
Differential Prognostic Impact of Risk-Prediction Models for Heart Failure in Acute Myocardial Infarction: The Original and Revised Heart Failure Time-Points
 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Population
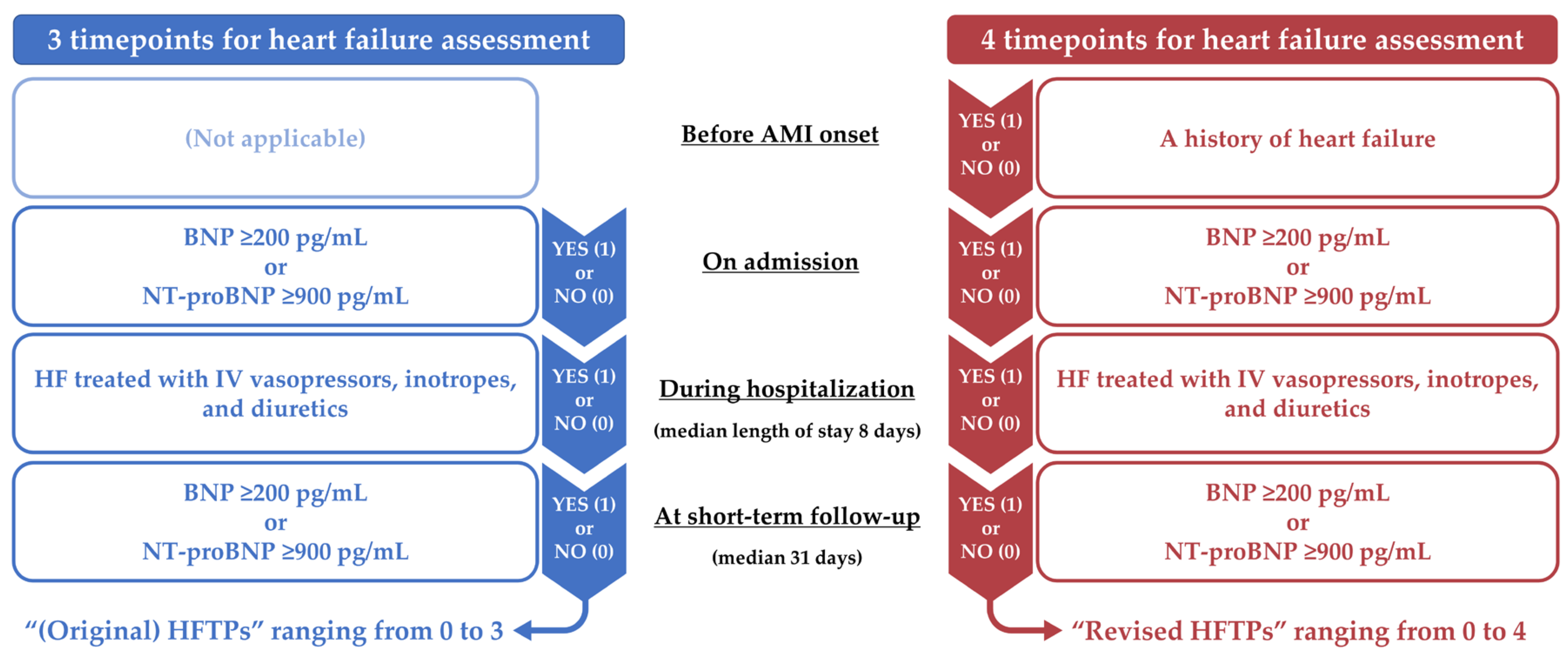
2.2. Heart Failure Evaluation
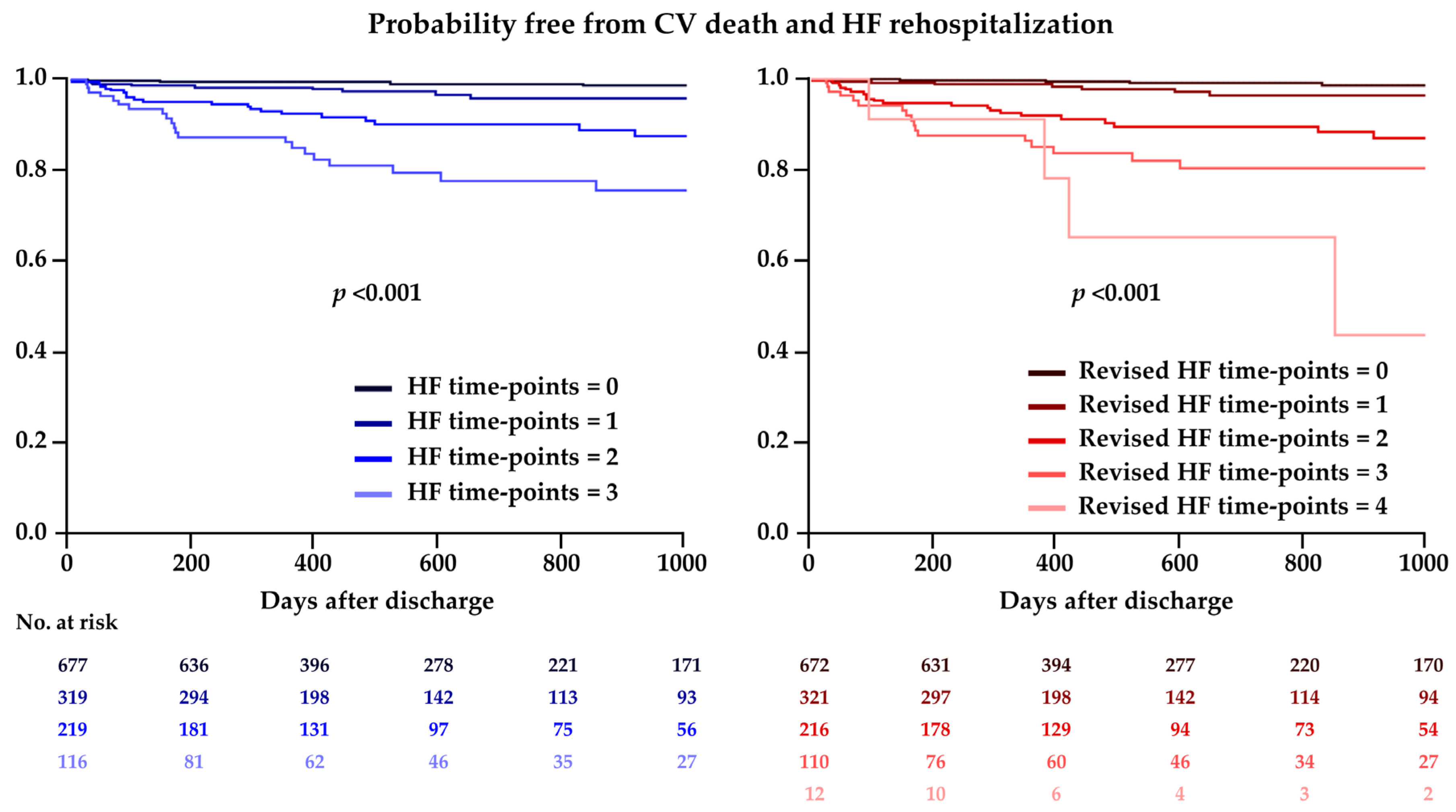
2.3. Outcomes and Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Shiba, N.; Nochioka, K.; Miura, M.; Kohno, H.; Shimokawa, H. CHART-2 Investigators. Trend of westernization of etiology and clinical characteristics of heart failure patients in Japan—First report from the CHART-2 study. Circ. J. 2011, 75, 823–833. [Google Scholar] [CrossRef] [PubMed]
- Tromp, J.; Ouwerkerk, W.; Cleland, J.G.F.; Angermann, C.E.; Dahlstrom, U.; Tiew-Hwa Teng, K.; Bamadhaj, S.; Ertl, G.; Hassanein, M.; Perrone, S.V.; et al. Global Differences in Burden and Treatment of Ischemic Heart Disease in Acute Heart Failure: REPORT-HF. JACC Heart Fail. 2021, 9, 349–359. [Google Scholar] [CrossRef] [PubMed]
- Gerber, Y.; Weston, S.A.; Enriquez-Sarano, M.; Berardi, C.; Chamberlain, A.M.; Manemann, S.M.; Jiang, R.; Dunlay, S.M.; Roger, V.L. Mortality Associated with Heart Failure After Myocardial Infarction: A Contemporary Community Perspective. Circ. Heart Fail. 2016, 9, e002460. [Google Scholar] [CrossRef] [PubMed]
- Frantz, S.; Hundertmark, M.J.; Schulz-Menger, J.; Bengel, F.M.; Bauersachs, J. Left ventricular remodelling post-myocardial infarction: Pathophysiology, imaging, and novel therapies. Eur. Heart J. 2022, 43, 2549–2561. [Google Scholar] [CrossRef] [PubMed]
- Lee, K.L.; Woodlief, L.H.; Topol, E.J.; Weaver, W.D.; Betriu, A.; Col, J.; Simoons, M.; Aylward, P.; Van de Werf, F.; Califf, R.M. Predictors of 30-day mortality in the era of reperfusion for acute myocardial infarction. Results from an international trial of 41,021 patients. GUSTO-I Investigators. Circulation 1995, 91, 1659–1668. [Google Scholar] [CrossRef]
- Kochar, A.; Doll, J.A.; Liang, L.; Curran, J.; Peterson, E.D. Temporal Trends in Post Myocardial Infarction Heart Failure and Outcomes Among Older Adults. J. Card. Fail. 2022, 28, 531–539. [Google Scholar] [CrossRef]
- Byrne, R.A.; Rossello, X.; Coughlan, J.J.; Barbato, E.; Berry, C.; Chieffo, A.; Claeys, M.J.; Dan, G.A.; Dweck, M.R.; Galbraith, M.; et al. 2023 ESC Guidelines for the management of acute coronary syndromes. Eur. Heart J. 2023, 44, 3720–3826. [Google Scholar] [CrossRef]
- Kimura, K.; Kimura, T.; Ishihara, M.; Nakagawa, Y.; Nakao, K.; Miyauchi, K.; Sakamoto, T.; Tsujita, K.; Hagiwara, N.; Miyazaki, S.; et al. JCS 2018 Guideline on Diagnosis and Treatment of Acute Coronary Syndrome. Circ. J. 2019, 83, 1085–1196. [Google Scholar] [CrossRef]
- Goetze, J.P.; Bruneau, B.G.; Ramos, H.R.; Ogawa, T.; de Bold, M.K.; de Bold, A.J. Cardiac natriuretic peptides. Nat. Rev. Cardiol. 2020, 17, 698–717. [Google Scholar] [CrossRef]
- Mega, J.L.; Morrow, D.A.; De Lemos, J.A.; Sabatine, M.S.; Murphy, S.A.; Rifai, N.; Gibson, C.M.; Antman, E.M.; Braunwald, E. B-type natriuretic peptide at presentation and prognosis in patients with ST-segment elevation myocardial infarction: An ENTIRE-TIMI-23 substudy. J. Am. Coll. Cardiol. 2004, 44, 335–339. [Google Scholar] [CrossRef]
- Suzuki, S.; Yoshimura, M.; Nakayama, M.; Mizuno, Y.; Harada, E.; Ito, T.; Nakamura, S.; Abe, K.; Yamamuro, M.; Sakamoto, T.; et al. Plasma level of B-type natriuretic peptide as a prognostic marker after acute myocardial infarction: A long-term follow-up analysis. Circulation 2004, 110, 1387–1391. [Google Scholar] [CrossRef] [PubMed]
- Bahit, M.C.; Lopes, R.D.; Clare, R.M.; Newby, L.K.; Pieper, K.S.; Van de Werf, F.; Armstrong, P.W.; Mahaffey, K.W.; Harrington, R.A.; Diaz, R.; et al. J Heart failure complicating non-ST-segment elevation acute coronary syndrome: Timing, predictors, and clinical outcomes. ACC Heart Fail. 2013, 1, 223–229. [Google Scholar] [CrossRef] [PubMed]
- Mebazaa, A.; Davison, B.; Chioncel, O.; Cohen-Solal, A.; Diaz, R.; Filippatos, G.; Metra, M.; Ponikowski, P.; Sliwa, K.; Voors, A.A.; et al. Safety, tolerability and efficacy of up-titration of guideline-directed medical therapies for acute heart failure (STRONG-HF): A multinational, open-label, randomised, trial. Lancet 2022, 400, 1938–1952. [Google Scholar] [CrossRef] [PubMed]
- Asada, K.; Saito, Y.; Sato, T.; Matsumoto, T.; Yamashita, D.; Suzuki, S.; Wakabayashi, S.; Kitahara, H.; Sano, K.; Kobayashi, Y. Prognostic Value of Natriuretic Peptide Levels and In-Hospital Heart Failure Events in Patients with Acute Myocardial Infarction. Circ. J. 2023, 87, 640–647. [Google Scholar] [CrossRef] [PubMed]
- Jenča, D.; Melenovský, V.; Stehlik, J.; Staněk, V.; Kettner, J.; Kautzner, J.; Adámková, V.; Wohlfahrt, P. Heart failure after myocardial infarction: Incidence and predictors. ESC Heart Fail. 2021, 8, 222–237. [Google Scholar] [CrossRef]
- Fox, K.A.; Dabbous, O.H.; Goldberg, R.J.; Pieper, K.S.; Eagle, K.A.; Van de Werf, F.; Avezum, A.; Goodman, S.G.; Flather, M.D.; Anderson, F.A., Jr.; et al. Prediction of risk of death and myocardial infarction in the six months after presentation with acute coronary syndrome: Prospective multinational observational study (GRACE). BMJ 2006, 333, 1091. [Google Scholar] [CrossRef] [PubMed]
- Abramov, D.; Kobo, O.; Mohamed, M.; Roguin, A.; Osman, M.; Patel, B.; Parwani, P.; Alraies, C.; Sauer, A.J.; Van Spall, H.G.C.; et al. Management and outcomes of acute myocardial infarction in patients with preexisting heart failure: An analysis of 2 million patients from the national inpatient sample. Expert Rev. Cardiovasc. Ther. 2022, 20, 233–240. [Google Scholar] [CrossRef] [PubMed]
- Matsumoto, T.; Saito, Y.; Yamashita, D.; Sato, T.; Wakabayashi, S.; Kitahara, H.; Sano, K.; Kobayashi, Y. Impact of Active and Historical Cancer on Short- and Long-Term Outcomes in Patients with Acute Myocardial Infarction. Am. J. Cardiol. 2021, 159, 59–64. [Google Scholar] [CrossRef] [PubMed]
- Yamashita, D.; Saito, Y.; Sato, T.; Matsumoto, T.; Saito, K.; Wakabayashi, S.; Kitahara, H.; Sano, K.; Kobayashi, Y. Impact of PARIS and CREDO-Kyoto Thrombotic and Bleeding Risk Scores on Clinical Outcomes in Patients with Acute Myocardial Infarction. Circ. J. 2022, 86, 622–629. [Google Scholar] [CrossRef]
- Suzuki, S.; Saito, Y.; Yamashita, D.; Matsumoto, T.; Sato, T.; Wakabayashi, S.; Kitahara, H.; Sano, K.; Kobayashi, Y. Clinical Characteristics and Prognosis of Patients with No Standard Modifiable Risk Factors in Acute Myocardial Infarction. Heart Lung. Circ. 2022, 31, 1228–1233. [Google Scholar] [CrossRef]
- Thygesen, K.; Alpert, J.S.; Jaffe, A.S.; Chaitman, B.R.; Bax, J.J.; Morrow, D.A.; White, H.D. Fourth Universal Definition of Myocardial Infarction (2018). J. Am. Coll. Cardiol. 2018, 72, 2231–2264. [Google Scholar] [CrossRef] [PubMed]
- Natsuaki, M.; Sonoda, S.; Yoshioka, G.; Hongo, H.; Kaneko, T.; Kashiyama, K.; Yokoi, K.; Hikichi, Y.; Node, K. Antiplatelet therapy after percutaneous coronary intervention: Current status and future perspectives. Cardiovasc. Interv. Ther. 2022, 37, 255–263. [Google Scholar] [CrossRef] [PubMed]
- Ozaki, Y.; Hara, H.; Onuma, Y.; Katagiri, Y.; Amano, T.; Kobayashi, Y.; Muramatsu, T.; Ishii, H.; Kozuma, K.; Tanaka, N.; et al. CVIT expert consensus document on primary percutaneous coronary intervention (PCI) for acute myocardial infarction (AMI) update 2022. Cardiovasc. Interv. Ther. 2022, 37, 1–34. [Google Scholar] [CrossRef] [PubMed]
- Saito, Y.; Kobayashi, Y.; Fujii, K.; Sonoda, S.; Tsujita, K.; Hibi, K.; Morino, Y.; Okura, H.; Ikari, Y.; Kozuma, K.; et al. CVIT 2023 clinical expert consensus document on intravascular ultrasound. Cardiovasc. Interv. Ther. 2024, 39, 1–14. [Google Scholar] [CrossRef] [PubMed]
- Fujii, K.; Kubo, T.; Otake, H.; Nakazawa, G.; Sonoda, S.; Hibi, K.; Shinke, T.; Kobayashi, Y.; Ikari, Y.; Akasaka, T. Expert consensus statement for quantitative measurement and morphological assessment of optical coherence tomography: Update 2022. Cardiovasc. Interv. Ther. 2022, 37, 248–254. [Google Scholar] [CrossRef] [PubMed]
- Saito, Y.; Kobayashi, Y. Contemporary coronary drug-eluting and coated stents: An updated mini-review (2023). Cardiovasc. Interv. Ther. 2024, 39, 15–17. [Google Scholar] [CrossRef] [PubMed]
- Saito, Y.; Tateishi, K.; Kanda, M.; Shiko, Y.; Kawasaki, Y.; Kobayashi, Y.; Inoue, T. Volume-outcome relationships for extracorporeal membrane oxygenation in acute myocardial infarction. Cardiovasc. Interv. Ther. 2024, 39, 156–163. [Google Scholar] [CrossRef] [PubMed]
- Ando, H.; Yamaji, K.; Kohsaka, S.; Ishii, H.; Wada, H.; Yamada, S.; Sawano, M.; Inohara, T.; Numasawa, Y.; Ikari, Y.; et al. Japanese Nationwide PCI (J-PCI) Registry Annual Report 2019: Patient demographics and in-hospital outcomes. Cardiovasc. Interv. Ther. 2022, 37, 243–247. [Google Scholar] [CrossRef]
- Tsutsui, H.; Ide, T.; Ito, H.; Kihara, Y.; Kinugawa, K.; Kinugawa, S.; Makaya, M.; Murohara, T.; Node, K.; Saito, Y.; et al. JCS/JHFS 2021 Guideline Focused Update on Diagnosis and Treatment of Acute and Chronic Heart Failure. Circ. J. 2021, 85, 2252–2291. [Google Scholar] [CrossRef]
- Sato, T.; Saito, Y.; Matsumoto, T.; Yamashita, D.; Saito, K.; Wakabayashi, S.; Kitahara, H.; Sano, K.; Kobayashi, Y. Impact of CADILLAC and GRACE risk scores on short- and long-term clinical outcomes in patients with acute myocardial infarction. J. Cardiol. 2021, 78, 201–205. [Google Scholar] [CrossRef]
- Garcia-Garcia, H.M.; McFadden, E.P.; Farb, A.; Mehran, R.; Stone, G.W.; Spertus, J.; Onuma, Y.; Morel, M.A.; van Es, G.A.; Zuckerman, B.; et al. Standardized End Point Definitions for Coronary Intervention Trials: The Academic Research Consortium-2 Consensus Document. Circulation 2018, 137, 2635–2650. [Google Scholar] [CrossRef]
- Bahit, M.C.; Kochar, A.; Granger, C.B. Post-Myocardial Infarction Heart Failure. JACC Heart Fail. 2018, 6, 179–186. [Google Scholar] [CrossRef] [PubMed]
- Armillotta, M.; Amicone, S.; Bergamaschi, L.; Angeli, F.; Rinaldi, A.; Paolisso, P.; Stefanizzi, A.; Sansonetti, A.; Impellizzeri, A.; Bodega, F.; et al. Predictive value of Killip classification in MINOCA patients. Eur. J. Intern. Med. 2023, 117, 57–65. [Google Scholar] [CrossRef] [PubMed]
- Pfeffer, M.A.; Braunwald, E.; Moyé, L.A.; Basta, L.; Brown, E.J., Jr.; Cuddy, T.E.; Davis, B.R.; Geltman, E.M.; Goldman, S.; Flaker, G.C.; et al. Effect of captopril on mortality and morbidity in patients with left ventricular dysfunction after myocardial infarction. Results of the survival and ventricular enlargement trial. The SAVE Investigators. N. Engl. J. Med. 1992, 327, 669–677. [Google Scholar] [CrossRef]
- Dargie, H.J. Effect of carvedilol on outcome after myocardial infarction in patients with left-ventricular dysfunction: The CAPRICORN randomised trial. Lancet 2001, 357, 1385–1390. [Google Scholar]
- Pitt, B.; Remme, W.; Zannad, F.; Neaton, J.; Martinez, F.; Roniker, B.; Bittman, R.; Hurley, S.; Kleiman, J.; Gatlin, M. Eplerenone, a selective aldosterone blocker, in patients with left ventricular dysfunction after myocardial infarction. N. Engl. J. Med. 2003, 348, 1309–1321. [Google Scholar] [CrossRef] [PubMed]
- von Lewinski, D.; Kolesnik, E.; Tripolt, N.J.; Pferschy, P.N.; Benedikt, M.; Wallner, M.; Alber, H.; Berger, R.; Lichtenauer, M.; Saely, C.H.; et al. Empagliflozin in acute myocardial infarction: The EMMY trial. Eur. Heart J. 2022, 43, 4421–4432. [Google Scholar] [CrossRef]
- Pfeffer, M.A.; Claggett, B.; Lewis, E.F.; Granger, C.B.; Køber, L.; Maggioni, A.P.; Mann, D.L.; McMurray, J.J.V.; Rouleau, J.L.; Solomon, S.D.; et al. Angiotensin Receptor-Neprilysin Inhibition in Acute Myocardial Infarction. N. Engl. J. Med. 2021, 385, 1845–1855. [Google Scholar] [CrossRef]
- Zannad, F.; Ferreira, J.P.; Pocock, S.J.; Anker, S.D.; Butler, J.; Filippatos, G.; Brueckmann, M.; Ofstad, A.P.; Pfarr, E.; Jamal, W.; et al. SGLT2 inhibitors in patients with heart failure with reduced ejection fraction: A meta-analysis of the EMPEROR-Reduced and DAPA-HF trials. Lancet 2020, 396, 819–829. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Variable | All (n = 1331) | Adverse Event (−) (n = 1266) | Adverse Event (+) (n = 65) | p Value |
|---|---|---|---|---|
| Age (years) | 67.1 ± 12.2 | 66.9 ± 12.3 | 70.9 ± 11.0 | 0.009 |
| Men | 1036 (77.8%) | 984 (77.7%) | 52 (80.0%) | 0.76 |
| Body mass index (kg/m2) | 24.5 ± 3.9 | 24.6 ± 3.9 | 23.4 ± 4.2 | 0.01 |
| Hypertension | 909 (68.3%) | 856 (67.6%) | 53 (81.5%) | 0.02 |
| Diabetes | 461 (34.6%) | 436 (34.4%) | 25 (38.5%) | 0.51 |
| Dyslipidemia | 890 (66.9%) | 850 (67.1%) | 40 (61.5%) | 0.35 |
| Current smoker | 496 (37.3%) | 474 (37.4%) | 22 (33.8%) | 0.60 |
| Previous MI | 105 (7.9%) | 94 (7.4%) | 11 (16.9%) | 0.02 |
| Previous PCI | 142 (10.7%) | 128 (10.1%) | 14 (21.5%) | 0.007 |
| eGFR (mL/min/1.73 m2) | 66.7 ± 23.1 | 67.7 ± 22.6 | 46.9 ± 23.7 | <0.001 |
| Hemoglobin (g/dL) | 14.2 ± 2.0 | 14.2 ± 1.9 | 12.8 ± 2.3 | <0.001 |
| LVEF (%) | 47.6 ± 11.2 | 48.0 ± 11.0 | 40.6 ± 13.0 | <0.001 |
| Cardiogenic shock | 123 (9.2%) | 119 (9.4%) | 4 (6.2%) | 0.51 |
| Type of MI | 0.26 | |||
| STEMI | 964 (72.4%) | 921 (72.7%) | 43 (66.2%) | |
| NSTEMI | 367 (27.6%) | 345 (27.3%) | 22 (33.8%) | |
| Medication at discharge | ||||
| Aspirin | 1227 (92.2%) | 1172 (92.6%) | 55 (84.6%) | 0.03 |
| P2Y12 inhibitor | 1283 (96.3%) | 1225 (96.8%) | 60 (92.3%) | 0.07 |
| Oral anticoagulation | 191 (14.4%) | 174 (13.7%) | 17 (26.2%) | 0.01 |
| Statin | 1267 (95.2%) | 1210 (95.6%) | 57 (87.7%) | 0.01 |
| ACE-i or ARB | 1043 (78.4%) | 992 (78.4%) | 51 (78.5%) | 1.00 |
| β-blocker | 1064 (79.9%) | 1011 (79.9%) | 53 (81.5%) | 0.87 |
| MRA | 249 (18.7%) | 229 (18.1%) | 20 (30.8%) | 0.01 |
| Diuretic | 265 (19.9%) | 227 (17.9%) | 38 (58.5%) | <0.001 |
| HF history before admission | 26 (2.0%) | 21 (1.7%) | 5 (7.7%) | 0.007 |
| High NP on admission | 350 (26.3%) | 311 (24.6%) | 39 (60.0%) | <0.001 |
| In-hospital HF | 288 (21.6%) | 248 (19.6%) | 40 (61.5%) | <0.001 |
| High NP at follow-up | 467 (35.1%) | 419 (33.1%) | 48 (73.8%) | <0.001 |
| Variable | Univariable | Multivariable (Original HFTPs) | Multivariable (Revised HFTPs) | |||
|---|---|---|---|---|---|---|
| HR (95% CI) | p Value | HR (95% CI) | p Value | HR (95% CI) | p Value | |
| Age (years) | 1.04 (1.01–1.06) | 0.002 | 1.00 (0.98–1.03) | 0.84 | 1.00 (0.98–1.03) | 0.86 |
| Men | 1.10 (0.60–2.01) | 0.77 | 1.60 (0.84–3.05) | 0.15 | 1.57 (0.82–3.01) | 0.17 |
| BMI (kg/m2) | 0.91 (0.86–0.98) | 0.009 | 0.96 (0.89–1.04) | 0.30 | 0.96 (0.89–1.04) | 0.32 |
| Hypertension | 2.04 (1.09–3.82) | 0.03 | 1.45 (0.73–2.84) | 0.28 | 1.44 (0.73–2.83) | 0.29 |
| eGFR (mL/min/1.73 m2) | 0.96 (0.95–0.97) | <0.001 | 0.98 (0.97–0.99) | 0.002 | 0.98 (0.97–0.99) | 0.004 |
| Hemoglobin (g/dL) | 0.75 (0.68–0.83) | <0.001 | 0.87 (0.76–0.99) | 0.04 | 0.87 (0.76–0.99) | 0.04 |
| LVEF (%) | 0.94 (0.92–0.96) | <0.001 | 0.98 (0.95–1.00) | 0.07 | 0.98 (0.95–1.00) | 0.07 |
| Cardiogenic shock | 0.65 (0.24–1.80) | 0.41 | 0.36 (0.11–1.19) | 0.10 | 0.38 (0.12–1.24) | 0.11 |
| Original HFTPs | ||||||
| 0 | Reference | Reference | ||||
| 1 | 3.45 (1.36–8.76) | 0.009 | 2.72 (0.99–7.45) | 0.051 | ||
| 2 | 10.54 (4.52–24.6) | <0.001 | 6.29 (2.35–16.8) | <0.001 | ||
| 3 | 21.48 (9.21–50.1) | <0.001 | 7.37 (2.48–21.9) | <0.001 | ||
| Revised HFTPs | ||||||
| 0 | Reference | Reference | ||||
| 1 | 3.11 (1.21–8.03) | 0.02 | 2.48 (0.89–6.90) | 0.08 | ||
| 2 | 11.19 (4.82–26.0) | <0.001 | 6.59 (2.47–17.6) | <0.001 | ||
| 3 | 18.08 (7.60–43.0) | <0.001 | 6.65 (2.22–19.9) | <0.001 | ||
| 4 | 40.32 (11.8–138.0) | <0.001 | 9.70 (2.25–41.8) | 0.002 | ||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Asada, K.; Saito, Y.; Goto, H.; Yaginuma, H.; Sato, T.; Hashimoto, O.; Kitahara, H.; Kobayashi, Y. Differential Prognostic Impact of Risk-Prediction Models for Heart Failure in Acute Myocardial Infarction: The Original and Revised Heart Failure Time-Points. J. Clin. Med. 2024, 13, 2501. https://doi.org/10.3390/jcm13092501
Asada K, Saito Y, Goto H, Yaginuma H, Sato T, Hashimoto O, Kitahara H, Kobayashi Y. Differential Prognostic Impact of Risk-Prediction Models for Heart Failure in Acute Myocardial Infarction: The Original and Revised Heart Failure Time-Points. Journal of Clinical Medicine. 2024; 13(9):2501. https://doi.org/10.3390/jcm13092501
Chicago/Turabian StyleAsada, Kazunari, Yuichi Saito, Hiroki Goto, Hiroaki Yaginuma, Takanori Sato, Osamu Hashimoto, Hideki Kitahara, and Yoshio Kobayashi. 2024. "Differential Prognostic Impact of Risk-Prediction Models for Heart Failure in Acute Myocardial Infarction: The Original and Revised Heart Failure Time-Points" Journal of Clinical Medicine 13, no. 9: 2501. https://doi.org/10.3390/jcm13092501