Effectiveness of Proadrenomedullin Enhanced CURB65 Score Algorithm in Patients with Community-Acquired Pneumonia in “Real Life”, an Observational Quality Control Survey

Abstract
:
1. Introduction
2. Methods
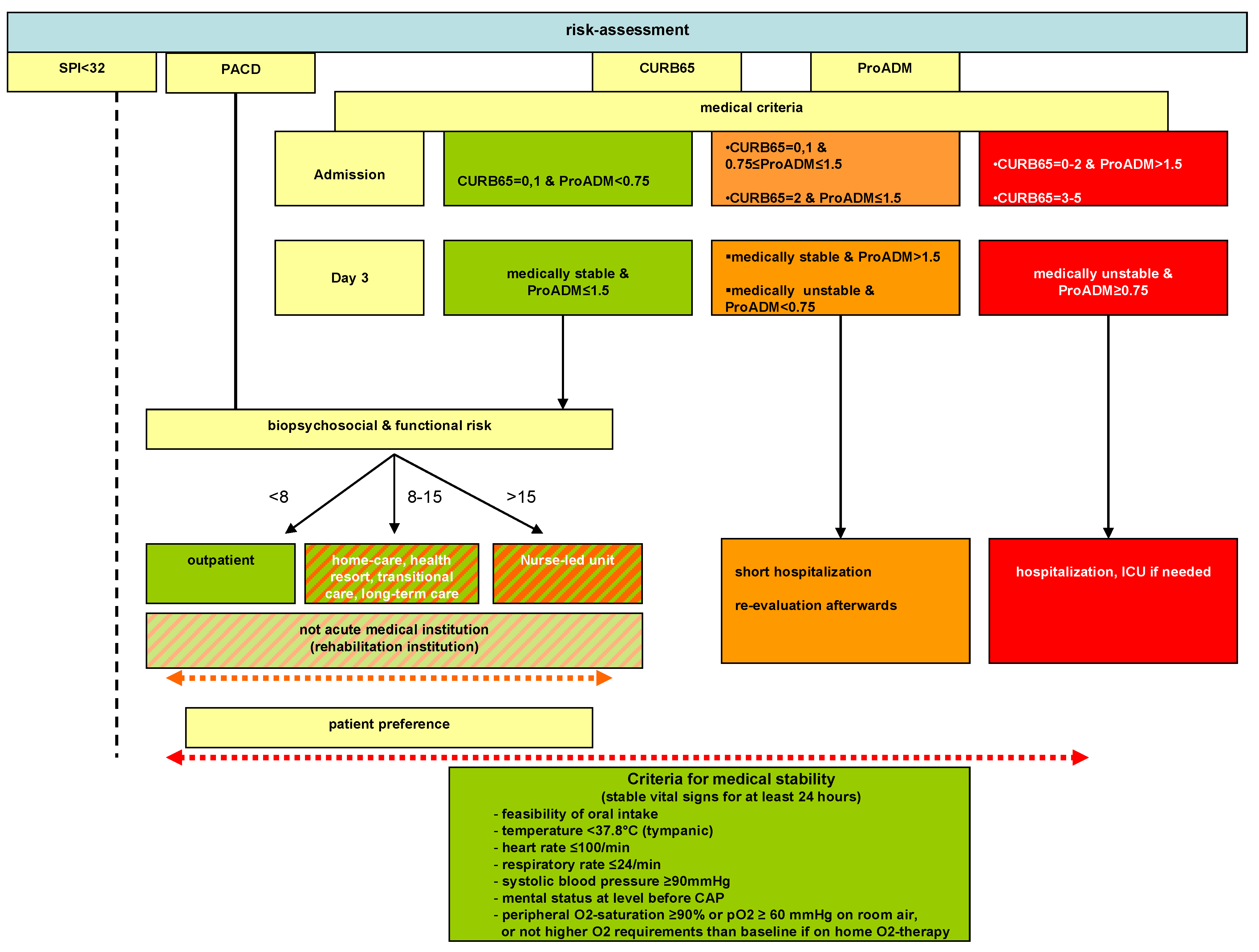
2.1. Medical Overruling Criteria
- Admission to ICU, based on respiratory (respiratory rate ≥ 30/min and/or SO2 < 90% with 6 L O2/min) or hemodynamic instability (systolic blood pressure for ≥1 h <90 mmHg despite adequate volume resuscitation or vasopressor requirement);
- Life-threatening co-morbidity, i.e., imminent death; complications (abscess, empyema); for COPD GOLD III & IV; O2-saturation < 90% despite 30 min intensive treatment;
- Acute illness requiring hospitalization independent from CAP;
- Comorbidity, i.e., immunodeficiency (neutrophils < 500/μL; if HIV+: CD4 < 350/μL, leukemia, lymphoma, myeloma, cytotoxic medications, hemodialysis), pneumonia within last 6 weeks, hospitalization independent of indication within the last week, other significant lung disease (cancer, fibrosis, bronchiectasis, tuberculosis, pulmonary embolism, cavitary lung disease);
- Confusion, delirium, or intravenous drug use.

2.3. Organizational Overruling Criteria
- Waiting for placement in a non-acute medical care facility (holiday bed, rehabilitation, nursing home, home health care);
- Waiting for laboratory results, imaging studies or consultant examinations.
2.4. Patient’s Preference Overruling Criteria
- Patient’s or relative’s concerns about safety at home;
- Lack of supporting social network;
- Financial reasons.
2.5. Definitions
2.6. End Points
2.7. Statistics
3. Results
3.1. Baseline Characteristics

{kind=link}
{kind=link}
{kind=link}
| Demographic Characteristics | Observation with ProADM | Intervention | Observation without ProADM | |
|---|---|---|---|---|
| (n = 89) | without ProADM (n = 93) | with ProADM (n = 76) | (n = 83) | |
| Mean age (years, range) | 64.3 (18–94) | 63.9 (18–93) | 67.6 (22–92) | 64.0 (16–93) |
| Sex (male), No. (%) | 52 (58.4%) | 56 (60.2%) | 49 (64.5%) | 47 (56.6%) |
| Initial treatment site, No. (%) | ||||
| Inpatient treatment | 85 (95.5%) | 81 (87.1%) | 55 (72.4%) | 76 (91.6%) |
| Outpatient treatment | 4 (4.5%) | 12 (12.9%) | 21 (27.6%) | 7 (8.4%) |
| Risk assessment | ||||
| CURB65 class (mean; median) | 1.6/1 | 1.7/1 | 1.7/1 | 1.9/2 |
| CURB65 I | 54 | 51 | 40 | 35 |
| CURB65 II | 20 | 24 | 19 | 17 |
| CURB65 III | 15 | 18 | 17 | 31 |
| CURB65-A class (mean; median) | 2.2/2 | not applicable | 2.2/2 | 2.2/2 |
| CURB65-A I (No.) | 13 | not applicable | 12 | 16 |
| CURB65-A II (No.) | 48 | not applicable | 35 | 32 |
| CURB65-A III (No.) | 28 | not applicable | 29 | 35 |
| Charlson comorbidity index (mean) | 4.6 | 3.9 | 3.8 | not available |
| Heart rate (bpm) | 98 | 96 | 94 | 100 |
| Temperature (°C) | 38 | 38 | 38 | 38.1 |
| Systolic blood pressure (mmHg) | 129.5 | 127.9 | 128.4 | 125.0 |
| Respiratory rate (/min) | 21.0 | 20.6 | 20.7 | 22.0 |
| Laboratory findings (mean) | ||||
| Proadrenomedullin (nmol/L) (admission) (mean, range) | 1.8 (0.4–12.2) | 1.6 (0.5–10.4) | 1.9 (0.4–22.1) | 1.3 (0.4–15.1) |
| Proadrenomedullin (nmol/L) (d3) (mean, range) | 2 (0.3–24.6) | 1.2 (0.4–4.6) (14 missing) | 1.4 (0.1–5.0) (13 missing) | not done |
| Procalcitonin (μg/L) (admission), (mean, range) | 3.1 (0.06–101) | 5.5 (0.06–170) | 3.4 (0.06–79.2) | 4.4 (0.06–58.4) |
| PCT < 0.25 (in %) | 38.2 (34/89) | 43.0 (40/93) | 44.7 (34/76) | 25.3 (21/83) |
| PCT 0.25–0.5 (in %) | 21.4 (19/89) | 20.4 (19/93) | 17.1 (13/76) | 18.1 (15/83) |
| PCT > 0.5 (in %) | 40.4 (36/89) | 35.6 (34/93) | 38.2 (29/76) | 56.6 (47/83) |
| C-Reactive protein, mg/L | 143.9 | 144.9 | 148.6 | not available |
| Leukocyte count, cells/μL | 12.8 | 13.4 | 12.8 | not available |
3.2. Allocation to Treatment Site according to Triage Algorithm
3.3. Historic Comparison
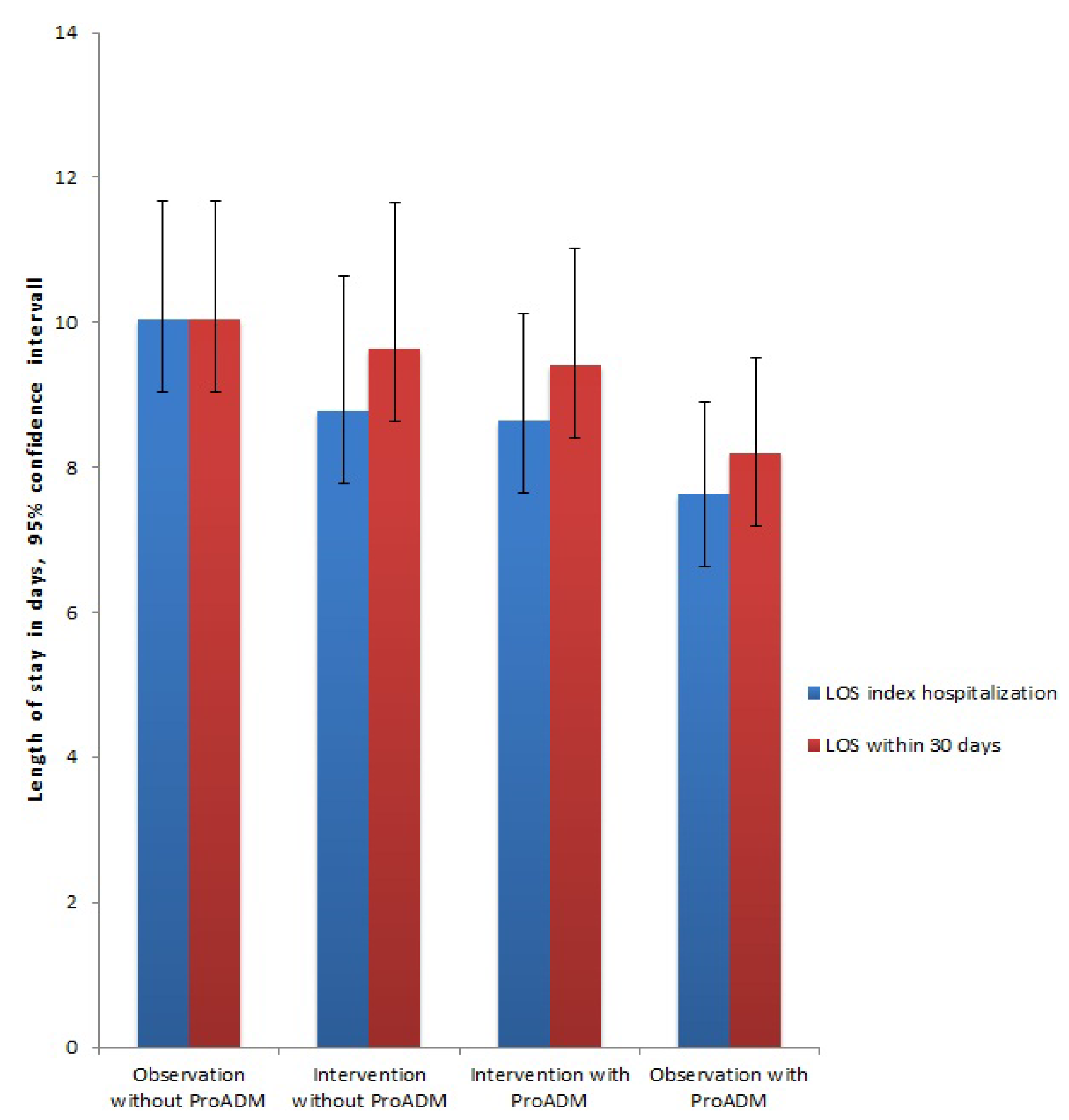
3.3.1. Length of Stay
| LOS during index hospitalization | ||
|---|---|---|
| Study | Regression Coefficient (95% CI) | p Value |
| Intervention without ProADM | −0.94 (−3.06 to 1.17) | 0.379 |
| Intervention with ProADM | 0.07 (−2.16 to 2.3) | 0.952 |
| Observation without ProADM | −2.32 (−4.51 to −0.13) | 0.038 |
| LOS within 30 days | ||
| Study | Regression Coefficient (95% CI) | p Value |
| Intervention without ProADM | −1.2 (−3.41 to 1.02) | 0.288 |
| Intervention with ProADM | −0.11 (−2.45 to 2.23) | 0.926 |
| Observation without ProADM | −1.84 (−4.14 to 0.46) | 0.116 |
| Mortality | ||
| Study | Adjusted OR (95% CI) | p Value |
| Intervention without ProADM | 0.47 (0.13 to 1.68) | 0.247 |
| Intervention with ProADM | 0.65 (0.2 to 2.09) | 0.465 |
| Observation without ProADM | 0.35 (0.09 to 1.29) | 0.115 |
| ICU admission | ||
| Study | Adjusted OR (95% CI) | p Value |
| Intervention without ProADM | 0.48 (0.15 to 1.53) | 0.214 |
| Intervention with ProADM | 0.43 (0.12 to 1.52) | 0.189 |
| Observation without ProADM | 0.65 (0.22 to 1.92) | 0.440 |

3.3.2. Mortality and ICU Admission
4. Discussion
5. Potential Limitations
6. Conclusions
Acknowledgments
Authors’ Contributions
Funding Sources
Conflicts of Interest
References
- File, T.M., Jr.; Marrie, T.J. Burden of community-acquired pneumonia in north American adults. Postgrad. Med. 2010, 122, 130–141. [Google Scholar] [CrossRef]
- Woodhead, M.; Blasi, F.; Ewig, S.; Garau, J.; Huchon, M.; Leven, M.; Ortqvist, A.; Schaberg, T.; Torres, A.; Read, R.; et al. Guidelines for the management of adult lower respiratory tract infections. Clin. Microbiol. Infect. 2011, 17, E1–E59. [Google Scholar]
- Fine, M.J.; Auble, T.E.; Yealy, D.M.; Hanusa, B.H.; Weissfeld, L.A.; Singer, D.E.; Coley, C.M.; Marrie, T.J.; Kapoor, W.N. A prediction rule to identify low-risk patients with community-acquired pneumonia. N. Engl. J. Med. 1997, 336, 243–250. [Google Scholar] [CrossRef]
- Christ-Crain, M.; Morgenthaler, N.G.; Stolz, D.; Muller, C.; Bingisser, R.; Harbarth, S.; Tamm, M.; Struck, J.; Bergmann, A.; Muller, B. Pro-adrenomedullin to predict severity and outcome in community-acquired pneumonia [ISRCTN04176397]. Crit. Care 2006, 10. [Google Scholar] [CrossRef]
- Huang, D.T.; Angus, D.C.; Kellum, J.A.; Pugh, N.A.; Weissfeld, L.A.; Struck, J.; Delude, R.L.; Rosengart, M.R.; Yealy, D.M. Midregional proadrenomedullin as a prognostic tool in community-acquired pneumonia. Chest 2009, 136, 823–831. [Google Scholar] [CrossRef]
- Lim, W.S.; van der Eerden, M.M.; Laing, R.; Boersma, W.G.; Karalus, N.; Town, G.I.; Lewis, S.A.; Macfarlane, J.T. Defining community acquired pneumonia severity on presentation to hospital: An international derivation and validation study. Thorax 2003, 58, 377–382. [Google Scholar] [CrossRef]
- Chalmers, J.D.; Singanayagam, A.; Akram, A.R.; Mandal, P.; Short, P.M.; Choudhury, G.; Wood, V.; Hill, A.T. Severity assessment tools for predicting mortality in hospitalised patients with community-acquired pneumonia. Systematic review and meta-analysis. Thorax 2010, 65, 878–883. [Google Scholar] [CrossRef]
- Albrich, W.C.; Dusemund, F.; Ruegger, K.; Christ-Crain, M.; Zimmerli, W.; Bregenzer, T.; Irani, S.; Buergi, U.; Reutlinger, B.; Mueller, B.; et al. Enhancement of CURB65 score with proadrenomedullin (CURB65-A) for outcome prediction in lower respiratory tract infections: Derivation of a clinical algorithm. BMC Infect. Dis. 2011, 11. [Google Scholar] [CrossRef]
- Albrich, W.C.; Ruegger, K.; Dusemund, F.; Bossart, R.; Regez, K.; Schild, U.; Conca, A.; Schuetz, P.; Sigrist, T.; Huber, A.; et al. Optimised patient transfer using an innovative multidisciplinary assessment in Kanton Aargau (OPTIMA I): An observational survey in lower respiratory tract infections. Swiss Med. Wkly. 2011, 141. [Google Scholar] [CrossRef]
- Conca, A.; Bossart, R.; Regez, K.; Schild, U.; Wallimann, G.; Schweingruber, R.; Hantikainen, V.; Tobias, P.; Albrich, W.; Ruegger, K.; et al. Optima—Optimierter patienten-transfer durch innovatives multidisziplinäres assessment. Projektbeschreibung der phase I. PrInt. Z. Pflegewissenschaft 2012, 14, 291–298. [Google Scholar]
- Labarere, J.; Stone, R.A.; Scott Obrosky, D.; Yealy, D.M.; Meehan, T.P.; Auble, T.E.; Fine, J.M.; Graff, L.G.; Fine, M.J. Factors associated with the hospitalization of low-risk patients with community-acquired pneumonia in a cluster-randomized trial. J. Gen. Intern. Med. 2006, 21, 745–752. [Google Scholar] [CrossRef]
- Baehni, C.; Meier, S.; Spreiter, P.; Schild, U.; Regez, K.; Bossart, R.; Thomann, R.; Falconnier, C.; Christ-Crain, M.; de Geest, S.; et al. Which patients with lower respiratory tract infections need inpatient treatment? Perceptions of physicians, nurses, patients and relatives. BMC Pulm. Med. 2010, 10. [Google Scholar] [CrossRef]
- McGregor, M.J.; Fitzgerald, J.M.; Reid, R.J.; Levy, A.R.; Schulzer, M.; Jung, D.; Groshaus, H.E.; Cox, M.B. Determinants of hospital length of stay among patients with pneumonia admitted to a large Canadian hospital from 1991 to 2001. Can. Respir. J. 2005, 12, 365–370. [Google Scholar]
- Louis Simonet, M.; Kossovsky, M.P.; Chopard, P.; Sigaud, P.; Perneger, T.V.; Gaspoz, J.M. A predictive score to identify hospitalized patients’ risk of discharge to a post-acute care facility. BMC Health Serv. Res. 2008, 8. [Google Scholar] [CrossRef]
- Große Schlarmann, J. Der CMS© im ePA©. In Verschiedene Qualitätsdimensionen eines Instruments; Eine Empirische Analyse; Private University Witten/Herdecke: Gelsenkirchen, Germany, 2007. [Google Scholar]
- Griffiths, P.D.; Edwards, M.H.; Forbes, A.; Harris, R.L.; Ritchie, G. Effectiveness of intermediate care in nursing-led in-patient units. Cochrane Database Syst. Rev. 2007, CD002214. [Google Scholar]
- Albrich, W.C.; Ruegger, K.; Dusemund, F.; Schuetz, P.; Arici, B.; Litke, A.; Blum, C.A.; Bossart, R.; Regez, K.; Schild, U.; et al. Biomarker-enhanced triage in respiratory infections—A proof-of-concept feasibility trial. Eur. Respir. J. 2013, 42, 1064–1075. [Google Scholar] [CrossRef]
- Fine, M.J.; Smith, M.A.; Carson, C.A.; Mutha, S.S.; Sankey, S.S.; Weissfeld, L.A.; Kapoor, W.N. Prognosis and outcomes of patients with community-acquired pneumonia. A meta-analysis. JAMA 1996, 275, 134–141. [Google Scholar] [CrossRef]
- Aujesky, D.; McCausland, J.B.; Whittle, J.; Obrosky, D.S.; Yealy, D.M.; Fine, M.J. Reasons why emergency department providers do not rely on the pneumonia severity index to determine the initial site of treatment for patients with pneumonia. Clin. Infect. Dis. 2009, 49, 100–108. [Google Scholar] [CrossRef]
- Karmakar, G.; Wilsher, M. Use of the “CURB 65” score in hospital practice. Intern. Med. J. 2010, 40, 828–832. [Google Scholar] [CrossRef]
- Schuetz, P.; Christ-Crain, M.; Thomann, R.; Falconnier, C.; Wolbers, M.; Widmer, I.; Neidert, S.; Fricker, T.; Blum, C.; Schild, U.; et al. Effect of procalcitonin-based guidelines vs. standard guidelines on antibiotic use in lower respiratory tract infections: The prohosp randomized controlled trial. JAMA 2009, 302, 1059–1066. [Google Scholar] [CrossRef]
- Hansson, J.; Korner, U.; Khorram-Manesh, A.; Solberg, A.; Lundholm, K. Randomized clinical trial of antibiotic therapy versus appendicectomy as primary treatment of acute appendicitis in unselected patients. Br. J. Surg. 2009, 96, 473–481. [Google Scholar] [CrossRef]
- Hansson, J.; Korner, U.; Ludwigs, K.; Johnsson, E.; Jonsson, C.; Lundholm, K. Antibiotics as first-line therapy for acute appendicitis: Evidence for a change in clinical practice. World J. Surg. 2012, 36, 2028–2036. [Google Scholar] [CrossRef]
- Drozdov, D.; Thomer, A.; Meili, M.; Schwarz, S.; Kouegbe, R.B.; Regez, K.; Guglielmetti, M.; Schild, U.; Conca, A.; Schafer, P.; et al. Procalcitonin, pyuria and proadrenomedullin in the management of urinary tract infections—“Triple p in uti”: Study protocol for a randomized controlled trial. Trials 2013, 14. [Google Scholar] [CrossRef]
- Litke, A.; Bossart, R.; Regez, K.; Schild, U.; Guglielmetti, M.; Conca, A.; Schafer, P.; Reutlinger, B.; Mueller, B.; Albrich, W.C. The potential impact of biomarker-guided triage decisions for patients with urinary tract infections. Infection 2013, 41, 799–809. [Google Scholar] [CrossRef]
- Schuetz, P.; Hausfater, P.; Amin, D.; Haubitz, S.; Fassler, L.; Grolimund, E.; Kutz, A.; Schild, U.; Caldara, Z.; Regez, K.; et al. Optimizing triage and hospitalization in adult general medical emergency patients: The triage project. BMC Emerg. Med. 2013, 13. [Google Scholar] [CrossRef]
© 2014 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution license (http://creativecommons.org/licenses/by/3.0/).
Share and Cite
Widmer, D.; Drozdov, D.; Rüegger, K.; Litke, A.; Arici, B.; Regez, K.; Guglielmetti, M.; Schild, U.; Conca, A.; Schäfer, P.; et al. Effectiveness of Proadrenomedullin Enhanced CURB65 Score Algorithm in Patients with Community-Acquired Pneumonia in “Real Life”, an Observational Quality Control Survey. J. Clin. Med. 2014, 3, 267-279. https://doi.org/10.3390/jcm3010267
Widmer D, Drozdov D, Rüegger K, Litke A, Arici B, Regez K, Guglielmetti M, Schild U, Conca A, Schäfer P, et al. Effectiveness of Proadrenomedullin Enhanced CURB65 Score Algorithm in Patients with Community-Acquired Pneumonia in “Real Life”, an Observational Quality Control Survey. Journal of Clinical Medicine. 2014; 3(1):267-279. https://doi.org/10.3390/jcm3010267
Chicago/Turabian StyleWidmer, Daniel, Daniel Drozdov, Kristina Rüegger, Alexander Litke, Birsen Arici, Katharina Regez, Merih Guglielmetti, Ursula Schild, Antoinette Conca, Petra Schäfer, and et al. 2014. "Effectiveness of Proadrenomedullin Enhanced CURB65 Score Algorithm in Patients with Community-Acquired Pneumonia in “Real Life”, an Observational Quality Control Survey" Journal of Clinical Medicine 3, no. 1: 267-279. https://doi.org/10.3390/jcm3010267