Preadmission Statin Therapy Is Associated with a Lower Incidence of Acute Kidney Injury in Critically Ill Patients: A Retrospective Observational Study

Abstract
:1. Introduction
2. Materials and Method
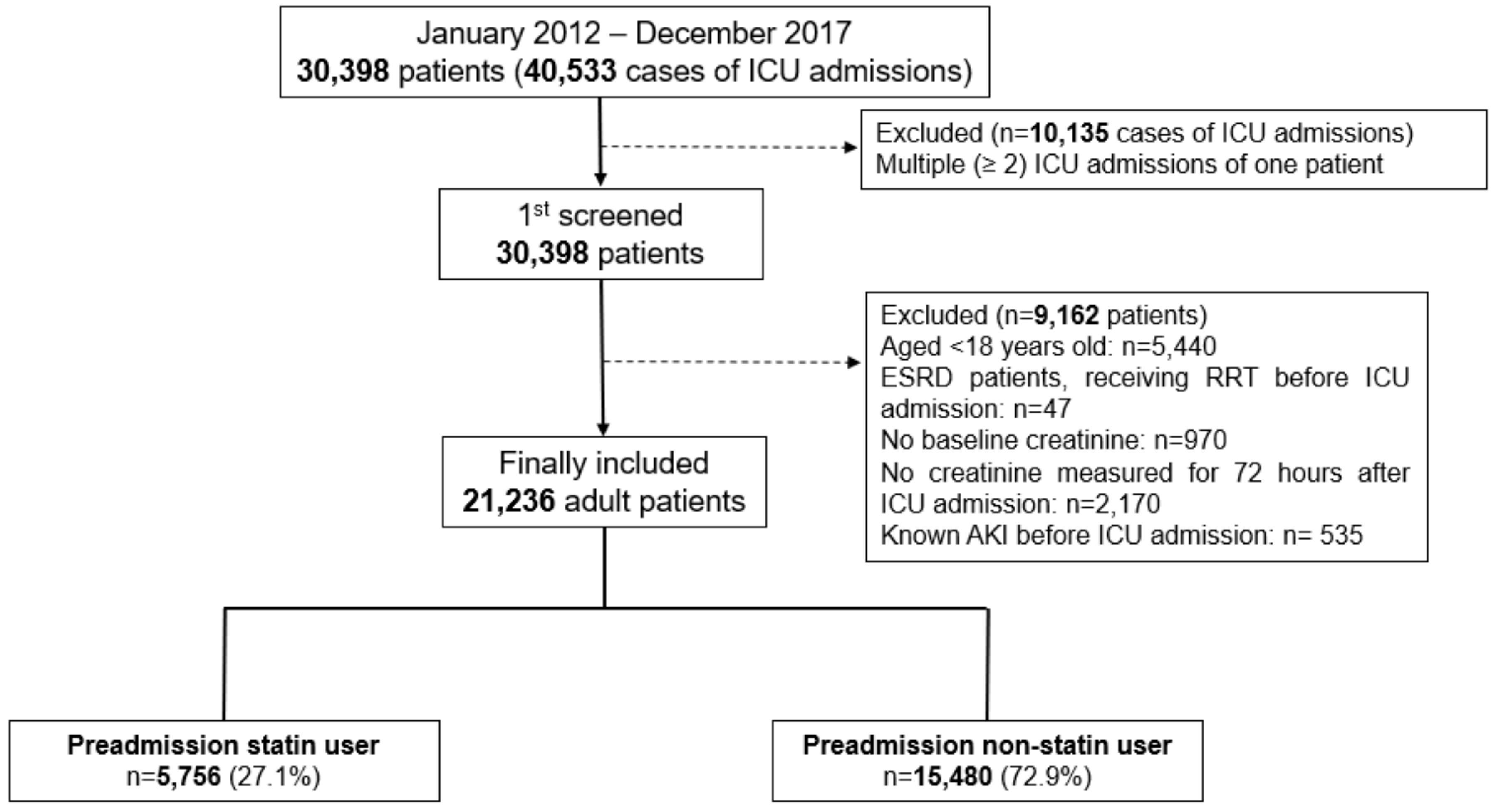
2.1. Patients
2.2. Preadmission Statin Use (Main Independent Variables)
2.3. Measurements (Covariates)
2.4. Diagnosis of AKI (Dependent Variable)
2.5. Outcomes
2.6. Statistical Analysis
3. Results
3.1. Preadmission Statin Use and AKI Incidence
3.2. Preadmission Statin Use and Stage ≥2 AKI Incidence
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
Appendix A. Staging of Postoperative Acute Kidney Injury (KDIGO)

{kind=link}
| Stage | Serum Creatinine |
|---|---|
| 1 | 1.5–1.9 times baseline or ≥0.3 mg dL−1 increase within 72 h after ICU admission |
| 2 | 2.0–2.9 times baseline within 72 h after ICU admission |
| 3 | 3.0 times baseline or increase in serum creatinine to ≥4.0 mg dL−1 or initiation of RRT within 72 h after ICU admission |
Appendix B. Univariable Logistic Regression Analysis of Covariates for Occurrence of Total Acute Kidney Injury during 72 h after ICU Admission
| Variables | Odds Ratio (95% CI) | p-Value | ||
|---|---|---|---|---|
| Sex: male | 1.06 (1.00–1.13) | 0.066 | ||
| Age, year | 1.02 (1.02–1.02) | <0.001 | ||
| Body mass index, kg m−2 | 0.96 (0.95–0.97) | <0.001 | ||
| APACHE II | 1.04 (1.04–1.04) | <0.001 | ||
| Comorbidities at ICU admission | ||||
| Hypertension | 1.26 (1.18–1.34) | <0.001 | ||
| Diabetes mellitus | 1.46 (1.32–1.61) | <0.001 | ||
| Ischemic heart disease | 1.17 (0.97–1.42) | 0.101 | ||
| Cerebrovascular disease | 1.31 (1.14–1.51) | <0.001 | ||
| Chronic obstructive lung disease | 1.13 (0.97–1.31) | 0.109 | ||
| Liver disease (LC, hepatitis, fatty liver) | 2.48 (2.13–2.89) | <0.001 | ||
| Anemia (Hb < 10 g dL−1) | 3.82 (3.58–4.07) | <0.001 | ||
| Cancer | 1.90 (1.77–2.05) | <0.001 | ||
| eGFR mL min−1 1.73 m−2 | ||||
| ≥90 | 1 | <0.001 | ||
| 60–90 | 0.99 (0.91–1.07) | 0.731 | ||
| 30–60 | 2.08 (1.89–2.28) | <0.001 | ||
| <30 | 5.18 (4.61–5.82) | <0.001 | ||
| Admission through emergency department | 1.52 (1.43–1.62) | <0.001 | ||
| Total serum cholesterol at ICU adm | ||||
| 160–200 mg dL−1 | 1 | <0.001 | ||
| <160, mg dL−1 | 2.21 (2.01, 2.43) | <0.001 | ||
| >200 mg dL−1 | 0.81 (0.69, 0.94) | <0.001 | ||
| Admission department | ||||
| Internal medicine | 1 | <0.001 | ||
| Neurologic center | 0.25 (0.23–0.28) | <0.001 | ||
| Cardiothoracic surgical department | 0.78 (0.72–0.84) | <0.001 | ||
| Other surgical department | 0.83 (0.76–0.90) | <0.001 | ||
| Year at ICU admission | ||||
| 2012 | 1 | <0.001 | ||
| 2013 | 1.31 (1.16–1.48) | <0.001 | ||
| 2014 | 1.26 (1.12–1.42) | <0.001 | ||
| 2015 | 1.09 (0.97–1.23) | 0.150 | ||
| 2016 | 1.02 (0.91–1.15) | 0.690 | ||
| 2017 | 0.96 (0.86–1.08) | 0.535 | ||
Appendix C. Univariable Logistic Regression Analysis of Covariates for Occurrence of Stage ≥ 2 AKI Acute Kidney Injury during 72 h after ICU Admission
| Variables | Odds Ratio (95% CI) | p-Value | ||
|---|---|---|---|---|
| Sex: male | 1.04 (0.95–1.13) | 0.452 | ||
| Age, year | 1.01 (1.01–1.02) | <0.001 | ||
| Body mass index, kg m−2 | 0.94 (0.92–0.95) | <0.001 | ||
| APACHE II | 1.04 (1.04–1.04) | <0.001 | ||
| Comorbidities at ICU admission | ||||
| Hypertension | 1.08 (0.99–1.18) | 0.106 | ||
| Diabetes mellitus | 1.25 (1.09–1.44) | 0.002 | ||
| Ischemic heart disease | 0.94 (0.70–1.25) | 0.654 | ||
| Cerebrovascular disease | 1.03 (0.83–1.27) | 0.795 | ||
| Chronic obstructive lung disease | 0.97 (0.78–1.21) | 0.816 | ||
| Liver disease (LC, hepatitis, fatty liver) | 3.26 (2.73–3.88) | <0.001 | ||
| Anemia (Hb < 10 g dL−1) | 4.86 (4.42–5.35) | <0.001 | ||
| Cancer | 2.23 (2.03–2.46) | <0.001 | ||
| eGFR mL min−1 1.73 m−2 | ||||
| ≥90 | 1 | <0.001 | ||
| 60–90 | 0.73 (0.64–0.82) | <0.001 | ||
| 30–60 | 1.10 (0.96–1.27) | 0.171 | ||
| <30 | 2.84 (2.47–3.26) | <0.001 | ||
| Admission through emergency department | 2.00 (1.82–2.21) | <0.001 | ||
| Total serum cholesterol at ICU adm | ||||
| 160–200 mg dL−1 | 1 | |||
| <160, mg dL−1 | 2.34 (2.02, 2.70) | <0.001 | ||
| >200 mg dL−1 | 0.81 (0.64, 1.04) | 0.095 | ||
| Admission department | ||||
| Internal medicine | 1 | <0.001 | ||
| Neurologic center | 0.20 (0.17–0.24) | <0.001 | ||
| Cardiothoracic surgical department | 0.52 (0.46–0.58) | <0.001 | ||
| Other surgical department | 0.67 (0.60–0.75) | <0.001 | ||
| Year at ICU admission | ||||
| 2012 | 1 | <0.001 | ||
| 2013 | 1.52 (1.27–1.80) | <0.001 | ||
| 2014 | 1.38 (1.16–1.63) | <0.001 | ||
| 2015 | 1.19 (1.00–1.41) | 0.053 | ||
| 2016 | 1.05 (0.88–1.24) | 0.605 | ||
| 2017 | 1.00 (0.84–1.19) | 0.999 | ||
References
- Waikar, S.S.; Bonventre, J.V. Creatinine kinetics and the definition of acute kidney injury. J. Am. Soc. Nephrol. 2009, 20, 672–679. [Google Scholar] [CrossRef] [PubMed]
- Bellomo, R.; Kellum, J.A.; Ronco, C. Acute kidney injury. Lancet 2012, 380, 756–766. [Google Scholar] [CrossRef]
- Lewington, A.J.; Cerda, J.; Mehta, R.L. Raising awareness of acute kidney injury: A global perspective of a silent killer. Kidney Int. 2013, 84, 457–467. [Google Scholar] [CrossRef] [PubMed]
- Nash, K.; Hafeez, A.; Hou, S. Hospital-acquired renal insufficiency. Am. J. Kidney Dis. 2002, 39, 930–936. [Google Scholar] [CrossRef] [PubMed]
- Thakar, C.V.; Christianson, A.; Freyberg, R.; Almenoff, P.; Render, M.L. Incidence and outcomes of acute kidney injury in intensive care units: A veterans administration study. Crit. Care Med. 2009, 37, 2552–2558. [Google Scholar] [CrossRef]
- Macedo, E.; Mehta, R.L. Preventing acute kidney injury. Crit. Care Clin. 2015, 31, 773–784. [Google Scholar] [CrossRef] [PubMed]
- Santodomingo-Garzon, T.; Cunha, T.M.; Verri, W.A., Jr.; Valerio, D.A.; Parada, C.A.; Poole, S.; Ferreira, S.H.; Cunha, F.Q. Atorvastatin inhibits inflammatory hypernociception. Br. J. Pharmacol. 2006, 149, 14–22. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rosenson, R.S. Low high-density lipoprotein cholesterol and cardiovascular disease: Risk reduction with statin therapy. Am. Heart J. 2006, 151, 556–563. [Google Scholar] [CrossRef]
- Novack, V.; Terblanche, M.; Almog, Y. Do statins have a role in preventing or treating sepsis? Crit. Care 2006, 10, 113. [Google Scholar] [CrossRef]
- Terblanche, M.; Almog, Y.; Rosenson, R.S.; Smith, T.S.; Hackam, D.G. Statins and sepsis: Multiple modifications at multiple levels. Lancet Infect Dis. 2007, 7, 358–368. [Google Scholar] [CrossRef]
- Wang, C.Y.; Liu, P.Y.; Liao, J.K. Pleiotropic effects of statin therapy: Molecular mechanisms and clinical results. Trends Mol. Med. 2008, 14, 37–44. [Google Scholar] [CrossRef] [PubMed]
- Molnar, A.O.; Coca, S.G.; Devereaux, P.J.; Jain, A.K.; Kitchlu, A.; Luo, J.; Parikh, C.R.; Paterson, J.M.; Siddiqui, N.; Wald, R.; et al. Statin use associates with a lower incidence of acute kidney injury after major elective surgery. J. Am. Soc. Nephrol. 2011, 22, 939–946. [Google Scholar] [CrossRef] [PubMed]
- Campbell, J. Hmg coa reductase inhibitors (statins) for preventing acute kidney injury after surgical procedures requiring cardiac bypass. J. Perioper. Pract. 2018, 28, 142–143. [Google Scholar] [CrossRef] [PubMed]
- Han, Y.; Zhu, G.; Han, L.; Hou, F.; Huang, W.; Liu, H.; Gan, J.; Jiang, T.; Li, X.; Wang, W.; et al. Short-term rosuvastatin therapy for prevention of contrast-induced acute kidney injury in patients with diabetes and chronic kidney disease. J. Am. Coll. Cardiol. 2014, 63, 62–70. [Google Scholar] [CrossRef] [PubMed]
- Yasuda, H.; Yuen, P.S.; Hu, X.; Zhou, H.; Star, R.A. Simvastatin improves sepsis-induced mortality and acute kidney injury via renal vascular effects. Kidney Int. 2006, 69, 1535–1542. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Su, X.; Zhang, L.; Lv, J.; Wang, J.; Hou, W.; Xie, X.; Zhang, H. Effect of statins on kidney disease outcomes: A systematic review and meta-analysis. Am. J. Kidney Dis. 2016, 67, 881–892. [Google Scholar] [CrossRef] [PubMed]
- Hallan, S.; Asberg, A.; Lindberg, M.; Johnsen, H. Validation of the modification of diet in renal disease formula for estimating gfr with special emphasis on calibration of the serum creatinine assay. Am. J. Kidney Dis. 2004, 44, 84–93. [Google Scholar] [CrossRef] [PubMed]
- Neaton, J.D.; Blackburn, H.; Jacobs, D.; Kuller, L.; Lee, D.J.; Sherwin, R.; Shih, J.; Stamler, J.; Wentworth, D. Serum cholesterol level and mortality findings for men screened in the multiple risk factor intervention trial. Multiple risk factor intervention trial research group. Arch. Intern. Med. 1992, 152, 1490–1500. [Google Scholar] [CrossRef] [PubMed]
- Sempos, C.T.; Cleeman, J.I.; Carroll, M.D.; Johnson, C.L.; Bachorik, P.S.; Gordon, D.J.; Burt, V.L.; Briefel, R.R.; Brown, C.D.; Lippel, K.; et al. Prevalence of high blood cholesterol among us adults. An update based on guidelines from the second report of the national cholesterol education program adult treatment panel. JAMA 1993, 269, 3009–3014. [Google Scholar] [CrossRef] [PubMed]
- Kellum, J.A.; Lameire, N.; Group, K.A.G.W. Diagnosis, evaluation, and management of acute kidney injury: A kdigo summary (part 1). Crit. Care 2013, 17, 204. [Google Scholar] [CrossRef] [PubMed]
- Chawla, L.S.; Eggers, P.W.; Star, R.A.; Kimmel, P.L. Acute kidney injury and chronic kidney disease as interconnected syndromes. N. Engl. J. Med. 2014, 371, 58–66. [Google Scholar] [CrossRef]
- Armstrong, R.A. When to use the bonferroni correction. Ophthalmic Physiol. Opt. 2014, 34, 502–508. [Google Scholar] [CrossRef]
- Sanguankeo, A.; Upala, S.; Cheungpasitporn, W.; Ungprasert, P.; Knight, E.L. Effects of statins on renal outcome in chronic kidney disease patients: A systematic review and meta-analysis. PLoS ONE 2015, 10, e0132970. [Google Scholar] [CrossRef]
- Messow, C.M.; Isles, C. Meta-analysis of statins in chronic kidney disease: Who benefits? QJM 2017, 110, 493–500. [Google Scholar] [CrossRef] [PubMed]
- Basile, D.P.; Anderson, M.D.; Sutton, T.A. Pathophysiology of acute kidney injury. Compr. Physiol. 2012, 2, 1303–1353. [Google Scholar] [PubMed]
- Liao, J.K.; Laufs, U. Pleiotropic effects of statins. Annu. Rev. Pharmacol. Toxicol. 2005, 45, 89–118. [Google Scholar] [CrossRef] [PubMed]
- Fuller, B.M.; Gajera, M.; Schorr, C.; Gerber, D.; Dellinger, R.P.; Zanotti, S. The association of prior statin use in septic shock treated with early goal directed therapy. Eur. J. Emerg. Med. 2012, 19, 226–230. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Thomsen, R.W.; Riis, A.; Kornum, J.B.; Christensen, S.; Johnsen, S.P.; Sorensen, H.T. Preadmission use of statins and outcomes after hospitalization with pneumonia: Population-based cohort study of 29,900 patients. Arch. Intern. Med. 2008, 168, 2081–2087. [Google Scholar] [CrossRef]
- Craig, T.; O’Kane, C.; McAuley, D. Potential mechanisms by which statins modulate the development of acute lung injury. In Intensive Care Medicine; Springer: Berlin, Germany, 2007; pp. 276–288. [Google Scholar]
- Nagendran, M.; McAuley, D.F.; Kruger, P.S.; Papazian, L.; Truwit, J.D.; Laffey, J.G.; Thompson, B.T.; Clarke, M.; Gordon, A.C. Statin therapy for acute respiratory distress syndrome: An individual patient data meta-analysis of randomised clinical trials. Intensive Care Med. 2017, 43, 663–671. [Google Scholar] [CrossRef]
- Thomas, G.; Hraiech, S.; Loundou, A.; Truwit, J.; Kruger, P.; McAuley, D.F.; Papazian, L.; Roch, A. Statin therapy in critically-ill patients with severe sepsis: A review and meta-analysis of randomized clinical trials. Minerva Anestesiol. 2015, 81, 921–930. [Google Scholar]
- Sastre, C.; Rubio-Navarro, A.; Buendia, I.; Gomez-Guerrero, C.; Blanco, J.; Mas, S.; Egido, J.; Blanco-Colio, L.M.; Ortiz, A.; Moreno, J.A. Hyperlipidemia-associated renal damage decreases klotho expression in kidneys from apoe knockout mice. PLoS ONE 2013, 8, e83713. [Google Scholar] [CrossRef] [PubMed]
- Wilson, R.F.; Barletta, J.F.; Tyburski, J.G. Hypocholesterolemia in sepsis and critically ill or injured patients. Crit. Care 2003, 7, 413–414. [Google Scholar] [CrossRef] [PubMed]
- Gui, D.; Spada, P.L.; De Gaetano, A.; Pacelli, F. Hypocholesterolemia and risk of death in the critically ill surgical patient. Intensive Care Med. 1996, 22, 790–794. [Google Scholar] [CrossRef] [PubMed]

| Variable | Total (21,236) | Mean | SD | |
|---|---|---|---|---|
| Sex: male | 12,434 (58.6%) | |||
| Age, year | 64.0 | 15.8 | ||
| Body mass index, kg m−2 | 23.7 | 3.9 | ||
| APACHE II | 20.0 | 10.0 | ||
| Comorbidities at ICU admission | ||||
| eGFR a ≥ 90 | 12,993 (61.2%) | |||
| 60 ≤ eGFR a < 90 | 4527 (21.3%) | |||
| 30 ≤ eGFR a < 60 | 2364 (11.1%) | |||
| eGFR a < 30 | 1352 (6.4%) | |||
| Hypertension | 9346 (44.0%) | |||
| Diabetes mellitus | 1969 (9.3%) | |||
| Ischemic heart disease | 538 (2.5%) | |||
| Cerebrovascular disease | 945 (4.4%) | |||
| Chronic obstructive lung disease | 921 (4.3%) | |||
| Liver disease (LC, hepatitis, fatty liver) | 683 (3.2%) | |||
| Anemia (Hb < 10 g dL−1) | 7569 (35.6%) | |||
| Cancer | 4308 (20.3%) | |||
| Characteristics of ICU admission | ||||
| Admission through emergency department | 12,042 (56.7%) | |||
| Admission department | ||||
| Internal medicine | 4671 (22.0%) | |||
| Neurologic center | 4975 (23.4%) | |||
| Cardiothoracic surgical department | 6875 (32.4%) | |||
| Other surgical department | 4715 (22.2%) | |||
| Length of ICU stay, day | 3.1 | 10.0 | ||
| Length of hospital stay, day | 12.9 | 20.1 | ||
| Preadmission statin use | 5756 (27.1%) | |||
| Total serum cholesterol at ICU adm, mg dL−1 | 138.2 | 47.9 | ||
| <160, mg dL−1 | 8584 (40.4%) | |||
| 160–200 mg dL−1 | 10,751 (50.6%) | |||
| >200 mg dL−1 | 1901 (9.0%) | |||
| Type of statin | ||||
| Atorvastatin | 3456 (16.3%) | |||
| Rosuvastatin | 1391 (6.6%) | |||
| Simvastatin | 396 (1.9%) | |||
| Pitavastatin | 346 (1.6%) | |||
| Other statin b | 167 (0.8%) | |||
| Total acute kidney injury | 5469 (25.8%) | |||
| Acute kidney injury stage ≥2 | 2216 (10.4%) | |||
| RRT after ICU adm within 72 h | 488 (2.3%) | |||
| Variables | Statin Group n = 5756 | Non-Statin Group n = 15,480 | p-Value | |
|---|---|---|---|---|
| Sex: male | 3398 (59.0%) | 9036 (58.4%) | 0.384 | |
| Age, year | 68.6 (12.0) | 62.2 (16.6) | <0.001 | |
| Body Mass Index, kg m−2 | 24.6 (3.8) | 23.3 (3.8) | <0.001 | |
| Comorbidities at ICU admission | ||||
| APACHE II | 19.8 (9.8) | 20.2 (10.1) | 0.012 | |
| eGFR a | <0.001 | |||
| ≥90 | 3073 (53.4%) | 9920 (64.1%) | ||
| 60–90 | 1488 (25.9%) | 3039 (19.6%) | ||
| 30–60 | 764 (13.3%) | 1.600 (10.3%) | ||
| <30 | 431 (7.5%) | 921 (5.9%) | ||
| Hypertension | 3672 (63.8%) | 5674 (36.7%) | <0.001 | |
| Diabetes mellitus | 830 (14.4%) | 1139 (7.4%) | <0.001 | |
| Ischemic heart disease | 314 (5.5%) | 224 (1.4%) | <0.001 | |
| Cerebrovascular disease | 505 (8.8%) | 440 (2.8%) | <0.001 | |
| Chronic obstructive lung disease | 229 (4.0%) | 692 (4.5%) | 0118 | |
| Liver disease (LC, hepatitis, fatty liver) | 87 (1.5%) | 596 (3.9%) | <0.001 | |
| Anemia (Hb < 10 g dL−1) | 1774 (30.8%) | 5795 (37.4%) | <0.001 | |
| Cancer | 875 (15.22%) | 3433 (22.2%) | <0.001 | |
| Admission through ED | 2640 (45.9%) | 9402 (60.7%) | <0.001 | |
| Admission department | <0.001 | |||
| Internal medicine | 1317 (22.9%) | 3354 (21.7%) | ||
| Neurologic center | 1252 (21.8%) | 3723 (24.1%) | ||
| Cardiothoracic surgical department | 2166 (37.6%) | 4709 (30.4%) | ||
| Other surgical department | 1021 (17.7%) | 3694 (23.9%) | ||
| Total serum cholesterol at ICU adm, mg dL−1 | 125.2 (37.6) | 143.1 (50.4) | <0.001 | |
| Length of hospital stay, day | 11.3 (22.5) | 13.5 (19.0) | <0.001 | |
| Length of ICU stay, day | 2.5 (15.3) | 3.3 (7.2) | <0.001 | |
| Total acute kidney injury | 1301 (22.6%) | 4168 (26.9%) | <0.001 | |
| Acute kidney injury stage ≥2 | 439 (7.6%) | 1777 (11.5%) | <0.001 | |
| RRT after ICU adm within 72 h | 140 (2.4%) | 348 (2.2%) | 0.426 | |
| Variable | Multivariable Model | |
|---|---|---|
| Odds Ratio (95% CI) | p-Value | |
| Dependent Variable: Total AKI | ||
| Model 1: Preadmission statin use | 0.69 (0.61, 0.79) | <0.001 |
| Total serum cholesterol at ICU adm | ||
| 160–200 mg dL−1 | 1 | <0.001 |
| <160, mg dL−1 | 1.63 (1.45, 1.83) | <0.001 |
| >200 mg dL−1 | 0.86 (0.72, 1.04) | 0.111 |
| Interaction: eGFR a ≥ 90 × Non-statin use | 1 | 0.001 |
| 60 ≤ eGFR a < 90 × Statin use | 1.19 (0.95, 1.49) | 0.132 |
| 30 ≤ eGFR a < 60 × Statin use | 0.97 (0.74, 1.26) | 0.801 |
| eGFR a < 30 × Statin use | 1.89 (1.35, 2.65) | <0.001 |
| Dependent Variable: Stage ≥2 AKI | ||
| Model 3: Preadmission statin use | 0.69 (0.57, 0.84) | <0.001 |
| Total serum cholesterol at ICU adm | ||
| 160–200 mg dL−1 | 1 | <0.001 |
| <160 mg dL−1 | 1.66 (1.38, 1.99) | <0.001 |
| >200 mg dL−1 | 0.85 (0.63, 1.15) | 0.295 |
| Interaction: eGFR a ≥ 90 × Non-statin use | 1 | |
| 60 ≤ eGFR a < 90 × Statin use | 0.95 (0.64, 1.40) | 0.788 |
| 30 ≤ eGFR a < 90 × Statin use | 1.04 (0.67, 1.61) | 0.856 |
| eGFR a < 30 × Statin use | 1.27 (0.85, 1.91) | 0.242 |
| Variable | Multivariable Model | ||
|---|---|---|---|
| Odds Ratio (95% CI) | p-Value * | ||
| eGFR a ≥ 90 (n = 12,993) | |||
| Preadmission statin use | 0.72 (0.63, 0.82) | <0.001 | |
| 60 ≤ eGFR a < 90 (n = 4527) | |||
| Preadmission statin use | 0.74 (0.61, 0.91) | 0.004 | |
| 30 ≤ eGFR a < 60 (n = 2364) | |||
| Preadmission statin use | 0.65 (0.51, 0.83) | 0.001 | |
| eGFR a < 30 (n = 1340) | |||
| Preadmission statin use | 1.33 (0.95, 1.86) | 0.095 | |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Oh, T.K.; Song, I.-A.; Cho, Y.-J.; Lim, C.; Jeon, Y.-T.; Bae, H.-J.; Jo, Y.H. Preadmission Statin Therapy Is Associated with a Lower Incidence of Acute Kidney Injury in Critically Ill Patients: A Retrospective Observational Study. J. Clin. Med. 2019, 8, 25. https://doi.org/10.3390/jcm8010025
Oh TK, Song I-A, Cho Y-J, Lim C, Jeon Y-T, Bae H-J, Jo YH. Preadmission Statin Therapy Is Associated with a Lower Incidence of Acute Kidney Injury in Critically Ill Patients: A Retrospective Observational Study. Journal of Clinical Medicine. 2019; 8(1):25. https://doi.org/10.3390/jcm8010025
Chicago/Turabian StyleOh, Tak Kyu, In-Ae Song, Young-Jae Cho, Cheong Lim, Young-Tae Jeon, Hee-Joon Bae, and You Hwan Jo. 2019. "Preadmission Statin Therapy Is Associated with a Lower Incidence of Acute Kidney Injury in Critically Ill Patients: A Retrospective Observational Study" Journal of Clinical Medicine 8, no. 1: 25. https://doi.org/10.3390/jcm8010025