
Impact of Cannabis Use on Treatment Outcomes among Adults Receiving Cognitive-Behavioral Treatment for PTSD and Substance Use Disorders

Abstract
:1. Introduction
2. Experimental Section
2.1. Participants
2.2. Cognitive-Behavioral Interventions
2.3. Measures
2.4. Statistical Analyses
3. Results
4. Discussion
Acknowledgments
Author Contributions
Conflicts of Interest
References
- McCauley, J.L.; Killeen, T.; Gros, D.F.; Brady, K.T.; Back, S.E. Posttraumatic Stress Disorder and Co-Occurring Substance Use Disorders: Advances in Assessment and Treatment. Clin. Psychol. Sci. Pract. 2012, 19, 283–304. [Google Scholar] [CrossRef] [PubMed]
- Torchalla, I.; Nosen, L.; Rostam, H.; Allen, P. Integrated treatment programs for individuals with concurrent substance use disorders and trauma experiences: A systematic review and meta-analysis. J. Subst. Abuse Treat. 2012, 42, 65–77. [Google Scholar] [CrossRef] [PubMed]
- Debell, F.; Fear, N.T.; Head, M.; Batt-Rawden, S.; Greenberg, N.; Wessely, S.; Goodwin, L. A systematic review of the comorbidity between PTSD and alcohol misuse. Soc. Psychiatry Psychiatr. Epidemiol. 2014, 49, 1401–1425. [Google Scholar] [CrossRef] [PubMed]
- Roberts, N.P.; Roberts, P.A.; Jones, N.; Bisson, J.I. Psychological interventions for post-traumatic stress disorder and comorbid substance use disorder: A systematic review and meta-analysis. Clin. Psychol. Rev. 2015, 38, 25–38. [Google Scholar] [CrossRef] [PubMed]
- Boden, M.T.; Kimerling, R.; Jacobs-Lentz, J.; Bowman, D.; Weaver, C.; Carney, D.; Walser, R.; Trafton, J.A. Seeking Safety treatment for male veterans with a substance use disorder and post-traumatic stress disorder symptomatology. Addiction 2012, 107, 578–586. [Google Scholar] [CrossRef] [PubMed]
- Gentes, E.L.; Schry, A.R.; Hicks, T.A.; Clancy, C.P.; Collie, C.F.; Kirby, A.C.; Dennis, M.F.; Hertzberg, M.A.; Beckham, J.C.; Calhoun, P.S. Prevalence and correlates of cannabis use in an outpatient VA posttraumatic stress disorder clinic. Psychol. Addict. Behav. 2016, 30, 415–421. [Google Scholar] [CrossRef] [PubMed]
- Cougle, J.R.; Bonn-Miller, M.O.; Vujanovic, A.A.; Zvolensky, M.J.; Hawkins, K.A. Posttraumatic stress disorder and cannabis use in a nationally representative sample. Psychol. Addict. Behav. 2011, 25, 554–558. [Google Scholar] [CrossRef] [PubMed]
- Kevorkian, S.; Bonn-Miller, M.O.; Belendiuk, K.; Carney, D.M.; Roberson-Nay, R.; Berenz, E.C. Associations among trauma, posttraumatic stress disorder, cannabis use, and cannabis use disorder in a nationally representative epidemiologic sample. Psychol. Addict. Behav. 2015, 29, 633–638. [Google Scholar] [CrossRef] [PubMed]
- Brown, P.J.; Wolfe, J. Substance abuse and post-traumatic stress disorder comorbidity. Drug Alcohol Depend. 1994, 35, 51–59. [Google Scholar] [CrossRef]
- Van Dam, D.; Vedel, E.; Ehring, T.; Emmelkamp, P.M.G. Psychological treatments for concurrent posttraumatic stress disorder and substance use disorder: A systematic review. Clin. Psychol. Rev. 2012, 32, 202–214. [Google Scholar] [CrossRef] [PubMed]
- Brady, K.T.; Back, S.E.; Coffey, S.F. Substance abuse and posttraumatic stress disorder. Curr. Dir. Psychol. Sci. 2004, 13, 206–209. [Google Scholar] [CrossRef]
- Ruglass, L.M.; Lopez-Castro, T.; Cheref, S.; Papini, S.; Hien, D.A. At the crossroads: The intersection of substance use disorders, anxiety disorders, and posttraumatic stress disorder. Curr. Psychiatry Rep. 2014, 16, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Vujanovic, A.A.; Bonn-Miller, M.O.; Petry, N.M. Co-occurring posttraumatic stress and substance use: Emerging research on correlates, mechanisms, and treatments—Introduction to the special issue. Psychol. Addict. Behav. 2016, 30, 713–719. [Google Scholar] [CrossRef] [PubMed]
- Eiroa-Orosa, F.J.; Giannoni-Pastor, A.; Fidel-Kinori, S.G.; Argüello, J.M. Substance use and misuse in burn patients: Testing the classical hypotheses of the interaction between post-traumatic symptomatology and substance use. J. Addict. Dis. 2016, 35, 194–204. [Google Scholar] [CrossRef] [PubMed]
- Reed, P.L.; Anthony, J.C.; Breslau, N. Incidence of drug problems in young adults exposed to trauma and posttraumatic stress disorder: Do early life experiences and predispositions matter? Arch. Gen. Psychiatry 2007, 64, 1435–1442. [Google Scholar] [CrossRef] [PubMed]
- Chilcoat, H.D.; Breslau, N. Posttraumatic stress disorder and drug disorders: Testing causal pathways. Arch. Gen. Psychiatry 1998, 55, 913–917. [Google Scholar] [CrossRef] [PubMed]
- Back, S.E.; Brady, K.T.; Jaanimägi, U.; Jackson, J.L. Cocaine dependence and PTSD: A pilot study of symptom interplay and treatment preferences. Addict. Behav. 2006, 31, 351–354. [Google Scholar] [CrossRef] [PubMed]
- Boden, M.T.; Babson, K.A.; Vujanovic, A.A.; Short, N.A.; Bonn-Miller, M.O. Posttraumatic stress disorder and cannabis use characteristics among military veterans with cannabis dependence. Am. J. Addict. 2013, 22, 277–284. [Google Scholar] [CrossRef] [PubMed]
- Bonn-Miller, M.O.; Vujanovic, A.A.; Boden, M.T.; Gross, J.J. Posttraumatic stress, difficulties in emotion regulation, and coping-oriented marijuana use. Cogn. Behav. Ther. 2011, 40, 34–44. [Google Scholar] [CrossRef] [PubMed]
- Norman, S.B.; Myers, U.S.; Wilkins, K.C.; Goldsmith, A.A.; Hristova, V.; Huang, Z.; McCullough, K.C.; Robinson, S.K. Review of biological mechanisms and pharmacological treatments of comorbid PTSD and substance use disorder. Neuropharmacology 2012, 62, 542–551. [Google Scholar] [CrossRef] [PubMed]
- Koenen, K.C. Developmental epidemiology of PTSD: Self-regulation as a central mechanism. Ann. N. Y. Acad. Sci. 2006, 1071, 255–266. [Google Scholar] [CrossRef] [PubMed]
- Sloboda, Z.; Glantz, M.D.; Tarter, R.E. Revisiting the Concepts of Risk and Protective Factors for Understanding the Etiology and Development of Substance Use and Substance Use Disorders: Implications for Prevention. Subst. Use Misuse 2012, 47, 944–962. [Google Scholar] [CrossRef] [PubMed]
- Swift, W.; Coffey, C.; Degenhardt, L.; Carlin, J.B.; Romaniuk, H.; Patton, G.C. Cannabis and progression to other substance use in young adults: Findings from a 13-year prospective population-based study. J. Epidemiol. Community Health 2012, 66, e26. [Google Scholar] [CrossRef] [PubMed]
- Blanco, C.; Hasin, D.S.; Wall, M.M.; Flórez-Salamanca, L.; Hoertel, N.; Wang, S.; Kerridge, B.T.; Olfson, M. Cannabis Use and Risk of Psychiatric Disorders: Prospective Evidence From a US National Longitudinal Study. JAMA Psychiatry 2016, 73, 388–395. [Google Scholar] [CrossRef] [PubMed]
- Connor, J.P.; Gullo, M.J.; White, A.; Kelly, A.B. Polysubstance use: Diagnostic challenges, patterns of use and health. Curr. Opin. Psychiatry 2014, 27, 269–275. [Google Scholar] [CrossRef] [PubMed]
- Betthauser, K.; Pilz, J.; Vollmer, L.E. Use and effects of cannabinoids in military veterans with posttraumatic stress disorder. Am. J. Health. Syst. Pharm. 2015, 72, 1279–1284. [Google Scholar] [CrossRef] [PubMed]
- Passie, T.; Emrich, H.M.; Karst, M.; Brandt, S.D.; Halpern, J.H. Mitigation of post-traumatic stress symptoms by Cannabis resin: A review of the clinical and neurobiological evidence. Drug Test. Anal. 2012, 4, 649–659. [Google Scholar] [CrossRef] [PubMed]
- Elliott, L.; Golub, A.; Bennett, A.; Guarino, H. PTSD and Cannabis-Related Coping Among Recent Veterans in New York City. Contemp. Drug Probl. 2015, 42, 60–76. [Google Scholar] [CrossRef]
- Berardi, A.; Schelling, G.; Campolongo, P. The endocannabinoid system and Post Traumatic Stress Disorder (PTSD): From preclinical findings to innovative therapeutic approaches in clinical settings. Pharmacol. Res. 2016, 111, 668–678. [Google Scholar] [CrossRef] [PubMed]
- Papini, S.; Sullivan, G.M.; Hien, D.A.; Shvil, E.; Neria, Y. Toward a translational approach to targeting the endocannabinoid system in posttraumatic stress disorder: A critical review of preclinical research. Biol. Psychol. 2015, 104, 8–18. [Google Scholar] [CrossRef] [PubMed]
- Papini, S.; Ruglass, L.M.; Lopez-Castro, T.; Powers, M.B.; Smits, J.A.J.; Hien, D.A. Chronic cannabis use is associated with impaired fear extinction in humans. J. Abnorm. Psychol. 2017, 126, 117. [Google Scholar] [CrossRef] [PubMed]
- Lin, H.-C.; Mao, S.-C.; Chen, P.-S.; Gean, P.-W. Chronic cannabinoid administration in vivo compromises extinction of fear memory. Learn. Mem. 2008, 15, 876–884. [Google Scholar] [CrossRef] [PubMed]
- Alessi, S.M.; Rash, C.; Petry, N.M. Contingency management is efficacious and improves outcomes in cocaine patients with pretreatment marijuana use. Drug Alcohol Depend. 2011, 118, 62–67. [Google Scholar] [CrossRef] [PubMed]
- Budney, A.J.; Bickel, W.K.; Amass, L. Marijuana use and treatment outcome among opioid-dependent patients. Addiction 1998, 93, 493–503. [Google Scholar] [CrossRef] [PubMed]
- Hill, K.P.; Bennett, H.E.; Griffin, M.L.; Connery, H.S.; Fitzmaurice, G.M.; Subramaniam, G.; Woody, G.E.; Weiss, R.D. Association of cannabis use with opioid outcomes among opioid-dependent youth. Drug Alcohol Depend. 2013, 132, 342–345. [Google Scholar] [CrossRef] [PubMed]
- Scavone, J.L.; Sterling, R.C.; Weinstein, S.P.; Van Bockstaele, E.J. Impact of Cannabis Use during Stabilization on Methadone Maintenance Treatment. Am. J. Addict. 2013, 22, 344–351. [Google Scholar] [CrossRef] [PubMed]
- Budney, A.J.; Higgins, S.T.; Wong, C.J. Marijuana use and treatment outcome in cocaine-dependent patients. Exp. Clin. Psychopharmacol. 1996, 4, 396–403. [Google Scholar] [CrossRef]
- Aharonovich, E.; Liu, X.; Samet, S.; Nunes, E.; Waxman, R.; Hasin, D. Postdischarge cannabis use and its relationship to cocaine, alcohol, and heroin use: A prospective study. Am. J. Psychiatry 2005, 162, 1507–1514. [Google Scholar] [CrossRef] [PubMed]
- Green, C.; Schmitz, J.; Lindsay, J.; Pedroza, C.; Lane, S.; Agnelli, R.; Kjome, K.; Moeller, F.G. The influence of baseline marijuana use on treatment of cocaine dependence: Application of an informative-priors bayesian approach. Front. Psychiatry 2012, 3, 92. [Google Scholar] [CrossRef] [PubMed]
- Wasserman, D.A.; Weinstein, M.G.; Havassy, B.E.; Hall, S.M. Factors associated with lapses to heroin use during methadone maintenance. Drug Alcohol Depend. 1998, 52, 183–192. [Google Scholar] [CrossRef]
- Hien, D.A.; Levin, F.R.; Ruglass, L.M.; Lopez-Castro, T.; Papini, S.; Hu, M.C.; Cohen, L.R. Enhancing the effects of cognitive behavioral therapy for PTSD and alcohol use disorders with antidepressant medication: A randomized clinical trial. Drug Alcohol Depend. 2015, 146, e142. [Google Scholar] [CrossRef]
- Ruglass, L.M.; Lopez-Castro, T.; Papini, S.; Killeen, T.; Back, S.; Hien, D.A. Concurrent treatment with prolonged exposure for co-occurring full or subthreshold posttraumatic stress disorder and substance use disorders: A randomized clinical trial. Psychother Psychosom. under review.
- Najavits, L.M. Seeking Safety: A Treatment Manual for PTSD and Substance Abuse; Guilford Press: New York, NY, USA, 2002. [Google Scholar]
- Back, S.E.; Foa, E.B.; Killeen, T.K.; Mills, K.L.; Teesson, M.; Cotton, B.D.; Carroll, K.M.; Brady, K.T. Concurrent Treatment of PTSD and Substance Use Disorders Using Prolonged Exposure (COPE): Therapist Guide; Oxford University Press: New York, NY, USA, 2014. [Google Scholar]
- Carroll, K.M. A Cognitive Behavioral Approach: Treating Cocaine Addiction; National Institute on Drug Abuse: Rockville, MD, USA, 1998. [Google Scholar]
- Marlatt, G.A.; Donovan, D.M. Relapse Prevention: Maintenance Strategies in the Treatment of Addictive Behaviors; Guilford Press: New York, NY, USA, 2007. [Google Scholar]
- First, M.B.; Spitzer, R.L.; Gibbon, M.; Williams, J.B.W. Structured Clinical Interview for DSM-IV-TR Axis I Disorders, Research Version, Patient Edition with Psychotic Screen; Biometrics Research, New York State Psychiatric Institute: New York, NY, USA, 2002. [Google Scholar]
- Blake, D.D.; Weathers, F.W.; Nagy, L.M.; Kaloupek, D.G.; Gusman, F.D.; Charney, D.S.; Keane, T.M. The development of a clinician-administered PTSD scale. J. Trauma. Stress 1995, 8, 75–90. [Google Scholar] [CrossRef] [PubMed]
- Falsetti, S.A.; Resnick, H.S.; Resick, P.A.; Kilpatrick, D.G. The Modified PTSD Symptom Scale: A brief self-report measure of posttraumatic stress disorder. Behav. Ther. 1993, 16, 161–162. [Google Scholar]
- Ruglass, L.M.; Papini, S.; Trub, L.; Hien, D.A. Psychometric Properties of the Modified Posttraumatic Stress Disorder Symptom Scale among Women with Posttraumatic Stress Disorder and Substance Use Disorders Receiving Outpatient Group Treatments. J. Trauma. Stress Disord. Treat. 2014, 4, 1–7. [Google Scholar]
- Sobell, L.C.; Sobell, M.B. Timeline Follow-Back. In Measuring Alcohol Consumption; Humana Press: Totowa, NJ, USA, 1992; pp. 41–72. [Google Scholar]
- Sobell, L.C.; Sobell, M.B.; Leo, G.I.; Cancilla, A. Reliability of a timeline method: Assessing normal drinkers’ reports of recent drinking and a comparative evaluation across several populations. Br. J. Addict. 1988, 83, 393–402. [Google Scholar] [CrossRef] [PubMed]
- Thomas McLellan, A.; Cacciola, J.C.; Alterman, A.I.; Rikoon, S.H.; Carise, D. The Addiction Severity Index at 25: Origins, Contributions and Transitions. Am. J. Addict. 2006, 15, 113–124. [Google Scholar] [CrossRef] [PubMed]
- Cacciola, J.S.; Alterman, A.I.; McLellan, A.T.; Lin, Y.-T.; Lynch, K.G. Initial evidence for the reliability and validity of a “Lite” version of the Addiction Severity Index. Drug Alcohol Depend. 2007, 87, 297–302. [Google Scholar] [CrossRef] [PubMed]
- Weiss, R.D.; Hufford, C.; Najavits, L.M. Weekly Substance Use Inventory (Unpublishe); Harvard Medical School: Boston, MA, USA, 1995. [Google Scholar]
- StataCorp. Stata Statistical Software: Release 14, StataCorp LP: College Station, TX, USA, 2015.
- Templin, J. Applied Multilevel Models for Cross-Sectional Data Lecture 13. Available online: http//jonathantemplin.com/files/mlm/mlm13icpsr/mlm13icpsr_lecture13.pdf (accessed on 16 September 2016).
- Lindsay, J.A.; Stotts, A.L.; Green, C.E.; Herin, D.V.; Schmitz, J.M. Cocaine Dependence and Concurrent Marijuana Use: A Comparison of Clinical Characteristics. Am. J. Drug Alcohol Abuse 2009, 35, 193–198. [Google Scholar] [CrossRef] [PubMed]
- Bonn-Miller, M.O.; Boden, M.T.; Vujanovic, A.A.; Drescher, K.D. Prospective investigation of the impact of cannabis use disorders on posttraumatic stress disorder symptoms among veterans in residential treatment. Psychol. Trauma Theory Res. Pract. Policy 2013, 5, 193–200. [Google Scholar] [CrossRef]
- Degenhardt, L.; Hall, W. Extent of illicit drug use and dependence, and their contribution to the global burden of disease. Lancet 2012, 379, 55–70. [Google Scholar] [CrossRef]

{kind=link}
| Variables | Non-Users (n = 104) | Cannabis Users (n = 32) | Statistics | |
|---|---|---|---|---|
| M (SD) or % | ||||
| Age | 44 (9.18) | 41.63 (9.38) | t = 1.273, p = 0.205 | |
| Gender (Male %) | 42% (n = 44) | 66% (n = 21) | χ2 = 5.33, p = 0.021 | |
| Education | 13.28 (2.52) | 13.08 (1.88) | t = 0.426, p = 0.671 | |
| Employment in the Past 3 Years * | % Employed | 69.23% (n = 72) | 78.13% (n = 25) | χ2 = 5.12, p = 0.402 |
| % Unemployed | 30.77% (n = 32) | 21.87% (n = 7) | ||
| Race/Ethnicity † | % White | 21.87 (n = 21) | 12.5 (n = 4) | χ2 = 5.12, p = 0.163 |
| % Black | 59.38 (n = 57) | 56.25 (n = 18) | ||
| % Hispanic | 12.5 (n = 12) | 28.12 (n = 9) | ||
| % Other (i.e., Native American) | 6.25 (n = 6) | 3.125 (n = 1) | ||
| Cocaine Use Disorder (% Yes) † | 37.5 (n = 36) | 59.37 (n = 19) | χ2 = 4.686, p = 0.030 | |
| Alcohol Use Disorder (% Yes) † | 94.79 (n = 91) | 78.13 (n = 25) | χ2 = 7.847, p = 0.005 | |
| Other SUD (Opioid, Hallucinogen; % Yes) † | 5.2 (n = 5) | 6.25 (n = 2) | χ2 = 3.403, p = 0.334 | |
| Variables | Age | Education | Days of Cannabis Use † | Days of Urge, Desire or Craving for Cannabis † | Baseline Primary Substance Use ‡ | End-of-Treatment Primary Substance Use ‡ | Baseline CAPS 1 | End-of-Treatment CAPS 1 |
|---|---|---|---|---|---|---|---|---|
| Age | 1 | 0.101 | −0.009 | −0.031 | −0.011 | −0.077 | 0.006 | −0.051 |
| Education | 1 | −0.114 | −0.194 | −0.091 | 0.129 | −0.022 | −0.001 | |
| Days of cannabis use † | 1 | 0.844 ** | 0.007 | 0.004 | 0.069 | 0.157 | ||
| Days of urge, desire or craving for cannabis † | 1 | 0.073 | −0.028 | 0.113 | 0.081 | |||
| Baseline Primary Substance use ‡ | 1 | 0.049 | 0.094 | −0.016 | ||||
| End-of-treatment Primary Substance use ‡ | 1 | 0.140 | 0.370 ** | |||||
| Baseline CAPS | 1 | 0.377 ** | ||||||
| End-of-treatment CAPS | 1 |
| Predictors | Unadjusted Model IRR (95% CI) | Final Adjusted Model IRR (95% CI) |
|---|---|---|
| Status at Week 2 of Treatment: | ||
| Intercept | 7.81 (5.05, 12.07) *** | 7.12 (5.32, 9.53) *** |
| Sex (female) | -- | NS |
| Age | -- | 0.96 (0.93, 0.98) *** |
| Lagged Cannabis Use | 0.74 (0.67, 0.80) *** | 0.74 (0.69, 0.79) *** |
| Lagged PTSD | 1.00 (1.00, 1.01) | NS |
| Rate of Change: | ||
| Time (linear) | 0.91 (0.87, 0.95) *** | 0.91 (0.89, 0.93) |
| Lagged Cannabis Use X Time (linear) | 0.98 (0.96, 1.00) | NS |
| Lagged PTSD X Time (linear) | 1.00 (1.00, 1.00) | NS |
| Variables | Unadjusted Model IRR (95% CI) | Final Adjusted Model IRR (95% CI) |
|---|---|---|
| Status at Week 2 of Treatment: | ||
| Intercept | 1.71 (0.85, 3.45) | 2.25 (1.42, 3.53) *** |
| Sex (female) | -- | 0.23 (0.15, 0.34) *** |
| Age | -- | 0.92 (0.89, 0.95) *** |
| Lagged Primary Substance Use | 0.83 (0.74, 0.93) ** | 0.86 (0.80, 0.93) *** |
| Lagged PTSD | 1.00 (1.00, 1.01) | NS |
| Rate of Change: | ||
| Time (linear) | 0.90 (0.81, 1.00) | 0.91 (0.86, 0.96) *** |
| Lagged Primary Substance use X Time (linear) | 1.00 (0.97, 1.02) | NS |
| Lagged PTSD X Time | 1.00 (1.00, 1.00) | NS |
| Variables | Unadjusted Model | Adjusted Model |
|---|---|---|
| Status at Week 2 of Treatment: | ||
| Intercept | 45.41 (39.85, 50.98) *** | 45.71 (40.65, 50.77) *** |
| Lagged Cannabis Use | 1.04 (−0.30, 2.37) | NS |
| Lagged Primary Substance Use | −0.06 (−1.05, 0.93) | 0.98 (−0.25, 2.21) |
| Sex (female) | -- | NS |
| Age | -- | NS |
| Rate of Change: | ||
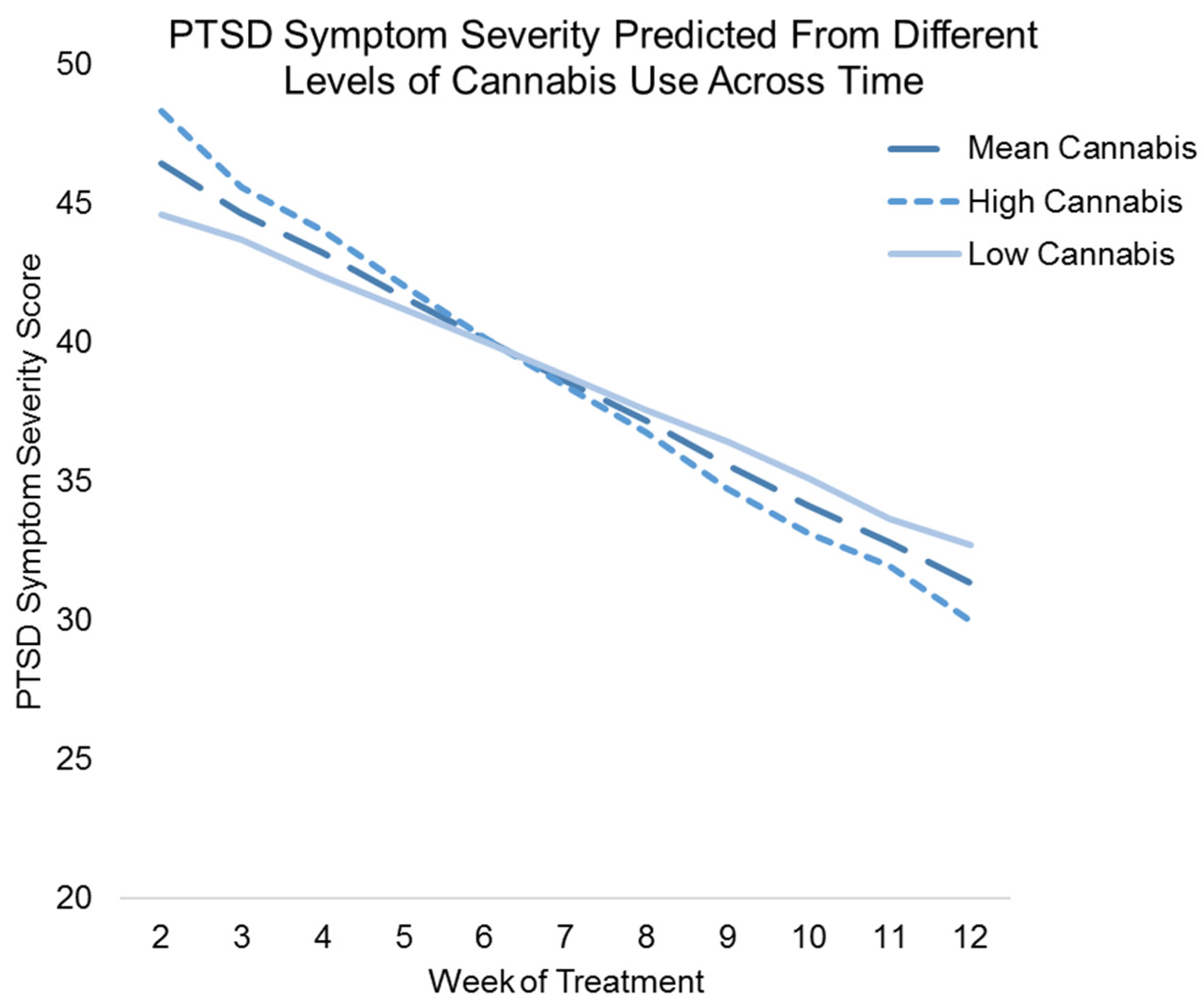
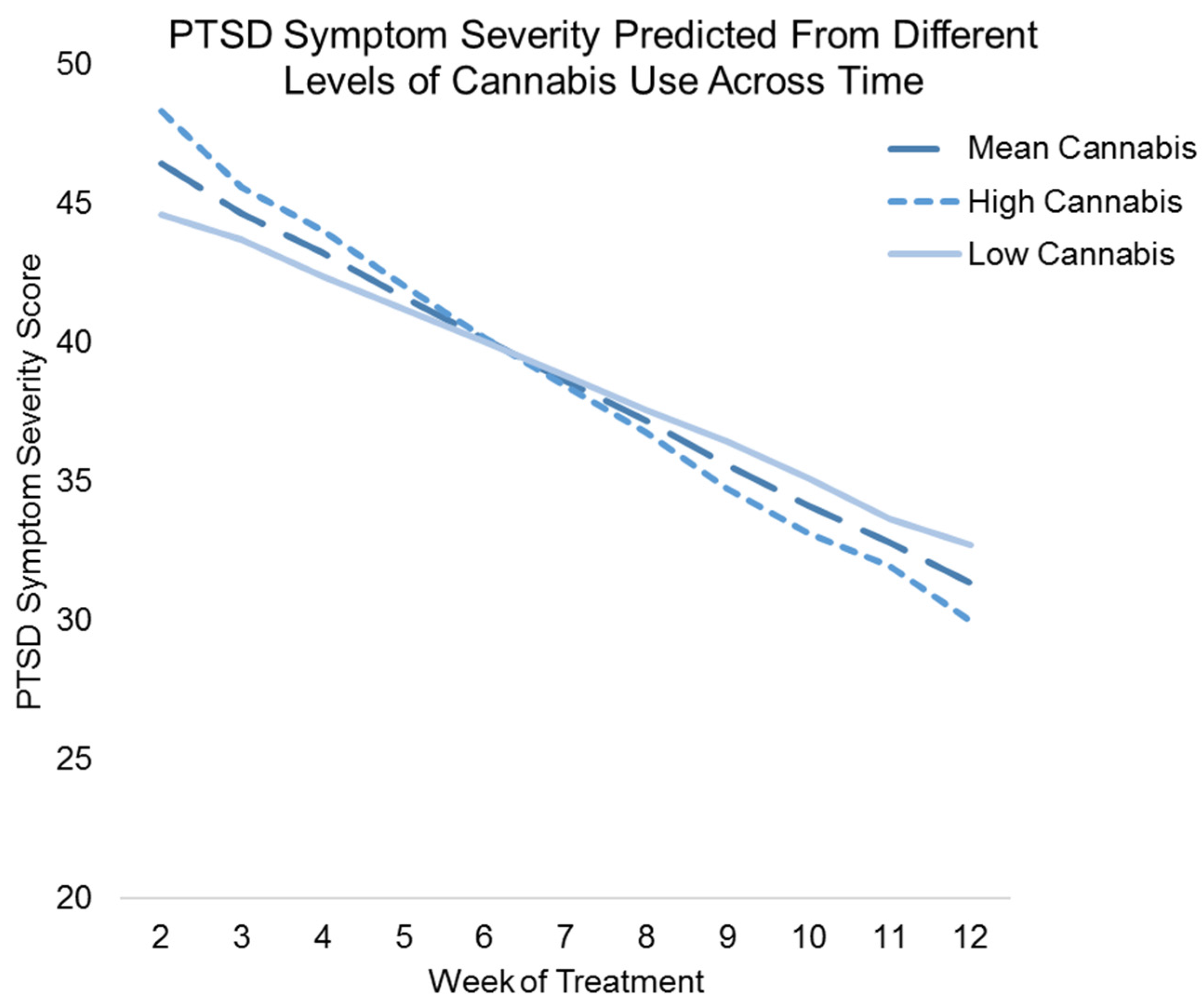
| Time (linear) | −1.60 (−2.06, −1.13) *** | −1.41 (−1.74, −1.07) *** |
| Lagged Cannabis Use X Time (linear) | −0.23 (−0.43, −0.02) * | −0.23 (−0.44, −0.03) * |
| Lagged Primary Substance Use X Time (linear) | 0.01 (−0.15, 0.17) | NS |
© 2017 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license ( http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ruglass, L.M.; Shevorykin, A.; Radoncic, V.; Smith, K.M.Z.; Smith, P.H.; Galatzer-Levy, I.R.; Papini, S.; Hien, D.A. Impact of Cannabis Use on Treatment Outcomes among Adults Receiving Cognitive-Behavioral Treatment for PTSD and Substance Use Disorders. J. Clin. Med. 2017, 6, 14. https://doi.org/10.3390/jcm6020014
Ruglass LM, Shevorykin A, Radoncic V, Smith KMZ, Smith PH, Galatzer-Levy IR, Papini S, Hien DA. Impact of Cannabis Use on Treatment Outcomes among Adults Receiving Cognitive-Behavioral Treatment for PTSD and Substance Use Disorders. Journal of Clinical Medicine. 2017; 6(2):14. https://doi.org/10.3390/jcm6020014
Chicago/Turabian StyleRuglass, Lesia M., Alina Shevorykin, Vanja Radoncic, Kathryn M. Z. Smith, Philip H. Smith, Isaac R. Galatzer-Levy, Santiago Papini, and Denise A. Hien. 2017. "Impact of Cannabis Use on Treatment Outcomes among Adults Receiving Cognitive-Behavioral Treatment for PTSD and Substance Use Disorders" Journal of Clinical Medicine 6, no. 2: 14. https://doi.org/10.3390/jcm6020014