Propensity Score-Matched Analysis of Perioperative Outcomes of Supine versus Prone Percutaneous Nephrolithotomy

 , and
, and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Patient Selection
2.2. Surgical Techniques
2.3. Measurements and Outcomes
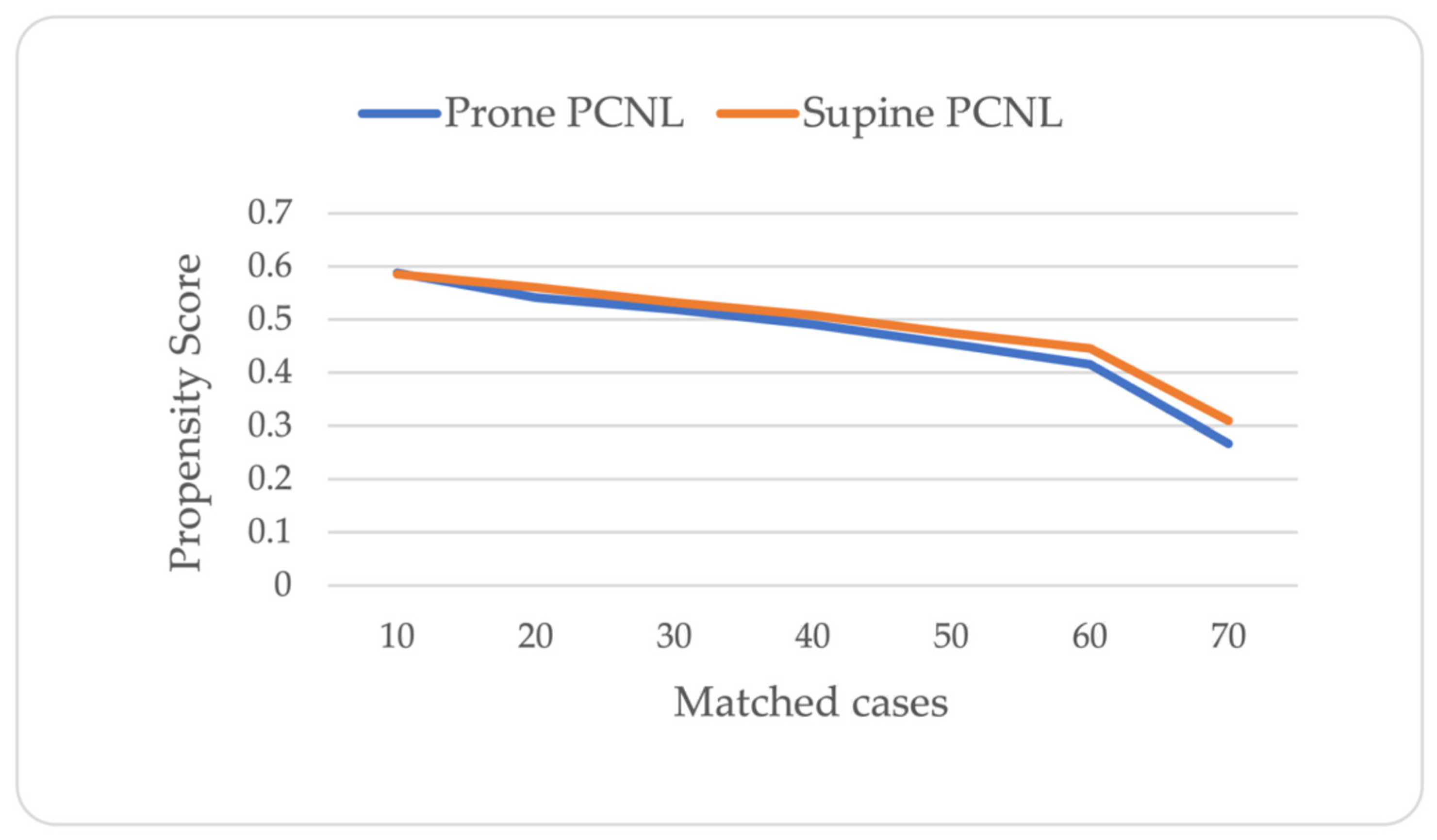
2.4. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Fernström, I.; Johansson, B. Percutaneous pyelolithotomy. Scand. J. Urol. Nephrol. 1976, 10, 257–259. [Google Scholar] [CrossRef] [PubMed]
- Mak, D.K.-C.; Smith, Y.; Buchholz, N.; El-Husseiny, T. What is better in percutaneous nephrolithotomy—Prone or supine? A systematic review. Arab. J. Urol. 2016, 14, 101–107. [Google Scholar] [CrossRef] [PubMed]
- Uria, J.G.V.; Gerhold, J.V.; Lopez, J.A.L.; Rodriguez, S.V.; Navarro, C.A.; Fabian, M.R.; Bazalo, J.M.R.; Elipe, M.A.S. Technique and complications of percutaneous nephroscopy: Experience with 557 patients in the supine position. J. Urol. 1998, 160, 1975–1978. [Google Scholar] [CrossRef]
- Giusti, G.; Proietti, S.; Pasin, L.; Casiraghi, G.M.; Gadda, G.M.; Rosso, M.; Kinzikeeva, E.; Doizi, S.; Gaboardi, F.; Traxer, O. Simultaneous bilateral endoscopic manipulation for bilateral renal stones. Urology 2016, 94, 265–269. [Google Scholar] [CrossRef] [PubMed]
- Vicentini, F.C.; Mazzucchi, E.; Gökçe, M.I.; Sofer, M.; Tanidir, Y.; Sener, T.E.; Melo, P.A.d.S.; Eisner, B.H.; Batter, T.H.; Chi, T.; et al. Percutaneous nephrolithotomy in horseshoe kidneys: Results of a multicentric study. J. Endourol. 2021, 35, 979–984. [Google Scholar] [CrossRef] [PubMed]
- Melo, P.A.D.S.; Vicentini, F.C.; Perrella, R.; Murta, C.B.; Claro, J.F.D.A. Comparative study of percutaneous nephrolithotomy performed in the traditional prone position and in three different supine positions. Int. Braz. J. Urol. 2019, 45, 108–117. [Google Scholar] [CrossRef] [PubMed]
- Valdivia, J.G.; Scarpa, R.M.; Duvdevani, M.; Gross, A.J.; Nadler, R.B.; Nutahara, K.; de la Rosette, J.J.M.C.H.; on behalf of the CROES PCNL Study Group. Supine versus prone position during percutaneous nephrolithotomy: A report from the Clinical Research Office of the Endourological Society Percutaneous Nephrolithotomy Global Study. J. Endourol. 2011, 25, 1619–1625. [Google Scholar] [CrossRef] [PubMed]
- Perrella, R.; Vicentini, F.C.; Paro, E.D.; Torricelli, F.C.M.; Marchini, G.S.; Danilovic, A.; Batagello, C.A.; Mota, P.K.V.; Ferreira, D.B.; Cohen, D.J.; et al. Supine versus prone percutaneous nephrolithotomy for complex stones: A multicenter randomized controlled trial. J. Urol. 2022, 207, 647–656. [Google Scholar] [CrossRef] [PubMed]
- Shoshany, O.; Margel, D.; Finz, C.; Ben-Yehuda, O.; Livne, P.M.; Holand, R.; Lifshitz, D. Percutaneous nephrolithotomy for infection stones: What is the risk for postoperative sepsis? A retrospective cohort study. Urolithiasis 2015, 43, 237–242. [Google Scholar] [CrossRef] [PubMed]
- Smith, A.; Averch, T.D.; Shahrour, K.; Opondo, D.; Daels, F.P.; Labate, G.; Turna, B.; de la Rosette, J.J.M.C.H.; CROES PCNL Study Group. A nephrolithometric nomogram to predict treatment success of percutaneous nephrolithotomy. J. Urol. 2013, 190, 149–156. [Google Scholar] [CrossRef] [PubMed]
- Thomas, K.; Smith, N.C.; Hegarty, N.; Glass, J.M. The Guy’s stone score—Grading the complexity of percutaneous nephrolithotomy procedures. Urology 2011, 78, 277–281. [Google Scholar] [CrossRef] [PubMed]
- Kamphuis, G.M.; Baard, J.; Westendarp, M.; De La Rosette, J.J.M.C.H. Lessons learned from the CROES percutaneous nephrolithotomy global study. World J. Urol. 2015, 33, 223–233. [Google Scholar] [CrossRef] [PubMed]
- Keller, E.X.; DE Coninck, V.; Proietti, S.; Talso, M.; Emiliani, E.; Ploumidis, A.; Mantica, G.; Somani, B.; Traxer, O.; Scarpa, R.M.; et al. European Association of Urology—European Society of Residents in Urology (EAU-ESRU). Prone versus supine percutaneous nephrolithotomy: A systematic review and meta-analysis of current literature. Minerva Urol. Nephrol. 2021, 73, 50–58. [Google Scholar] [CrossRef] [PubMed]
- de la Rosette, J.J.; Opondo, D.; Daels, F.P.J.; Giusti, G.; Serrano, A.; Kandasami, S.V.; Wolf, J.S., Jr.; Grabe, M.; on behalf of the CROES PCNL Study Group. Categorisation of complications and validation of the Clavien score for percutaneous nephrolithotomy. Eur. Urol. 2012, 62, 246–255. [Google Scholar] [CrossRef] [PubMed]
- Shoma, A.M.; Elshal, A.M. Nephrostomy tube placement after percutaneous nephrolithotomy: Critical evaluation through a prospective randomized study. Urology 2012, 79, 771–776. [Google Scholar] [CrossRef] [PubMed]
- Falahatkar, S.; Moghaddam, K.G.; Kazemnezhad, E.; Farzan, A.; Aval, H.B.; Ghasemi, A.; Shahab, E.; Esmaeili, S.S.; Motiee, R.; Langroodi, S.A.M.; et al. Factors affecting complications according to the modified Clavien classification in complete supine percutaneous nephrolithotomy. Can. Urol. Assoc. J. 2015, 9, e83–e92. [Google Scholar] [CrossRef] [PubMed]
- EAU Guidelines. Edn. Presented at the EAU Annual Congress Paris 2024. ISBN 978-94-92671-23-3. Available online: https://uroweb.org/guidelines/urolithiasis/chapter/guidelines (accessed on 15 April 2024).
- Miçooğullari, U.; Kamaci, D.; Yildizhan, M.; Kiliç, F.U.; Çetin, T.; Çakici, U.; Keske, M.; Yalçin, M.Y.; Ardiçoğlu, A. Prone versus Barts “flank-free” modified supine percutaneous nephrolithotomy: A match-pair analysis. Turk. J. Med. Sci. 2021, 51, 1373–1379. [Google Scholar] [CrossRef] [PubMed]
- Ozdemir, H.; Erbin, A.; Sahan, M.; Savun, M.; Cubuk, A.; Yazici, O.; Akbulut, M.F.; Sarilar, O. Comparison of supine and prone miniaturized percutaneous nephrolithotomy in the treatment of lower pole, middle pole, and renal pelvic stones: A matched pair analysis. Int. Braz. J. Urol. 2019, 45, 956–964. [Google Scholar] [CrossRef] [PubMed]
- Chow, A.K.; Ogawa, S.; Seigel, C.; Sands, K.G.; Vetter, J.; Desai, A.; Venkatesh, R.J. Evaluation of perirenal anatomic landmarks on computed tomography to reduce the risk of thoracic complications during supracostal percutaneous nephrolithotomy. J. Endourol. 2021, 35, 589–595. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Variable | Supine PCNL (n = 70) | Prone PCNL (n = 70) | Total Cohort (n = 140) | p-Value |
|---|---|---|---|---|
| Age (yr), mean ± SD | 54.3 ± 14.0 | 55.5 ± 13.8 | 54.9 ± 13.9 | 0.618 |
| Gender, n (%) | 0.493 | |||
| Male | 43 (52.4) | 39 (47.6) | 82 (58.7) | |
| Female | 27 (46.6) | 31 (53.4) | 58 (41.42) | |
| BMI (Kg/m2), mean ± SD | 29.0 ± 5.4 | 28.6 ± 6.6 | 28.8 ± 6.0 | 0.674 |
| GFR (mL/min), mean ± SD | 109.2 ± 39.8 | 111.0 ± 13.7 | 110.1 ± 36.6 | 0.773 |
| Stone burden (mm2), mean ± SD | 239.6 ± 116.5 | 266.0 ± 145.2 | 252.8 ± 131.4 | 0.237 |
| Side (left), n (%) | 47 (67.1) | 38 (54.3) | 85 (60.7) | 0.166 |
| Stone Score | Supine PCNL (n = 70) | Prone PCNL (n = 70) | Total Cohort (n = 140) | p-Value |
|---|---|---|---|---|
| Grade I, n (%) | 30 (42.8) | 33 (47.2) | 63 (45) | 0.749 |
| Grade II, n (%) | 30 (42.9) | 29 (41.4) | 59 (42.1) | |
| Grade III, n (%) | 9 (12.8 | 8 (11.4) | 17 (12.1) | |
| Grade IV, n (%) | 1 (1.4) | 0 | 1 (0.7) |
| Covariate | Supine PCNL (n = 70) | Prone PCNL (n = 70) | Total Cohort (n = 140) | p-Value |
|---|---|---|---|---|
| Operative time (min), mean ± SD | 85.5 ± 25.2 | 96.4 ± 25.8 | 91.0 ± 26.0 | 0.012 |
| Change in hemoglobin (g/dl), mean ± SD | 1.7 ± 1.5 | 1.2 ± 1.1 | 1.4 ± 1.3 | 0.026 |
| Change in hematocrit (%) mean ± SD | 5.6 ± 4.2 | 4.4 ± 3.8 | 5.0 ± 4.0 | 0.063 |
| Infracostal percutaneous access, n (%) | 60 (85.7) | 47 (67.1) | 107 (76.4) | 0.016 |
| Complications, n (%) | 6 (8.6) | 3 (4.3) | 9 (6.4) | 0.301 |
| Fever | 1 (1.4) | 3 (4.3) | 4 (2.9) | 0.310 |
| Need for blood transfusion | 5 (7.1) | Nil | 5 (3.6) | 0.023 |
| Stone-free rate, n (%) | 52 (74.3) | 46 (65.7) | 98 (70.0) | 0.268 |
| Stone-free rate with residual (≤2 mm) fragments, n (%) | 57 (81.4) | 56 (80.0) | 113 (80.7) | 0.830 |
| Outcome Measure | Odds Ratio | 95% Confidence Interval | p-Value |
|---|---|---|---|
| Stone-free rate | 0.88 | 0.39–1.91 | 0.855 |
| Stone-free rate with residual (≤2 mm) fragments | 1.10 | 0.42–2.88 | 1.000 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Babaoff, R.; Creiderman, G.; Darawsha, A.E.; Ehrlich, Y.; Somani, B.; Lifshitz, D.A. Propensity Score-Matched Analysis of Perioperative Outcomes of Supine versus Prone Percutaneous Nephrolithotomy. J. Clin. Med. 2024, 13, 2492. https://doi.org/10.3390/jcm13092492
Babaoff R, Creiderman G, Darawsha AE, Ehrlich Y, Somani B, Lifshitz DA. Propensity Score-Matched Analysis of Perioperative Outcomes of Supine versus Prone Percutaneous Nephrolithotomy. Journal of Clinical Medicine. 2024; 13(9):2492. https://doi.org/10.3390/jcm13092492
Chicago/Turabian StyleBabaoff, Roi, Gherman Creiderman, Abd Elhalim Darawsha, Yaron Ehrlich, Bhaskar Somani, and David A. Lifshitz. 2024. "Propensity Score-Matched Analysis of Perioperative Outcomes of Supine versus Prone Percutaneous Nephrolithotomy" Journal of Clinical Medicine 13, no. 9: 2492. https://doi.org/10.3390/jcm13092492