
A Comparison of Sensorimotor Integration and Motor Fitness Components between Collegiate Athletes with and without Long COVID: A Cross-Sectional Study with Pair-Matched Controls

 , , and
, , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Population
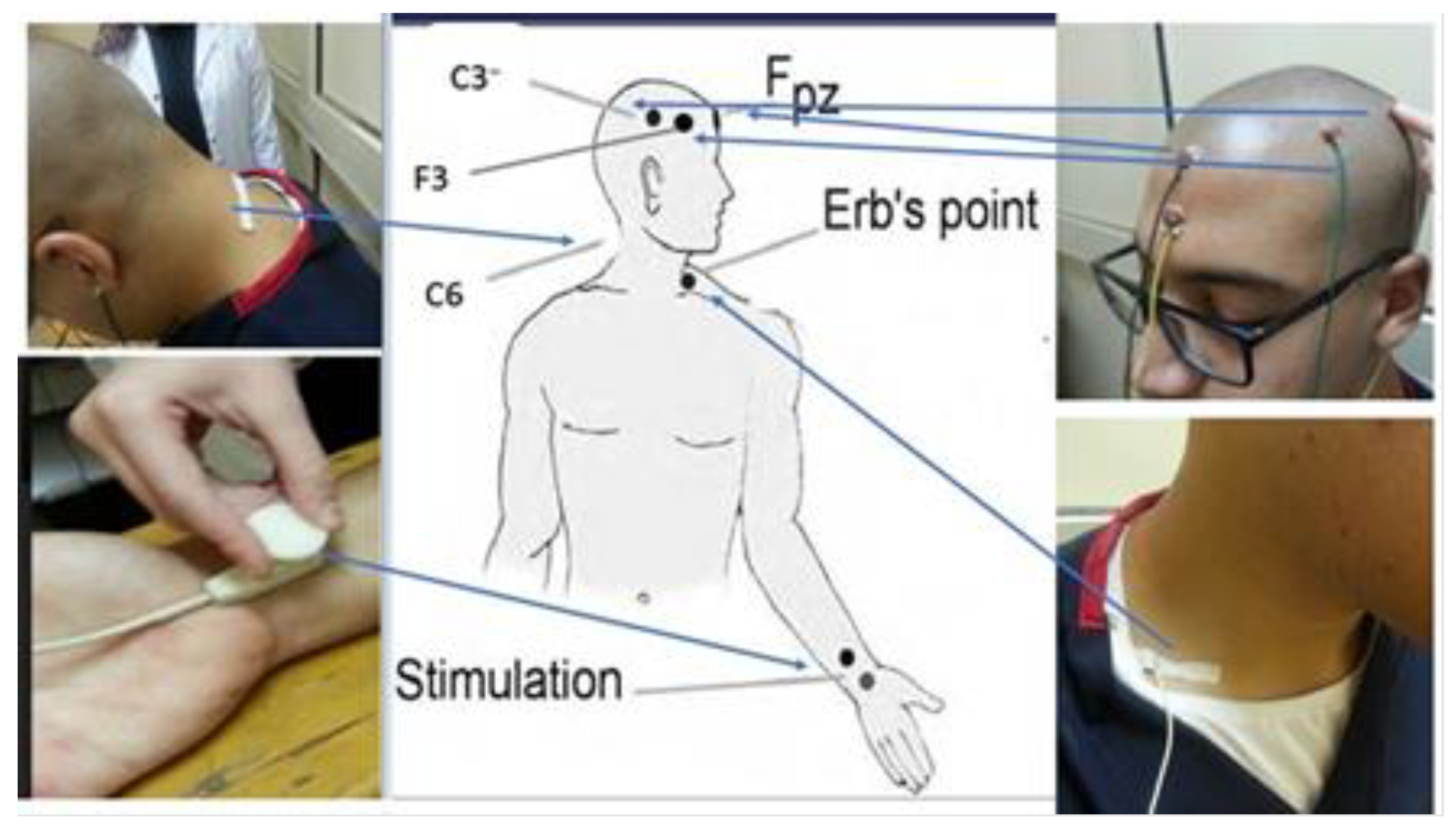
2.2. Evaluation of Sensorimotor Integration and Somatosensory Processing
2.3. Athletic Performances
2.3.1. Agility: T-Test
2.3.2. Leg Power: Non-Countermovement Vertical Jump Test
2.3.3. Static Balance: Stork Static Balance Test
2.3.4. Dynamic Balance: Y-Balance Test or YBT
2.4. Sample Size Determination
2.5. Data Analysis
3. Results
3.1. Participant Demographics and Characteristics
3.2. Inter-Group Analysis
3.3. Correlations between Fatigue Score and Neurophysiological/Motor Fitness Variables in Long COVID
3.4. Correlations between N30 Score and Neurophysiological/Motor Fitness Variables in Long COVID
4. Discussion
4.1. Sensorimotor Integration Differences
4.2. Correlation with Fatigue
4.3. Athletic Performance Differences
4.4. Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Ciotti, M.; Ciccozzi, M.; Terrinoni, A.; Jiang, W.C.; Wang, C.B.; Bernardini, S. The COVID-19 Pandemic. Crit. Rev. Clin. Lab. Sci. 2020, 57, 365–388. [Google Scholar] [CrossRef] [PubMed]
- Sohrabi, C.; Alsafi, Z.; O’Neill, N.; Khan, M.; Kerwan, A.; Al-Jabir, A.; Iosifidis, C.; Agha, R. World Health Organization Declares Global Emergency: A Review of the 2019 Novel Coronavirus (COVID-19). Int. J. Surg. 2020, 76, 71–76. [Google Scholar] [CrossRef] [PubMed]
- Pascarella, G.; Strumia, A.; Piliego, C.; Bruno, F.; Del Buono, R.; Costa, F.; Scarlata, S.; Agrò, F.E. COVID-19 Diagnosis and Management: A Comprehensive Review. J. Intern. Med. 2020, 288, 192–206. [Google Scholar] [CrossRef] [PubMed]
- Yuki, K.; Fujiogi, M.; Koutsogiannaki, S. COVID-19 Pathophysiology: A Review. Clin. Immunol. 2020, 215, 108427. [Google Scholar] [CrossRef]
- Struyf, T.; Deeks, J.J.; Dinnes, J.; Takwoingi, Y.; Davenport, C.; Leeflang, M.M.G.; Spijker, R.; Hooft, L.; Emperador, D.; Domen, J.; et al. Signs and Symptoms to Determine If a Patient Presenting in Primary Care or Hospital Outpatient Settings Has COVID-19. Cochrane Database Syst. Rev. 2022, 2022. [Google Scholar]
- Berentschot, J.C.; Drexhage, H.A.; Mersha, D.G.A.; Wijkhuijs, A.J.M.; GeurtsvanKessel, C.H.; Koopmans, M.P.G.; Voermans, J.; Heijenbrok-Kal, M.H.; Bek, L.M.; Ribbers, G.M.; et al. Severe Fatigue as Symptom of Long COVID Is Characterized by Increased Expression of Inflammatory Genes in Monocytes, Increased Serum pro-Inflammatory Cytokines, and Increased CD8+ T-Lymphocytes: A Putative Dysregulation of the Immune-Brain Axis, the Coagulation Process, and Auto-Inflammation to Explain the Diversity of Long COVID Symptoms. medRxiv 2022. medRxiv:2022.09.15.22279970. [Google Scholar] [CrossRef]
- Stavem, K.; Ghanima, W.; Olsen, M.K.; Gilboe, H.M.; Einvik, G. Prevalence and Determinants of Fatigue after COVID-19 in Non-Hospitalized Subjects: A Population-Based Study. Int. J. Environ. Res. Public Health 2021, 18, 2030. [Google Scholar] [CrossRef] [PubMed]
- Halpin, S.J.; McIvor, C.; Whyatt, G.; Adams, A.; Harvey, O.; McLean, L.; Walshaw, C.; Kemp, S.; Corrado, J.; Singh, R.; et al. Postdischarge Symptoms and Rehabilitation Needs in Survivors of COVID-19 Infection: A Cross-Sectional Evaluation. J. Med. Virol. 2021, 93, 1013–1022. [Google Scholar] [CrossRef] [PubMed]
- Liang, L.; Yang, B.; Jiang, N.; Fu, W.; He, X.; Zhou, Y.; Ma, W.L.; Wang, X. Three-Month Follow-up Study of Survivors of Coronavirus Disease 2019 after Discharge. J. Korean Med. Sci. 2020, 35, e418. [Google Scholar] [CrossRef]
- Guevarra, C.C.; Murray, N.; Cipriani, D.; Mailland, K.; Char, A.; Coffman, K.; Davis, C.; Truong, F.; Danielian, A.; Barnes, G. Cardiovascular Involvement among Collegiate Athletes Following COVID-19 Infection. J. Clin. Transl. Res. 2022, 8, 1. [Google Scholar] [CrossRef]
- Lemes, I.R.; Smaira, F.; José, W.; Ribeiro, D.; Lúcia, A.; Pinto, S.; Smaira, F.I.; Ribeiro, W.J.D.; Favero, N.K.; Nagem, L.D.; et al. Acute and Post-Acute COVID-19 Presentations in Athletes: A Systematic Review and Meta-Analysis. Br. J. Sports Med. 2022, 56, 941–947. [Google Scholar] [CrossRef] [PubMed]
- Lakatos, B.K.; Tokodi, M.; Fábián, A.; Ladányi, Z.; Vágó, H.; Szabó, L.; Sydó, N.; Csulak, E.; Kiss, O.; Babity, M.; et al. Frequent Constriction-Like Echocardiographic Findings in Elite Athletes Following Mild COVID-19: A Propensity Score-Matched Analysis. Front. Cardiovasc. Med. 2021, 8, 760651. [Google Scholar] [CrossRef] [PubMed]
- Radin, J.M.; Quer, G.; Ramos, E.; Baca-Motes, K.; Gadaleta, M.; Topol, E.J.; Steinhubl, S.R. Assessment of Prolonged Physiological and Behavioral Changes Associated with COVID-19 Infection. JAMA Netw. Open 2021, 4, e2115959. [Google Scholar] [CrossRef] [PubMed]
- Reiss, A.B.; Greene, C.; Dayaramani, C.; Rauchman, S.H.; Stecker, M.M.; De Leon, J.; Pinkhasov, A. Long COVID, the Brain, Nerves, and Cognitive Function. Neurol. Int. 2023, 15, 821–841. [Google Scholar] [CrossRef] [PubMed]
- Ahmad, S.J.; Feigen, C.M.; Vazquez, J.P.; Kobets, A.J.; Altschul, D.J. Neurological Sequelae of COVID-19. J. Integr. Neurosci. 2022, 21, 77. [Google Scholar] [CrossRef] [PubMed]
- Maury, A.; Lyoubi, A.; Peiffer-Smadja, N.; de Broucker, T.; Meppiel, E. Neurological Manifestations Associated with SARS-CoV-2 and Other Coronaviruses: A Narrative Review for Clinicians. Rev. Neurol. 2021, 177, 51–64. [Google Scholar] [CrossRef] [PubMed]
- Luvizutto, G.J.; Bazan, R. Electrophysiological and Neuroimaging Tools to Evaluate Neurological Symptoms, Manifestations, and Complications in Patients with Long COVID-19. Neurol. Neurochir. Pol. 2023, 57, 8–10. [Google Scholar] [CrossRef] [PubMed]
- Williams, S.; Wynford-Thomas, R.; Robertson, N.P. Long-COVID: Neurological Manifestations and Management. J. Neurol. 2021, 268, 4915. [Google Scholar] [CrossRef]
- Branscheidt, M.; Kassavetis, P.; Anaya, M.; Rogers, D.; Huang, H.D.; Lindquist, M.A.; Celnik, P. Fatigue Induces Long-Lasting Detrimental Changes in Motor-Skill Learning. Elife 2019, 8, e40578. [Google Scholar] [CrossRef]
- Tanaka, M.; Watanabe, Y. Neural Compensation Mechanisms to Regulate Motor Output during Physical Fatigue. Brain Res. 2011, 1395, 46–52. [Google Scholar] [CrossRef]
- Moustafa, I.; Kim, M.; Harrison, D.E. Comparison of Sensorimotor Integration and Skill-Related Physical Fitness Components Between College Athletes with and Without Forward Head Posture. J. Sport. Rehabil. 2023, 32, 53–62. [Google Scholar] [CrossRef] [PubMed]
- Podrihalo, O.; Jagiello, W.; Xiaohong, G.; Podrigalo, L.; Yermakova, T.; Cieslicka, M. Sensory Integration Research: Priority Scientific Directions Based on the Analysis of Web of Science Core Collection Resources. Phys. Educ. Stud. 2023, 27, 358–377. [Google Scholar] [CrossRef]
- Machado, S.; Cunha, M.; Velasques, B.; Minc, D.; Teixeira, S.; Domingues, C.A.; Silva, J.G.; Bastos, V.H.; Budde, H.; Cagy, M.; et al. Sensorimotor Integration: Basic Concepts, Abnormalities Related to Movement Disorders and Sensorimotor Training-Induced Cortical Reorganization. Rev. Neurol. 2010, 51, 427–436. [Google Scholar] [CrossRef] [PubMed]
- Machado, D.; Bastos, V.H.; Cunha, M.; Velasques, B.; Machado, S.; Basile, L.; Cagy, M.; Piedade, R.; Ribeiro, P. Efectos Del Bromacepam En El Desarrollo de Una Actividad Sensoriomotora: Un Estudio Electroencefalográfico. Rev. Neurol. 2009, 49, 295–299. [Google Scholar] [CrossRef] [PubMed]
- Krakauer, J.W.; Mazzoni, P.; Ghazizadeh, A.; Ravindran, R.; Shadmehr, R. Generalization of Motor Learning Depends on the History of Prior Action. PLoS Biol. 2006, 4, e316. [Google Scholar] [CrossRef] [PubMed]
- Grosso, M.J.; Hwang, R.; Mroz, T.; Benzel, E.; Steinmetz, M.P. Relationship between Degree of Focal Kyphosis Correction and Neurological Outcomes for Patients Undergoing Cervical Deformity Correction Surgery. J. Neurosurg. Spine 2013, 18, 537–544. [Google Scholar] [CrossRef] [PubMed]
- Smith, J.S.; Lafage, V.; Ryan, D.J.; Shaffrey, C.I.; Schwab, F.J.; Patel, A.A.; Brodke, D.S.; Arnold, P.M.; Riew, K.D.; Traynelis, V.C.; et al. Association of Myelopathy Scores with Cervical Sagittal Balance and Normalized Spinal Cord Volume. Spine 2013, 38, S161–S170. [Google Scholar] [CrossRef] [PubMed]
- Diab, A.M.; Harrison, D.E.; Moustafa, I.M.; Attiah, A.; Diab, M.; Harrison, D.E. Does Forward Head Posture Influence Somatosensory Evoked Potentials and Somatosensory Processing in Asymptomatic Young Adults? J. Clin. Med. 2023, 12, 3217. [Google Scholar] [CrossRef]
- Goss, M.; Bernal, R.; Patel, V.N.; Li, K.; Garbarino, V.R.; Nair, R.R.; Snyder, H.M.; de Erausquin, G.A.; Ganguli, M.; Snitz, B.E.; et al. COVID-19 May Have a Detrimental Impact on Sensorimotor Function. Alzheimer’s Dement. 2023, 19, e083191. [Google Scholar] [CrossRef]
- Sobreira, M.; Almeida, M.P.; Gomes, A.; Lucas, M.; Oliveira, A.; Marques, A. Minimal Clinically Important Differences for Measures of Pain, Lung Function, Fatigue, and Functionality in Spinal Cord Injury. Phys. Ther. 2021, 101, pzaa210. [Google Scholar] [CrossRef]
- Blevins, C.A.; Weathers, F.W.; Davis, M.T.; Witte, T.K.; Domino, J.L. The Posttraumatic Stress Disorder Checklist for DSM-5 (PCL-5): Development and Initial Psychometric Evaluation. J. Trauma. Stress 2015, 28, 489–498. [Google Scholar] [CrossRef] [PubMed]
- Beck, A.T.; Guth, D.; Steer, R.A.; Ball, R. Screening for Major Depression Disorders in Medical Inpatients with the Beck Depression Inventory for Primary Care. Behav. Res. Ther. 1997, 35, 785–791. [Google Scholar] [CrossRef] [PubMed]
- Abu El Kasem, S.T.; Kattabie, O.M.; Raoof, N.A.A.; Moustafa, I.M. Effect of forward Head Posture on Sensorimotor Integration. Int. J. Physiother. 2017, 4, 118–125. [Google Scholar] [CrossRef]
- Moustafa, I.M.; Diab, A.; Shousha, T.; Raigangar, V.; Harrison, D.E. Sensorimotor Integration, Cervical Sensorimotor Control, and Cost of Cognitive-Motor Dual Tasking: Are There Differences in Patients with Chronic Whiplash-Associated Disorders and Chronic Idiopathic Neck Pain Compared to Healthy Controls? Eur. Spine J. 2022, 31, 3452–3461. [Google Scholar] [CrossRef] [PubMed]
- Electrodiagnostic Medicine-2nd Edition. Available online: https://www.elsevier.com/books/electrodiagnostic-medicine/dumitru/978-1-56053-433-4 (accessed on 30 December 2021).
- Tinazzi, M.; Fiaschi, A.; Rosso, T.; Faccioli, F.; Grosslercher, J.; Aglioti, S.M. Neuroplastic Changes Related to Pain Occur at Multiple Levels of the Human Somatosensory System: A Somatosensory-Evoked Potentials Study in Patients with Cervical Radicular Pain. J. Neurosci. 2000, 20, 9277–9283. [Google Scholar] [CrossRef] [PubMed]
- Desmedt, J.E.; Cheron, G. Prevertebral (Oesophageal) Recording of Subcortical Somatosensory Evoked Potentials in Man: The Spinal P13 Component and the Dual Nature of the Spinal Generators. Electroencephalogr. Clin. Neurophysiol. 1981, 52, 257–275. [Google Scholar] [CrossRef] [PubMed]
- Allison, T.; McCarthy, G.; Wood, C.C.; Jones, S.J. Potentials Evoked in Human and Monkey Cerebral Cortex by Stimulation of the Median Nerve. A Review of Scalp and Intracranial Recordings. Brain 1991, 114, 2465–2503. [Google Scholar] [CrossRef] [PubMed]
- Mauguière, F.; Desmedt, J.E.; Courjon, J. Astereognosis and Dissociated Loss of Frontal or Parietal Components of Somatosensory Evoked Potentials in Hemispheric Lesions. Detailed Correlations with Clinical Signs and Computerized Tomographic Scanning. Brain 1983, 106 Pt 2, 271–311. [Google Scholar] [CrossRef] [PubMed]
- Nuwer, M.R.; Aminoff, M.; Desmedt, J.; Eisen, A.A.; Goodin, D.; Matsuoka, S.; Mauguière, F.; Shibasaki, H.; Sutherling, W.; Vibert, J.F. IFCN Recommended Standards for Short Latency Somatosensory Evoked Potentials. Report of an IFCN Committee. International Federation of Clinical Neurophysiology. Electroencephalogr. Clin. Neurophysiol. 1994, 91, 6–11. [Google Scholar] [CrossRef]
- Kang, S.Y.; Ma, H.-I. N30 Somatosensory Evoked Potential Is Negatively Correlated with Motor Function in Parkinson’s Disease. J. Mov. Disord. 2016, 9, 35–39. [Google Scholar] [CrossRef]
- Cebolla, A.M.; Palmero-Soler, E.; Dan, B.; Cheron, G. Frontal Phasic and Oscillatory Generators of the N30 Somatosensory Evoked Potential. Neuroimage 2011, 54, 1297–1306. [Google Scholar] [CrossRef]
- Desmedt, J.E.; Nguyen, T.H.; Bourguet, M. Bit-Mapped Color Imaging of Human Evoked Potentials with Reference to the N20, P22, P27 and N30 Somatosensory Responses. Electroencephalogr. Clin. Neurophysiol. 1987, 68, 1–19. [Google Scholar] [CrossRef]
- Waberski, T.D.; Buchner, H.; Perkuhn, M.; Gobbelé, R.; Wagner, M.; Kücker, W.; Silny, J. N30 and the Effect of Explorative Finger Movements: A Model of the Contribution of the Motor Cortex to Early Somatosensory Potentials. Clin. Neurophysiol. 1999, 110, 1589–1600. [Google Scholar] [CrossRef]
- Kaňovský, P.; Bareš, M.; Rektor, I. The Selective Gating of the N30 Cortical Component of the Somatosensory Evoked Potentials of Median Nerve Is Different in the Mesial and Dorsolateral Frontal Cortex: Evidence from Intracerebral Recordings. Clin. Neurophysiol. 2003, 114, 981–991. [Google Scholar] [CrossRef]
- Muzyka, I.M.; Estephan, B. Somatosensory Evoked Potentials. In Handbook of Clinical Neurology; Elsevier: Amsterdam, The Netherlands, 2019; Volume 160, pp. 523–540. [Google Scholar] [CrossRef]
- Ben Hassen, S.; Negra, Y.; Uthoff, A.; Chtara, M.; Jarraya, M. Reliability, Validity, and Sensitivity of a Specific Agility Test and Its Relationship with Physical Fitness in Karate Athletes. Front. Physiol. 2022, 13, 841498. [Google Scholar] [CrossRef]
- Venegas-Carro, M.; Kramer, A.; Moreno-Villanueva, M.; Gruber, M. Test–Retest Reliability and Sensitivity of Common Strength and Power Tests over a Period of 9 Weeks. Sports 2022, 10, 171. [Google Scholar] [CrossRef]
- Curnow, D.; Cobbin, D.; Wyndham, J. Reliability of the Stork Test: Is Starting Stance Important? Chiropr. J. Aust. 2010, 40, 137–141. [Google Scholar]
- Greenberg, E.T.; Barle, M.; Glassmann, E.; Jung, M.K. Interrater and test-retest reliability of the y balance test in healthy, early adolescent female athletes. Int. J. Sports Phys. Ther. 2019, 14, 204–213. [Google Scholar] [CrossRef]
- Wasaka, T.; Kakigi, R. Sensorimotor Integration: The Somatosensory System and Voluntary Movement. In Magnetoencephalography: From Signals to Dynamic Cortical Networks, 2nd ed.; Springer International Publishing: New York, NY, USA, 2019; pp. 957–975. ISBN 9783030000875. [Google Scholar]
- Dancey, E.; Murphy, B.; Srbely, J.; Yielder, P. The Effect of Experimental Pain on Motor Training Performance and Sensorimotor Integration. Exp. Brain Res. 2014, 232, 2879–2889. [Google Scholar] [CrossRef]
- Taylor, H.H.; Murphy, B. Altered Sensorimotor Integration with Cervical Spine Manipulation. J. Manip. Physiol. Ther. 2008, 31, 115–126. [Google Scholar] [CrossRef] [PubMed]
- Kuppuswamy, A. The Neurobiology of Pathological Fatigue: New Models, New Questions. Neuroscientist 2021, 28, 238–253. [Google Scholar] [CrossRef] [PubMed]
- Palotai, M.; Cavallari, M.; Koubiyr, I.; Morales Pinzon, A.; Nazeri, A.; Healy, B.C.; Glanz, B.; Weiner, H.L.; Chitnis, T.; Guttmann, C.R.G. Microstructural Fronto-Striatal and Temporo-Insular Alterations Are Associated with Fatigue in Patients with Multiple Sclerosis Independent of White Matter Lesion Load and Depression. Mult. Scler. J. 2020, 26, 1708–1718. [Google Scholar] [CrossRef] [PubMed]
- De Doncker, W.; Dantzer, R.; Ormstad, H.; Kuppuswamy, A. Mechanisms of Poststroke Fatigue. J. Neurol. Neurosurg. Psychiatry 2018, 89, 287–293. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variable | Long COVID (n = 60) | Control (n = 60) |
|---|---|---|
| Age (years) | 21 ± 2 | 21 ± 1.5 |
| BMI | 18.8 ± 1 | 18.9 ± 1.2 |
| Gender | ||
| Male | 20 | 20 |
| Female | 40 | 40 |
| Type of Sport, percentage (%) | ||
| Handball | 10 (16.7) | 8 (13.3) |
| Volleyball | 12 (20) | 11 (18.3) |
| Football | 16 (26.7) | 18 (30) |
| Basketball | 12 (20) | 12 (20) |
| Swimming | 10 (26.7) | 11 (18.3) |
| Smoking/tobacco product consumption | ||
| Yes | 9 | 5 |
| No | 51 | 55 |
| Weeks since symptom onset or diagnosis of COVID-19 | 24 ± 5 | - |
| P14 (µV) | 1.71 ± 0.23 | 1.1 ± 0.24 |
| N20 (µV) | 2.6 ±.5 | 1.8 ± 0.9 |
| P27 (µV) | 2.4 ± 0.43 | 1.8 ± 0.37 |
| N30 (µV) | 2.9 ± 0.51 | 2 ± 0.41 |
| N13 (µV) | 1.5 ± 0.3 | 1 ± 0.2 |
| T-test agility (s) | 8.81 ± 1.3 | 7.4 ± 1.2 |
| Leg power (cm) | 37.28 ± 4.3 | 41.14 ± 4.6 |
| Stork static balance test (s) | 55.5 ± 6.3 | 61.8 ± 4.3 |
| Y-Balance Test (CS)a | 88.2 ± 6.5 | 93.5 ± 7 |
| Fatigue score | 38 ± 2 | - |
| Measure of Neurophysiological Outcome | Mean Difference between the Two Groups | SEM | (95% CI) | Cohen’s d | p-Value |
|---|---|---|---|---|---|
| P14 (µV) | 0.60 | 0.04 | [0.6, 0.5] | 2.7 | <0.005 |
| N20 (µV) | 0.8 | 0.13 | [1.1, 0.5] | 1.09 | <0.005 |
| P27 (µV) | 0.6 | 0.07 | [0.7, 0.45] | 1.7 | <0.005 |
| N30 (µV) | 0.9 | 0.08 | [1.06, 0.7] | 1.9 | <0.005 |
| N13 (µV) | 0.5 | 0.04 | [0.59, 0.41] | 1.9 | <0.005 |
| T-test agility (s) | 1.4 | 0.2 | [1.8, 0.9] | 1.1 | <0.005 |
| Leg power (cm) | −3.9 | 0.8 | [−2.3, −5.4] | 0.8 | <0.005 |
| Stork static balance test (s) | −6.3 | 0.9 | [−4.3, −8.2] | 1.16 | <0.005 |
| Y-Balance Test (CS)a | −5.5 | 1.2 | [−2.8, −7.7] | 0.9 | <0.005 |
| Correlation | Long COVID Group r (p-Value) |
|---|---|
| N13 (µV) | 0.49 <0.001 |
| P14 (µV) | 0.57 <0.001 |
| N20 (µV) | 0.61 <0.001 |
| P27 (µV) | 0.48 <0.001 |
| N30 (µV) | 0.61 <0.001 |
| T-test agility (s) | 0.21 0.08 |
| Leg power (cm) | −0.24 0.07 |
| Stork static balance test (s) | −0.1 0.09 |
| Y-Balance Test (CS)a | −0.11 0.09 |
| Correlation | Long COVID Group r (p-Value) N30 | Matched Control Group r (p-Value) N30 |
|---|---|---|
| T-test agility (s) | 0.57 <0.001 | −51 <0.001 |
| Leg power (cm) | −0.51 <0.001 | −0.48 <0.001 |
| Stork static balance test (s) | −0.67 <0.001 | −0.5 <0.001 |
| Y-Balance Test (CS)a | −0.66 <0.001 | 0.49 <0.001 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Moustafa, I.M.; Ahbouch, A.; Kader, R.P.; Shousha, T.M.; Alrahoomi, A. A Comparison of Sensorimotor Integration and Motor Fitness Components between Collegiate Athletes with and without Long COVID: A Cross-Sectional Study with Pair-Matched Controls. J. Clin. Med. 2024, 13, 2469. https://doi.org/10.3390/jcm13092469
Moustafa IM, Ahbouch A, Kader RP, Shousha TM, Alrahoomi A. A Comparison of Sensorimotor Integration and Motor Fitness Components between Collegiate Athletes with and without Long COVID: A Cross-Sectional Study with Pair-Matched Controls. Journal of Clinical Medicine. 2024; 13(9):2469. https://doi.org/10.3390/jcm13092469
Chicago/Turabian StyleMoustafa, Ibrahim M., Amal Ahbouch, Raheesa P. Kader, Tamer Mohamed Shousha, and Abdulla Alrahoomi. 2024. "A Comparison of Sensorimotor Integration and Motor Fitness Components between Collegiate Athletes with and without Long COVID: A Cross-Sectional Study with Pair-Matched Controls" Journal of Clinical Medicine 13, no. 9: 2469. https://doi.org/10.3390/jcm13092469