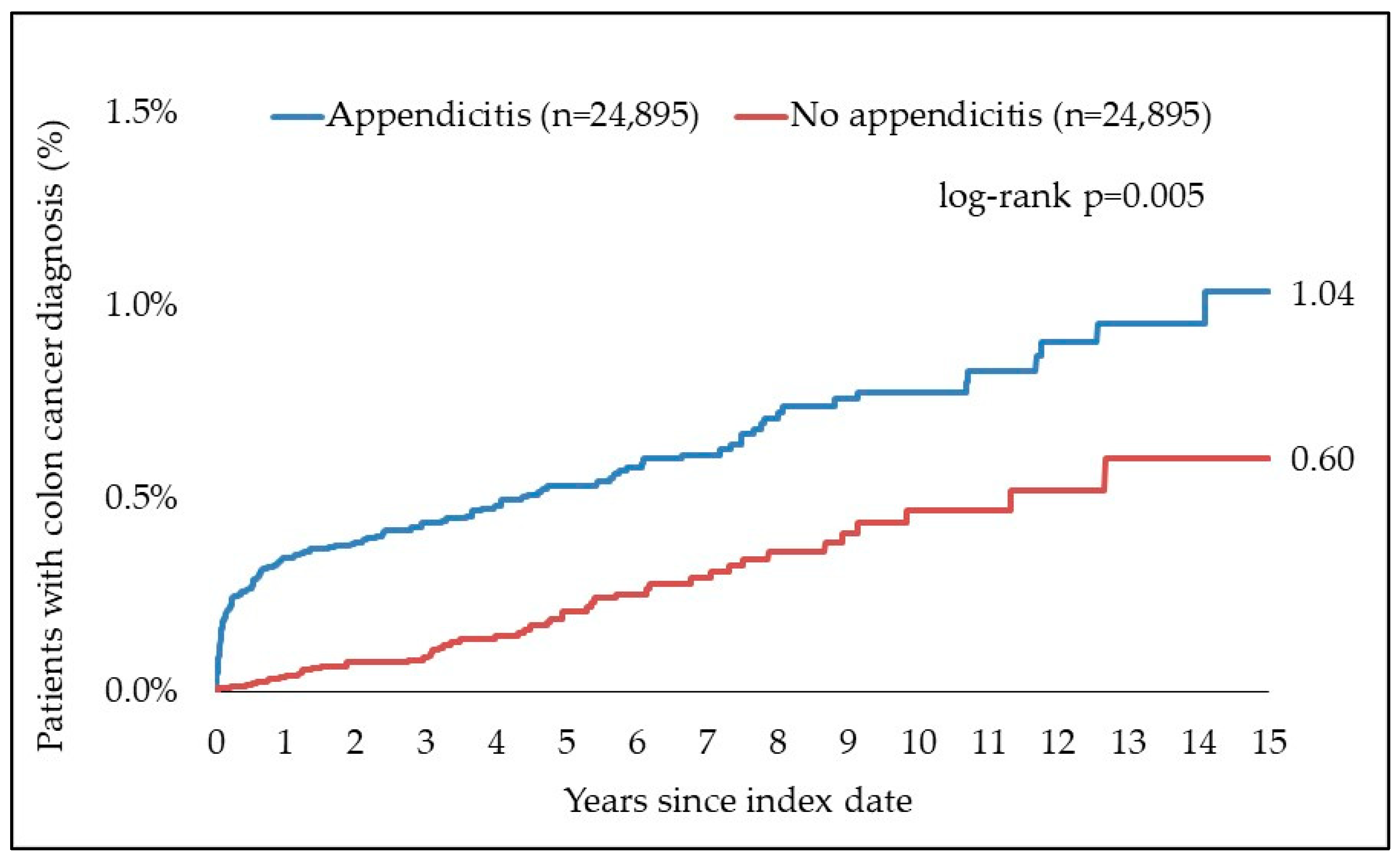
3.2. Association between Appendicitis and Subsequent Colon Cancer Diagnosis
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Butler, C. Surgical pathology of acute appendicitis. Hum. Pathol. 1981, 12, 870–878. [Google Scholar] [CrossRef] [PubMed]
- Acute Appendicitis in Adults: Clinical Manifestations and Differential Diagnosis—UpToDate. Available online: https://www.uptodate.com/contents/acute-appendicitis-in-adults-clinical-manifestations-and-differential-diagnosis?search=ursachen%20Apeendizitis&source=search_result&selectedTitle=1~150&usage_type=default&display_rank=1 (accessed on 7 September 2023).
- Gaetke-Udager, K.; Maturen, K.E.; Hammer, S.G. Beyond acute appendicitis: Imaging and pathologic spectrum of appendiceal pathology. Emerg. Radiol. 2014, 21, 535–542. [Google Scholar] [CrossRef] [PubMed]
- Entstehung Kolorektaler Karzinome. Available online: https://www.aerzteblatt.de/archiv/78907/Entstehung-kolorektaler-Karzinome (accessed on 14 April 2024).
- Weitz, J.; Koch, M.; Debus, J.; Höhler, T.; Galle, P.R.; Büchler, M.W. Colorectal cancer. Lancet 2005, 365, 153–165. [Google Scholar] [CrossRef] [PubMed]
- Bonnet, M.; Buc, E.; Sauvanet, P.; Darcha, C.; Dubois, D.; Pereira, B.; Déchelotte, P.; Bonnet, R.; Pezet, D.; Darfeuille-Michaud, A. Colonization of the Human Gut by E. coli and Colorectal Cancer Risk. Clin. Cancer Res. 2014, 20, 859–867. [Google Scholar] [CrossRef]
- Hossain, M.S.; Karuniawati, H.; Jairoun, A.A.; Urbi, Z.; Ooi, D.J.; John, A.; Lim, Y.C.; Kibria, K.M.K.; Mohiuddin, A.K.M.; Ming, L.C.; et al. Colorectal Cancer: A Review of Carcinogenesis, Global Epidemiology, Current Challenges, Risk Factors, Preventive and Treatment Strategies. Cancers 2022, 14, 1732. [Google Scholar] [CrossRef]
- Colorectal Cancer: Epidemiology, Risk Factors, and Protective Factors—UpToDate. Available online: https://www.uptodate.com/contents/colorectal-cancer-epidemiology-risk-factors-and-protective-factors?search=inzidenz%20von%20Kolonkarzinomen&source=search_result&selectedTitle=1~150&usage_type=default&display_rank=1 (accessed on 7 September 2023).
- Clay, S.L.; Fonseca-Pereira, D.; Garrett, W.S. Colorectal cancer: The facts in the case of the microbiota. J. Clin. Investig. 2022, 132, e155101. [Google Scholar] [CrossRef]
- Vitetta, L.; Chen, J.; Clarke, S. The vermiform appendix: An immunological organ sustaining a microbiome inoculum. Clin. Sci. 2019, 133, 1–8. [Google Scholar] [CrossRef]
- Imperiale, T.F.; Glowinski, E.A.; Lin-Cooper, C.; Larkin, G.N.; Rogge, J.D.; Ransohoff, D.F. Five-Year Risk of Colorectal Neoplasia after Negative Screening Colonoscopy. N. Engl. J. Med. 2008, 359, 1218–1224. [Google Scholar] [CrossRef]
- Statistisches Bundesamt Deutschland—GENESIS-Online: Ergebnis K35, K36, K37 [Internet]. Available online: https://www-genesis.destatis.de/genesis/online?operation=abruftabelleBearbeiten&levelindex=1&levelid=1694159053186&auswahloperation=abruftabelleAuspraegungAuswaehlen&auswahlverzeichnis=ordnungsstruktur&auswahlziel=werteabruf&code=23131-0001&auswahltext=&nummer=3&variable=3&name=GES025&werteabruf=Werteabruf#abreadcrumb (accessed on 8 September 2023).
- Statistisches Bundesamt Deutschland—GENESIS-Online: Ergebnis C18 [Internet]. Available online: https://www-genesis.destatis.de/genesis/online?operation=abruftabelleBearbeiten&levelindex=1&levelid=1694176726513&auswahloperation=abruftabelleAuspraegungAuswaehlen&auswahlverzeichnis=ordnungsstruktur&auswahlziel=werteabruf&code=23131-0001&auswahltext=&nummer=3&variable=3&name=GES025&werteabruf=Werteabruf#abreadcrumb (accessed on 8 September 2023).
- Lai, H.W.; Loong, C.C.; Tai, L.C.; Wu, C.W.; Lui, W.Y. Incidence and odds ratio of appendicitis as first manifestation of colon cancer: A retrospective analysis of 1873 patients. J. Gastroenterol. Hepatol. 2006, 21, 1693–1696. [Google Scholar] [CrossRef]
- Mohamed, I.; Chan, S.; Bhangu, A.; Karandikar, S. Appendicitis as a manifestation of colon cancer: Should we image the colon after appendicectomy in patients over the age of 40 years? Int. J. Color. Dis. 2019, 34, 527–531. [Google Scholar] [CrossRef]
- Shine, R.J.; Zarifeh, A.; Frampton, C.; Rossaak, J. Appendicitis presenting as the first manifestation of colorectal carcinoma: A 13-year retrospective study. N. Z. Med. J. 2017, 130, 25–32. [Google Scholar] [PubMed]
- Rajebhosale, R.P.; Robinson, N.M.; Kader, N.A.; Ratnayake, I.C.; Sawant, M.H.; Halahakoon, V.C. Is It Worth Considering Colonic Evaluation after Appendicectomy? Cureus. 9 August 2023. Available online: https://www.cureus.com/articles/156159-is-it-worth-considering-colonic-evaluation-after-appendicectomy (accessed on 6 September 2023).
- Andric, M.; Kalff, J.C.; Schwenk, W.; Farkas, S.; Hartwig, W.; Türler, A.; Croner, R. Empfehlungen zur Therapie der akuten Appendizitis: Empfehlungen einer Expertengruppe vor dem Hintergrund der aktuellen Literatur. Die Chir. 2020, 91, 700–711. [Google Scholar] [CrossRef] [PubMed]
- Hajibandeh, S.; Hajibandeh, S.; Morgan, R.; Maw, A. The incidence of right-sided colon cancer in patients aged over 40 years with acute appendicitis: A systematic review and meta-analysis. Int. J. Surg. Lond. Engl. 2020, 79, 1–5. [Google Scholar] [CrossRef] [PubMed]
- Viennet, M.; Tapia, S.; Cottenet, J.; Bernard, A.; Ortega-Deballon, P.; Quantin, C. Increased risk of colon cancer after acute appendicitis: A nationwide, population-based study. Eclinicalmedicine 2023, 63, 102196. [Google Scholar] [CrossRef] [PubMed]
- Jolly, S.; McCullough, T.; Gunning, T.; Maddern, G.; Wichmann, M. The role of screening colonoscopy after appendicitis in patients over 40 years of age. ANZ J. Surg. 2023, 93, 602–605. [Google Scholar] [CrossRef] [PubMed]
- Rathmann, W.; Bongaerts, B.; Carius, H.J.; Kruppert, S.; Kostev, K. Basic characteristics and representativeness of the German Disease Analyzer database. Int. J. Clin. Pharmacol. Ther. 2018, 56, 459–466. [Google Scholar] [CrossRef] [PubMed]
- About IQVIA. Available online: https://www.iqvia.com/about-us (accessed on 12 April 2024).
- Loosen, S.H.; Schöler, D.; Labuhn, S.; Mertens, A.; Jördens, M.S.; Luedde, M.; Kostev, K.; Luedde, T.; Roderburg, C. The Spectrum of Co-Diagnoses in Patients with Colorectal Cancer: A Retrospective Cohort Study of 17,824 Outpatients in Germany. Cancers 2022, 14, 3825. [Google Scholar] [CrossRef] [PubMed]
- Roderburg, C.; Loosen, S.H.; Hippe, H.; Luedde, T.; Kostev, K.; Luedde, M. Pulmonary hypertension is associated with an increased incidence of cancer diagnoses. Pulm. Circ. 2021, 12, e12000. Available online: https://onlinelibrary.wiley.com/doi/10.1002/pul2.12000 (accessed on 24 July 2023). [CrossRef]
- Quan, H.; Sundararajan, V.; Halfon, P.; Fong, A.; Burnand, B.; Luthi, J.-C.; Saunders, L.D.; Beck, C.A.; Feasby, T.E.; Ghali, W.A. Coding Algorithms for Defining Comorbidities in ICD-9-CM and ICD-10 Administrative Data. Med. Care 2005, 43, 1130–1139. [Google Scholar] [CrossRef]
- Van de Moortele, M.; De Hertogh, G.; Sagaert, X.; Van Cutsem, E. Appendiceal cancer: A review of the literature. Acta Gastro-Enterol. Belg. 2020, 83, 441–448. [Google Scholar]
- Fabri, P.J.; Carey, L.C. Cecal Carcinoma Presenting as Acute Appendicitis: A Reappraisal. J. Clin. Gastroenterol. 1980, 2, 173–174. [Google Scholar] [CrossRef] [PubMed]
- Weil Früher Besser Ist—Die Wichtigsten Fragen zur Darmkrebs-Vorsorge. Available online: https://www.bundesgesundheitsministerium.de/themen/praevention/frueherkennung-vorsorge/fragen-zur-darmkrebs-vorsorge.html (accessed on 17 September 2023).
- Girard-Madoux, M.J.H.; de Agüero, M.G.; Ganal-Vonarburg, S.C.; Mooser, C.; Belz, G.T.; Macpherson, A.J.; Vivier, E. The immunological functions of the Appendix: An example of redundancy? Semin. Immunol. 2018, 36, 31–44. [Google Scholar] [CrossRef]
- Wu, S.C.; Chen, W.T.L.; Muo, C.H.; Ke, T.W.; Fang, C.W.; Sung, F.C. Association between Appendectomy and Subsequent Colorectal Cancer Development: An Asian Population Study. Delmas D, editor. PLoS ONE 2015, 10, e0118411. [Google Scholar] [CrossRef] [PubMed]
- Arnbjörnsson, E. Acute appendicitis as a sign of a colorectal carcinoma. J. Surg. Oncol. 1982, 20, 17–20. [Google Scholar] [CrossRef] [PubMed]
- Dhadlie, S.; Mehanna, D. Rates of colorectal cancer detection in screening colonoscopy post appendicectomy in patients 50 years and over. Ann. Med. Surg. 2018, 36, 239–241. [Google Scholar] [CrossRef] [PubMed]
- Seretis, C.; Gill, J.; Lim, P.; Archer, L.; Seretis, F.; Yahia, S. Surveillance Colonoscopy after Appendicectomy in Patients over the Age of 40: Targeted Audit of Outcomes and Variability in Practice. Chirurgia 2020, 115, 595–599. [Google Scholar] [CrossRef] [PubMed]
- Bizer, L.S. Acute appendicitis is rarely the initial presentation of cecal cancer in the elderly patient. J. Surg. Oncol. 1993, 54, 45–46. [Google Scholar] [CrossRef]
- Khan, S.A.; Khokhar, H.A.; Nasr, A.R.H.; Carton, E. Incidence of right-sided colonic tumors (non-appendiceal) in patient’s ≥40 years of age presenting with features of acute appendicitis. Int. J. Surg. 2013, 11, 301–304. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Variable | Proportion among Appendicitis Patients (N, %) N = 24,895 | Proportion among Non-Appendicitis Patients (N, %) N = 24,895 | p-Value |
|---|---|---|---|
| Age (Mean, SD) | 41.0 (17.7) | 41.0 (17.7) | 1.000 |
| Age 18–30 | 9134 (36.7) | 9134 (36.7) | 1.000 |
| Age 31–40 | 4332 (17.4) | 4332 (17.4) | |
| Age 41–50 | 3930 (15.8) | 3930 (15.8) | |
| Age 51–60 | 3555 (14.3) | 3555 (14.3) | |
| Age > 60 | 3944 (15.8) | 3944 (15.8) | |
| Female | 13,846 (55.6) | 13,846 (55.6) | 1.000 |
| Male | 11,049 (44.4) | 11,049 (44.4) | |
| Number of physician visits per year during the follow-up (Mean, SD) | 6.0 (3.8) | 6.0 (3.8) | 1.000 |
| Charlson Comorbidity Score (CCS) | 1.0 (1.4) | 1.0 (1.4) | 1.000 |
| CCS 0 | 11,118 (44.7) | 11,118 (44.7) | 1.000 |
| CCS 1 | 7733 (31.1) | 7733 (31.1) | |
| CCS 2 | 3104 (12.5) | 3104 (12.5) | |
| CCS 3 | 1474 (5.9) | 1474 (5.9) | |
| CCS > 3 | 1466 (5.9) | 1466 (5.9) | |
| Index year 2005–2008 | 2595 (10.4) | 2595 (10.4) | 1.000 |
| Index year 2009–2012 | 4604 (18.5) | 4604 (18.5) | |
| Index year 2013–2016 | 6725 (27.0) | 6725 (27.0) | |
| Index year 2017–2021 | 10,971 (44.1) | 10,971 (44.1) |
| Time to Cancer Diagnosis | N | % |
|---|---|---|
| ≤6 months | 71 | 36.4% |
| 7–12 months | 25 | 12.8% |
| 13–24 months | 16 | 8.2% |
| 25–36 months | 11 | 5.6% |
| 37–60 months | 29 | 14.9% |
| 61–120 months | 34 | 17.4% |
| >120 months | 9 | 4.6% |
| Total | 195 |
| Time to Cancer Diagnosis | N | % |
|---|---|---|
| 7–12 months | 25 | 20.2% |
| 13–24 months | 16 | 12.9% |
| 25–36 months | 11 | 8.9% |
| 37–60 months | 29 | 23.4% |
| 61–120 months | 34 | 27.4% |
| >120 months | 9 | 7.3% |
| Total | 124 |
| Colon Cancer (Diagnoses Starting from Day 1 after Index Date) | Colon Cancer (Excluding Cases Documented within 3 Months after the Index Date) | Colon Cancer (Excluding Cases Documented within 6 Months after the Index Date) | ||||
|---|---|---|---|---|---|---|
| Subcohort | HR (95% CI) | p-Value | HR (95% CI) | p-Value | HR (95% CI) | p-Value |
| Total | 2.51 (1.83–3.45) | <0.001 | 1.45 (1.02–2.07) | 0.039 | 1.34 (0.93–1.93) | 0.111 |
| Age 18–30 | 8.17 (1.03–64.58) | 0.046 | 5.21 (0.63–43.32) | 0.127 | 4.23 (0.49–36.30) | 0.188 |
| Age 31–40 | 3.77 (0.80–17.81) | 0.093 | 1.33 (0.22–7.98) | 0.759 | 1.32 (0.21–7.97) | 0.759 |
| Age 41–50 | 10.30 (2.42–43.82) | 0.002 | 5.34 (1.19–23.86) | 0.029 | 4.36 (0.95–19.90) | 0.058 |
| Age 51–60 | 1.61 (0.90–2.88) | 0.108 | 0.85 (0.43–1.68) | 0.640 | 0.84 (0.42–1.70) | 0.628 |
| Age > 60 | 2.24 (1.46–3.45) | <0.001 | 1.41 (0.87–2.27) | 0.164 | 1.30 (0.80–2.11) | 0.288 |
| Female | 1.91 (1.26–2.89) | 0.002 | 0.97 (0.59–1.59) | 0.912 | 0.85 (0.51–1.41) | 0.527 |
| Male | 3.56 (2.15–5.89) | <0.001 | 2.22 (1.30–3.78) | 0.003 | 2.18 (1.26–3.77) | 0.005 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Steffes, S.; Kostev, K.; Schattenberg, J.M.; Heinzow, H.S.; Maschmeier, M. Elevated Colon Cancer Rates Linked to Prior Appendicitis: A Retrospective Cohort Study Based on Data from German General Practices. J. Clin. Med. 2024, 13, 2342. https://doi.org/10.3390/jcm13082342
Steffes S, Kostev K, Schattenberg JM, Heinzow HS, Maschmeier M. Elevated Colon Cancer Rates Linked to Prior Appendicitis: A Retrospective Cohort Study Based on Data from German General Practices. Journal of Clinical Medicine. 2024; 13(8):2342. https://doi.org/10.3390/jcm13082342
Chicago/Turabian StyleSteffes, Susann, Karel Kostev, Jörn M. Schattenberg, Hauke S. Heinzow, and Miriam Maschmeier. 2024. "Elevated Colon Cancer Rates Linked to Prior Appendicitis: A Retrospective Cohort Study Based on Data from German General Practices" Journal of Clinical Medicine 13, no. 8: 2342. https://doi.org/10.3390/jcm13082342