
TaKeTiNa Music Therapy for Outpatient Treatment of Depression: Study Protocol for a Randomized Clinical Trial
 , , , , and
, , , , and
Abstract
:1. Background
2. Materials and Methods
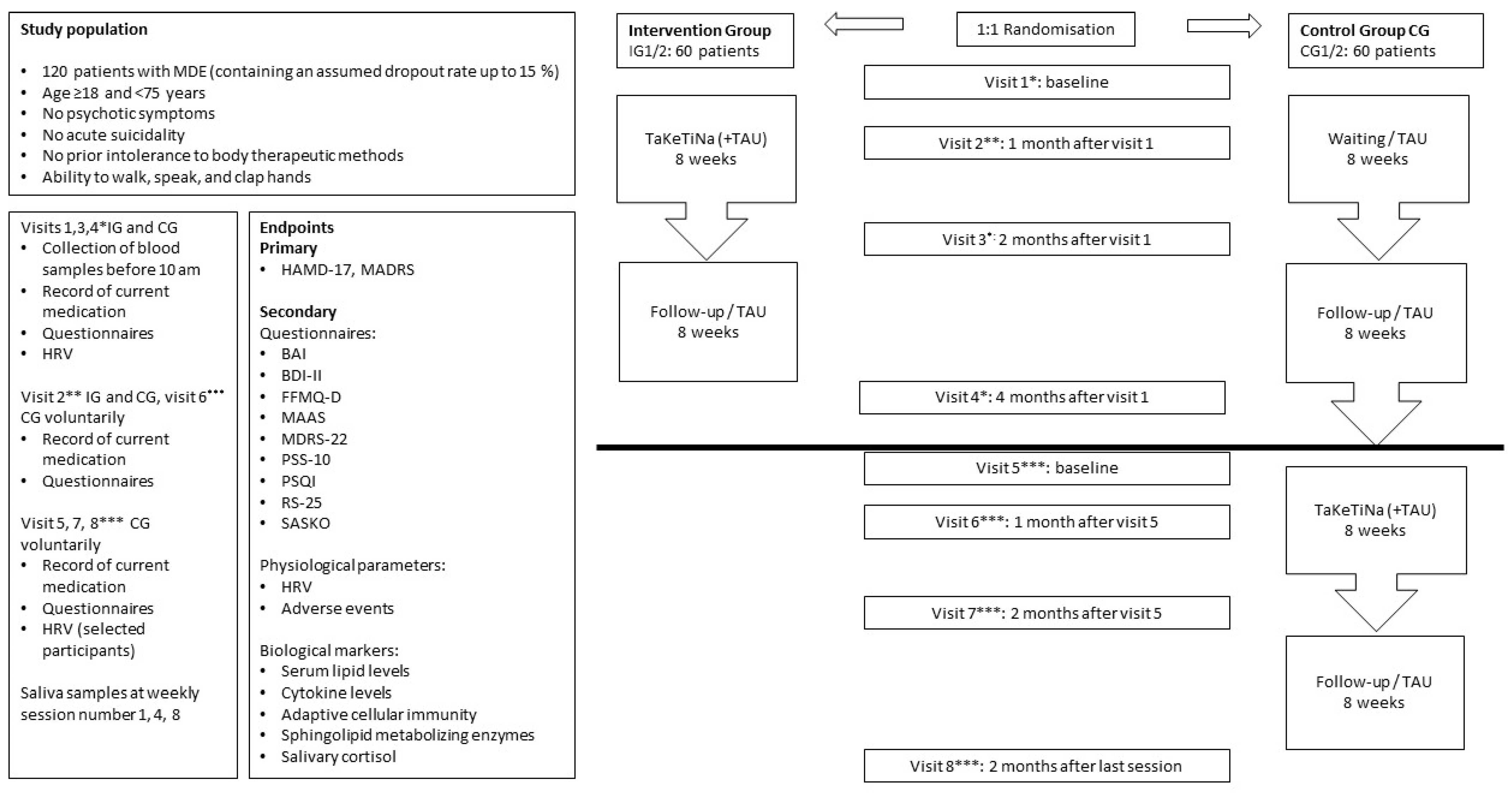
2.1. Study Design
2.2. Objectives
- To investigate the effects of TaKeTiNa music therapy on depression scores and blood-based parameters, especially LDL cholesterol, in patients with depression.
- To identify the modifying factors of therapy response, such as anxiety, resilience, and mindfulness.
- To investigate the relationships between depression-related physiological markers, such as HRV, and biological markers, including immune-system-based biomarkers, lipids, and sphingolipids.
- TaKeTiNa results in a significant decrease in depression severity due to the intervention (from before visit 1 to visit 3 after 8 weeks of therapy) (combined IG1 and IG2 groups).
- TaKeTiNa results in significantly stronger pre-to-postintervention depression severity decrease (visit 1 to visit 3) in the IG1/IG2 group compared to the CG1/CG2 group.
- The antidepressive effect of TaKeTiNa postintervention is stable over eight weeks (from visit 3 to visit 4).
- Depressed patients with higher LDL cholesterol also show higher cortisol levels.
- A higher LDL cholesterol level and higher acid sphingomyelinase activity in depressed patients predict greater symptom reduction with (additional) non-pharmacological treatment strategies such as TaKeTiNa.
- TaKeTiNa significantly reduces salivary cortisol levels in depressed patients.
- TaKeTiNa significantly reduces proinflammatory cytokines in depressed patients.
- The HRV at baseline is inversely correlated with the depression severity score and improves during treatment.
2.3. Participants
2.4. Eligibility Criteria
2.5. Sample Size
2.6. Randomization/Blinding
2.7. Intervention—TaKeTiNa Music Therapy
- Introduction: A brief explanation of the purpose of the session is provided. After that, the teacher introduces the topic (Supplementary Materials List S1) of the session that the participants should pay attention to and to refer to during the rhythmic process.
- Building the rhythmic foundation: The teacher chooses a TaKeTiNa rhythmic journey among the basic available journeys (Supplementary Materials List S2). Participants gather in a circle. The teacher leads the participants into a repetition of syllables, which facilitates orientation in the music cycle, with a bass drum instrument (Surdo, Remo, CA, USA) in the middle of the circle providing the main rhythm for the process. Then, specific repeating footsteps following the bass drum rhythm are introduced that the participants perform throughout. Last, single or multiple claps are added to introduce a second layer of rhythm that the participants perform. Once the participants are stable in terms of the repeating pattern of talking syllables, stepping, and clapping, the teacher begins the rhythmic journey using a percussive string instrument (Berimbau, Afroton Röttger, Frankfurt am Main, Germany).
- Rhythmic journey: As the group continues the rhythmic pattern with feet and claps, the teacher moves in the middle of the circle and starts a call response of different melodies and syllables, which the participants sing back as a whole group after they have finished one cycle. The Berimbau provides a subdivision of the main rhythm, making it easier to follow rhythmic melodies in, e.g., the offbeats. The purpose is to use stabilizing and destabilizing rhythms with the voice to increase the flexibility of the participants.
- Relaxation: As the music slowly fades, the participants are asked to increasingly go inward, with more gentle movements and voices until all movements and sounds subside into an inner feeling of the rhythmic patterns and the participants lay down for approximately 5 min.
- Integration: Participants and teachers gather in a circle sitting. There is an invitation to share experiences. Here, typical experiences, behavioral patterns, and emotions experienced can be shared and discussed.
2.8. Assessment (Primary and Secondary Endpoints)
2.8.1. Data Collection
2.8.2. Blood Collection and Analysis and HRV
2.9. Statistical Analysis
2.10. Safety
3. Discussion
3.1. Choice of Intervention
3.2. Frequency and Timespan of Therapy
3.3. Expected Benefits
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
List of Abbreviations
| BAI | Beck Anxiety Inventory |
| BDI-II | Beck Depression Inventory II |
| BFI-10 | Big Five Inventory-10 |
| CG | control group |
| DSM | Diagnostic and Statistical Manual of Mental Disorders |
| DZI | Center for Immune Therapy in Germany |
| FFMQ-D | Five Facet Mindfulness Questionnaire |
| HAMD-17 | Hamilton Rating Scale for Depression—17 |
| HRV | heart rate variability |
| IG | intervention group |
| IL | interleukin |
| LDL | low-density lipoprotein |
| MAAS | Mindful Attention and Awareness Scale |
| MADRS | Montgomery–Åsberg Depression Rating Scale |
| MDE | major depressive episode |
| MDRS-22 | Male Depression Risk Scale |
| PHQ-9 | Patient Health Questionnaire |
| PSQI | Pittsburgh Sleep Quality Index |
| PSS-10 | Perceived Stress Scale—10 |
| RS-25 | Resilience Scale—25 |
| SASKO | Fragebogen zu sozialer Angst und sozialen Kompetenzdefiziten |
| TAU | treatment as usual |
| TGF | transforming growth factor |
| TNF | tumor necrosis factor |
References
- Bundesärztekammer (BÄK); Arbeitsgemeinschaft der Wissenschaftli-chen Medizinischen Fachgesellschaften (AWMF). Nationale Versorgungs Leitlinie Unipolare Depression—Langfassung, Version 3.1. 2022. Available online: https://register.awmf.org/assets/guidelines/nvl-005l_S3_Unipolare-Depression_2023-01.pdf (accessed on 14 May 2023).
- WHO. Depressive Disorder. Available online: https://www.who.int/news-room/fact-sheets/detail/depression (accessed on 15 April 2024).
- Malhi, G.S.; Mann, J.J. Depression. Lancet 2018, 392, 2299–2312. [Google Scholar] [CrossRef] [PubMed]
- Kennedy, S.H. Core symptoms of major depressive disorder: Relevance to diagnosis and treatment. Dialogues Clin. Neurosci. 2008, 10, 271–277. [Google Scholar] [CrossRef] [PubMed]
- Wiles, N.; Thomas, L.; Abel, A.; Ridgway, N.; Turner, N.; Campbell, J.; Garland, A.; Hollinghurst, S.; Jerrom, B.; Kessler, D.; et al. Cognitive behavioural therapy as an adjunct to pharmacotherapy for primary care based patients with treatment resistant depression: Results of the CoBalT randomised controlled trial. Lancet 2013, 381, 375–384. [Google Scholar] [CrossRef] [PubMed]
- van der Velden, A.M.; Kuyken, W.; Wattar, U.; Crane, C.; Pallesen, K.J.; Dahlgaard, J.; Fjorback, L.O.; Piet, J. A systematic review of mechanisms of change in mindfulness-based cognitive therapy in the treatment of recurrent major depressive disorder. Clin. Psychol. Rev. 2015, 37, 26–39. [Google Scholar] [CrossRef] [PubMed]
- Chiang, M.; Reid-Varley, W.B.; Fan, X. Creative art therapy for mental illness. Psychiatry Res. 2019, 275, 129–136. [Google Scholar] [CrossRef] [PubMed]
- Kvam, S.; Kleppe, C.L.; Nordhus, I.H.; Hovland, A. Exercise as a treatment for depression: A meta-analysis. J. Affect. Disord. 2016, 202, 67–86. [Google Scholar] [CrossRef]
- Kind, L.; Luttenberger, K.; Leßmann, V.; Dorscht, L.; Mühle, C.; Müller, C.P.; Siegmann, E.M.; Schneider, S.; Kornhuber, J. New ways to cope with depression-study protocol for a randomized controlled mixed methods trial of bouldering psychotherapy (BPT) and mental model therapy (MMT). Trials 2023, 24, 602. [Google Scholar] [CrossRef] [PubMed]
- Aalbers, S.; Fusar-Poli, L.; Freeman, R.E.; Spreen, M.; Ket, J.C.; Vink, A.C.; Maratos, A.; Crawford, M.; Chen, X.J.; Gold, C. Music therapy for depression. Cochrane Database Syst. Rev. 2017, 11, CD004517. [Google Scholar] [CrossRef] [PubMed]
- Särkämö, T.; Tervaniemi, M.; Laitinen, S.; Numminen, A.; Kurki, M.; Johnson, J.K.; Rantanen, P. Cognitive, emotional, and social benefits of regular musical activities in early dementia: Randomized controlled study. Gerontologist 2014, 54, 634–650. [Google Scholar] [CrossRef]
- Baker, F.A.; Lee, Y.C.; Sousa, T.V.; Stretton-Smith, P.A.; Tamplin, J.; Sveinsdottir, V.; Geretsegger, M.; Wake, J.D.; Assmus, J.; Gold, C. Clinical effectiveness of music interventions for dementia and depression in elderly care (MIDDEL): Australian cohort of an international pragmatic cluster-randomised controlled trial. Lancet Healthy Longev. 2022, 3, e153–e165. [Google Scholar] [CrossRef]
- van der Steen, J.T.; Smaling, H.J.; van der Wouden, J.C.; Bruinsma, M.S.; Scholten, R.J.; Vink, A.C. Music-based therapeutic interventions for people with dementia. Cochrane Database Syst. Rev. 2018, 7, CD003477. [Google Scholar] [CrossRef] [PubMed]
- Lun, T.; Chen, Y.; Liu, J.; Li, L.; Yu, J.; Xiang, M. Music therapy and anxiety: A bibliometric review from 1993 to 2023. Medicine 2024, 103, e37459. [Google Scholar] [CrossRef] [PubMed]
- Hauser, J.; Sarlon, J.; Liwinski, T.; Brühl, A.B.; Lang, U.E. Listening to music during intranasal (es)ketamine therapy in patients with treatment-resistant depression correlates with better tolerability and reduced anxiety. Front. Psychiatry 2024, 15, 1327598. [Google Scholar] [CrossRef] [PubMed]
- Dean, J.; Keshavan, M. The neurobiology of depression: An integrated view. Asian J. Psychiatry 2017, 27, 101–111. [Google Scholar] [CrossRef] [PubMed]
- Haroon, E.; Daguanno, A.W.; Woolwine, B.J.; Goldsmith, D.R.; Baer, W.M.; Wommack, E.C.; Felger, J.C.; Miller, A.H. Antidepressant treatment resistance is associated with increased inflammatory markers in patients with major depressive disorder. Psychoneuroendocrinology 2018, 95, 43–49. [Google Scholar] [CrossRef] [PubMed]
- Hughes, M.M.; Connor, T.J.; Harkin, A. Stress-Related Immune Markers in Depression: Implications for Treatment. Int. J. Neuropsychopharmacol. 2016, 19. [Google Scholar] [CrossRef] [PubMed]
- Bekhbat, M.; Chu, K.; Le, N.A.; Woolwine, B.J.; Haroon, E.; Miller, A.H.; Felger, J.C. Glucose and lipid-related biomarkers and the antidepressant response to infliximab in patients with treatment-resistant depression. Psychoneuroendocrinology 2018, 98, 222–229. [Google Scholar] [CrossRef] [PubMed]
- Miller, A.H.; Raison, C.L. The role of inflammation in depression: From evolutionary imperative to modern treatment target. Nat. Rev. Immunol. 2016, 16, 22–34. [Google Scholar] [CrossRef] [PubMed]
- Perrin, A.J.; Horowitz, M.A.; Roelofs, J.; Zunszain, P.A.; Pariante, C.M. Glucocorticoid Resistance: Is It a Requisite for Increased Cytokine Production in Depression? A Systematic Review and Meta-Analysis. Front. Psychiatry 2019, 10, 423. [Google Scholar] [CrossRef]
- de Melo, L.G.P.; Nunes, S.O.V.; Anderson, G.; Vargas, H.O.; Barbosa, D.S.; Galecki, P.; Carvalho, A.F.; Maes, M. Shared metabolic and immune-inflammatory, oxidative and nitrosative stress pathways in the metabolic syndrome and mood disorders. Prog. Neuropsychopharmacol. Biol. Psychiatry 2017, 78, 34–50. [Google Scholar] [CrossRef]
- Ortiz, R.; Joseph, J.J.; Lee, R.; Wand, G.S.; Golden, S.H. Type 2 diabetes and cardiometabolic risk may be associated with increase in DNA methylation of FKBP5. Clin. Epigenet. 2018, 10, 82. [Google Scholar] [CrossRef] [PubMed]
- Dhama, K.; Latheef, S.K.; Dadar, M.; Samad, H.A.; Munjal, A.; Khandia, R.; Karthik, K.; Tiwari, R.; Yatoo, M.I.; Bhatt, P.; et al. Biomarkers in Stress Related Diseases/Disorders: Diagnostic, Prognostic, and Therapeutic Values. Front. Mol. Biosci. 2019, 6, 91. [Google Scholar] [CrossRef] [PubMed]
- Immanuel, S.; Teferra, M.N.; Baumert, M.; Bidargaddi, N. Heart Rate Variability for Evaluating Psychological Stress Changes in Healthy Adults: A Scoping Review. Neuropsychobiology 2023, 82, 187–202. [Google Scholar] [CrossRef] [PubMed]
- Schiweck, C.; Piette, D.; Berckmans, D.; Claes, S.; Vrieze, E. Heart rate and high frequency heart rate variability during stress as biomarker for clinical depression. A systematic review. Psychol. Med. 2019, 49, 200–211. [Google Scholar] [CrossRef] [PubMed]
- Wagner, C.J.; Musenbichler, C.; Böhm, L.; Färber, K.; Fischer, A.I.; von Nippold, F.; Winkelmann, M.; Richter-Schmidinger, T.; Mühle, C.; Kornhuber, J.; et al. LDL cholesterol relates to depression, its severity, and the prospective course. Prog. Neuropsychopharmacol. Biol. Psychiatry 2019, 92, 405–411. [Google Scholar] [CrossRef]
- van der Heijden, A.R.; Houben, T. Lipids in major depressive disorder: New kids on the block or old friends revisited? Front. Psychiatry 2023, 14, 1213011. [Google Scholar] [CrossRef] [PubMed]
- Mühle, C.; Bilbao Canalejas, R.D.; Kornhuber, J. Sphingomyelin Synthases in Neuropsychiatric Health and Disease. Neuro-Signals 2019, 27, 54–76. [Google Scholar] [CrossRef]
- Hannun, Y.A.; Obeid, L.M. Sphingolipids and their metabolism in physiology and disease. Nat. Rev. Mol. Cell Biol. 2018, 19, 175–191. [Google Scholar] [CrossRef]
- Zoicas, I.; Mühle, C.; Schumacher, F.; Kleuser, B.; Kornhuber, J. Development of Comorbid Depression after Social Fear Conditioning in Mice and Its Effects on Brain Sphingolipid Metabolism. Cells 2023, 12, 1355. [Google Scholar] [CrossRef]
- Zoicas, I.; Mühle, C.; Schmidtner, A.K.; Gulbins, E.; Neumann, I.D.; Kornhuber, J. Anxiety and Depression Are Related to Higher Activity of Sphingolipid Metabolizing Enzymes in the Rat Brain. Cells 2020, 9, 1239. [Google Scholar] [CrossRef]
- Dinoff, A.; Herrmann, N.; Lanctôt, K.L. Ceramides and depression: A systematic review. J. Affect. Disord. 2017, 213, 35–43. [Google Scholar] [CrossRef] [PubMed]
- Narayan, S.; Thomas, E.A. Sphingolipid abnormalities in psychiatric disorders: A missing link in pathology? Front. Biosci. (Landmark Ed.) 2011, 16, 1797–1810. [Google Scholar] [CrossRef] [PubMed]
- Schumacher, F.; Edwards, M.J.; Mühle, C.; Carpinteiro, A.; Wilson, G.C.; Wilker, B.; Soddemann, M.; Keitsch, S.; Scherbaum, N.; Müller, B.W.; et al. Ceramide levels in blood plasma correlate with major depressive disorder severity and its neutralization abrogates depressive behavior in mice. J. Biol. Chem. 2022, 298, 102185. [Google Scholar] [CrossRef] [PubMed]
- Gracia-Garcia, P.; Rao, V.; Haughey, N.J.; Bandaru, V.V.; Smith, G.; Rosenberg, P.B.; Lobo, A.; Lyketsos, C.G.; Mielke, M.M. Elevated plasma ceramides in depression. J. Neuropsychiatry Clin. Neurosci. 2011, 23, 215–218. [Google Scholar] [CrossRef] [PubMed]
- Brunkhorst-Kanaan, N.; Klatt-Schreiner, K.; Hackel, J.; Schröter, K.; Trautmann, S.; Hahnefeld, L.; Wicker, S.; Reif, A.; Thomas, D.; Geisslinger, G.; et al. Targeted lipidomics reveal derangement of ceramides in major depression and bipolar disorder. Metabolism 2019, 95, 65–76. [Google Scholar] [CrossRef] [PubMed]
- Mühle, C.; Wagner, C.J.; Färber, K.; Richter-Schmidinger, T.; Gulbins, E.; Lenz, B.; Kornhuber, J. Secretory Acid Sphingomyelinase in the Serum of Medicated Patients Predicts the Prospective Course of Depression. J. Clin. Med. 2019, 8, 846. [Google Scholar] [CrossRef] [PubMed]
- American Psychiatric Association. Diagnostisches und Statistisches Manual Psychischer Störungen DSM-5®; American Psychiatric Association: Washington, DC, USA, 2018. [Google Scholar] [CrossRef]
- Hamilton, M. A rating scale for depression. J. Neurol. Neurosurg. Psychiatry 1960, 23, 56–62. [Google Scholar] [CrossRef]
- Montgomery, S.A.; Åsberg, M. A New Depression Scale Designed to be Sensitive to Change. Br. J. Psychiatry 1979, 134, 382–389. [Google Scholar] [CrossRef] [PubMed]
- Hautzinger, M.K.F.; Kühner, C. BDI-II-Depressionsinventar, 2nd ed.; Serv, H.T., Ed.; Hogrefe: Göttingen, Germany, 2006. [Google Scholar]
- von Zimmermann, C.; Hübner, M.; Mühle, C.; Müller, C.P.; Weinland, C.; Kornhuber, J.; Lenz, B. Masculine depression and its problem behaviors: Use alcohol and drugs, work hard, and avoid psychiatry! Eur. Arch. Psychiatry Clin. Neurosci. 2023, 274, 1–13. [Google Scholar] [CrossRef]
- Rice, S.M.; Fallon, B.J.; Aucote, H.M.; Möller-Leimkühler, A.M. Development and preliminary validation of the male depression risk scale: Furthering the assessment of depression in men. J. Affect. Disord. 2013, 151, 950–958. [Google Scholar] [CrossRef]
- Beck, A.T.; Epstein, N.; Brown, G.; Steer, R.A. An inventory for measuring clinical anxiety: Psychometric properties. J. Consult. Clin. Psychol. 1988, 56, 893–897. [Google Scholar] [CrossRef] [PubMed]
- Brown, K.W.; Ryan, R.M. The benefits of being present: Mindfulness and its role in psychological well-being. J. Personal. Soc. Psychol. 2003, 84, 822–848. [Google Scholar] [CrossRef] [PubMed]
- Baer, R.A.; Smith, G.T.; Hopkins, J.; Krietemeyer, J.; Toney, L. Using self-report assessment methods to explore facets of mindfulness. Assessment 2006, 13, 27–45. [Google Scholar] [CrossRef] [PubMed]
- Michalak, J.; Zarbock, G.; Drews, M.; Otto, D.; Mertens, D.; Ströhle, G.; Schwinger, M.; Dahme, B.; Heidenreich, T. Erfassung von Achtsamkeit mit der deutschen Version des Five Facet Mindfulness Questionnaires (FFMQ-D). [Assessment of mindfulness with the German version of the Five Facet Mindfulness Questionnaires (FFMQ-D)]. Z. Gesundheitspsychol. 2016, 24, 1–12. [Google Scholar] [CrossRef]
- Klein, E.M.; Brähler, E.; Dreier, M.; Reinecke, L.; Müller, K.W.; Schmutzer, G.; Wölfling, K.; Beutel, M.E. The German version of the Perceived Stress Scale—Psychometric characteristics in a representative German community sample. BMC Psychiatry 2016, 16, 159. [Google Scholar] [CrossRef] [PubMed]
- Cohen, S.; Kamarck, T.; Mermelstein, R. A global measure of perceived stress. J. Health Soc. Behav. 1983, 24, 385–396. [Google Scholar] [CrossRef] [PubMed]
- Wagnild, G.M.; Young, H.M. Development and psychometric evaluation of the Resilience Scale. J. Nurs. Meas. 1993, 1, 165–178. [Google Scholar] [PubMed]
- Buysse, D.J.; Reynolds, C.F., 3rd; Monk, T.H.; Berman, S.R.; Kupfer, D.J. The Pittsburgh Sleep Quality Index: A new instrument for psychiatric practice and research. Psychiatry Res. 1989, 28, 193–213. [Google Scholar] [CrossRef]
- Kolbeck, S.; Maß, R. Fragebogen zu Sozialer Angst und Sozialen Kompetenzdefiziten; SASKO; Hogrefe: Göttingen, Germany, 2009. [Google Scholar]
- Rammstedt, B.; John, O.P. Measuring personality in one minute or less: A 10-item short version of the Big Five Inventory in English and German. J. Res. Personal. 2007, 41, 203–212. [Google Scholar] [CrossRef]
- Mühle, C.; Kornhuber, J. Assay to measure sphingomyelinase and ceramidase activities efficiently and safely. J. Chromatogr. A 2017, 1481, 137–144. [Google Scholar] [CrossRef]
- Mühle, C.; Kornhuber, J. Characterization of a Neutral Sphingomyelinase Activity in Human Serum and Plasma. Int. J. Mol. Sci. 2023, 24, 2467. [Google Scholar] [CrossRef] [PubMed]
- Wang, S.; Agius, M. The use of Music Therapy in the treatment of Mental Illness and the enhancement of Societal Wellbeing. Psychiatr. Danub. 2018, 30, 595–600. [Google Scholar] [PubMed]
- Witusik, A.; Pietras, T. Music therapy as a complementary form of therapy for mental disorders. Pol. Merkur. Lek. 2019, 47, 240–243. [Google Scholar]
- Zhao, K.; Bai, Z.G.; Bo, A.; Chi, I. A systematic review and meta-analysis of music therapy for the older adults with depression. Int. J. Geriatr. Psychiatry 2016, 31, 1188–1198. [Google Scholar] [CrossRef]
- Dhippayom, T.; Saensook, T.; Promkhatja, N.; Teaktong, T.; Chaiyakunapruk, N.; Devine, B. Comparative effects of music interventions on depression in older adults: A systematic review and network meta-analysis. EClinicalMedicine 2022, 50, 101509. [Google Scholar] [CrossRef] [PubMed]
- Dayuan, Z.; Lan, L.; Hui, C.; Huanjie, L.; Deliang, L.; Yihui, D. The effect of music as an intervention for post-stroke depression: A systematic review and meta-analysis. Complement. Ther. Med. 2022, 71, 102901. [Google Scholar] [CrossRef] [PubMed]
- Belski, N.; Abdul-Rahman, Z.; Youn, E.; Balasundaram, V.; Diep, D. Review: The effectiveness of musical therapy in improving depression and anxiety symptoms among children and adolescents—A systematic review. Child. Adolesc. Ment. Health 2022, 27, 369–377. [Google Scholar] [CrossRef] [PubMed]
- Pearce, M.; Garcia, L.; Abbas, A.; Strain, T.; Schuch, F.B.; Golubic, R.; Kelly, P.; Khan, S.; Utukuri, M.; Laird, Y.; et al. Association Between Physical Activity and Risk of Depression: A Systematic Review and Meta-analysis. JAMA Psychiatry 2022, 79, 550–559. [Google Scholar] [CrossRef]
- Hofmann, S.G.; Gómez, A.F. Mindfulness-Based Interventions for Anxiety and Depression. Psychiatr. Clin. N. Am. 2017, 40, 739–749. [Google Scholar] [CrossRef]
- Dudek, K.A.; Dion-Albert, L.; Kaufmann, F.N.; Tuck, E.; Lebel, M.; Menard, C. Neurobiology of resilience in depression: Immune and vascular insights from human and animal studies. Eur. J. Neurosci. 2021, 53, 183–221. [Google Scholar] [CrossRef]
- Ribeiro, M.K.A.; Alcântara-Silva, T.R.M.; Oliveira, J.C.M.; Paula, T.C.; Dutra, J.B.R.; Pedrino, G.R.; Simões, K.; Sousa, R.B.; Rebelo, A.C.S. Music therapy intervention in cardiac autonomic modulation, anxiety, and depression in mothers of preterms: Randomized controlled trial. BMC Psychol. 2018, 6, 57. [Google Scholar] [CrossRef] [PubMed]
- Sedlinská, T.; Mühle, C.; Richter-Schmidinger, T.; Weinland, C.; Kornhuber, J.; Lenz, B. Male depression syndrome is characterized by pronounced Cluster B personality traits. J. Affect. Disord. 2021, 292, 725–732. [Google Scholar] [CrossRef] [PubMed]
- von Zimmermann, C.; Brückner, L.; Mühle, C.; Weinland, C.; Kornhuber, J.; Lenz, B. Bioimpedance Body Measures and Serum Lipid Levels in Masculine Depression. Front. Psychiatry 2022, 13, 794351. [Google Scholar] [CrossRef]
- Bowling, D.L. Biological principles for music and mental health. Transl. Psychiatry 2023, 13, 374. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Visits | Prescreening | Screening | V1,3,4 | V2, V6 ** | V5,7,8 ** |
|---|---|---|---|---|---|
| PHQ-9 or telephone interview | x | ||||
| Inclusion/exclusion criteria | x | x | |||
| Informed consent | x | ||||
| Recording of | |||||
| x | x | |||
| x | x | x | ||
| x | ||||
| x | ||||
| x | x | x | ||
| x | x | x | ||
| x | x | x | ||
| x | x | x | ||
| x | x | x | ||
| x | x | x | ||
| x | x | |||
| x | ||||
| x | ||||
| |||||
| x | x |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Behzad, A.; Feldmann-Schulz, C.; Lenz, B.; Clarkson, L.; Ludwig, C.; Luttenberger, K.; Völkl, S.; Kornhuber, J.; Mühle, C.; von Zimmermann, C. TaKeTiNa Music Therapy for Outpatient Treatment of Depression: Study Protocol for a Randomized Clinical Trial. J. Clin. Med. 2024, 13, 2494. https://doi.org/10.3390/jcm13092494
Behzad A, Feldmann-Schulz C, Lenz B, Clarkson L, Ludwig C, Luttenberger K, Völkl S, Kornhuber J, Mühle C, von Zimmermann C. TaKeTiNa Music Therapy for Outpatient Treatment of Depression: Study Protocol for a Randomized Clinical Trial. Journal of Clinical Medicine. 2024; 13(9):2494. https://doi.org/10.3390/jcm13092494
Chicago/Turabian StyleBehzad, Ali, Christoph Feldmann-Schulz, Bernd Lenz, Lucy Clarkson, Celine Ludwig, Katharina Luttenberger, Simon Völkl, Johannes Kornhuber, Christiane Mühle, and Claudia von Zimmermann. 2024. "TaKeTiNa Music Therapy for Outpatient Treatment of Depression: Study Protocol for a Randomized Clinical Trial" Journal of Clinical Medicine 13, no. 9: 2494. https://doi.org/10.3390/jcm13092494