
Lipid and Glucose Profile across Different Mental Disorders

 , , , ,
, , , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Data Collection
2.2. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Wainberg, M.L.; Scorza, P.; Shultz, J.M.; Helpman, L.; Mootz, J.J.; Johnson, K.A.; Neria, Y.; Bradford, J.-M.E.; Oquendo, M.A.; Arbuckle, M.R. Challenges and opportunities in global mental health: A research-to-practice perspective. Curr. Psychiatry Rep. 2017, 19, 28. [Google Scholar] [CrossRef] [PubMed]
- Heiberg, I.H.; Jacobsen, B.K.; Balteskard, L.; Bramness, J.G.; Næss, Ø.; Ystrom, E.; Reichborn-Kjennerud, T.; Hultman, C.M.; Nesvåg, R.; Høye, A. Undiagnosed cardiovascular disease prior to cardiovascular death in individuals with severe mental illness. Acta Psychiatr. Scand. 2019, 139, 558–571. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization (WHO). Depression and Other Common Mental Disorders: Global Health Estimates. 2017. Available online: https://www.who.int/publications-detail-redirect/depression-global-health-estimates (accessed on 23 April 2023).
- Wysokiński, A.; Strzelecki, D.; Kłoszewska, I. Levels of triglycerides, cholesterol, LDL, HDL and glucose in patients with schizophrenia, unipolar depression and bipolar disorder. Diabetes Metab. Syndr. Clin. Res. Rev. 2015, 9, 168–176. [Google Scholar] [CrossRef]
- Grundy, S.M.; Stone, N.J.; Bailey, A.L.; Beam, C.; Birtcher, K.K.; Blumenthal, R.S.; Braun, L.T.; de Ferranti, S.; Faiella-Tommasino, J.; Forman, D.E.; et al. 2018 AHA/ACC/AACVPR/AAPA/ABC/ACPM/ADA/AGS/APhA/ASPC/NLA/PCNA guideline on the management of blood cholesterol: Executive summary: A report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines. J. Am. Coll. Cardiol. 2019, 139, E1082–E1143. [Google Scholar] [CrossRef]
- Alexander, C.M.; Landsman, P.B.; Teutsch, S.M.; Haffner, S.M. NCEP-defined metabolic syndrome, diabetes, and prevalence of coronary heart disease among NHANES III participants age 50 years and older. Diabetes 2003, 52, 1210–1214. [Google Scholar] [CrossRef] [PubMed]
- Vaccarino, V.; McClure, C.; Johnson, B.D.; Sheps, D.S.; Bittner, V.; Rutledge, T.; Shaw, L.J.; Sopko, G.; Olson, M.B.; Krantz, D.S.; et al. Depression, the metabolic syndrome and cardiovascular risk. Psychosom. Med. 2008, 70, 40–48. [Google Scholar] [CrossRef] [PubMed]
- Goff, D.C.; Sullivan, L.M.; McEvoy, J.P.; Meyer, J.M.; Nasrallah, H.A.; Daumit, G.L.; Lamberti, S.; D’Agostino, R.B.; Stroup, T.S.; Davis, S.; et al. A comparison of ten-year cardiac risk estimates in schizophrenia patients from the CATIE study and matched controls. Schizophr. Res. 2005, 80, 45–53. [Google Scholar] [CrossRef] [PubMed]
- de Leon, J.; Susce, M.T.; Johnson, M.; Hardin, M.; Pointer, L.; Ruaño, G.; Windemuth, A.; Diaz, F.J. A clinical study of the association of antipsychotics with hyperlipidemia. Schizophr. Res. 2007, 92, 95–102. [Google Scholar] [CrossRef] [PubMed]
- Wysokiński, A.; Kowman, M.; Kłoszewska, I. The prevalence of metabolic syndrome and Framingham cardiovascular risk scores in adult inpatients taking antipsychotics-a retrospective medical records review. Psychiatr. Danub. 2012, 24, 314–322. [Google Scholar] [PubMed]
- De Hert, M.A.; van Winkel, R.; Van Eyck, D.; Hanssens, L.; Wampers, M.; Scheen, A.; Peuskens, J. Prevalence of the metabolic syndrome in patients with schizophrenia treated with antipsychotic medication. Schizophr. Res. 2006, 83, 87–93. [Google Scholar] [CrossRef] [PubMed]
- Richter, N.; Juckel, G.; Assion, H.-J. Metabolic syndrome: A follow-up study of acute depressive inpatients. Eur. Arch. Psychiatry Clin. Neurosci. 2010, 260, 41–49. [Google Scholar] [CrossRef] [PubMed]
- Sicras-Mainar, A.; Blanca-Tamayo, M.; Rejas-Gutiérrez, J.; Navarro-Artieda, R. Metabolic syndrome in outpatients receiving antipsychotic therapy in routine clinical practice: A cross-sectional assessment of a primary health care database. Eur. Psychiatry 2008, 23, 100–108. [Google Scholar] [CrossRef] [PubMed]
- Kinder, L.S.; Carnethon, M.R.; Palaniappan, L.P.; King, A.C.; Fortmann, S.P. Depression and the metabolic syndrome in young adults: Findings from the third national health and nutrition examination survey. Psychosom. Med. 2004, 66, 316–322. [Google Scholar] [CrossRef] [PubMed]
- Mozaffarian, D.; Kamineni, A.; Prineas, R.J.; Siscovick, D.S. Metabolic syndrome and mortality in older adults: The Cardiovascular Health Study. Arch. Intern. Med. 2008, 168, 969–978. [Google Scholar] [CrossRef] [PubMed]
- Nadalin, S.; Peitl, V.; Karlović, D.; Huskić, S.; Zatković, L.; Buretić-Tomljanović, A. Correlations Between Clinical and Metabolic Variables and Smoking among Antipsychotic- Naïve First-Episode and Nonadherent Chronic Patients with Psychosis. Arch. Psychiatry Res. Int. J. Psychiatry Relat. Sci. 2023, 59, 241–250. [Google Scholar] [CrossRef]
- Li, Z.; Wang, S.; Chen, Y.; Wu, X.; Gu, Y.; Lang, X.; Wu, F.; Zhang, X.Y. Smoking affects the patterns of metabolic disorders and metabolic syndrome in patients with first-episode drug-naive schizophrenia: A large sample study based on the Chinese Han population. Int. J. Neuropsychopharmacol. 2021, 24, 798–807. [Google Scholar] [CrossRef] [PubMed]
- Sonnenschein, S.F. State-Dependent Dopamine System Regulation Using Current and Novel Antipsychotic Drug Mechanisms: Developmental Implications in a Schizophrenia Model. Ph.D. Thesis, University of Pittsburgh, Pittsburgh, PA, USA, 2020. [Google Scholar]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Diagnosis | Gender | Age Category | Total | |||
|---|---|---|---|---|---|---|
| <25 | 25–45 | 45–65 | >65 | N (%) | ||
| Schizophrenia | Male | 31 | 100 | 80 | 31 | 242 (48.4%) |
| Female | 26 | 148 | 76 | 8 | 258 (52.6%) | |
| Total N (%) | 57 (11.4%) | 248 (49.6%) | 156 (31.2%) | 39 (7.8%) | 500 (100%) | |
| Unipolar depression | Male | 51 | 11 | 78 | 9 | 149 (33.18%) |
| Female | 70 | 40 | 30 | 160 | 300 (66.82%) | |
| Total N | 121 (26.95%) | 51 (11.36%) | 108 (24.05%) | 169 (37.64%) | 449 (100%) | |
| Bipolar disorder | Male | 28 | 55 | 21 | 17 | 121 (50.84%) |
| Female | 31 | 43 | 30 | 13 | 117 (49.16%) | |
| Total N | 59 (24.79%) | 98 (41.18%) | 51 (21.43%) | 30 (12.61%) | 238 (100%) | |
| Bipolar depression | Male | 20 | 29 | 14 | 10 | 73 (48.99%) |
| Female | 21 | 26 | 19 | 10 | 76 (51.01%) | |
| Total N | 41 (27.52%) | 55 (36.91%) | 33 (22.15%) | 20 (13.42%) | 149 (100%) | |
| Bipolar mania | Male | 8 | 26 | 7 | 7 | 48 (53.93%) |
| Female | 10 | 17 | 11 | 3 | 41 (46.07%) | |
| Total N | 18 (20.22%) | 43 (48.31%) | 18 (20.22%) | 10 (20.22%) | 89 (100%) | |
| Total | 237 (19.67%) | 397 (33.45%) | 315 (26.54%) | 238 (20.05%) | 1187 (100%) | |
| High LDL N (%) | Low HDL N (%) | High TC N (%) | High TGA N (%) | High FPG N (%) | |
|---|---|---|---|---|---|
| Schizophrenia OR | 1.00 | 1.00 | 1.00 | 1.00 | 1.00 |
| Men | 72 (29.75%) | 135 (55.79%) | 61 (25.21%) | 97 (40.08%) | 49 (20.25%) |
| Women | 64 (24.81%) | 160 (62.02%) | 83 (32.17%) | 69 (26.74%) | 81 (31.40%) |
| Schizophrenia | 136 (27.20%) | 295 (59.00%) | 144 (28.80%) | 166 (33.20%) | 130 (26.00%) |
| Unipolar depression OR | 1.79 [1.09–2.15] | 0.78 [0.56–1.25] | 2 [1.41–2.36] | 1 [0.49–0.91] | 1 [0.84–1.29] |
| Men | 54 (36.24%) | 98 (65.77%) | 49 (32.89%) | 69 (46.31%) | 46 (30.87%) |
| Women | 104 (34.67%) | 188 (62.67%) | 147 (49.00%) | 107 (35.50%) | 116 (38.67%) |
| Unipolar depression | 158 (35.189%) | 286 (63.697%) | 196 (43.65%) | 176 (39.087%) | 162 (36.08%) |
| Bipolar disorder OR | 1.56 [0.79–1.79] | 1.01 [0.68–1.59] | 1 [0.96–1.76] | 1 [0.93–1.82] | 1 [0.79–1.53] |
| Men | 37 (30.58%) | 71 (58.68%) | 40 (33.06%) | 55 (45.45%) | 29 (23.97%) |
| Women | 35 (29.91%) | 70 (59.83%) | 53 (45.30%) | 36 (30.77%) | 34 (29.06%) |
| Bipolar disorder | 72 (30.25%) | 141 (59.24%) | 93 (39.08%) | 91 (38.24%) | 63 (26.47%) |
| Bipolar depression OR | 1.59 [1.13–2.08] | 1.35 [0.91–1.61] | 1 [1.1–1.64] | 1 [1.08–1.74] | 1 [0.79–1.27] |
| Men | 22 (30.14%) | 45 (61.64%) | 30 (41.10%) | 36 (49.32%) | 19 (26.03%) |
| Women | 29 (38.16%) | 45 (59.21%) | 36 (47.37%) | 31 (40.79%) | 27 (35.00%) |
| Bipolar depression | 51 (34.23%) | 90 (60.40%) | 66 (44.30%) | 67 (44.97%) | 46 (30.60%) |
| Bipolar mania OR | 0.74 [0.36–1.32] | 0.86 [0.49–1.39] | 1 [0.55–1.98] | 1 [0.41–0.89] | 1 [0.31–1.29] |
| Men | 8 (16.67%) | 22 (45.83%) | 3 (6.25%) | 11 (22.92%) | 9 (18.54%) |
| Women | 13 (31.71%) | 23 (56.10%) | 12 (29.27%) | 8 (20.00%) | 12 (29.27%) |
| Bipolar mania | 21 (23.60%) | 45 (50.56%) | 15 (16.85%) | 19 (21.57%) | 21 (23.48%) |
| <25 | 25–45 | 45–65 | >65 | Total | H | p | |
|---|---|---|---|---|---|---|---|
| LDL [mg/dL] | |||||||
| Male | 100.34 ± 59.05 | 108.45 ± 20.18 | 119.42 ± 15.80 | 100.89 ± 80.10 | 110.07 ± 31.39 | 33.91 | <0.001 |
| Female | 97.54 ± 20.15 | 113.71 ± 90.81 | 121.94 ± 50.10 | 105.91 ± 30.51 | 114.26 ± 69.83 | 20.40 | <0.001 |
| Schizophrenic | 99.06 ± 41.31 | 111.59 ± 62.33 | 120.65 ± 32.51 | 101.92 ± 69.93 | 112.23 ± 51.22 | 19.60 | <0.001 |
| Z | 0.40 | −2.30 | −0.08 | −2.91 | −2.90 | ||
| P | 0.90 | 0.04 | 0.80 | 0.03 | 0.01 | ||
| Men | 87.25 ± 89.07 | 118.44 ± 58.18 | 125.42 ± 43.80 | 118.89 ± 89.10 | 111.45 ± 63.09 | 11.29 | 0.01 |
| Women | 97.80 ± 20.15 | 109.7 ± 91.17 | 124.07 ± 60.10 | 116.85 ± 50.89 | 112.19 ± 50.01 | 4.90 | 0.40 |
| Unipolar depression | 93.35 ± 49.20 | 111.66 ± 84.05 | 125.05 ± 48.33 | 116.96 ± 52.92 | 111.94 ± 54.35 | 9.10 | 0.05 |
| Z | 0.90 | 0.25 | −0.03 | 0.30 | −0.24 | ||
| P | 0.99 | 0.90 | 0.89 | 0.92 | 0.92 | ||
| Men | 104.40 ± 33.1 | 105.450 ± 36.3 | 116.00 ± 35.1 | 125.65 ± 43.15 | 111.85 ± 37.17 | 4.10 | 0.09 |
| Women | 109.45 ± 40.1 | 103.950 ± 17.6 | 119.05 ± 42.85 | 119.65 ± 33.35 | 112.057 ± 32.62 | 6.66 | 0.06 |
| Bipolar disorder | 107.18 ± 37.04 | 104.617 ± 27.51 | 118.13 ± 40.14 | 123.80 ± 40.5 | 111.845 ± 34.57 | 2.90 | 0.06 |
| Z | −0.98 | −1.98 | 0.30 | −0.25 | −20.70 | ||
| P | 0.40 | 0.07 | 0.90 | 0.85 | 0.40 | ||
| Men | 125.70 ± 46.10 | 96.30 ± 40.20 | 125.20 ± 52.20 | 130.10 ± 42.20 | 114.53 ± 44.39 | 3.10 | 0.40 |
| Women | 126.80 ± 43.80 | 90.10 ± 4.00 | 110.10 ± 35.10 | 129.60 ± 46.50 | 110.44 ± 28.36 | 8.01 | 0.05 |
| Bipolar depression | 126.26 ± 44.92 | 93.37 ± 23.09 | 116.51 ± 42.35 | 129.85 ± 44.06 | 112.44 ± 36.18 | 10.81 | 0.01 |
| Z | 0.15 | 0.25 | 0.10 | 0.28 | −0.25 | ||
| P | 0.90 | 0.91 | 0.89 | 0.85 | 0.79 | 7.70 | 0.06 |
| Men | 83.10 ± 20.10 | 114.60 ± 32.40 | 106.80 ± 18.00 | 121.20 ± 44.10 | 109.18 ± 29.96 | 1.81 | 0.70 |
| Women | 92.10 ± 36.40 | 117.80 ± 31.20 | 128.00 ± 50.60 | 109.70 ± 20.20 | 113.68 ± 36.87 | 6.70 | 0.08 |
| Bipolar mania | 88.10 ± 29.16 | 115.87 ± 31.93 | 119.76 ± 37.92 | 117.75 ± 36.93 | 111.25 ± 33.14 | ||
| Z | −0.90 | −1.90 | 0.23 | −0.32 | −2.70 | ||
| P | 0.40 | 0.07 | 0.82 | 0.70 | 0.40 | ||
| HDL [mg/dL] | |||||||
| Male | 48.23 ± 10.08 | 60.45 ± 9.50 | 65.92 ± 15.80 | 44.89 ± 8.50 | 58.70 ± 11.53 | 30.70 | 0.01 |
| Female | 53.91 ± 7.89 | 55.78 ± 8.19 | 67.94 ± 50.10 | 43.98 ± 10.51 | 58.81 ± 20.58 | 17.50 | 0.00 |
| Schizophrenic | 50.82 ± 9.08 | 57.66 ± 8.72 | 66.90 ± 32.51 | 44.70 ± 8.91 | 58.76 ± 16.20 | 4.10 | 0.40 |
| Z | −1.50 | −1.81 | −6.10 | −1.10 | −11.30 | ||
| P | 0.10 | 0.00 | 0.00 | 0.74 | 0.00 | ||
| Men | 38.25 ± 9.81 | 47.64 ± 5.18 | 50.02 ± 3.87 | 63.99 ± 9.18 | 46.66 ± 6.32 | 0.91 | 0.91 |
| Women | 43.80 ± 12.15 | 55.79 ± 8.19 | 40.27 ± 6.18 | 54.95 ± 5.70 | 50.99 ± 7.59 | 0.55 | 0.81 |
| unipolar depression | 41.46 ± 11.16 | 54.03 ± 7.54 | 47.31 ± 4.51 | 55.43 ± 5.89 | 49.55 ± 7.17 | 1.85 | 0.51 |
| Z | −1.80 | −2.80 | −2.90 | −2.15 | −6.10 | ||
| P | 0.06 | 0.00 | 0.01 | 0.01 | 0.00 | ||
| Men | 45.54 ± 6.84 | 40.9 ± 9.26 | 38.68 ± 18.75 | 44.17 ± 15.0 | 41.69 ± 11.61 | 2.50 | 0.50 |
| Women | 53.64 ± 7.68 | 55.04 ± 13.57 | 47.15 ± 18.42 | 53.53 ± 13.5 | 52.69 ± 13.25 | 2.91 | 0.80 |
| Bipolar disorder | 49.73 ± 7.29 | 46.88 ± 11.32 | 43.68 ± 18.53 | 48.48 ± 14.62 | 47.04 ± 12.47 | 2.13 | 0.60 |
| Z | −1.45 | −4.10 | −3.80 | −3.10 | −6.10 | ||
| P | 0.20 | 0.00 | 0.00 | 0.01 | 0.00 | ||
| Men | 40.18 ± 9.56 | 40.89 ± 5.12 | 36.41 ± 19.10 | 40.15 ± 11.20 | 39.73 ± 9.85 | 1.30 | 0.94 |
| Women | 54.18 ± 10.20 | 50.98 ± 14.25 | 46.12 ± 20.14 | 55.19 ± 12.20 | 51.20 ± 14.33 | 1.56 | 0.67 |
| Bipolar depression | 47.35 ± 9.89 | 45.66 ± 9.44 | 42.00 ± 19.70 | 47.67 ± 11.63 | 45.58 ± 12.13 | 2.15 | 0.65 |
| Z | 1.84 | 3.50 | 3.40 | 2.10 | 4.99 | ||
| P | 0.06 | 0.00 | 0.01 | 0.01 | <0.001 | 3.19 | 0.49 |
| Men | 50.89 ± 4.12 | 40.90 ± 13.40 | 40.95 ± 18.40 | 48.19 ± 18.80 | 43.64 ± 13.37 | 5.16 | 0.56 |
| Women | 53.10 ± 5.16 | 59.10 ± 12.89 | 48.18 ± 16.70 | 51.87 ± 14.80 | 54.18 ± 12.17 | 20.15 | 0.80 |
| Bipolar mania | 52.12 ± 4.70 | 48.10 ± 13.20 | 45.37 ± 17.36 | 49.29 ± 17.60 | 48.49 ± 12.82 | ||
| Z | 1.50 | 2.19 | 3.46 | 0.98 | 2.01 | ||
| P | 0.26 | 0.15 | 0.21 | 0.69 | <0.001 | ||
| TC [mg/dL] | |||||||
| Male | 150.21 ± 89.04 | 165.95 ± 20.50 | 189.00 ± 55.70 | 190.080 ± 44.560 | 174.64 ± 43.99 | H = 46.90 | <0.001 |
| Female | 165.00 ± 3.82 | 175.97 ± 18.89 | 171.94 ± 10.10 | 198.980 ± 15.140 | 174.39 ± 14.67 | H = 21.60 | 0.00 |
| Schizophrenic | 156.96 ± 5 0.17 | 171.93 ± 19.54 | 180.69 ± 33.48 | 191.906 ± 38.525 | 174.51 ± 28.86 | H = 28.09 | <0.001 |
| Z | 0.05 | −3.40 | −0.81 | −2.90 | −4.50 | ||
| P | 0.80 | 0.006 | 0.45 | 0.005 | 0.001 | ||
| Men | 140.25 ± 9.80 | 168.64 ± 5.18 | 180.02 ± 3.78 | 190.99 ± 9.18 | 166.23 ± 6.27 | 9.80 | 0.02 |
| Women | 160.92 ± 44.15 | 170.00 ± 38.13 | 175.85 ± 60.18 | 188.35 ± 35.70 | 178.25 ± 40.44 | 8.90 | 0.07 |
| unipolar depression | 152.21 ± 29.67 | 169.71 ± 31.02 | 178.86 ± 19.45 | 188.49 ± 34.29 | 174.26 ± 29.10 | 2.60 | 0.70 |
| Z | −1.10 | −1.80 | 0.50 | −0.71 | −2.90 | ||
| P | 0.33 | 0.07 | 0.89 | 0.80 | 0.01 | ||
| Men | 159.20 ± 21.18 | 173.20 ± 57.75 | 189.80 ± 42.9 | 189.60 ± 37.57 | 175.16 ± 44.08 | 40.78 | <0.001 |
| Women | 167.95 | 174.80 ± 31.77 | 189.85 ± 41.60 | 194.55 ± 53.35 | 178.31 ± 33.70 | 10.50 | <0.001 |
| Bipolar disorder | 164.1 | 173.75 ± 46.44 | 189.81 ± 42.11 | 191.01 ± 42.88 | 176.6 ± 38.94 | 24.60 | <0.001 |
| Z | −1.90 | −2.50 | −0.77 | 0.81 | −1.81 | ||
| P | 0.17 | 0.18 | 0.60 | 0.40 | 0.1 | ||
| Men | 177.30 ± 17.25 | 190.80 ± 60.30 | 199.40 ± 50.20 | 190.10 ± 42.10 | 188.65 ± 44.08 | 3.08 | 0.40 |
| Women | 175.70 ± 1.80 | 188.70 ± 33.40 | 200.60 ± 50.10 | 189.30 ± 50.80 | 188.16 ± 31.13 | 8.95 | 0.01 |
| Bipolar depression | 176.48 ± 9.34 | 189.81 ± 47.58 | 200.09 ± 50.14 | 189.70 ± 45.87 | 188.40 ± 37.40 | 12.80 | 0.01 |
| Z | −0.35 | −0.50 | −0.80 | −0.34 | −1.40 | ||
| P | 0.70 | 0.71 | 0.55 | 0.73 | 0.20 | ||
| Men | 141.10 ± 25.10 | 155.60 ± 55.20 | 180.20 ± 35.60 | 189.10 ± 33.03 | 161.66 ± 44.09 | 9.10 | 2.13 |
| Women | 160.20 ± 44.30 | 160.90 ± 30.13 | 179.10 ± 33.10 | 199.80 ± 55.90 | 168.46 ± 36.27 | 0.03 | 0.60 |
| Bipolar mania | 151.71 ± 35.77 | 157.70 ± 45.29 | 179.53 ± 34.07 | 192.31 ± 39.89 | 164.79 ± 40.49 | 80.55 | 0.02 |
| Z | −1.10 | −1.80 | 0.33 | −0.07 | −2.30 | ||
| P | 0.28 | 0.05 | 0.80 | 0.99 | 0.02 | ||
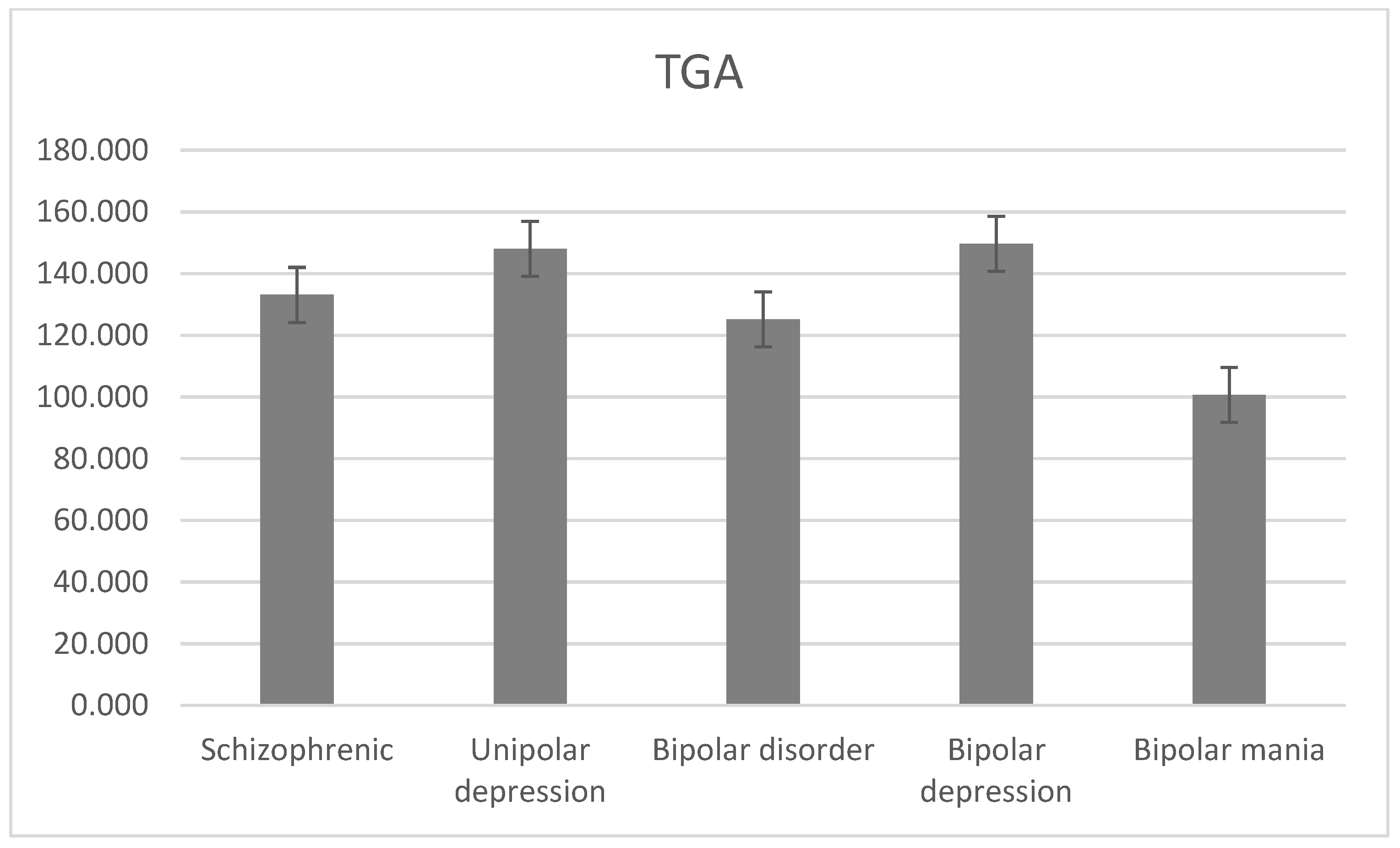
| TGA [mg/dL] | |||||||
| Male | 110.21 ± 45.09 | 142.690 ± 29.57 | 146.90 ± 59.78 | 109.81 ± 38.98 | 135.71 ± 42.75 | 25.91 | <0.001 |
| Female | 102.01 ± 20.12 | 136.04 ± 25.89 | 130.99 ± 30.89 | 120.98 ± 22.18 | 130.66 ± 26.67 | 20.15 | <0.001 |
| Schizophrenic | 106.47 ± 33.70 | 138.72 ± 27.37 | 139.15 ± 45.71 | 112.10 ± 35.53 | 133.10 ± 34.45 | 23.10 | <0.001 |
| Z | 2.03 | 5.90 | 1.80 | −1.60 | 4.90 | ||
| P | 0.035 | <0.001 | 0.005 | 0.40 | <0.001 | ||
| Men | 140.25 ± 9.81 | 168.64 ± 5.18 | 170.02 ± 3.87 | 171.99 ± 9.18 | 159.85 ± 6.32 | 7.17 | 0.07 |
| Women | 136.42 ± 54.19 | 137.12 ± 58.18 | 142.91 ± 80.98 | 145.75 ± 36.14 | 142.14 ± 47.77 | 8.51 | 0.94 |
| unipolar depression | 138.03 ± 35.48 | 143.92 ± 46.75 | 162.49 ± 25.29 | 147.15 ± 34.70 | 148.02 ± 34.02 | 11.59 | 0.04 |
| Z | 1.67 | 0.60 | 0.31 | 1.3 | 1.20 | ||
| P | 0.11 | 0.58 | 0.80 | 0.26 | 0.29 | ||
| Men | 153.85 ±103.0 | 134.65 ± 116.1 | 145.45 ± 93.9 | 160.85 ± 95.25 | 140.21 ± 99.42 | 24.70 | <0.001 |
| Women | 127.95 ± 63.6 | 82.90 ± 33.75 | 116.20 ± 56.9 | 140.50 ± 66.7 | 110.34 ± 51.21 | 11.40 | 0.01 |
| Bipolar disorder | 139.63 ± 81.36 | 109.6 ± 77.54 | 127.88 ± 71.37 | 153.93 ± 85.67 | 125.18 ± 75.64 | 27.46 | <0.001 |
| Z | 0.01 | 0.1 | 0.40 | 1.41 | 0.60 | ||
| P | 0.89 | 0.81 | 0.82 | 0.09 | 0.70 | ||
| Men | 163.50 ± 88.10 | 199.20 ± 197.10 | 145.70 ± 75.30 | 175.10 ± 100.30 | 175.86 ± 130.62 | 0.75 | 0.86 |
| Women | 155.60 ± 76.60 | 80.50 ± 41.90 | 128.20 ± 70.60 | 166.90 ± 85.10 | 124.54 ± 64.35 | 10.77 | 0.16 |
| Bipolar depression | 159.45 ± 82.21 | 143.09 ± 123.73 | 135.62 ± 72.59 | 171.00 ± 93.71 | 149.68 ± 96.95 | 7.66 | 0.07 |
| Z | 1.73 | 0.60 | 0.31 | 0.20 | 1.08 | ||
| P | 0.12 | 0.55 | 0.80 | 0.23 | 0.30 | ||
| Men | 144.20 ± 117.90 | 70.10 ± 35.10 | 145.20 ± 112.50 | 146.60 ± 90.20 | 104.56 ± 68.22 | 5.55 | 0.08 |
| Women | 100.30 ± 50.60 | 85.30 ± 25.60 | 104.20 ± 43.20 | 114.10 ± 48.30 | 96.14 ± 38.08 | 0.90 | 0.85 |
| Bipolar mania | 119.81 ± 80.51 | 76.11 ± 31.34 | 120.14 ± 70.15 | 136.85 ± 77.63 | 100.68 ± 54.34 | 7.45 | 0.07 |
| Z | −1.85 | −0.50 | 0.51 | 1.11 | −0.70 | ||
| P | 0.08 | 0.60 | 0.60 | 0.29 | 0.53 | ||
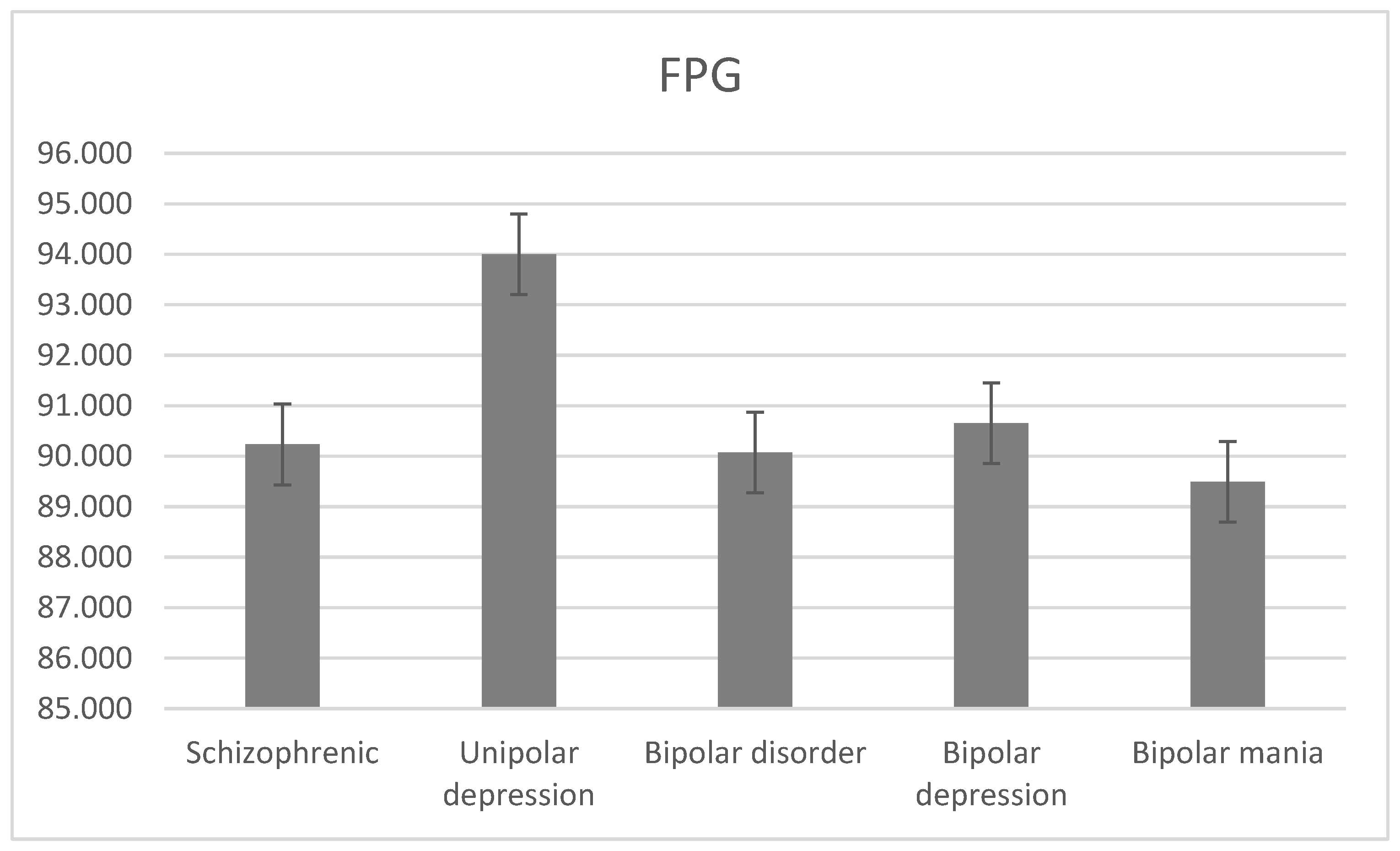
| FPG [mg/dL] | |||||||
| Male | 99.30 ± 42.30 | 88.90 ± 15.10 | 99.30 ± 22.90 | 93.30 ± 20.30 | 94.23 ± 21.83 | 25.30 | <0.001 |
| Female | 8.13 ± 16.10 | 93.70 ± 17.00 | 97.10 ± 23.60 | 106.60 ± 50.70 | 86.48 ± 19.90 | 22.37 | <0.001 |
| Schizophrenic | 57.71 ± 30.35 | 91.76 ± 16.23 | 98.23 ± 23.24 | 96.03 ± 26.54 | 90.23 ± 20.83 | 37.00 | <0.001 |
| Z | 0.80 | 1.80 | 2.02 | −1.65 | 0.90 | ||
| P | 0.33 | 0.06 | 0.03 | 0.08 | 0.40 | ||
| Men | 88.30 ± 10.20 | 83.30 ± 12.20 | 99.10 ± 33.20 | 102.20 ± 35.60 | 94.42 ± 23.92 | 23.50 | <0.001 |
| Women | 86.70 ± 10.90 | 84.60 ± 16.90 | 93.20 ± 16.70 | 99.30 ± 25.80 | 93.79 ± 20.23 | 35.70 | <0.001 |
| unipolar depression | 87.37 ± 10.60 | 84.32 ± 15.89 | 97.46 ± 28.62 | 99.45 ± 26.32 | 94.00 ± 21.45 | 53.74 | <0.001 |
| Z | −0.70 | 0.85 | 1.03 | 2.30 | 1.70 | ||
| P | 0.52 | 0.41 | 0.41 | 0.03 | 0.10 | ||
| Men | 83.20 ± 10.05 | 85.95 ± 15.90 | 94.50 ± 17.45 | 99.56 ± 15.79 | 88.38 ± 14.55 | 9.03 | 0.02 |
| Women | 82.45 ± 12.45 | 90.15 ± 7.1 | 103.60 ± 40.5 | 93.82 ± 18.95 | 92.06 ± 18.35 | 23.70 | <0.001 |
| Bipolar disorder | 82.92 ± 11.38 | 87.55 ± 11.99 | 99.87 ± 31.13 | 97.54 ± 17.08 | 90.07 ± 16.34 | 27.13 | <0.001 |
| Z | 0.02 | −0.18 | −2.10 | 1.33 | −0.90 | ||
| P | 0.98 | 0.50 | 0.05 | 0.30 | 0.45 | ||
| Men | 85.70 ± 10.80 | 91.20 ± 20.50 | 90.60 ± 17.30 | 99.01 ± 17.07 | 90.65 ± 16.76 | 6.70 | 0.08 |
| Women | 79.30 ± 10.90 | 89.70 ± 9.30 | 101.70 ± 40.50 | 96.04 ± 22.30 | 90.66 ± 19.25 | 8.71 | 0.04 |
| Bipolar depression | 82.42 ± 10.85 | 90.49 ± 15.21 | 96.99 ± 30.66 | 97.53 ± 19.34 | 90.65 ± 17.98 | 10.55 | 0.02 |
| Z | −1.70 | 1.70 | −2.25 | −0.25 | −1.71 | ||
| P | 0.12 | 0.35 | 0.03 | 0.08 | 0.11 | ||
| Men | 80.70 ± 9.30 | 80.70 ± 11.30 | 98.40 ± 17.60 | 100.10 ± 14.50 | 86.11 ± 12.35 | 8.29 | 0.03 |
| Women | 85.60 ± 14.00 | 90.60 ± 4.89 | 105.50 ± 40.50 | 91.60 ± 15.60 | 93.45 ± 17.45 | 5.20 | 0.17 |
| Bipolar mania | 83.42 ± 11.91 | 84.61 ± 8.77 | 102.74 ± 31.59 | 97.55 ± 14.83 | 89.49 ± 14.70 | 13.90 | 0.00 |
| Z | 0.55 | −1.30 | −0.52 | 1.31 | −1.12 | ||
| P | 0.61 | 0.40 | 0.71 | 0.14 | 0.28 | ||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Abdel-Qader, D.H.; Albassam, A.; Taybeh, E.; Al Mazrouei, N.; Meer, S.M.A.; Al-Kubaisi, K.A.; Ibrahim, R.; Elnour, A.A.; Mohamed Ibrahim, O.; AbuRuz, S. Lipid and Glucose Profile across Different Mental Disorders. J. Clin. Med. 2024, 13, 2499. https://doi.org/10.3390/jcm13092499
Abdel-Qader DH, Albassam A, Taybeh E, Al Mazrouei N, Meer SMA, Al-Kubaisi KA, Ibrahim R, Elnour AA, Mohamed Ibrahim O, AbuRuz S. Lipid and Glucose Profile across Different Mental Disorders. Journal of Clinical Medicine. 2024; 13(9):2499. https://doi.org/10.3390/jcm13092499
Chicago/Turabian StyleAbdel-Qader, Derar H., Abdullah Albassam, Esra’ Taybeh, Nadia Al Mazrouei, Sara Murad Albarkat Meer, Khalid Awad Al-Kubaisi, Rana Ibrahim, Asim Ahmed Elnour, Osama Mohamed Ibrahim, and Salah AbuRuz. 2024. "Lipid and Glucose Profile across Different Mental Disorders" Journal of Clinical Medicine 13, no. 9: 2499. https://doi.org/10.3390/jcm13092499