
Athlete Fear Avoidance, Depression, and Anxiety Are Associated with Acute Concussion Symptoms in Athletes


Abstract
:1. Introduction
2. Materials and Methods
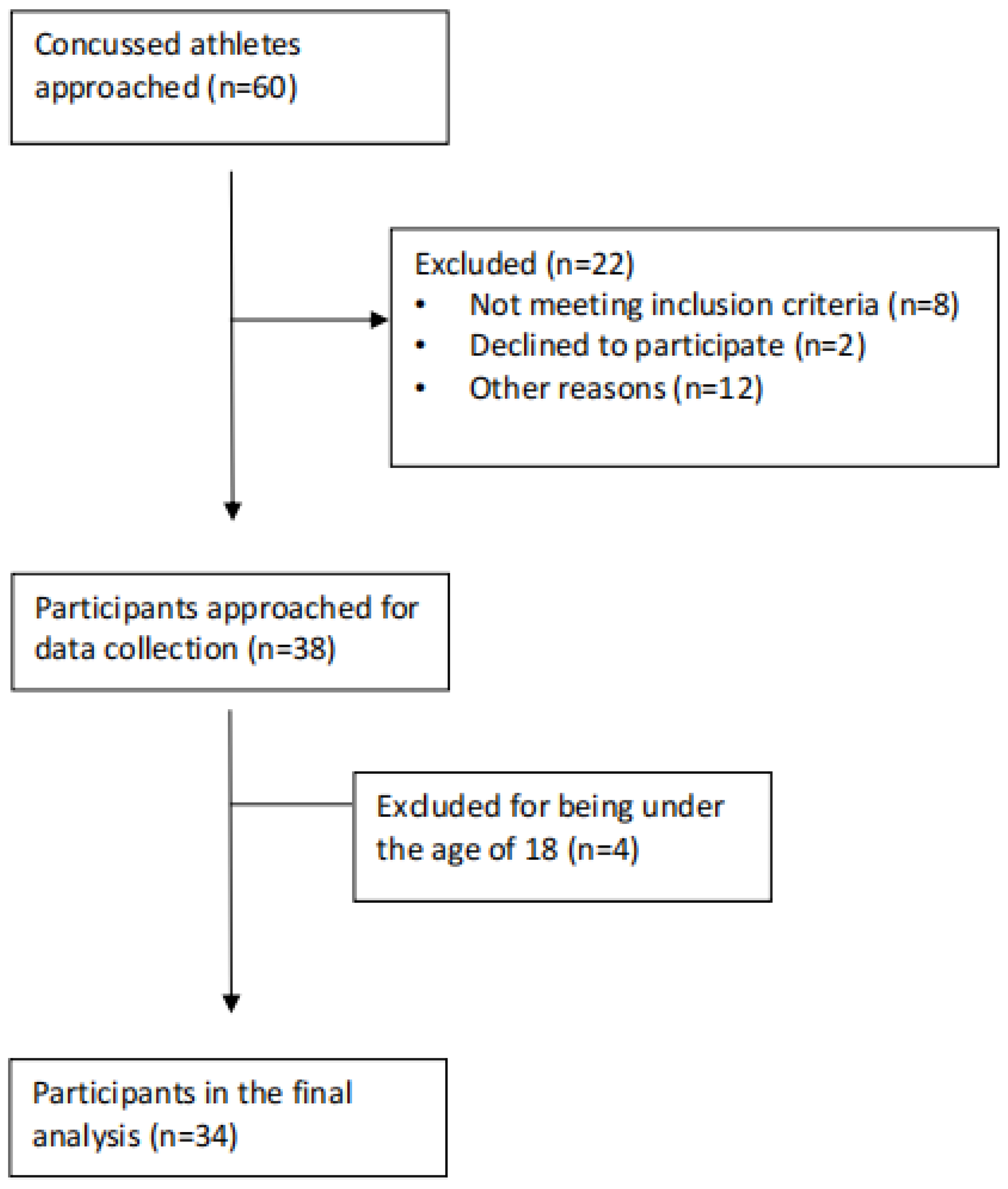
2.1. Participants
2.2. Tools
2.2.1. Sport Concussion Assessment Tool 5
2.2.2. Athlete Fear Avoidance Questionnaire
2.2.3. Pain Catastrophizing Scale
2.2.4. Tampa Scale of Kinesiophobia
2.2.5. Hospital Anxiety and Depression Scale
2.2.6. 36-Item Short Form
2.3. Procedures
2.4. Statistical Analysis
3. Results
3.1. Participants
3.2. Relationship between SCAT5 and Psychological Variables
3.2.1. Total Number of Symptoms and Symptom Severity Score on the SCAT5 and Fear Avoidance
3.2.2. Total Number of Symptoms and Symptom Severity Score on the SCAT5 and Anxiety and Depression
3.2.3. Total Number of Symptoms and Symptom Severity Score on the SCAT5 and Mental Health Pre-Concussion
3.2.4. Significant Predictors of Symptom Number and Symptom Severity on the SCAT5
4. Discussion
4.1. Total Number of Symptoms and Symptom Severity Score on the SCAT5 and Pain-Related Fear
4.2. Relationship between Anxiety and Depression and Concussion Symptoms and Severity
4.3. Symptom Level of Concussed Athletes in This Study
4.4. Mental Health Subscore of the SF-36 Questionnaire
4.5. Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Harmon, K.G.; Drezner, J.; Gammons, M.; Guskiewicz, K.; Halstead, M.; Herring, S.; Kutcher, J.; Pana, A.; Putukian, M.; Roberts, W. American Medical Society for Sports Medicine Position Statement: Concussion in Sport. Clin. J. Sport Med. 2013, 23, 1–18. [Google Scholar] [CrossRef] [PubMed]
- Maas, A.I.; Menon, D.K.; Adelson, P.D.; Andelic, N.; Bell, M.J.; Belli, A.; Bragge, P.; Brazinova, A.; Büki, A.; Chesnut, R.M. Traumatic Brain Injury: Integrated Approaches to Improve Prevention, Clinical Care, and Research. Lancet Neurol. 2017, 16, 987–1048. [Google Scholar] [CrossRef] [PubMed]
- Cassidy, J.D.; Cancelliere, C.; Carroll, L.J.; Côté, P.; Hincapié, C.A.; Holm, L.W.; Hartvigsen, J.; Donovan, J.; Nygren-de Boussard, C.; Kristman, V.L. Systematic Review of Self-Reported Prognosis in Adults after Mild Traumatic Brain Injury: Results of the International Collaboration on Mild Traumatic Brain Injury Prognosis. Arch. Phys. Med. Rehabil. 2014, 95, S132–S151. [Google Scholar] [CrossRef] [PubMed]
- Iverson, G.L.; McCracken, L.M. ‘Postconcussive’Symptoms in Persons with Chronic Pain. Brain Inj. 1997, 11, 783–790. [Google Scholar] [CrossRef] [PubMed]
- McCrory, P.; Meeuwisse, W.H.; Aubry, M.; Cantu, R.C.; Dvořák, J.; Echemendia, R.J.; Engebretsen, L.; Johnston, K.; Kutcher, J.S.; Raftery, M. Consensus Statement on Concussion in Sport: The 4th International Conference on Concussion in Sport, Zurich, November 2012. J. Athl. Train. 2013, 48, 554–575. [Google Scholar] [CrossRef] [PubMed]
- McCrea, M.; Guskiewicz, K.M.; Marshall, S.W.; Barr, W.; Randolph, C.; Cantu, R.C.; Onate, J.A.; Yang, J.; Kelly, J.P. Acute Effects and Recovery Time Following Concussion in Collegiate Football Players: The NCAA Concussion Study. JAMA 2003, 290, 2556–2563. [Google Scholar] [CrossRef]
- Davis, G.A.; Purcell, L.; Schneider, K.J.; Yeates, K.O.; Gioia, G.A.; Anderson, V.; Ellenbogen, R.G.; Echemendia, R.J.; Makdissi, M.; Sills, A. The Child Sport Concussion Assessment Tool 5th Edition (Child SCAT5): Background and Rationale. Br. J. Sports Med. 2017, 51, 859–861. [Google Scholar]
- Echemendia, R.J.; Meeuwisse, W.; McCrory, P.; Davis, G.A.; Putukian, M.; Leddy, J.; Makdissi, M.; Sullivan, S.J.; Broglio, S.P.; Raftery, M. The Sport Concussion Assessment Tool 5th Edition (SCAT5): Background and Rationale. Br. J. Sports Med. 2017, 51, 848–850. [Google Scholar] [PubMed]
- Ponsford, J.; Cameron, P.; Fitzgerald, M.; Grant, M.; Mikocka-Walus, A.; Schönberger, M. Predictors of Postconcussive Symptoms 3 Months after Mild Traumatic Brain Injury. Neuropsychology 2012, 26, 304. [Google Scholar] [CrossRef]
- Van Veldhoven, L.; Sander, A.; Struchen, M.; Sherer, M.; Clark, A.N.; Hudnall, G.E.; Hannay, H. Predictive Ability of Preinjury Stressful Life Events and Post-Traumatic Stress Symptoms for Outcomes Following Mild Traumatic Brain Injury: Analysis in a Prospective Emergency Room Sample. J. Neurol. Neurosurg. Psychiatry 2011, 82, 782–787. [Google Scholar] [CrossRef]
- Ponsford, J.; Cameron, P.; Fitzgerald, M.; Grant, M.; Mikocka-Walus, A. Long-Term Outcomes after Uncomplicated Mild Traumatic Brain Injury: A Comparison with Trauma Controls. J. Neurotrauma 2011, 28, 937–946. [Google Scholar] [CrossRef] [PubMed]
- Silverberg, N.D.; Gardner, A.J.; Brubacher, J.R.; Panenka, W.J.; Li, J.J.; Iverson, G.L. Systematic Review of Multivariable Prognostic Models for Mild Traumatic Brain Injury. J. Neurotrauma 2015, 32, 517–526. [Google Scholar] [CrossRef] [PubMed]
- Moore, E.L.; Terryberry-Spohr, L.; Hope, D.A. Mild Traumatic Brain Injury and Anxiety Sequelae: A Review of the Literature. Brain Inj. 2006, 20, 117–132. [Google Scholar] [CrossRef] [PubMed]
- Scholten, A.C.; Haagsma, J.A.; Cnossen, M.C.; Olff, M.; Van Beeck, E.F.; Polinder, S. Prevalence of and Risk Factors for Anxiety and Depressive Disorders after Traumatic Brain Injury: A Systematic Review. J. Neurotrauma 2016, 33, 1969–1994. [Google Scholar] [CrossRef] [PubMed]
- Lethem, J.; Slade, P.D.; Troup, J.D.G.; Bentley, G. Outline of a Fear-Avoidance Model of Exaggerated Pain Perception—I. Behav. Res. Ther. 1983, 21, 401–408. [Google Scholar] [CrossRef]
- Lundberg, M.K.; Styf, J.; Carlsson, S.G. A Psychometric Evaluation of the Tampa Scale for Kinesiophobia—From a Physiotherapeutic Perspective. Physiother. Theory Pract. 2004, 20, 121–133. [Google Scholar] [CrossRef]
- Anderson, M.N.; Womble, M.N.; Mohler, S.A.; Said, A.; Stephenson-Brown, K.; Kontos, A.P.; Elbin, R. Preliminary Study of Fear of Re-Injury Following Sport-Related Concussion in High School Athletes. Dev. Neuropsychol. 2019, 44, 443–451. [Google Scholar] [CrossRef]
- Wijenberg, M.L.; Stapert, S.Z.; Verbunt, J.A.; Ponsford, J.L.; Van Heugten, C.M. Does the Fear Avoidance Model Explain Persistent Symptoms after Traumatic Brain Injury? Brain Inj. 2017, 31, 1597–1604. [Google Scholar] [CrossRef]
- Katz, M.; Lenoski, S.; Ali, H.; Craton, N. Concussion Office Based Rehabilitation Assessment: A Novel Clinical Tool for Concussion Assessment and Management. Brain Sci. 2020, 10, 593. [Google Scholar] [CrossRef]
- Dover, G.; Amar, V. Development and Validation of the Athlete Fear Avoidance Questionnaire. J. Athl. Train. 2015, 50, 634–642. [Google Scholar] [CrossRef]
- Echemendia, R.J.; Broglio, S.P.; Davis, G.A.; Guskiewicz, K.M.; Hayden, K.A.; Leddy, J.J.; Meehan, W.P.; Putukian, M.; Sullivan, S.J.; Schneider, K.J. What Tests and Measures Should Be Added to the SCAT3 and Related Tests to Improve Their Reliability, Sensitivity and/or Specificity in Sideline Concussion Diagnosis? A Systematic Review. Br. J. Sports Med. 2017, 51, 895–901. [Google Scholar] [CrossRef]
- Riemann, B.L.; Guskiewicz, K.M.; Shields, E.W. Relationship between Clinical and Forceplate Measures of Postural Stability. J. Sport Rehabil. 1999, 8, 71–82. [Google Scholar] [CrossRef]
- Lephart, S.M.; Ferris, C.M.; Riemann, B.L.; Myers, J.B.; Fu, F.H. Gender Differences in Strength and Lower Extremity Kinematics During Landing. Clin. Orthop. 2002, 401, 162–169. [Google Scholar] [CrossRef]
- Sullivan, M.J.; Bishop, S.R.; Pivik, J. The Pain Catastrophizing Scale: Development and Validation. Psychol. Assess. 1995, 7, 524. [Google Scholar] [CrossRef]
- Vlaeyen, J.W.S.; Kole-Snijders, A.M.J.; Boeren, R.G.B.; van Eek, H. Fear of Movement/(Re)Injury in Chronic Low Back Pain and Its Relation to Behavioral Performance. Pain 1995, 62, 363–372. [Google Scholar] [CrossRef]
- Whelan-Goodinson, R.; Ponsford, J.; Schönberger, M. Validity of the Hospital Anxiety and Depression Scale to Assess Depression and Anxiety Following Traumatic Brain Injury as Compared with the Structured Clinical Interview for DSM-IV. J. Affect. Disord. 2009, 114, 94–102. [Google Scholar] [CrossRef]
- Instrument Ware Jr, J.; Sherbourne, C. The MOS 36-Item Short-Form Health Survey (SF-36): I. Conceptual Framework and Item Selection. Med. Care 1992, 30, 473–483. [Google Scholar]
- Vlaeyen, J.W.; Linton, S.J. Fear-Avoidance Model of Chronic Musculoskeletal Pain: 12 Years On. Pain 2012, 153, 1144–1147. [Google Scholar] [CrossRef] [PubMed]
- Silverberg, N.D.; Panenka, W.J.; Iverson, G.L. Fear Avoidance and Clinical Outcomes from Mild Traumatic Brain Injury. J. Neurotrauma 2018, 35, 1864–1873. [Google Scholar] [CrossRef]
- Silverberg, N.D.; Iverson, G.L. Is Rest after Concussion “the Best Medicine?”: Recommendations for Activity Resumption Following Concussion in Athletes, Civilians, and Military Service Members. J. Head Trauma Rehabil. 2013, 28, 250–259. [Google Scholar] [CrossRef]
- Bunzli, S.; Smith, A.; Schütze, R.; Lin, I.; O’Sullivan, P. Making Sense of Low Back Pain and Pain-Related Fear. J. Orthop. Sports Phys. Ther. 2017, 47, 628–636. [Google Scholar] [CrossRef] [PubMed]
- Komandur, B.; Martin, P.R.; Bandarian-Balooch, S. Mindfulness and Chronic Headache/Migraine: Mechanisms Explored through the Fear-Avoidance Model of Chronic Pain. Clin. J. Pain 2018, 34, 638–649. [Google Scholar] [CrossRef] [PubMed]
- Greenberg, J.; Mace, R.A.; Funes, C.J.; Silverberg, N.D.; Iverson, G.L.; Caplan, D.N.; Vranceanu, A.-M. Pain Catastrophizing and Limiting Behavior Mediate the Association between Anxiety and Postconcussion Symptoms. Psychosomatics 2020, 61, 49–55. [Google Scholar] [CrossRef] [PubMed]
- Edmed, S.; Sullivan, K. Depression, Anxiety, and Stress as Predictors of Postconcussion-like Symptoms in a Non-Clinical Sample. Psychiatry Res. 2012, 200, 41–45. [Google Scholar] [CrossRef] [PubMed]
- King, N.S. Emotional, Neuropsychological, and Organic Factors: Their Use in the Prediction of Persisting Postconcussion Symptoms after Moderate and Mild Head Injuries. J. Neurol. Neurosurg. Psychiatry 1996, 61, 75–81. [Google Scholar] [CrossRef]
- Iverson, G.L. A Biopsychosocial Conceptualization of Poor Outcome from Mild Traumatic Brain Injury. In PTSD and Mild Traumatic Brain Injury; The Guilford Press: New York, NY, USA, 2012. [Google Scholar]
- Putukian, M.; Echemendia, R.; Dettwiler-Danspeckgruber, A.; Duliba, T.; Bruce, J.; Furtado, J.L.; Murugavel, M. Prospective Clinical Assessment Using Sideline Concussion Assessment Tool-2 Testing in the Evaluation of Sport-Related Concussion in College Athletes. Clin. J. Sport Med. 2015, 25, 36–42. [Google Scholar] [CrossRef] [PubMed]
- Bin Zahid, A.; Hubbard, M.E.; Dammavalam, V.M.; Balser, D.Y.; Pierre, G.; Kim, A.; Kolecki, R.; Mehmood, T.; Wall, S.P.; Frangos, S.G. Assessment of Acute Head Injury in an Emergency Department Population Using Sport Concussion Assessment Tool–3rd Edition. Appl. Neuropsychol. Adult 2018, 25, 110–119. [Google Scholar] [CrossRef]
- Tito, N.; Porter, E.; Castonguay, T.; Dover, G. Longitudinal Validation of a Specific Measure of Fear Avoidance in Athletes: Predicting Time from Injury to Return to Sports Competition. J. Pain Res. 2023, 16, 1103–1114. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| M ± SD or f | |
|---|---|
| Demographics/history | |
| Sex | |
| Male (n) | 23 |
| Female (n) | 11 |
| Age in years (M, SD) | 20.9 ± 1.8 |
| Height in cm (M, SD) | 178.1 ± 11.1 |
| Weight in kg (M, SD) | 84.7 ± 25.6 |
| Sport, (n) | |
| Basketball | 4 |
| Cheerleading | 2 |
| Football | 7 |
| Hockey | 12 |
| Lacrosse | 1 |
| Ringuette | 1 |
| Rugby | 4 |
| Soccer | 2 |
| Volleyball | 1 |
| Education level (n) | |
| University | 26 |
| College | 8 |
| SCAT5 (M, SD) † | |
| Number of past concussions ‡ | 1.9 ± 1.7 |
| Total number of symptoms ‡ | 7.4 ± 5.1 |
| Symptom severity score ‡ | 16.3 ± 17.0 |
| Hours from injury to assessment § | 33.4 ± 17.9 |
| Orientation score (/5) | 4.94 ± 0.25 |
| Digits backwards (/4) | 3.26 ± 0.93 |
| Months score (/1) | 0.90 ± 0.30 |
| Concentration score (/5) | 4.19 ± 0.91 |
| Balance (errors/10) | |
| Double leg | 1.65 ± 3.73 |
| Single leg | 3.81 ± 2.90 |
| Tandem stance | 2.23 ± 3.41 |
| Variable | 2. Symptom Severity Score | 3. No. of Past Concussions | 4. SF-36 Physical Functioning Subscore | 5. SF-36 Role Physical Subscore | 6. SF-36 Mental Health Subscore | 7. SF-36 Vitality Subscore | 8. SF-36 General Health Subscore | 9. PCS Score | 10. TSK Score | 11. AFAQ Score | 12. HADS Anxiety Score | 13. HADS Depression Score | 14. HADS Total Score |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 1. Total no. of symptoms | 0.908 ** | −0.003 | −0.431 * | −0.266 | −0.571 ** | −0.455 ** | −0.228 | 0.299 | 0.282 | 0.493 ** | 0.563 ** | 0.614 ** | 0.686 ** |
| 2. Symptom Severity score | - | 0.109 | −0.374 * | −0.250 | −0.518 ** | −0.360 * | −0.151 | 0.33 | 0.253 | 0.481 ** | 0.492 ** | 0.541 ** | 0.602 ** |
| 3. No. of past concussions | - | 0.103 | 0.074 | −0.180 | −0.135 | −0.148 | 0.305 | 0.138 | 0.332 | −0.013 | −0.029 | −0.26 | |
| 4. SF-36 Physical Functioning subscore | - | −0.120 | 0.473 ** | 0.412 * | 0.357 * | 0.285 | −0.215 | −0.504 ** | −0.174 | −0.626 ** | −0.494 ** | ||
| 5. SF-36 Role Physical subscore | - | 0.148 | −0.048 | 0.092 | −0.096 | 0.165 | −0.228 | −0.037 | 0.024 | −0.003 | |||
| 6. SF-36 Mental Health subscore | - | 0.798 ** | 0.493 ** | −0.396 * | −0.208 | −0.532 ** | −0.484 ** | −0.418 * | −0.519 ** | ||||
| 7. SF-36 Vitality subscore | - | 0.452 ** | −0.184 | −0.156 | −0.416 * | −0.307 | −0.286 | −0.342 * | |||||
| 8. SF-36 General Health subscore | - | −0.138 | −0.146 | −0.185 | −0.170 | −0.300 | −0.281 | ||||||
| 9. PCS score | - | 0.485 ** | 0.711 ** | 0.526 ** | 0.356 * | 0.500 ** | |||||||
| 10. TSK score | - | 0.637 ** | 0.165 | 0.366 * | 0.321 | ||||||||
| 11. AFAQ score | - | 0.346 * | 0.475 | 0.484 ** | |||||||||
| 12. HADS anxiety score | - | 0.481 ** | 0.824 ** | ||||||||||
| 13. HADS depression score | - | 0.893 ** | |||||||||||
| 14. HADS total score | - |
| Model 1—Concussion Symptoms | Coefficient B | t-Value | Sig | r2 |
|---|---|---|---|---|
| Athlete Fear Avoidance | 0.152 | 1.434 | 0.162 | 0.504 |
| HADS—Depression | 0.521 | 2.286 | 0.030 * | |
| HADS—Anxiety | 0.571 | 2.130 | 0.041 * | |
| Model 2—Symptom Severity | ||||
| Athlete Fear Avoidance | 0.592 | 1.545 | 0.133 | 0.410 |
| HADS—Depression | 1.411 | 1.717 | 0.096 | |
| HADS—Anxiety | 1.571 | 1.624 | 0.115 | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Patlan, I.; Gamelin, G.; Khalaj, K.; Castonguay, T.; Dover, G. Athlete Fear Avoidance, Depression, and Anxiety Are Associated with Acute Concussion Symptoms in Athletes. J. Clin. Med. 2024, 13, 2401. https://doi.org/10.3390/jcm13082401
Patlan I, Gamelin G, Khalaj K, Castonguay T, Dover G. Athlete Fear Avoidance, Depression, and Anxiety Are Associated with Acute Concussion Symptoms in Athletes. Journal of Clinical Medicine. 2024; 13(8):2401. https://doi.org/10.3390/jcm13082401
Chicago/Turabian StylePatlan, Ilana, Gabrielle Gamelin, Kosar Khalaj, Tristan Castonguay, and Geoffrey Dover. 2024. "Athlete Fear Avoidance, Depression, and Anxiety Are Associated with Acute Concussion Symptoms in Athletes" Journal of Clinical Medicine 13, no. 8: 2401. https://doi.org/10.3390/jcm13082401