Pattern of Response to Bronchial Challenge with Histamine in Patients with Non-Atopic Cough-Variant and Classic Asthma


Abstract
:1. Introduction
2. Material and Methods
2.1. Study Group
- Age greater than 18 years
- Established diagnosis of CA or CVA in the previous 12 months
- Diagnosis of CA was made according to Global Initiative for Asthma (GINA) criteria [12]
- Diagnosis of CVA was based on: positive challenge testing, clinical improvement while on inhaled corticosteroid (ICS) treatment, and exclusion of other causes of chronic cough. All three criteria were fulfilled in patients with CVA.
- Stable diseases, without exacerbation in the 3 months prior to screening. GINA criteria for CA exacerbation were followed, while for CVA, exacerbation was defined by a board certified senior physician.
- Non-smoker or ex-smokers with smoking history of less than 10 pack/years
- Well-controlled chronicvasomotoric rhinitis
- Non-atopy, defined as negative prick skin testing in previous 6 months, normal values of serum immunoglobulin E (IgE), and normal blood eosinophils count.
- Exacerbation of CA or CVA in the 3 months prior to screening
- Exacerbation of CA or CVA between screening and testing
- Exacerbation of chronic rhinitis before screening or between two visits
- Documented positive skin prick testing and/or eosinophylls (Eo) peripheral blood count greater than 150 cells/mm3, and or sIgE levels greater than 300 I/U
- Verified allergic rhinitis, seasonal or perennial
- Active smokers or ex-smokers with history of more than 10 pack/years
- Unwillingness to further participate in the study
- D1—second to last dose of histamine before fall of FEV1 > 10%
- D2—last dose of histamine after which fall of FEV1 > 10% was recorded
- R1—Percentage of FEV1 fall after D1
- R2—Percentage of FEV1 fall after D2
- D1—second to last dose of histamine before fall of FEV1 > 20%
- D2—last dose of histamine after which fall of FEV1 > 20% was recorded
- R1—Percentage of FEV1 fall after D1
- R2—Percentage of FEV1 fall after D2
2.2. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Glauser, F.L. Variant asthma. Ann. Allergy 1972, 30, 457–459. [Google Scholar] [PubMed]
- Corrao, W.M.; Braman, S.S.; Irwin, R.S. Chronic cough as the sole presenting manifestation of bronchial asthma. N. Engl. J. Med. 1979, 300, 633–637. [Google Scholar] [CrossRef] [PubMed]
- Fujimura, M.; Nishizawa, Y.; Nishitsuji, M.; Abo, M.; Kita, T.; Nomura, S. Longitudinal decline in pulmonary function in atopic cough and cough variant asthma. Clin. Exp. Allergy 2003, 33, 588–594. [Google Scholar] [CrossRef] [PubMed]
- Irwin, R.S.; Ownbey, R.; Cagle, P.T.; Baker, S.; Fraire, A.E. Interpreting the histopathology of chronic cough: A prospective, controlled, comparative study. Chest 2006, 130, 362–370. [Google Scholar] [CrossRef] [PubMed]
- Ohkura, N.; Fujimura, M.; Hara, J.; Ohsawa, M.; Kamei, J.; Nakao, S. Bronchoconstrictiontriggered cough in conscious guinea pigs. Exp. Lung Res. 2009, 35, 296–306. [Google Scholar] [CrossRef] [PubMed]
- Niimi, A.; Amitani, R.; Suzuki, K.; Tanaka, E.; Murayama, T.; Kuze, F. Eosinophilic inflammation in cough variant asthma. Eur. Respir. J. 1998, 11, 1064–1069. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Niimi, A.; Matsumoto, H.; Minakuchi, M.; Kitaichi, M.; Amitani, R. Airway remodelling in cough-variant asthma. Lancet 2000, 356, 564–565. [Google Scholar] [CrossRef]
- Niimi, A.; Torrego, A.; Nicholson, A.G.; Cosio, B.G.; Oates, T.B.; Chung, K.F. Nature of airway inflammation and remodeling in chronic cough. J. Allergy Clin. Immunol. 2005, 116, 565–570. [Google Scholar] [CrossRef] [PubMed]
- Irwin, R.S.; French, C.T.; Smyrnios, N.A.; Curley, F.J. Interpretation of positive results of a methacholine inhalation challenge and 1 week of inhaled bronchodilator use in diagnosing and treating cough-variant asthma. Arch. Intern. Med. 1997, 157, 1981–1987. [Google Scholar] [CrossRef] [PubMed]
- Matsumoto, H.; Niimi, A.; Takemura, M.; Ueda, T.; Yamaguchi, M.; Matsuoka, H.; Jinnai, M.; Chin, K.; Mishima, M. Features of cough variant asthma and classic asthma during methacholine-induced brochoconstriction: A cross-sectional study. Cough 2009, 5, 3. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- De Diego, A.; Martínez, E.; Perpiñá, M.; Nieto, L.; Compte, L.; Macián, V.; Senent, L. Airway inflammation and cough sensitivity in cough-variant asthma. Allergy 2005, 60, 1407–1411. [Google Scholar] [CrossRef] [PubMed]
- Global Initiative for Asthma: Global Strategy for Asthma Management and Prevention. Update 2015. Available online: www.ginasthma.org (accessed on 16 February 2016).
- Miller, M.R.; Hankinson, J.; Brusasco, V.; Burgos, F.; Casaburi, R.; Coates, A.; Crapo, R.; Enright, P.; van der Grinten, C.P.; Gustafsson, P.; et al. ATS/ERS Task Force. Standardization of spirometry. Eur. Respir. J. 2005, 26, 319–338. [Google Scholar] [CrossRef] [PubMed]
- Sterk, P.J.; Bel, E.H. The shape of the dose-responsecurve to inhaled bronchoconstrictor agents in asthma and inchronic obstructive pulmonary disease. Am. Rev. Respir. Dis. 1991, 143, 1433–1437. [Google Scholar] [CrossRef] [PubMed]
- Sterk, P.J.; Fabbri, L.M.; Quanjer, P.H.; Cockcroft, D.W.; O’Byrne, P.M.; Anderson, S.D.; Juniper, E.F.; Malo, J.L. Airway responsiveness. Standardized challenge testing with pharmacological, physical and sensitizing stimuli in adults. Report Working Party Standardization of Lung Function Tests, European Community for Steel and Coal. Official Statement of the European Respiratory Society. Eur. Respir. J. Suppl. 1993, 16, 53–83. [Google Scholar] [PubMed]
- Mochizuki, H.; Arakawa, H.; Tokuyama, K.; Morikawa, A. Bronchialsensitivity and bronchial reactivity in children with cough variant asthma. Chest 2005, 128, 2427–2434. [Google Scholar] [CrossRef] [PubMed]
- Makino, S. Clinical significance of bronchialsensitivity to acetylcholine andhistamine in bronchial asthma. J. Allergy 1966, 38, 127–142. [Google Scholar] [CrossRef]
- Kang, H.; Koh, Y.Y.; Yoo, Y.; Yu, J.; Kim, D.K.; Kim, C.K. Maximal Airway Response to Methacholine in Cough-Variant Asthma. Comparison with Classic Asthma and Its Relationship to Peak Expiratory Flow Variability. Chest 2005, 128, 3881–3887. [Google Scholar] [CrossRef] [PubMed]
- Woolcock, A.J.; Salome, C.M.; Yan, K. The shape of the dose–response curve to histamine in asthmatic and normal subjects. Am. Rev. Respir. Dis. 1984, 130, 71–75. [Google Scholar] [PubMed]
- Koh, Y.Y.; Park, Y.; Kim, C.K. The importance of maximal airway response to methacholine in the prediction of wheezing development in patients with cough-variant asthma. Allergy 2002, 57, 1165–1170. [Google Scholar] [CrossRef] [PubMed]
- Fujimura, M.; Sakamoto, S.; Kamio, Y.; Matsuda, T. Cough receptor sensitivity and bronchial responsiveness in normal and asthmatic subjects. Eur. Respir. 1992, 5, 291–295. [Google Scholar]
- Tajiri, T.; Niimi, A.; Matsumoto, H.; Ito, I.; Oguma, T.; Otsuka, K.; Takeda, T.; Nakaji, H.; Inoue, H.; Iwata, T.; et al. Prevalence and Clinical Relevance of Allergic Rhinitis in Patients with Classic Asthma and Cough Variant Asthma. Respiration 2014, 87, 211–218. [Google Scholar] [CrossRef] [PubMed]
- Salome, C.M.; Schoeffel, R.E.; Woolcock, A.J. Comparison of bronchial reactivity to histamine and methacholine in asthmatics. Clin. Allergy 1980, 10, 541–546. [Google Scholar] [CrossRef] [PubMed]
- Matsuoka, H.; Niimi, A.; Matsumoto, H.; Takemura, M.; Ueda, T.; Yamaguchi, M.; Jinnai, M.; Inoue, H.; Ito, I.; Chin, K.; et al. Inflammatory subtypes in cough-variant asthma. Association with maintenance doses of inhaled corticosteroids. Chest 2010, 138, 1418–1425. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Parameter | Cough-Variant Asthma (n = 49) | “Classic” Asthma (n = 108) | p |
|---|---|---|---|
| Age (years, MV ± SD) | 40.84 ± 11.39 | 37.52 ± 11.24 | >0.05 a |
| Age of asthma diagnosis (years, MV ± SD) | 30.53 ± 10.34 | 28.17 ± 9.51 | >0.05 a |
| Males (n, percent) | 11, 22.4% | 37, 34.3% | <0.01 b |
| Females (n, percent) | 38, 77.6% | 71, 65.7% | <0.01 b |
| Family history of asthma (n, percent) | 10, 20.4% | 29, 26.9% | <0.01 b |
| Chronic vasomotoric rhinitis (n, percent) | 18, 36.7% | 61, 56.5% | <0.01 b |
| Eo (cells/mm3, MV ± SD) | 116.69 ± 27.25 | 103.10 ± 27.68 | <0.05 a |
| sIgE (IU, MV ± SD) | 112.18 ± 35.43 | 111.99 ± 36.15 | >0.05 a |
| BMI (kg/m2, MV ± SD) | 26.11 ± 4.69 | 24.73 ± 4.09 | >0.05 a |
| Daily ICS dose (mcg budesonide equivalent, MV ± SD) | 289.79 ± 100.5 | 283.33 ± 99.06 | >0.05 a |
| FVC (% of predicted, MV ± SD) | 101.04 ± 6.33 | 102.04 ± 6.34 | >0.05 a |
| FEV1 (% o fpredicted, MV ± SD) | 94.57 ± 5.81 | 95.97 ± 5.93 | >0.05 a |
| Parameter | Cough-Variant Asthma (N = 49) | “Classic” Asthma (N = 108) | p |
|---|---|---|---|
| Positive challenge (n, percent) | 22, 44.9% | 69, 63.9% | <0.05 a |
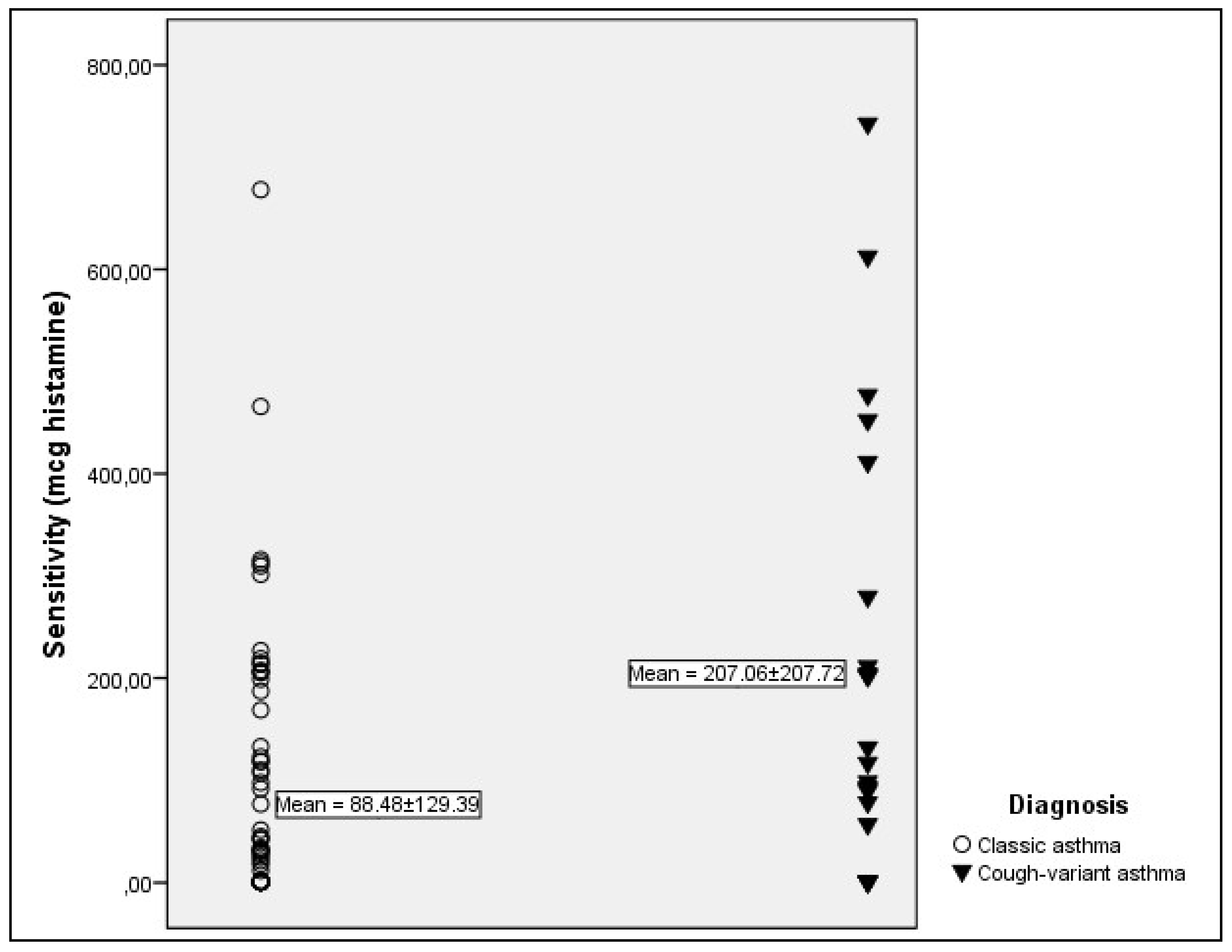
| PD10 (mcg, MV ± SD) | 207.06 ± 207.72 | 88.48 ± 129.39 | <0.05 b |
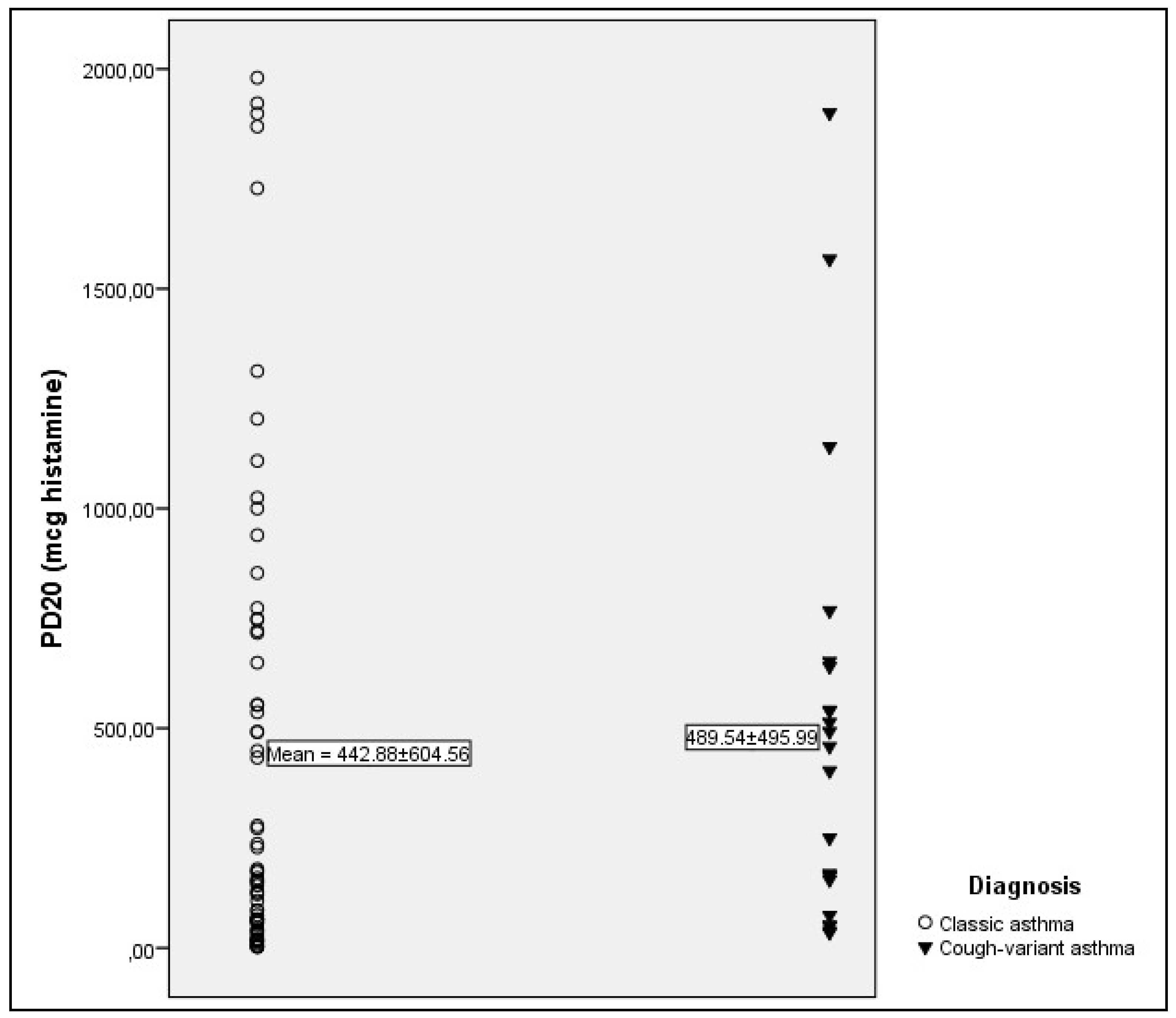
| PD20 (mcg, MV ± SD) | 489.54 ± 495.99 | 442.88 ± 604.56 | >0.05 b |
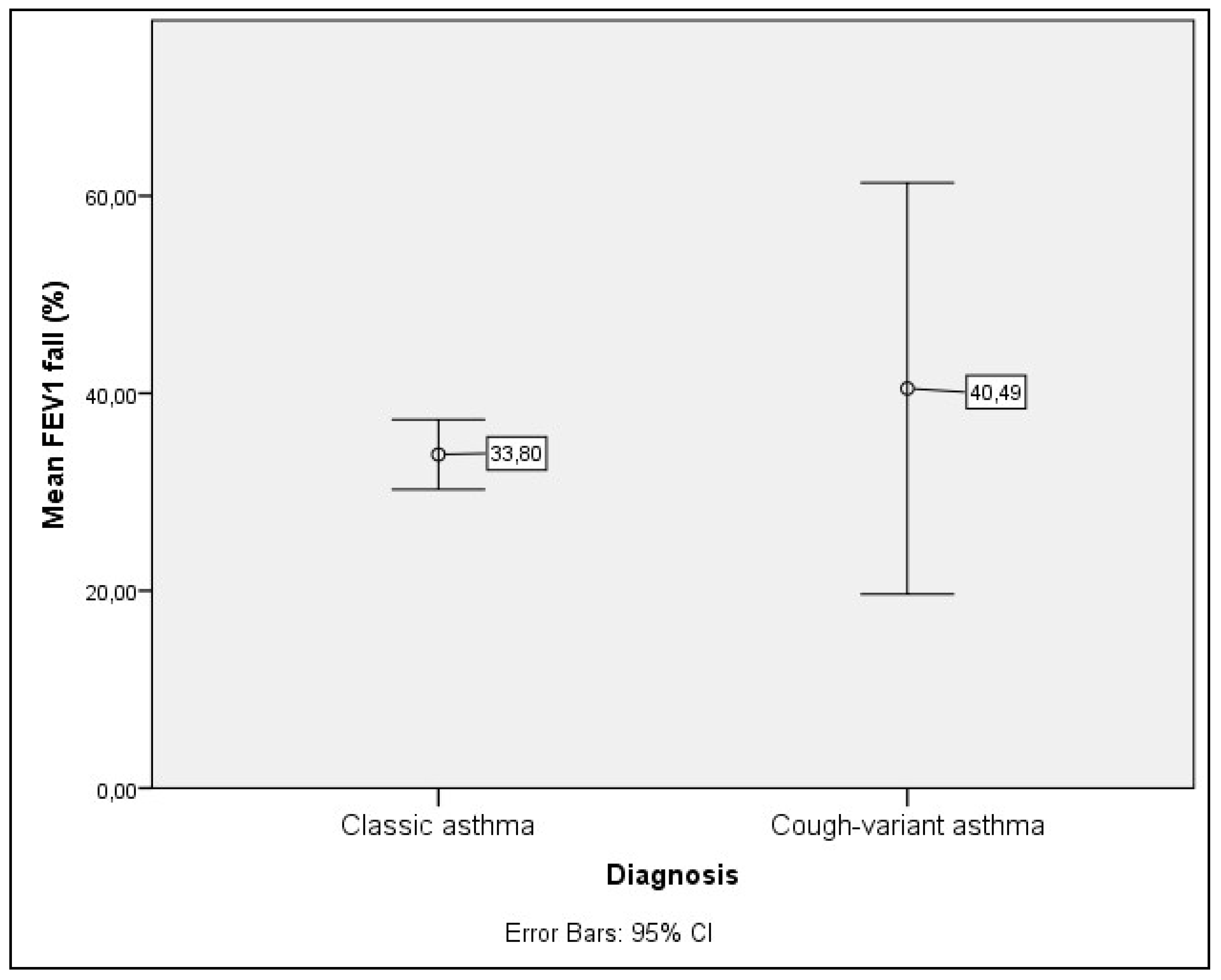
| FEV1 fall (percent, MV ± SD) | 40.48 ± 46.98 | 33.80 ± 14.75 | >0.05 b |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zugic, V.; Mujovic, N.; Hromis, S.; Jankovic, J.; Drvenica, M.; Perovic, A.; Kopitovic, I.; Ilic, A.; Nikolic, D. Pattern of Response to Bronchial Challenge with Histamine in Patients with Non-Atopic Cough-Variant and Classic Asthma. J. Clin. Med. 2018, 7, 174. https://doi.org/10.3390/jcm7070174
Zugic V, Mujovic N, Hromis S, Jankovic J, Drvenica M, Perovic A, Kopitovic I, Ilic A, Nikolic D. Pattern of Response to Bronchial Challenge with Histamine in Patients with Non-Atopic Cough-Variant and Classic Asthma. Journal of Clinical Medicine. 2018; 7(7):174. https://doi.org/10.3390/jcm7070174
Chicago/Turabian StyleZugic, Vladimir, Natasa Mujovic, Sanja Hromis, Jelena Jankovic, Mirjana Drvenica, Aleksandra Perovic, Ivan Kopitovic, Aleksandra Ilic, and Dejan Nikolic. 2018. "Pattern of Response to Bronchial Challenge with Histamine in Patients with Non-Atopic Cough-Variant and Classic Asthma" Journal of Clinical Medicine 7, no. 7: 174. https://doi.org/10.3390/jcm7070174