
Mechanical Support in High-Risk Pulmonary Embolism: Review Article

 ,
, {kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Mechanism of Hemodynamic Collapse
3. Treatment Options for High-Risk PE
4. Mechanical Circulatory Support (MCS)
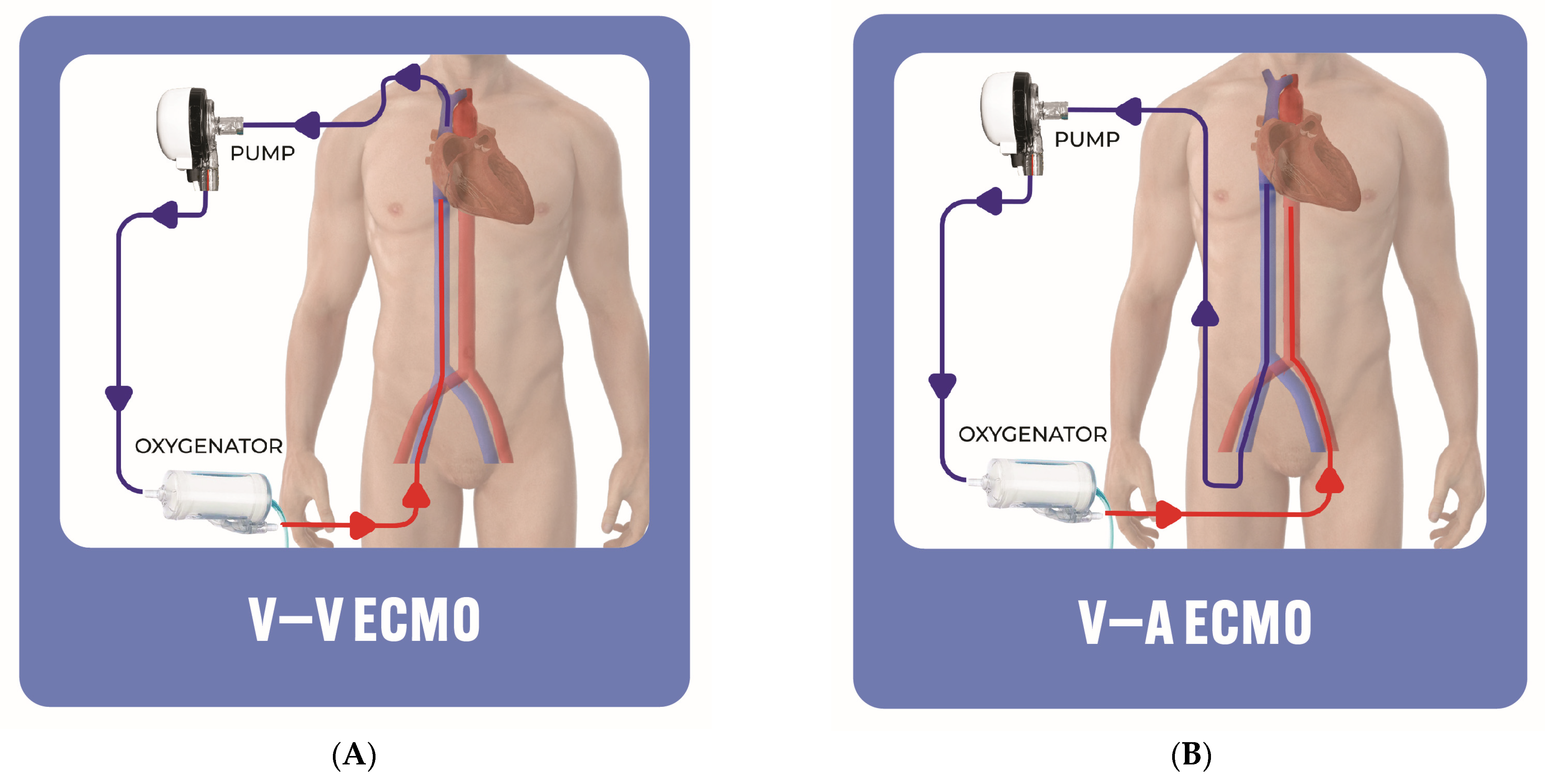
5. ECMO
- Cons: ECMO is associated with major complications that strongly influence the recovery and prognosis of patients, including vascular access complications, hemolysis, bleeding, and stroke, which are secondary to cardioembolic or cerebral hypoperfusion [43]. In addition, there is a risk of worsening LV function or LV distention, particularly in patients with pre-existing LV systolic dysfunction. Hence, various LV venting techniques can be implemented to decompress the LV in high-risk patients [44,45].
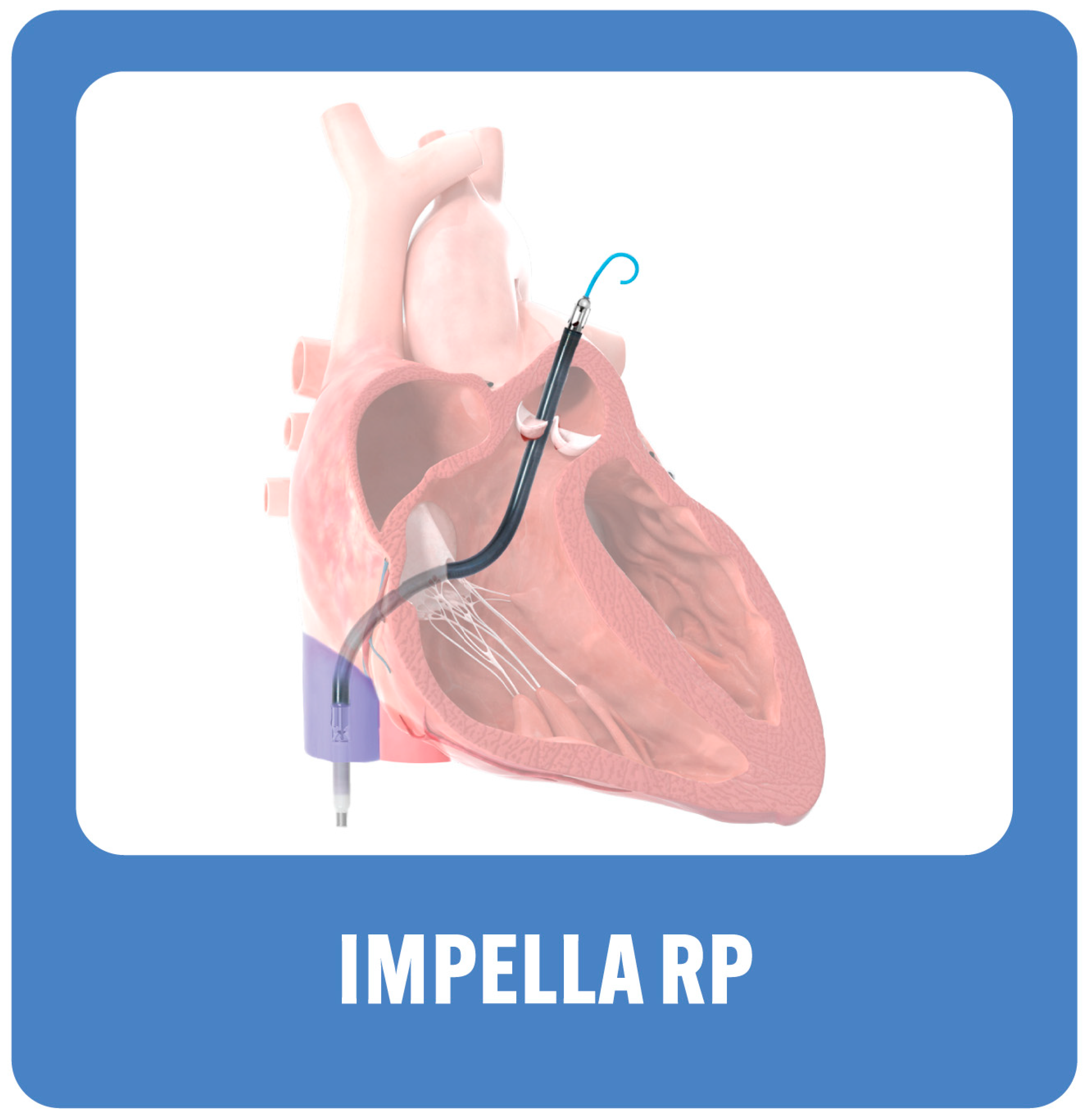
6. Right Ventricular Assist Device (RVAD): Right-Sided Impella Device, Impella RP (Abiomed Inc., Danvers, MA, USA)
- Pros: The Impella RP offers easy insertion through a single venous access point, without the need for perfusionist support. The risk of hemolysis is mild. Additionally, a left-sided Impella can be added for LV support.
- Cons: The Impella RP does not provide pulmonary support with oxygenation. It cannot be used in patients with abnormal pulmonary artery anatomy as it precludes the placement of the device, those with right-sided mechanical valves or severe stenosis or regurgitation, anatomical limitations of the inferior vena cava that preclude the advancement of the device to the right atrium, or thrombus in the inferior vena cava or the right atrium.
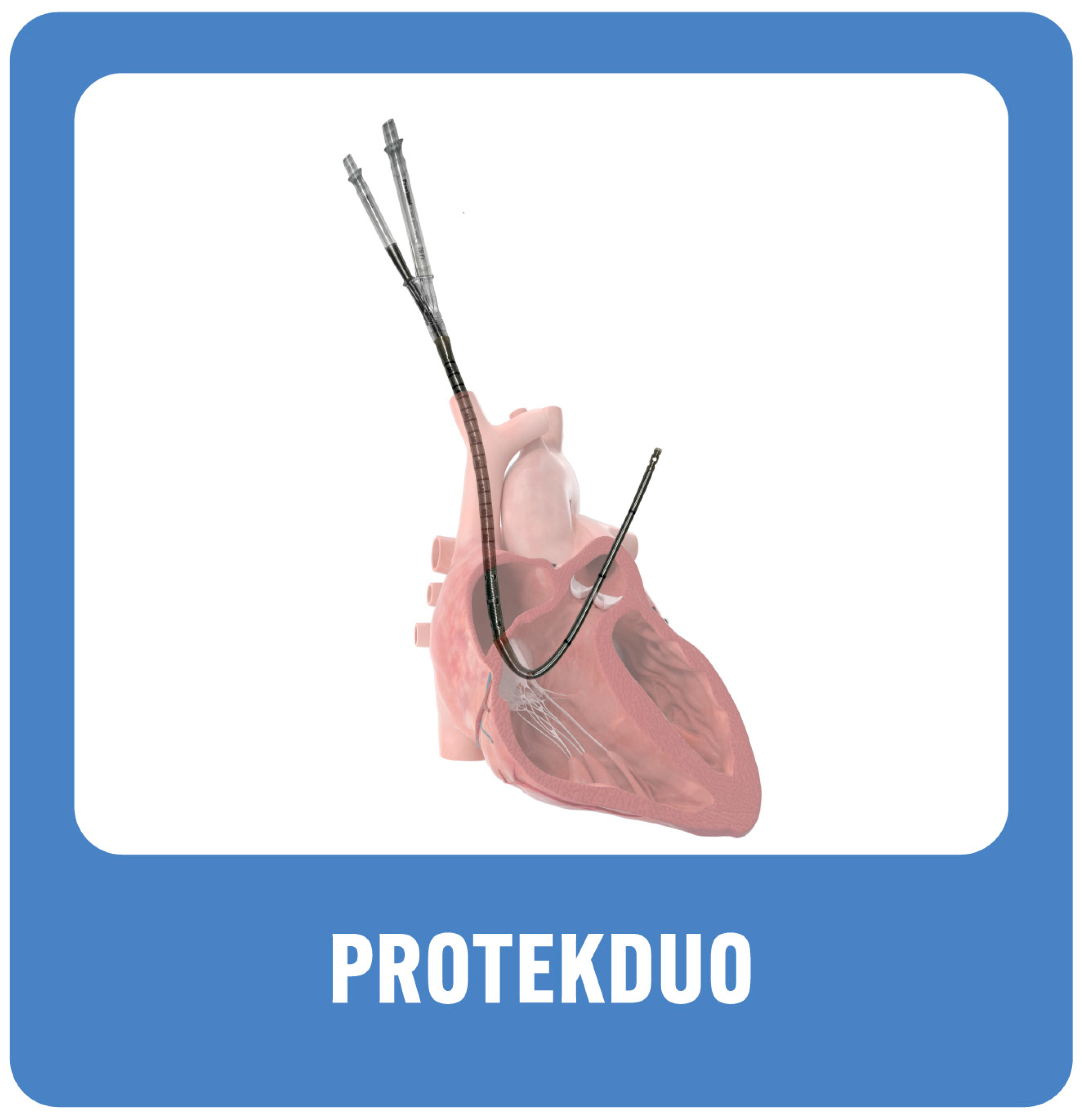
7. Right Ventricular Assist Device (RVAD): ProtekDuo (Livanova, UK)
- Pros: single access via internal jugular vein, patient can ambulate if needed, and an oxygenator can be added if necessary. Less risk of hemolysis.
- Cons: Insertion requires careful measurement and time investment. Similar to Impella RP, it needs fluoroscopic guidance; thus, insertion has to be performed in the cath lab.
8. Special Considerations and Future Directions: Proposed Management Approach
9. Conclusions
Funding
Conflicts of Interest
References
- Tsao, C.W.; Aday, A.W.; Almarzooq, Z.I.; Alonso, A.; Beaton, A.Z.; Bittencourt, M.S.; Boehme, A.K.; Buxton, A.E.; Carson, A.P.; Commodore-Mensah, Y.; et al. Heart Disease and Stroke Statistics-2022 Update: A Report from the American Heart Association. Circulation 2022, 145, e153–e639. [Google Scholar] [PubMed]
- Giri, J.; Sista, A.K.; Weinberg, I.; Kearon, C.; Kumbhani, D.J.; Desai, N.D.; Piazza, G.; Gladwin, M.T.; Chatterjee, S.; Kobayashi, T.; et al. Interventional Therapies for Acute Pulmonary Embolism: Current Status and Principles for the Development of Novel Evidence. Circulation 2019, 140, E774–E801. [Google Scholar] [CrossRef] [PubMed]
- Piazza, G. Advanced Management of Intermediate- and High-Risk Pulmonary Embolism: JACC Focus Seminar. J. Am. Coll. Cardiol. 2020, 76, 2117–2127. [Google Scholar] [CrossRef] [PubMed]
- Rooke, T.W.; Hirsch, A.T.; Misra, S.; Sidawy, A.N.; Beckman, J.A.; Findeiss, L.K.; Golzarian, J.; Gornik, H.L.; Halperin, J.L.; Jaff, M.R.; et al. 2011 ACCF/AHA Focused Update of the Guideline for the Management of Patients with Peripheral Artery Disease (Updating the 2005 Guideline): A Report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guideli. Catheter. Cardiovasc. Interv. Off. J. Soc. Card. Angiogr. Interv. 2012, 79, 501–531. [Google Scholar] [CrossRef]
- Becattini, C.; Agnelli, G.; Lankeit, M.; Masotti, L.; Pruszczyk, P.; Casazza, F.; Vanni, S.; Nitti, C.; Kamphuisen, P.; Vedovati, M.C.; et al. Acute Pulmonary Embolism: Mortality Prediction by the 2014 European Society of Cardiology Risk Stratification Model. Eur. Respir. J. 2016, 48, 780–786. [Google Scholar] [CrossRef]
- Stein, P.D.; Matta, F.; Hughes, M.J. Hospitalizations for High-Risk Pulmonary Embolism. Am. J. Med. 2021, 134, 621–625. [Google Scholar] [CrossRef]
- Wendelboe, A.M.; Raskob, G.E. Global Burden of Thrombosis: Epidemiologic Aspects. Circ. Res. 2016, 118, 1340–1347. [Google Scholar] [CrossRef] [PubMed]
- Quezada, A.; Jiménez, D.; Bikdeli, B.; Moores, L.; Porres-Aguilar, M.; Aramberri, M.; Lima, J.; Ballaz, A.; Yusen, R.D.; Monreal, M. Systolic Blood Pressure and Mortality in Acute Symptomatic Pulmonary Embolism. Int. J. Cardiol. 2020, 302, 157–163. [Google Scholar] [CrossRef]
- Carroll, B.J.; Larnard, E.A.; Pinto, D.S.; Giri, J.; Secemsky, E.A. Percutaneous Management of High-Risk Pulmonary Embolism. Circ. Cardiovasc. Interv. 2023, 16, E012166. [Google Scholar] [CrossRef]
- Thandavarayan, R.A.; Chitturi, K.R.; Guha, A. Pathophysiology of Acute and Chronic Right Heart Failure. Cardiol. Clin. 2020, 38, 149–160. [Google Scholar] [CrossRef]
- McIntyre, K.M.; Sasahara, A.A. The Hemodynamic Response to Pulmonary Embolism in Patients without Prior Cardiopulmonary Disease. Am. J. Cardiol. 1971, 28, 288–294. [Google Scholar] [CrossRef]
- Matthews, J.C.; McLaughlin, V. Acute Right Ventricular Failure in the Setting of Acute Pulmonary Embolism or Chronic Pulmonary Hypertension: A Detailed Review of the Pathophysiology, Diagnosis, and Management. Curr. Cardiol. Rev. 2008, 4, 49–59. [Google Scholar] [CrossRef] [PubMed]
- Van Wolferen, S.A.; Marcus, J.T.; Westerhof, N.; Spreeuwenberg, M.D.; Marques, K.M.J.; Bronzwaer, J.G.F.; Henkens, I.R.; Gan, C.T.J.; Boonstra, A.; Postmus, P.E.; et al. Right Coronary Artery Flow Impairment in Patients with Pulmonary Hypertension. Eur. Heart J. 2008, 29, 120–127. [Google Scholar] [CrossRef] [PubMed]
- Wood, K.E. Major Pulmonary Embolism: Review of a Pathophysiologic Approach to the Golden Hour of Hemodynamically Significant Pulmonary Embolism. Chest 2002, 121, 877–905. [Google Scholar] [CrossRef] [PubMed]
- Vlahakes, G.U.S.J.; Turley, K.; Hoffman, J.I.E. The Pathophysiology of Failure in Acute Right Ventricular Hypertension: Hemodynamic and Biochemical Correlations. Circulation 1981, 63, 87–95. [Google Scholar] [CrossRef] [PubMed]
- Rosenberger, P.; Shernan, S.K.; Shekar, P.S.; Tuli, J.K.; Weissmüller, T.; Aranki, S.F.; Eltzschig, H.K. Acute Hemodynamic Collapse after Induction of General Anesthesia for Emergent Pulmonary Embolectomy. Anesth. Analg. 2006, 102, 1311–1315. [Google Scholar] [CrossRef] [PubMed]
- Grifoni, S.; Olivotto, I.; Cecchini, P.; Pieralli, F.; Camaiti, A.; Santoro, G.; Conti, A.; Agnelli, G.; Berni, G. Short-Term Clinical Outcome of Patients with Acute Pulmonary Embolism, Normal Blood Pressure, and Echocardiographic Right Ventricular Dysfunction. Circulation 2000, 101, 2817–2822. [Google Scholar] [CrossRef]
- Konstam, M.A.; Kiernan, M.S.; Bernstein, D.; Bozkurt, B.; Jacob, M.; Kapur, N.K.; Kociol, R.D.; Lewis, E.F.; Mehra, M.R.; Pagani, F.D.; et al. Evaluation and Management of Right-Sided Heart Failure: A Scientific Statement From the American Heart Association. Circulation 2018, 137, e578–e622. [Google Scholar] [CrossRef] [PubMed]
- Elder, M.; Blank, N.; Shemesh, A.; Pahuja, M.; Kaki, A.; Mohamad, T.; Schreiber, T.; Giri, J. Mechanical Circulatory Support for High-Risk Pulmonary Embolism. Interv. Cardiol. Clin. 2018, 7, 119–128. [Google Scholar] [CrossRef]
- Arrigo, M.; Price, S.; Harjola, V.-P.; Huber, L.C.; Schaubroeck, H.A.I.; Vieillard-Baron, A.; Masip, J.; Mebazaa, A. Diagnosis and Treatment of Right Ventricular Failure Secondary to Acutely Increased Right Ventricular Afterload (Acute Cor Pulmonale). A Clinical Consensus Statement of the Association for Acute CardioVascular Care (ACVC) of the ESC. Eur. Heart J. Acute Cardiovasc. Care 2024, 13, 304–312. [Google Scholar] [CrossRef]
- Groeneveld, N.T.A.; Swier, C.E.L.; Montero-Cabezas, J.; Elzo Kraemer, C.V.; Klok, F.A.; van den Brink, F.S. Mechanical Support Strategies for High-Risk Procedures in the Invasive Cardiac Catheterization Laboratory: A State-of-the-Art Review. J. Clin. Med. 2023, 12, 7755. [Google Scholar] [CrossRef] [PubMed]
- Maggio, P.; Hemmila, M.; Haft, J.; Bartlett, R. Extracorporeal Life Support for Massive Pulmonary Embolism. J. Trauma. 2007, 62, 570–576. [Google Scholar] [CrossRef] [PubMed]
- Kmiec, L.; Philipp, A.; Floerchinger, B.; Lubnow, M.; Unterbuchner, C.; Creutzenberg, M.; Lunz, D.; Mueller, T.; Schmid, C.; Camboni, D. Extracorporeal Membrane Oxygenation for Massive Pulmonary Embolism as Bridge to Therapy. ASAIO J. 2020, 66, 146–152. [Google Scholar] [CrossRef] [PubMed]
- Rao, P.; Khalpey, Z.; Smith, R.; Burkhoff, D.; Kociol, R.D. Venoarterial Extracorporeal Membrane Oxygenation for Cardiogenic Shock and Cardiac Arrest. Circulation. Heart Fail. 2018, 11, e004905. [Google Scholar] [CrossRef] [PubMed]
- Oh, Y.N.; Oh, D.K.; Koh, Y.; Lim, C.-M.; Huh, J.-W.; Lee, J.S.; Jung, S.-H.; Kang, P.-J.; Hong, S.-B. Use of Extracorporeal Membrane Oxygenation in Patients with Acute High-Risk Pulmonary Embolism: A Case Series with Literature Review. Acute Crit. Care 2019, 34, 148–154. [Google Scholar] [CrossRef] [PubMed]
- Burkhoff, D.; Sayer, G.; Doshi, D.; Uriel, N. Hemodynamics of Mechanical Circulatory Support. J. Am. Coll. Cardiol. 2015, 66, 2663–2674. [Google Scholar] [CrossRef] [PubMed]
- Ain, D.L.; Albaghdadi, M.; Giri, J.; Abtahian, F.; Jaff, M.R.; Rosenfield, K.; Roy, N.; Villavicencio-Theoduloz, M.; Sundt, T.; Weinberg, I. Extra-Corporeal Membrane Oxygenation and Outcomes in Massive Pulmonary Embolism: Two Eras at an Urban Tertiary Care Hospital. Vasc. Med. 2018, 23, 60–64. [Google Scholar] [CrossRef]
- Elder, M.; Blank, N.; Kaki, A.; Alraies, M.C.; Grines, C.L.; Kajy, M.; Hasan, R.; Mohamad, T.; Schreiber, T. Mechanical Circulatory Support for Acute Right Ventricular Failure in the Setting of Pulmonary Embolism. J. Interv. Cardiol. 2018, 31, 518–524. [Google Scholar] [CrossRef]
- Hobohm, L.; Sagoschen, I.; Habertheuer, A.; Barco, S.; Valerio, L.; Wild, J.; Schmidt, F.P.; Gori, T.; Münzel, T.; Konstantinides, S.; et al. Clinical Use and Outcome of Extracorporeal Membrane Oxygenation in Patients with Pulmonary Embolism. Resuscitation 2022, 170, 285–292. [Google Scholar] [CrossRef]
- Karami, M.; Mandigers, L.; Miranda, D.D.R.; Rietdijk, W.J.R.; Binnekade, J.M.; Knijn, D.C.M.; Lagrand, W.K.; den Uil, C.A.; Henriques, J.P.S.; Vlaar, A.P.J. Survival of Patients with Acute Pulmonary Embolism Treated with Venoarterial Extracorporeal Membrane Oxygenation: A Systematic Review and Meta-Analysis. J. Crit. Care 2021, 64, 245–254. [Google Scholar] [CrossRef]
- Konstantinides, S.V.; Meyer, G.; Becattini, C.; Bueno, H.; Geersing, G.-J.; Harjola, V.-P.; Huisman, M.V.; Humbert, M.; Jennings, C.S.; Jiménez, D.; et al. 2019 ESC Guidelines for the Diagnosis and Management of Acute Pulmonary Embolism Developed in Collaboration with the European Respiratory Society (ERS). Eur. Heart J. 2020, 41, 543–603. [Google Scholar] [CrossRef] [PubMed]
- Goldberg, J.B.; Giri, J.; Kobayashi, T.; Ruel, M.; Mittnacht, A.J.C.; Rivera-Lebron, B.; DeAnda, A.J.; Moriarty, J.M.; MacGillivray, T.E. Surgical Management and Mechanical Circulatory Support in High-Risk Pulmonary Embolisms: Historical Context, Current Status, and Future Directions: A Scientific Statement From the American Heart Association. Circulation 2023, 147, e628–e647. [Google Scholar] [CrossRef] [PubMed]
- Pooboni, S.K.; Gulla, K.M. Vascular Access in ECMO. Indian J. Thorac. Cardiovasc. Surg. 2021, 37, 221–231. [Google Scholar] [CrossRef] [PubMed]
- Pavlushkov, E.; Berman, M.; Valchanov, K. Cannulation Techniques for Extracorporeal Life Support. Ann. Transl. Med. 2017, 5, 70. [Google Scholar] [CrossRef]
- Pasrija, C.; Kron, A.; George, P.; Raithel, M.; Boulos, F.; Herr, D.L.; Gammie, J.S.; Pham, S.M.; Grif, B.P.; Kon, Z.N. Utilization of Veno-Arterial Extracorporeal Membrane Oxygenation for Massive Pulmonary Embolism. Ann. Thorac. Surg. 2018, 105, 498–504. [Google Scholar] [CrossRef] [PubMed]
- Gangaraju, R.; Klok, F.A. Advanced Therapies and Extracorporeal Membrane Oxygenation for the Management of High-Risk Pulmonary Embolism. Hematol. Am. Soc. Hematology. Educ. Program. 2020, 2020, 195–200. [Google Scholar] [CrossRef]
- Pasrija, C.; Shah, A.; George, P.; Kronfli, A.; Raithel, M.; Boulos, F.; Ghoreishi, M.; Bittle, G.J.; Mazzeffi, M.A.; Rubinson, L.; et al. Triage and Optimization: A New Paradigm in the Treatment of Massive Pulmonary Embolism. J. Thorac. Cardiovasc. Surg. 2018, 156, 672–681. [Google Scholar] [CrossRef] [PubMed]
- Aissaoui, N.; El-Banayosy, A.; Combes, A. How to Wean a Patient from Veno-Arterial Extracorporeal Membrane Oxygenation. Intensive Care Med. 2015, 41, 902–905. [Google Scholar] [CrossRef]
- Lüsebrink, E.; Stremmel, C.; Stark, K.; Joskowiak, D.; Czermak, T.; Born, F.; Kupka, D.; Scherer, C.; Orban, M.; Petzold, T.; et al. Update on Weaning from Veno-Arterial Extracorporeal Membrane Oxygenation. J. Clin. Med. 2020, 9, 992. [Google Scholar] [CrossRef]
- Ius, F.; Hoeper, M.M.; Fegbeutel, C.; Kühn, C.; Olsson, K.; Koigeldiyev, N.; Tudorache, I.; Warnecke, G.; Optenhöfel, J.; Puntigam, J.O.; et al. Extracorporeal Membrane Oxygenation and Surgical Embolectomy for High-Risk Pulmonary Embolism. Eur. Respir. J. 2019, 53, 10–13. [Google Scholar] [CrossRef]
- Alba, A.C.; Foroutan, F.; Buchan, T.A.; Alvarez, J.; Kinsella, A.; Clark, K.; Zhu, A.; Lau, K.; McGuinty, C.; Aleksova, N.; et al. Mortality in Patients with Cardiogenic Shock Supported with VA ECMO: A Systematic Review and Meta-Analysis Evaluating the Impact of Etiology on 29,289 Patients. J. Heart Lung Transplant. Off. Publ. Int. Soc. Heart Transplant. 2021, 40, 260–268. [Google Scholar] [CrossRef] [PubMed]
- Corsi, F.; Lebreton, G.; Bréchot, N.; Hekimian, G.; Nieszkowska, A.; Trouillet, J.L.; Luyt, C.E.; Leprince, P.; Chastre, J.; Combes, A.; et al. Life-Threatening Massive Pulmonary Embolism Rescued by Venoarterial-Extracorporeal Membrane Oxygenation. Crit. Care 2017, 21, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Lorusso, R.; Gelsomino, S.; Parise, O.; Di Mauro, M.; Barili, F.; Geskes, G.; Vizzardi, E.; Rycus, P.T.; Muellenbach, R.; Mueller, T.; et al. Neurologic Injury in Adults Supported With Veno-Venous Extracorporeal Membrane Oxygenation for Respiratory Failure: Findings From the Extracorporeal Life Support Organization Database. Crit. Care Med. 2017, 45, 1389–1397. [Google Scholar] [CrossRef] [PubMed]
- Lo Coco, V.; Lorusso, R.; Raffa, G.M.; Malvindi, P.G.; Pilato, M.; Martucci, G.; Arcadipane, A.; Zieliński, K.; Suwalski, P.; Kowalewski, M. Clinical Complications during Veno-Arterial Extracorporeal Membrane Oxigenation in Post-Cardiotomy and Non Post-Cardiotomy Shock: Still the Achille’s Heel. J. Thorac. Dis. 2018, 10, 6993–7004. [Google Scholar] [CrossRef] [PubMed]
- Choi, J.H.; Kim, S.W.; Kim, Y.U.; Kim, S.; Kim, K.; Joo, S.; Lee, J.S. Application of Veno-Arterial-Venous Extracorporeal Membrane Oxygenation in Differential Hypoxia. Multidiscip. Respir. Med. 2014, 9, 1–5. [Google Scholar] [CrossRef]
- Anderson, M.B.; Goldstein, J.; Milano, C.; Morris, L.D.; Kormos, R.L.; Bhama, J.; Kapur, N.K.; Bansal, A.; Garcia, J.; Baker, J.N.; et al. Benefits of a Novel Percutaneous Ventricular Assist Device for Right Heart Failure: The Prospective RECOVER RIGHT Study of the Impella RP Device. J. Heart Lung Transplant. 2015, 34, 1549–1560. [Google Scholar] [CrossRef] [PubMed]
- Youssef, A.; Selle, A.; Ende, G.; Ibrahim, K. The Successful Use of the Impella RP after a Long Cardiopulmonary Resuscitation and Systemic Thrombolytic Therapy in a Patient with a Fulminant Pulmonary Embolism: The First Case Report. Eur. Heart J. Case Rep. 2018, 2, 1–4. [Google Scholar] [CrossRef] [PubMed]
- Shokr, M.; Rashed, A.; Mostafa, A.; Mohamad, T.; Schreiber, T.; Elder, M.; Kaki, A. Impella Rp Support and Catheter-Directed Thrombolysis: To Treat Right Ventricular Failure Caused by Pulmonary Embolism in 2 Patients. Tex. Heart Inst. J. 2018, 45, 182–185. [Google Scholar] [CrossRef]
- Zuin, M.; Rigatelli, G.; Daggubati, R.; Nguyen, T.; Roncon, L. Impella RP in Hemodynamically Unstable Patients with Acute Pulmonary Embolism. J. Artif. Organs 2020, 23, 105–112. [Google Scholar] [CrossRef]
- Kumar Bhatia, N.; Dickert, N.W.; Samady, H.; Babaliaros, V. The Use of Hemodynamic Support in Massive Pulmonary Embolism. Catheter. Cardiovasc. Interv. 2017, 90, 516–520. [Google Scholar] [CrossRef]
- Abdelshafy, M.; Caliskan, K.; Guven, G.; Elkoumy, A.; Elsherbini, H.; Elzomor, H.; Tenekecioglu, E.; Akin, S.; Soliman, O. Temporary Right-Ventricular Assist Devices: A Systematic Review. J. Clin. Med. 2022, 11, 613. [Google Scholar] [CrossRef] [PubMed]
- Oliveros, E.; Collado, F.M.; Poulin, M.F.; Seder, C.W.; March, R.; Kavinsky, C.J. Percutaneous Right Ventricular Assist Device Using the TandemHeart ProtekDuo: Real-World Experience. J. Invasive Cardiol. 2021, 33, E407–E411. [Google Scholar]
- Brewer, J.M.; Sharif, A.; Maybauer, M.O. Perspective Chapter: The ProtekDuo® Cannula for Acute Mechanical Circulatory Support. In Ventricular Assist Devices-Advances and Applications in Heart Failure; Purevjav, E., Martinez, H., Towbin, J.A., Boston, U., Eds.; IntechOpen: Rijeka, Croatia, 2023; pp. 283–287. ISBN 978-1-80356-453-1. [Google Scholar]
- Nasser, M.F.; Jabri, A.; Limaye, S.; Sharma, S.; Hamade, H.; Mhanna, M.; Aneja, A.; Gandhi, S. Echocardiographic Evaluation of Pulmonary Embolism: A Review. J. Am. Soc. Echocardiogr. 2023, 36, 906–912. [Google Scholar] [CrossRef] [PubMed]
- Saxena, A.; Garan, A.R.; Kapur, N.K.; O’Neill, W.W.; Lindenfeld, J.; Pinney, S.P.; Uriel, N.; Burkhoff, D.; Kern, M. Value of Hemodynamic Monitoring in Patients With Cardiogenic Shock Undergoing Mechanical Circulatory Support. Circulation 2020, 141, 1184–1197. [Google Scholar] [CrossRef] [PubMed]
- Ranka, S.; Mastoris, I.; Kapur, N.K.; Tedford, R.J.; Rali, A.; Acharya, P.; Weidling, R.; Goyal, A.; Sauer, A.J.; Gupta, B.; et al. Right Heart Catheterization in Cardiogenic Shock Is Associated With Improved Outcomes: Insights From the Nationwide Readmissions Database. J. Am. Heart Assoc. 2021, 10, e019843. [Google Scholar] [CrossRef]
- Ardeshna, N.S.; Song, M.; Hyder, S.N.; Grace, K.A.; O’Hare, C.; Schaeffer, W.J.; Stover, M.; Greineder, C.F.; Barnes, G.D. Effect of Pulmonary Embolism Response Team on Advanced Therapies Administered: The University of Michigan Experience. Thromb. Res. 2023, 221, 73–78. [Google Scholar] [CrossRef] [PubMed]
- Ramos-López, N.; Ferrera, C.; Luque, T.; Enríquez-Vázquez, D.; Mahía-Casado, P.; Galván-Herráez, L.; Pedrajas, J.M.; Salinas, P. Impact of a Pulmonary Embolism Response Team Initiative on Hospital Mortality of Patients with Bilateral Pulmonary Embolism. Med. Clin. 2023, 160, 469–475. [Google Scholar] [CrossRef] [PubMed]
- Gorder, K.; Rudick, S.; Smith, T.D. Advocacy and Legislation for Regionalization Practices in the Treatment of Cardiogenic Shock: The Time Is Now. US Cardiol. Rev. 2022, 16, e06. [Google Scholar] [CrossRef]
- Shaefi, S.; O’Gara, B.; Kociol, R.D.; Joynt, K.; Mueller, A.; Nizamuddin, J.; Mahmood, E.; Talmor, D.; Shahul, S. Effect of Cardiogenic Shock Hospital Volume on Mortality in Patients with Cardiogenic Shock. J. Am. Heart Assoc. 2015, 4, e001462. [Google Scholar] [CrossRef]
- Rab, T.; Ratanapo, S.; Kern, K.B.; Basir, M.B.; McDaniel, M.; Meraj, P.; King, S.B., 3rd; O’Neill, W. Cardiac Shock Care Centers: JACC Review Topic of the Week. J. Am. Coll. Cardiol. 2018, 72, 1972–1980. [Google Scholar] [CrossRef]






Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kadri, A.N.; Alrawashdeh, R.; Soufi, M.K.; Elder, A.J.; Elder, Z.; Mohamad, T.; Gnall, E.; Elder, M. Mechanical Support in High-Risk Pulmonary Embolism: Review Article. J. Clin. Med. 2024, 13, 2468. https://doi.org/10.3390/jcm13092468
Kadri AN, Alrawashdeh R, Soufi MK, Elder AJ, Elder Z, Mohamad T, Gnall E, Elder M. Mechanical Support in High-Risk Pulmonary Embolism: Review Article. Journal of Clinical Medicine. 2024; 13(9):2468. https://doi.org/10.3390/jcm13092468
Chicago/Turabian StyleKadri, Amer N., Razan Alrawashdeh, Mohamad K. Soufi, Adam J. Elder, Zachary Elder, Tamam Mohamad, Eric Gnall, and Mahir Elder. 2024. "Mechanical Support in High-Risk Pulmonary Embolism: Review Article" Journal of Clinical Medicine 13, no. 9: 2468. https://doi.org/10.3390/jcm13092468