

Three-Dimensional Printed Patient-Specific Vestibular Augmentation: A Case Report
 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Case Presentation
2.2. Patient-Specific Bone Graft: Description, Virtual Surgical Planning (VSP), and Design
2.3. Surgical Procedures
2.3.1. Vestibular Augmentation
2.3.2. Dental Implant Placement
2.4. CBCT Follow-Up
2.5. Biopsy Evaluation
2.5.1. μ-CT Assessment
2.5.2. μ-CT Assessment
3. Results
3.1. Case Follow-Up
3.1.1. General Aspects and Radiological Assessment
3.1.2. Radiological Quantification
3.2. μ-CT Assessment
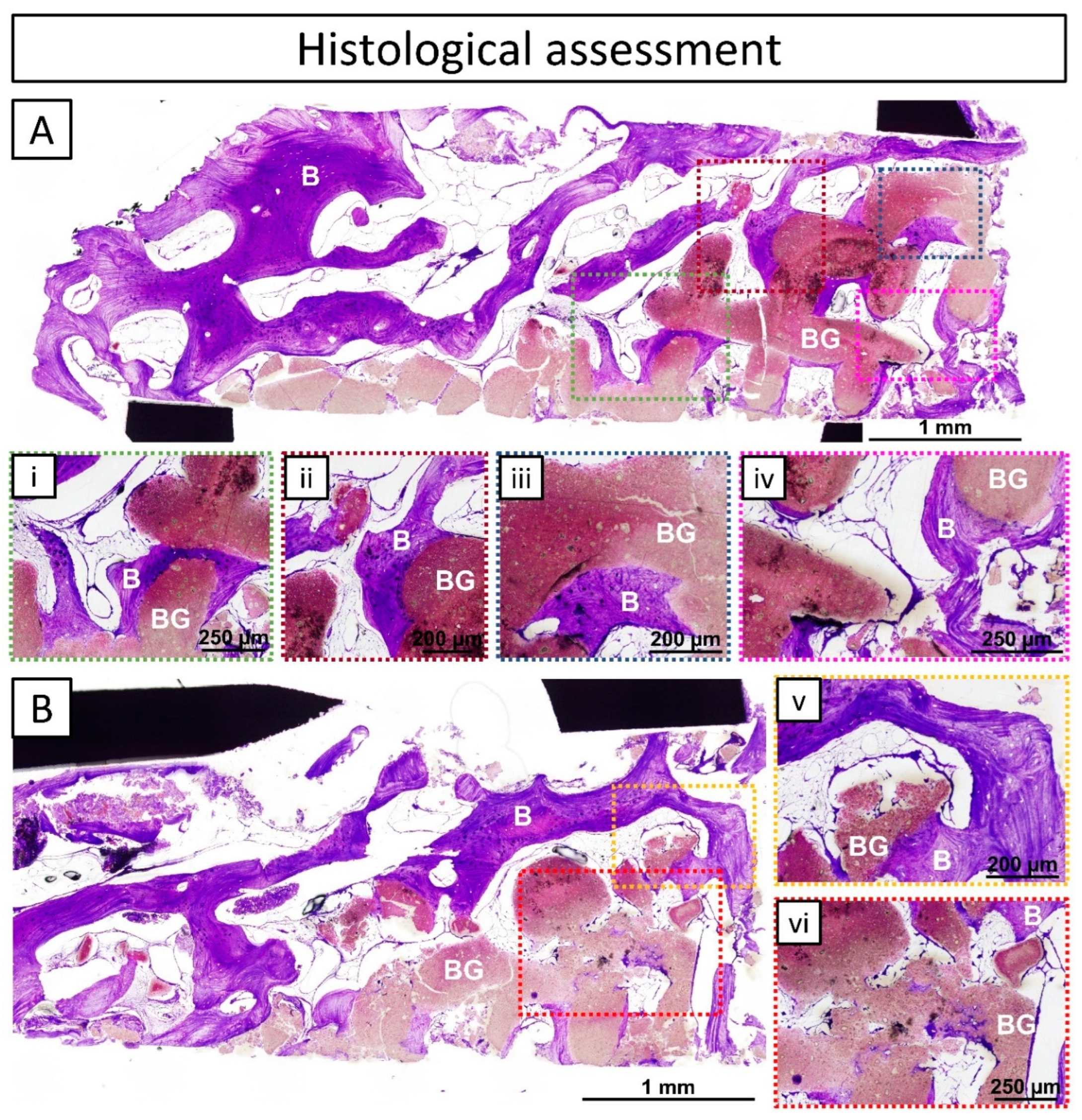
3.3. Histological Assessment
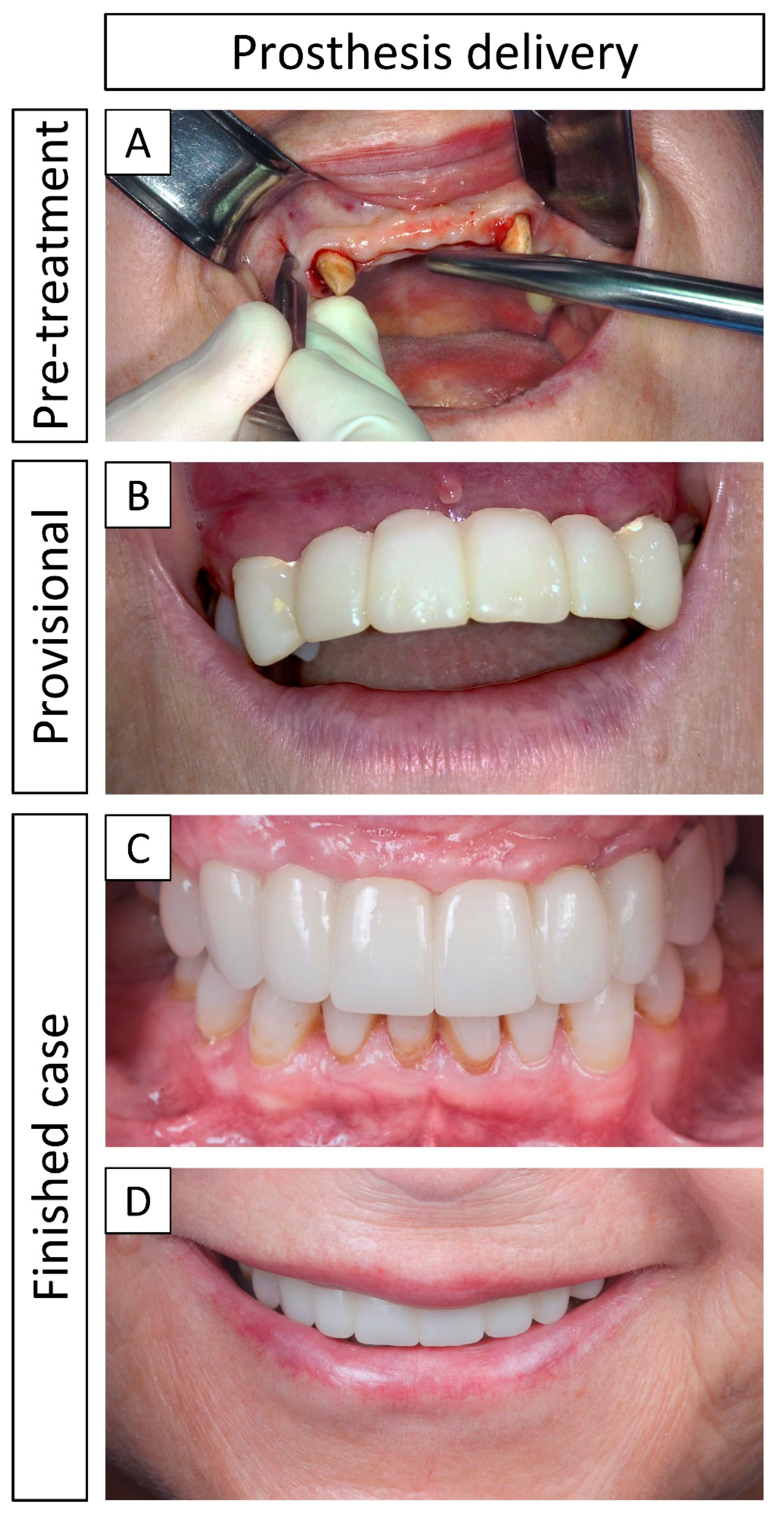
3.4. Definitive Prosthesis Delivery and 1-Year Follow-Up
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| α-TCP | Alpha-tricalcium phosphate |
| β-TCP | Beta-tricalcium phosphate |
| µ-CT | Micro-computed tomography |
| 3D-printed | Three-dimensional-printed |
| CaP | Calcium phosphate |
| CBCT | Cone-beam computed tomography |
| CDHA | Calcium-deficient hydroxyapatite |
| DICOM | Digital imaging and communications in medicine |
| DIW | Direct ink writing |
| GBR | Guided bone regeneration |
| HA | Hydroxyapatite |
| MDR | Medical device regulation |
| OR | Operating room |
| STL | Stereolithography |
| VOI | Volume of interest |
| VSP | Virtual surgical planning |
References
- Schropp, L.; Wenzel, A.; Kostopoulos, L.; Karring, T. Bone Healing and Soft Tissue Contour Changes Following Single-Tooth Extraction: A Clinical and Radiographic 12-Month Prospective Study. Int. J. Periodontics Restor. Dent. 2003, 23, 313–323. [Google Scholar]
- Dong, J.K.; Jin, T.H.; Cho, H.W.; Oh, S.C. The Esthetics of the Smile: A Review of Some Recent Studies. Int. J. Prosthodont. 1999, 12, 9–19. [Google Scholar] [PubMed]
- Urban, I.A.; Montero, E.; Amerio, E.; Palombo, D.; Monje, A. Techniques on Vertical Ridge Augmentation: Indications and Effectiveness. Periodontology 2000 2023, 93, 153–182. [Google Scholar] [CrossRef] [PubMed]
- Kuchler, U.; von Arx, T. Horizontal Ridge Augmentation in Conjunction with or Prior to Implant Placement in the Anterior Maxilla: A Systematic Review. Int. J. Oral. Maxillofac. Implant. 2014, 29, 14–24. [Google Scholar] [CrossRef] [PubMed]
- Sanz-Sánchez, I.; Sanz-Martín, I.; Ortiz-Vigón, A.; Molina, A.; Sanz, M. Complications in Bone-grafting Procedures: Classification and Management. Periodontology 2000 2022, 88, 86–102. [Google Scholar] [CrossRef] [PubMed]
- Sethi, A.; Kaus, T. Ridge Augmentation Using Mandibular Block Bone Grafts: Preliminary Results of an Ongoing Prospective Study. Int. J. Oral. Maxillofac. Implant. 2001, 16, 378–388. [Google Scholar]
- Raymond, Y.; Johansson, L.; Thorel, E.; Ginebra, M.-P. Translation of Three-Dimensional Printing of Ceramics in Bone Tissue Engineering and Drug Delivery. MRS Bull. 2022, 47, 59–69. [Google Scholar] [CrossRef]
- Urban, I. Vertical and Horizontal Ridge Augmentation: New Perspectives; Quintessence Publishing: Berlin, Germany, 2017; Volume 1, ISBN 978-1-78698-000-7. [Google Scholar]
- Venet, L.; Perriat, M.; Mangano, F.G.; Fortin, T. Horizontal Ridge Reconstruction of the Anterior Maxilla Using Customized Allogeneic Bone Blocks with a Minimally Invasive Technique—A Case Series. BMC Oral. Health 2017, 17, 146. [Google Scholar] [CrossRef] [PubMed]
- Sakkas, A.; Wilde, F.; Heufelder, M.; Winter, K.; Schramm, A. Autogenous Bone Grafts in Oral Implantology—Is It Still a “Gold Standard”? A Consecutive Review of 279 Patients with 456 Clinical Procedures. Int. J. Implant. Dent. 2017, 3, 23. [Google Scholar] [CrossRef]
- Sohn, H.-S.; Oh, J.-K. Review of Bone Graft and Bone Substitutes with an Emphasis on Fracture Surgeries. Biomater. Res. 2019, 23, 9. [Google Scholar] [CrossRef]
- Nkenke, E.; Neukam, F.W. Autogenous Bone Harvesting and Grafting in Advanced Jaw Resorption: Morbidity, Resorption and Implant Survival. Eur. J. Oral. Implantol. 2014, 7 (Suppl. 2), S203–S217. [Google Scholar] [PubMed]
- Shibuya, N.; Jupiter, D.C. Bone Graft Substitute: Allograft and Xenograft. Clin. Podiatr. Med. Surg. 2015, 32, 21–34. [Google Scholar] [CrossRef] [PubMed]
- Vidal, L.; Kampleitner, C.; Krissian, S.; Brennan, M.Á.; Hoffmann, O.; Raymond, Y.; Maazouz, Y.; Ginebra, M.-P.; Rosset, P.; Layrolle, P. Regeneration of Segmental Defects in Metatarsus of Sheep with Vascularized and Customized 3D-Printed Calcium Phosphate Scaffolds. Sci. Rep. 2020, 10, 7068. [Google Scholar] [CrossRef] [PubMed]
- Raymond, Y.; Bonany, M.; Lehmann, C.; Thorel, E.; Benítez, R.; Franch, J.; Espanol, M.; Solé-Martí, X.; Manzanares, M.-C.; Canal, C.; et al. Hydrothermal Processing of 3D-Printed Calcium Phosphate Scaffolds Enhances Bone Formation in Vivo: A Comparison with Biomimetic Treatment. Acta Biomater. 2021, 135, 671–688. [Google Scholar] [CrossRef] [PubMed]
- Barba, A.; Maazouz, Y.; Diez-Escudero, A.; Rappe, K.; Espanol, M.; Montufar, E.B.; Öhman-Mägi, C.; Persson, C.; Fontecha, P.; Manzanares, M.-C.; et al. Osteogenesis by Foamed and 3D-Printed Nanostructured Calcium Phosphate Scaffolds: Effect of Pore Architecture. Acta Biomater. 2018, 79, 135–147. [Google Scholar] [CrossRef] [PubMed]
- Gagnier, J.J.; Kienle, G.; Altman, D.G.; Moher, D.; Sox, H.; Riley, D. The CARE Guidelines: Consensus-Based Clinical Case Report Guideline Development. J. Clin. Epidemiol. 2014, 67, 46–51. [Google Scholar] [CrossRef]
- Donath, K. The Diagnostic Value of the New Method for the Study of Undecalcified Bones and Teeth with Attached Soft Tissue, (Säge-Schliff, (Sawing and Grinding) Technique). Pathol. Res. Pract. 1985, 179, 631–633. [Google Scholar] [CrossRef]
- Jenö, L.; Géza, L. A Simple Differential Staining Method for Semi-Thin Sections of Ossifying Cartilage and Bone Tissues Embedded in Epoxy Resin. Mikroskopie 1975, 31, 1–4. [Google Scholar] [PubMed]
- Lekholm, U.; Zarb, G.A. Patient Selection and Preparation. Tissue Integrated Prostheses. In Tissue-Integrated Prostheses, Osseointegration in Clinical Dentistry; Brånemark, P.-I., Zarb, G.A., Albrektsson, T., Eds.; Quintessence Publishing: Chicago, IL, USA, 1985; pp. 199–209. [Google Scholar]
- Brie, J.; Chartier, T.; Chaput, C.; Delage, C.; Pradeau, B.; Caire, F.; Boncoeur, M.P.; Moreau, J.J. A New Custom Made Bioceramic Implant for the Repair of Large and Complex Craniofacial Bone Defects. J. Cranio-Maxillofac. Surg. 2013, 41, 403–407. [Google Scholar] [CrossRef]
- Saijo, H.; Igawa, K.; Kanno, Y.; Mori, Y.; Kondo, K.; Shimizu, K.; Suzuki, S.; Chikazu, D.; Iino, M.; Anzai, M.; et al. Maxillofacial Reconstruction Using Custom-Made Artificial Bones Fabricated by Inkjet Printing Technology. J. Artif. Organs 2009, 12, 200–205. [Google Scholar] [CrossRef]
- Sanz-Sánchez, I.; Ortiz-Vigón, A.; Sanz-Martín, I.; Figuero, E.; Sanz, M. Effectiveness of Lateral Bone Augmentation on the Alveolar Crest Dimension. J. Dent. Res. 2015, 94, 128S–142S. [Google Scholar] [CrossRef] [PubMed]
- Urban, I.A.; Montero, E.; Monje, A.; Sanz-Sánchez, I. Effectiveness of Vertical Ridge Augmentation Interventions: A Systematic Review and Meta-analysis. J. Clin. Periodontol. 2019, 46, 319–339. [Google Scholar] [CrossRef] [PubMed]
- Urban, I.; Sanz-Sánchez, I.; Monje, A.; Montero, E. Complications and Treatment Errors in Peri-implant Hard Tissue Management. Periodontology 2000 2023, 92, 278–298. [Google Scholar] [CrossRef] [PubMed]
- Chiapasco, M.; Tommasato, G.; Palombo, D.; Del Fabbro, M. A Retrospective 10-year Mean Follow-up of Implants Placed in Ridges Grafted Using Autogenous Mandibular Blocks Covered with Bovine Bone Mineral and Collagen Membrane. Clin. Oral. Implants Res. 2020, 31, 328–340. [Google Scholar] [CrossRef] [PubMed]
- Vidal, L.; Kampleitner, C.; Brennan, M.Á.; Hoornaert, A.; Layrolle, P. Reconstruction of Large Skeletal Defects: Current Clinical Therapeutic Strategies and Future Directions Using 3D Printing. Front. Bioeng. Biotechnol. 2020, 8, 61. [Google Scholar] [CrossRef]
- Del-Mazo-Barbara, L.; Johansson, L.; Tampieri, F.; Ginebra, M.-P. Toughening 3D Printed Biomimetic Hydroxyapatite Scaffolds: Polycaprolactone-Based Self-Hardening Inks. Acta Biomater. 2024, 177, 506–524. [Google Scholar] [CrossRef]









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| [mm] | Initial Bone Thickness (i) | Bone Augmentation (a) | Total Bone Thickness (t) |
|---|---|---|---|
| Pre-surgery | 4.3 | 3.7 (planned) | 4.3 |
| 11 D post-surgery | - | 3.6 | 7.9 |
| 8 M post-surgery | - | 3.7 | 8.0 |
| 13 M post-surgery | - | 3.7 | 8.0 |
| New Bone | Bone Graft | Soft Tissue | VOI | |
|---|---|---|---|---|
| Volume [mm3] | 1.912 | 1.947 | 0.831 | 4.689 |
| Fraction [%] | 40.77 | 41.51 | 17.72 | - |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Johansson, L.; Latorre, J.L.; Liversain, M.; Thorel, E.; Raymond, Y.; Ginebra, M.-P. Three-Dimensional Printed Patient-Specific Vestibular Augmentation: A Case Report. J. Clin. Med. 2024, 13, 2408. https://doi.org/10.3390/jcm13082408
Johansson L, Latorre JL, Liversain M, Thorel E, Raymond Y, Ginebra M-P. Three-Dimensional Printed Patient-Specific Vestibular Augmentation: A Case Report. Journal of Clinical Medicine. 2024; 13(8):2408. https://doi.org/10.3390/jcm13082408
Chicago/Turabian StyleJohansson, Linh, Jose Luis Latorre, Margaux Liversain, Emilie Thorel, Yago Raymond, and Maria-Pau Ginebra. 2024. "Three-Dimensional Printed Patient-Specific Vestibular Augmentation: A Case Report" Journal of Clinical Medicine 13, no. 8: 2408. https://doi.org/10.3390/jcm13082408