Acute Kidney Injury in Patients Undergoing Total Hip Arthroplasty: A Systematic Review and Meta-Analysis


 , , , , and
, , , , and 
Abstract
:1. Introduction
2. Methods
2.1. Search Strategy and Literature Review
2.2. Selection Criteria
2.3. Data Abstraction
2.4. Statistical Analysis
3. Results
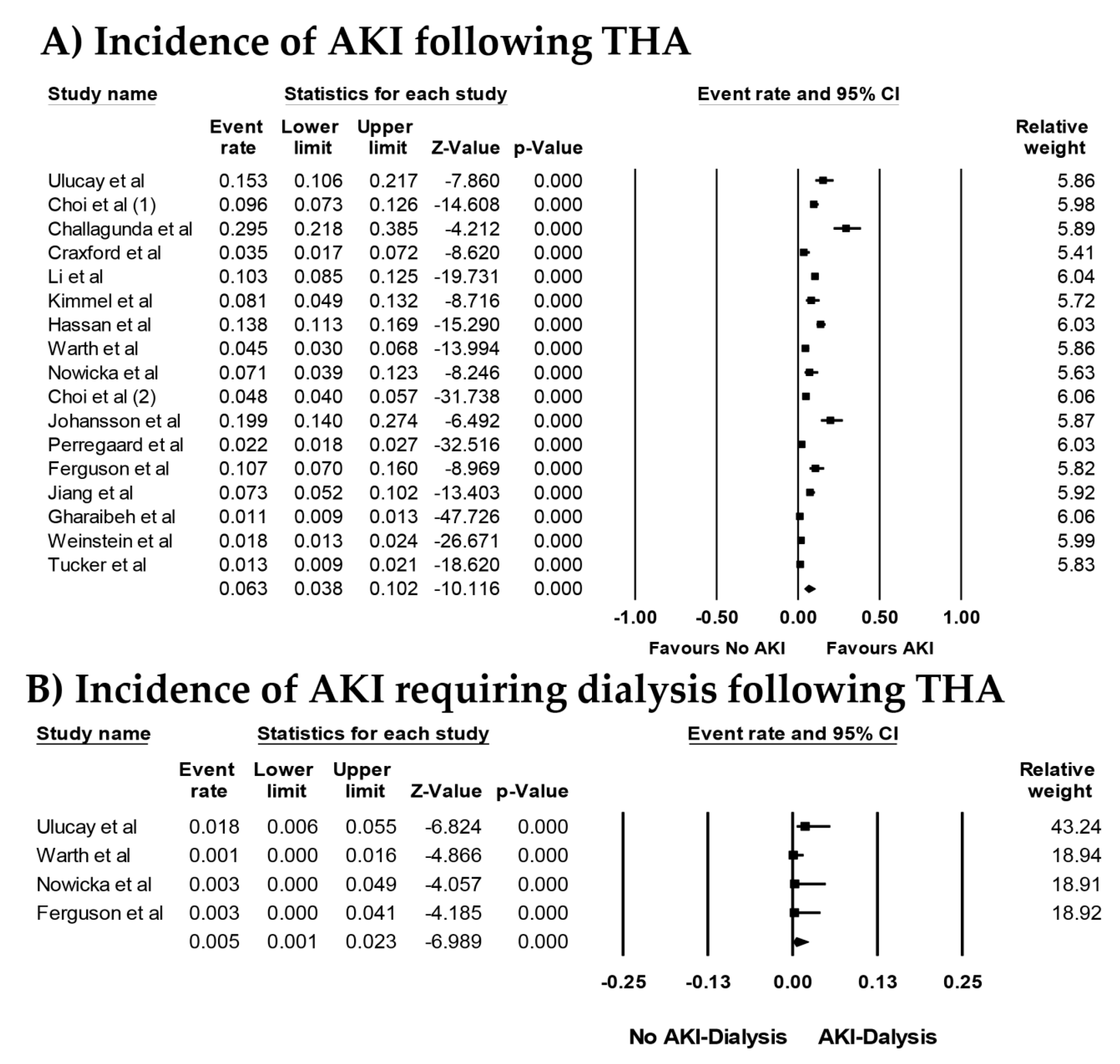
3.1. Incidence of AKI in Patients Undergoing THA
3.2. Risk Factors for AKI in Patients Undergoing THA
3.3. Evaluation for Publication Bias
4. Discussion
Supplementary Materials
Author Contributions
Acknowledgments
Conflicts of Interest
References
- Thongprayoon, C.; Cheungpasitporn, W.; Harrison, A.M.; Kittanamongkolchai, W.; Ungprasert, P.; Srivali, N.; Akhoundi, A.; Kashani, K.B. The comparison of the commonly used surrogates for baseline renal function in acute kidney injury diagnosis and staging. BMC Nephrol. 2016, 17, 6. [Google Scholar] [CrossRef] [PubMed]
- Cheungpasitporn, W.; Thongprayoon, C.; Srivali, N.; O’corragain, O.A.; Edmonds, P.J.; Ungprasert, P.; Kittanamongkolchai, W.; Erickson, S.B. Preoperative renin-angiotensin system inhibitors use linked to reduced acute kidney injury: A systematic review and meta-analysis. Nephrol. Dial. Transplant. 2015, 30, 978–988. [Google Scholar] [CrossRef] [PubMed]
- Hoste, E.A.; Kellum, J.A.; Selby, N.M.; Zarbock, A.; Palevsky, P.M.; Bagshaw, S.M.; Goldstein, S.L.; Cerdá, J.; Chawla, L.S. Global epidemiology and outcomes of acute kidney injury. Nat. Rev. Nephrol. 2018, 14, 607–625. [Google Scholar] [CrossRef] [PubMed]
- Gameiro, J.; Agapito Fonseca, J.; Jorge, S.; Lopes, J.A. Acute Kidney Injury Definition and Diagnosis: A Narrative Review. J. Clin. Med. 2018, 7, 307. [Google Scholar] [CrossRef]
- Sehgal, V.; Bajwa, S.J.; Sehgal, R.; Eagan, J.; Reddy, P.; Lesko, S.M. Predictors of acute kidney injury in geriatric patients undergoing total knee replacement surgery. Int. J. Endocrinol. Metab. 2014, 12, e16713. [Google Scholar] [CrossRef] [PubMed]
- Kim, H.J.; Koh, W.U.; Kim, S.G.; Park, H.S.; Song, J.G.; Ro, Y.J.; Yang, H.S. Early postoperative albumin level following total knee arthroplasty is associated with acute kidney injury: A retrospective analysis of 1309 consecutive patients based on kidney disease improving global outcomes criteria. Medicine 2016, 95, e4489. [Google Scholar] [CrossRef] [PubMed]
- Mehta, R.L.; Burdmann, E.A.; Cerdá, J.; Feehally, J.; Finkelstein, F.; García-García, G.; Godin, M.; Jha, V.; Lameire, N.H.; Levin, N.W.; et al. Recognition and management of acute kidney injury in the International Society of Nephrology 0by25 Global Snapshot: A multinational cross-sectional study. Lancet 2016, 387, 2017–2025. [Google Scholar] [CrossRef]
- Mehta, R.L.; Cerdá, J.; Burdmann, E.A.; Tonelli, M.; García-García, G.; Jha, V.; Susantitaphong, P.; Rocco, M.; Vanholder, R.; Sever, M.S.; et al. International Society of Nephrology’s 0by25 initiative for acute kidney injury (zero preventable deaths by 2025): A human rights case for nephrology. Lancet 2015, 385, 2616–2643. [Google Scholar] [CrossRef]
- Coventry, M.B.; Beckenbaugh, R.D.; Nolan, D.R.; Ilstrup, D.M. 2012 total hip arthroplasties. A study of postoperative course and early complications. J. Bone Joint Surg. Am. 1974, 56, 273–284. [Google Scholar] [CrossRef]
- Sharrock, N.E.; Beksac, B.; Flynn, E.; Go, G.; Della Valle, A.G. Hypotensive epidural anaesthesia in patients with preoperative renal dysfunction undergoing total hip replacement. Br. J. Anaesth. 2006, 96, 207–212. [Google Scholar] [CrossRef] [Green Version]
- Jameson, S.S.; Khan, S.K.; Baker, P.; James, P.; Gray, A.; Reed, M.R.; Deehan, D.J. A national analysis of complications following hemiarthroplasty for hip fracture in older patients. QJM 2012, 105, 455–460. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Horstmann, W.G.; Swierstra, M.J.; Ohanis, D.; Castelein, R.M.; Kollen, B.J.; Verheyen, C.C. Reduction of blood loss with the use of a new combined intra-operative and post-operative autologous blood transfusion system compared with no drainage in primary total hip replacement. Bone Joint J. 2013, 95-B, 616–622. [Google Scholar] [CrossRef] [PubMed]
- Regenbogen, S.E.; Cain-Nielsen, A.H.; Norton, E.C.; Chen, L.M.; Birkmeyer, J.D.; Skinner, J.S. Costs and Consequences of Early Hospital Discharge After Major Inpatient Surgery in Older Adults. JAMA Surg. 2017, 152, e170123. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Frenkel Rutenberg, T.; Daglan, E.; Heller, S.; Velkes, S. A comparison of treatment setting for elderly patients with hip fracture, is the geriatric ward superior to conventional orthopedic hospitalization? Injury 2017, 48, 1584–1588. [Google Scholar] [CrossRef] [PubMed]
- Pulido, L.; Parvizi, J.; Macgibeny, M.; Sharkey, P.F.; Purtill, J.J.; Rothman, R.H.; Hozack, W.J. In hospital complications after total joint arthroplasty. J. Arthroplast. 2008, 23 (Suppl. 1), 139–145. [Google Scholar] [CrossRef] [PubMed]
- McDermott, K.W.; Freeman, W.J.; Elixhauser, A. Overview of Operating Room Procedures During Inpatient Stays in U.S. Hospitals, 2014: Statistical Brief #233. 2006. Available online: https://www.hcup-us.ahrq.gov/reports/statbriefs/sb233-Operating-Room-Procedures-United-States-2014.pdf (accessed on 9 January 2019).
- Abdel, M.P.; Watts, C.D.; Houdek, M.T.; Lewallen, D.G.; Berry, D.J. Epidemiology of periprosthetic fracture of the femur in 32 644 primary total hip arthroplasties: A 40-year experience. Bone Joint J. 2016, 98-B, 461–467. [Google Scholar] [CrossRef] [PubMed]
- Ulucay, C.; Eren, Z.; Kaspar, E.C.; Ozler, T.; Yuksel, K.; Kantarci, G.; Altintas, F. Risk factors for acute kidney injury after hip fracture surgery in the elderly individuals. Geriatr. Orthop. Surg. Rehabil. 2012, 3, 150–156. [Google Scholar] [CrossRef] [PubMed]
- Choi, Y.J.; Lee, E.H.; Hahm, K.D.; Kwon, K.; Ro, Y.J. Transplantation is a risk factor for acute kidney injury in patients undergoing total hip replacement arthroplasty for avascular necrosis: An observational study. Transplant. Proc. 2013, 45, 2220–2225. [Google Scholar] [CrossRef]
- Challagundla, S.R.; Knox, D.; Hawkins, A.; Hamilton, D.; WVFlynn, R.; Robertson, S.; Isles, C. Renal impairment after high-dose flucloxacillin and single-dose gentamicin prophylaxis in patients undergoing elective hip and knee replacement. Nephrol. Dial. Transplant. 2013, 28, 612–619. [Google Scholar] [CrossRef]
- Craxford, S.; Bayley, E.; Needoff, M. Antibiotic-associated complications following lower limb arthroplasty: A comparison of two prophylactic regimes. Eur. J. Orthop. Surg. Traumatol. 2014, 24, 539–543. [Google Scholar] [CrossRef]
- Li, X.; Guo, D.; Shi, G.; Li, R.; Li, X.; Shen, R.; Wang, H.; Li, Y.; Yuan, F.; Han, G. Role of total hip replacement arthroplasty between transplantation and acute kidney injury. Ren. Fail. 2014, 36, 899–903. [Google Scholar] [CrossRef] [Green Version]
- Kimmel, L.A.; Wilson, S.; Janardan, J.D.; Liew, S.M.; Walker, R.G. Incidence of acute kidney injury following total joint arthroplasty: A retrospective review by RIFLE criteria. Clin. Kidney J. 2014, 7, 546–551. [Google Scholar] [CrossRef]
- Warth, L.C.; Noiseux, N.O.; Hogue, M.H.; Klaassen, A.L.; Liu, S.S.; Callaghan, J.J. Risk of Acute Kidney Injury After Primary and Revision Total Hip Arthroplasty and Total Knee Arthroplasty Using a Multimodal Approach to Perioperative Pain Control Including Ketorolac and Celecoxib. J. Arthroplast. 2016, 31, 253–255. [Google Scholar] [CrossRef] [PubMed]
- Nowicka, A.; Selvaraj, T. Incidence of acute kidney injury after elective lower limb arthroplasty. J. Clin. Anesth. 2016, 34, 520–523. [Google Scholar] [CrossRef] [PubMed]
- Choi, Y.J.; Kim, S.O.; Sim, J.H.; Hahm, K.D. Postoperative Anemia Is Associated with Acute Kidney Injury in Patients Undergoing Total Hip Replacement Arthroplasty: A Retrospective Study. Anesth. Analg. 2016, 122, 1923–1928. [Google Scholar] [CrossRef] [PubMed]
- Johansson, S.; Christensen, O.M.; Thorsmark, A.H. A retrospective study of acute kidney injury in hip arthroplasty patients receiving gentamicin and dicloxacillin. Acta Orthop. 2016, 87, 589–591. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Perregaard, H.; Damholt, M.B.; Solgaard, S.; Petersen, M.B. Renal function after elective total hip replacement. Acta Orthop. 2016, 87, 235–238. [Google Scholar] [CrossRef]
- Ferguson, K.B.; Winter, A.; Russo, L.; Khan, A.; Hair, M.; MacGregor, M.S.; Holt, G. Acute kidney injury following primary hip and knee arthroplasty surgery. Ann. R. Coll. Surg. Engl. 2017, 99, 307–312. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jiang, E.X.; Gogineni, H.C.; Mayerson, J.L.; Glassman, A.H.; Magnussen, R.A.; Scharschmidt, T.J. Acute Kidney Disease After Total Hip and Knee Arthroplasty: Incidence and Associated Factors. J. Arthroplast. 2017, 32, 2381–2385. [Google Scholar] [CrossRef]
- Gharaibeh, K.A.; Hamadah, A.M.; Sierra, R.J.; Leung, N.; Kremers, W.K.; El-Zoghby, Z.M. The Rate of Acute Kidney Injury After Total Hip Arthroplasty Is Low but Increases Significantly in Patients with Specific Comorbidities. J. Bone Joint Surg. Am. 2017, 99, 1819–1826. [Google Scholar]
- Weinstein, S.M.; YaDeau, J.T.; Memtsoudis, S.G. Lack of Association Between Levels and Length of Intraoperative Controlled Hypotension and Acute Kidney Injury in Total Hip Arthroplasty Patients Receiving Neuraxial Anesthesia. Reg. Anesth. Pain Med. 2018, 43, 725–731. [Google Scholar] [CrossRef] [PubMed]
- Tucker, A.; Hegarty, P.; Magill, P.J.; Blaney, J.; Armstrong, L.V.; McCaffrey, J.E.; Beverland, D.E. Acute Kidney Injury After Prophylactic Cefuroxime and Gentamicin in Patients Undergoing Primary Hip and Knee Arthroplasty-A Propensity Score-Matched Study. J. Arthroplast. 2018, 33, 3009–3015. [Google Scholar] [CrossRef] [PubMed]
- Dubrovskaya, Y.; Tejada, R.; Bosco, I.I.I.J.; Stachel, A.; Chen, D.; Feng, M.; Rosenberg, A.; Phillips, M. Single high dose gentamicin for perioperative prophylaxis in orthopedic surgery: Evaluation of nephrotoxicity. SAGE Open Med. 2015, 3. [Google Scholar] [CrossRef] [PubMed]
- Bell, S.; Davey, P.; Nathwani, D.; Marwick, C.; Vadiveloo, T.; Sneddon, J.; Patton, A.; Bennie, M.; Fleming, S.; Donnan, P.T. Risk of AKI with gentamicin as surgical prophylaxis. J. Am. Soc. Nephrol. 2014, 25, 2625–2632. [Google Scholar] [CrossRef] [PubMed]
- Ross, A.D.; Boscainos, P.J.; Malhas, A.; Wigderowitz, C. Peri-operative renal morbidity secondary to gentamicin and flucloxacillin chemoprophylaxis for hip and knee arthroplasty. Scott. Med. J. 2013, 58, 209–212. [Google Scholar] [CrossRef] [PubMed]
- Hassan, B.K.; Sahlstrom, A.; Dessau, R.B. Risk factors for renal dysfunction after total hip joint replacement; a retrospective cohort study. J. Orthop. Surg. Res. 2015, 10, 158. [Google Scholar] [CrossRef] [PubMed]
- Bailey, O.; Torkington, M.S.; Anthony, I.; Wells, J.; Blyth, M.; Jones, B. Antibiotic-related acute kidney injury in patients undergoing elective joint replacement. Bone Joint J. 2014, 96-B, 395–398. [Google Scholar] [CrossRef]
- Bennet, S.J.; Berry, O.M.; Goddard, J.; Keating, J.F. Acute renal dysfunction following hip fracture. Injury 2010, 41, 335–338. [Google Scholar] [CrossRef]
- Bjerregaard, L.S.; Jorgensen, C.C.; Kehlet, H. Serious renal and urological complications in fast-track primary total hip and knee arthroplasty; a detailed observational cohort study. Minerva Anestesiol. 2016, 82, 757–776. [Google Scholar]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. PLoS Med. 2009, 6, e1000097. [Google Scholar] [CrossRef]
- Von Elm, E.; Altman, D.G.; Egger, M.; Pocock, S.J.; Gotzsche, P.C.; Vandenbroucke, J.P. The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement: Guidelines for reporting observational studies. PLoS Med. 2007, 4, e296. [Google Scholar] [CrossRef] [PubMed]
- DerSimonian, R.; Laird, N. Meta-analysis in clinical trials. Control. Clin. Trials 1986, 7, 177–188. [Google Scholar] [CrossRef]
- Higgins, J.P.; Thompson, S.G.; Deeks, J.J.; Altman, D.G. Measuring inconsistency in meta-analyses. BMJ 2003, 327, 557–560. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Easterbrook, P.J.; Berlin, J.A.; Gopalan, R.; Matthews, D.R. Publication bias in clinical research. Lancet 1991, 337, 867–872. [Google Scholar] [CrossRef]
- Jafari, S.M.; Huang, R.; Joshi, A.; Parvizi, J.; Hozack, W.J. Renal impairment following total joint arthroplasty: Who is at risk? J. Arthroplast. 2010, 25, 49–53. [Google Scholar] [CrossRef] [PubMed]
- Weingarten, T.N.; Gurrieri, C.; Jarett, P.D.; Brown, D.R.; Berntson, N.J.; Calaro, R.D., Jr.; Kor, D.J.; Berry, D.J.; Garovic, V.D.; Nicholson, W.T.; et al. Acute kidney injury following total joint arthroplasty: Retrospective analysis. Can. J. Anaesth. 2012, 59, 1111–1118. [Google Scholar] [CrossRef] [PubMed]
- Nielson, E.; Hennrikus, E.; Lehman, E.; Mets, B. Angiotensin axis blockade, hypotension, and acute kidney injury in elective major orthopedic surgery. J. Hosp. Med. 2014, 9, 283–288. [Google Scholar] [CrossRef] [Green Version]
- Ward, D.T.; Metz, L.N.; Horst, P.K.; Kim, H.T.; Kuo, A.C. Complications of Morbid Obesity in Total Joint Arthroplasty: Risk Stratification Based on BMI. J. Arthroplast. 2015, 30, 42–46. [Google Scholar] [CrossRef]
- Marty, P.; Szatjnic, S.; Ferre, F.; Conil, J.M.; Mayeur, N.; Fourcade, O.; Silva, S.; Minville, V. Doppler renal resistive index for early detection of acute kidney injury after major orthopaedic surgery: A prospective observational study. Eur. J. Anaesthesiol. 2015, 32, 37–43. [Google Scholar] [CrossRef]
- Courtney, P.M.; Melnic, C.M.; Zimmer, Z.; Anari, J.; Lee, G.C. Addition of Vancomycin to Cefazolin Prophylaxis Is Associated With Acute Kidney Injury After Primary Joint Arthroplasty. Clin. Orthop. Relat. Res. 2015, 473, 2197–2203. [Google Scholar] [CrossRef]
- Opperer, M.; Poeran, J.; Rasul, R.; Mazumdar, M.; Memtsoudis, S.G. Use of perioperative hydroxyethyl starch 6% and albumin 5% in elective joint arthroplasty and association with adverse outcomes: A retrospective population based analysis. BMJ 2015, 350, h1567. [Google Scholar] [CrossRef] [PubMed]
- Aeng, E.S.; Shalansky, K.F.; Lau, T.T.; Zalunardo, N.; Li, G.; Bowie, W.R.; Duncan, C.P. Acute Kidney Injury With Tobramycin-Impregnated Bone Cement Spacers in Prosthetic Joint Infections. Ann. Pharmacother. 2015, 49, 1207–1213. [Google Scholar] [CrossRef] [PubMed]
- Tan, T.L.; Kheir, M.M.; Tan, D.D.; Filippone, E.J.; Tischler, E.H.; Chen, A.F. Chronic Kidney Disease Linearly Predicts Outcomes After Elective Total Joint Arthroplasty. J. Arthroplast. 2016, 31, 175–179. [Google Scholar] [CrossRef]
- Nadkarni, G.N.; Patel, A.A.; Ahuja, Y.; Annapureddy, N.; Agarwal, S.K.; Simoes, P.K.; Konstantinidis, I.; Kamat, S.; Archdeacon, M.; Thakar, C.V. Incidence, Risk Factors, and Outcome Trends of Acute Kidney Injury in Elective Total Hip and Knee Arthroplasty. Am. J. Orthop. 2016, 45, E12–E19. [Google Scholar] [PubMed]
- Meller, M.M.; Toossi, N.; Gonzalez, M.H.; Son, M.S.; Lau, E.C.; Johanson, N. Surgical Risks and Costs of Care are Greater in Patients Who Are Super Obese and Undergoing THA. Clin. Orthop. Relat. Res. 2016, 474, 2472–2481. [Google Scholar] [CrossRef] [Green Version]
- Geller, J.A.; Cunn, G.; Herschmiller, T.; Murtaugh, T.; Chen, A. Acute Kidney Injury After First-Stage Joint Revision for Infection: Risk Factors and the Impact of Antibiotic Dosing. J. Arthroplast. 2017, 32, 3120–3125. [Google Scholar] [CrossRef]
- Zainudheen, A.; Scott, I.A.; Caney, X. Association of renin angiotensin antagonists with adverse perioperative events in patients undergoing elective orthopaedic surgery: A case-control study. Intern. Med. J. 2017, 47, 999–1005. [Google Scholar] [CrossRef]
- Jamsa, P.; Jamsen, E.; Lyytikainen, L.P.; Kalliovalkama, J.; Eskelinen, A.; Oksala, N. Risk factors associated with acute kidney injury in a cohort of 20,575 arthroplasty patients. Acta Orthop. 2017, 88, 370–376. [Google Scholar] [CrossRef]
- Yadav, A.; Alijanipour, P.; Ackerman, C.T.; Karanth, S.; Hozack, W.J.; Filippone, E.J. Acute Kidney Injury Following Failed Total Hip and Knee Arthroplasty. J. Arthroplast. 2018, 33, 3297–3303. [Google Scholar] [CrossRef]
- Klement, M.R.; Nickel, B.T.; Bala, A.; Penrose, C.T.; Green, C.L.; Wellman, S.S.; Bolognesi, M.P.; Seyler, T.M. Dual Diagnosis and Total Hip Arthroplasty. Orthopedics 2018, 41, e321–e327. [Google Scholar] [CrossRef]
- Abar, O.; Toossi, N.; Johanson, N. Cost and determinants of acute kidney injury after elective primary total joint arthroplasty. Arthroplast. Today. 2018, 4, 335–339. [Google Scholar] [CrossRef] [PubMed]
- Cheungpasitporn, W.; Thongprayoon, C.; Kittanamongkolchai, W.; Srivali, N.; O’Corragain, O.A.; Edmonds, P.J.; Ratanapo, S.; Spanuchart, I.; Erickson, S.B. Comparison of renal outcomes in off-pump versus on-pump coronary artery bypass grafting: A systematic review and meta-analysis of randomized controlled trials. Nephrology 2015, 20, 727–735. [Google Scholar] [CrossRef] [PubMed]
- Sakhuja, A.; Kashani, K.; Schold, J.; Cheungpasitporn, W.; Soltesz, E.; Demirjian, S. Hospital procedure volume does not predict acute kidney injury after coronary artery bypass grafting-a nationwide study. Clin. Kidney J. 2017, 10, 769–775. [Google Scholar] [CrossRef] [PubMed]
- Cheungpasitporn, W.; Thongprayoon, C.; Kashani, K. Transcatheter Aortic Valve Replacement: A Kidney’s Perspective. J. Ren. Inj. Prev. 2016, 5, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Thongprayoon, C.; Cheungpasitporn, W.; Lin, J.; Mao, M.A.; Qian, Q. Acute kidney injury in octogenarians after heart valve replacement surgery: A study of two periods over the last decade. Clin. Kidney J. 2017, 10, 648–654. [Google Scholar] [CrossRef] [PubMed]
- Napier, R.J.; Spence, D.; Diamond, O.; O’Brien, S.; Walsh, T.; Beverland, D.E. Modifiable factors delaying early discharge following primary joint arthroplasty. Eur. J. Orthop. Surg. Traumatol. 2013, 23, 665–669. [Google Scholar] [CrossRef] [PubMed]
- Panteli, M.; Habeeb, S.; McRoberts, J.; Porteous, M.J. Enhanced care for primary hip arthroplasty: Factors affecting length of hospital stay. Eur. J. Orthop. Surg. Traumatol. 2014, 24, 353–358. [Google Scholar] [CrossRef] [PubMed]
- Schairer, W.W.; Vail, T.P.; Bozic, K.J. What are the rates and causes of hospital readmission after total knee arthroplasty? Clin. Orthop. Relat. Res. 2014, 472, 181–187. [Google Scholar] [CrossRef] [PubMed]
- Pugely, A.J.; Callaghan, J.J.; Martin, C.T.; Cram, P.; Gao, Y. Incidence of and risk factors for 30-day readmission following elective primary total joint arthroplasty: Analysis from the ACS-NSQIP. J. Arthroplast. 2013, 28, 1499–1504. [Google Scholar] [CrossRef]
- Coca, S.G.; Yusuf, B.; Shlipak, M.G.; Garg, A.X.; Parikh, C.R. Long-term risk of mortality and other adverse outcomes after acute kidney injury: A systematic review and meta-analysis. Am. J. Kidney Dis. 2009, 53, 961–973. [Google Scholar] [CrossRef]
- Murugan, R.; Kellum, J.A. Acute kidney injury: what’s the prognosis? Nat. Rev. Nephrol. 2011, 7, 209–217. [Google Scholar] [CrossRef] [PubMed]
- Goren, O.; Matot, I. Perioperative acute kidney injury. Br. J. Anaesth. 2015, 115 (Suppl. 2), ii3–ii14. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Xu, N.; Long, Q.; He, T.; Liu, X.; Dai, H.; Lu, Y.; Wen, J.; Wu, Q.; Yuan, H. Association between preoperative renin-angiotensin system inhibitor use and postoperative acute kidney injury risk in patients with hypertension. Clin. Nephrol. 2018, 89, 403–414. [Google Scholar] [CrossRef] [PubMed]
- Tagawa, M.; Ogata, A.; Hamano, T. Pre- and/or Intra-Operative Prescription of Diuretics, but Not Renin-Angiotensin-System Inhibitors, Is Significantly Associated with Acute Kidney Injury after Non-Cardiac Surgery: A Retrospective Cohort Study. PLoS ONE 2015, 10, e0132507. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Study | Year | Country | Study Design | Procedures/Patients | Number of Patients | AKI Definition | Incidence |
|---|---|---|---|---|---|---|---|
| Ulucay et al. [18] | 2012 | Turkey | Cohort | Cemented bipolar hip arthroplasty for femur neck fracture; aged ≥65 years | 163 | Acute kidney injury; AKIN criteria | 25/163 (15.3%) Dialysis 3/163 (1.8%) |
| Choi et al. [1,19] | 2013 | South Korea | Cohort | Total hip replacement for avascular necrosis | 489 | Acute kidney injury; AKIN criteria | 47/489 (9.6%) |
| Challagunda et al. [20] | 2013 | UK | Cohort | Elective hip surgery | 112 | Acute kidney injury; RIFLE criteria | 33/112 (29.5%) |
| Craxford et al. [21] | 2014 | UK | Cohort | Total hip replacement | 200 | Acute kidney injury; RIFLE criteria | 7/200 (3.5%) |
| Li et al. [22] | 2014 | China | Cohort | Total hip replacement | 900 | Acute kidney injury; AKIN criteria | 93/900 (10.3%) |
| Kimmel et al. [23] | 2014 | Australia | Cohort | Primary elective total hip arthroplasty | 173 | Acute kidney injury; RIFLE criteria | 14/173 (8.1%) |
| Hassan et al. [37] | 2015 | Denmark | Cohort | Primary hip replacement | 586 | Acute kidney injury; RIFLE criteria | 81/586 (13.8%) |
| Warth et al. [24] | 2016 | USA | Cohort | Total hip arthroplasty | 488 | Acute kidney injury; AKIN criteria | 22/488 (4.5%) Dialysis 0/488 (0%) |
| Nowicka et al. [25] | 2016 | UK | Cohort | Elective hip arthroplasty | 156 | Acute kidney injury; AKIN criteria | 11/156 (7.1%) Dialysis 0/156 (0%) |
| Choi et al. [2,26] | 2016 | South Korea | Cohort | Total hip replacement | 2467 | Acute kidney injury; AKIN criteria | 119/2467 (4.8%) |
| Johansson et al. [27] | 2016 | Denmark | Cohort | Elective total hip replacement | 136 | Acute kidney injury; KDIGO criteria | 27/136 (19.9%) |
| Perregaard et al. [28] | 2016 | Denmark | Cohort | Primary elective total hip replacement | 3416 | Acute kidney injury; KDIGO criteria | 75/3416 (2.2%) |
| Ferguson et al. [29] | 2017 | UK | Cohort | Primary hip arthroplasty | 187 | Acute kidney injury; KDIGO criteria | 20/187 (10.7%) Dialysis 0/187 (0%) |
| Jiang et al. [30] | 2017 | USA | Cohort | Total hip arthroplasty | 411 | Acute kidney injury; RIFLE criteria | 30/411 (7.3%) |
| Gharaibeh et al. [31] | 2017 | USA | Cohort | Total hip arthroplasty | 10323 | Acute kidney injury; KDIGO criteria | 114/10323 (1.1%) |
| Weinstein et al. [32] | 2018 | USA | Cohort | Unilateral total hip arthroplasty with intraoperative controlled hypotension under neuraxial anesthesia | 2431 | Acute kidney injury; RIFLE or AKIN criteria | 45/2431 (1.9%) |
| Tucker et al. [33] | 2018 | UK | Cohort | Primary hip arthroplasty | 1420 | Acute kidney injury; AKIN criteria | 19/1420 (1.3%) |
| Study | Risk Factors for AKI |
|---|---|
| Jafari et al. [46] | Elevated BMI, elevated baseline creatinine, history of COPD, liver disease, CHF, hypertension, underlying heart disease |
| Weingarten et al. [47] | Elevated BMI, DM, the number of baseline antihypertensive medications, cerebral or peripheral vascular disease, the use of general anesthesia, perioperative blood transfusion |
| Ulucay et al. [18] | Lower baseline eGFR |
| Choi et al. [1,19] | Transplantation, increased weight |
| Li et al. [22] | Transplantation, increased weight |
| Challagundla et al. [20] | Male, ACEI/ARB |
| Nielson et al. [48] | Preoperative ACEI/ARB, BMI, CAD, intra-operative hypotension |
| Kimmel et al. [23] | Older age, increased BMI, lower baseline eGFR, NSAID use, ACEI/ARB use, blood transfusion |
| Ward et al. [49] | Increased BMI |
| Marty et al. [50] | Postoperative resistive index |
| Courtney et al. [51] | Dual antibiotics prophylaxis (cefazolin + vancomycin vs. cefazolin), ASA classification, preoperative kidney disease |
| Opperer et al. [52] | Perioperative fluid resuscitation with 6% HES or 5% albumin |
| Aeng et al. [53] | Gentamicin in premanufactured bone cement, intraoperative blood transfusion, postoperative NSAID use |
| Warth et al. [24] | Older age, elevated BMI, DM, smoking |
| Tan et al. [54] | CKD |
| Nadkarni et al. [55] | Older age, male sex, black race, CKD, CHF, chronic liver disease, hypertension, DM, atrial fibrillation, HCV infection, postoperative sepsis, acute MI, blood transfusion, urban hospital, small hospital size |
| Meller et al. [56] | Morbid obesity |
| Choi et al. [2,26] | Postoperative anemia, older age, male sex, BMI <22 or ≥25, DM, beta-blocker, ARB use |
| Ferguson et al. [29] | Older age, the use of ≥1 L of postoperative fluid |
| Johansson et al. [27] | Gentamicin, female sex |
| Geller et al. [57] | Higher BMI, lower baseline hemoglobin, history of comorbid condition (DM, CKD, CVD, hypertension) |
| Jiang et al. [30] | Perioperative ACEI/ARB use, vancomycin use, increased BMI |
| Zainudheen et al. [58] | Use of renin-angiotensin antagonists |
| Jamsa et al. [59] | Lower preoperative eGFR, ASA classification, BMI, duration of operation |
| Ghareibeh et al. [31] | Entire cohort: older age, male, CKD, heart failure, diabetes, hypertension Nested case control: elevated BMI, heart failure, DM, hypertension, lower GFR, transfusion |
| Yadav et al. [60] | Older age, surgery for periprosthetic joint infection, CKD, total number of surgeries |
| Weinstein et al. [32] | Lower baseline GFR, lower baseline hemoglobin, previous NSAID use |
| Tucker et al. [33] | Gentamicin use |
| Klement et al. [61] | Co-occurrence of a mental illness and a substance abuse disorder |
| Abar et al. [62] | Elevated preoperative creatinine, larger postoperative drop in hemoglobin, and higher ASA classification |
| Hassan et al. [37] | Older age, hypertension, general anesthesia, high ASA score, low baseline systolic and diastolic blood pressure, hip fracture |
| Dubrovskaya et al. [34] | Hospital stay >1 day prior to surgery, knee or hip surgery, DM |
| Bailey et al. [38] | Prophylactic use of flucloxacillin and gentamicin versus cefuroxime alone |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Thongprayoon, C.; Kaewput, W.; Thamcharoen, N.; Bathini, T.; Watthanasuntorn, K.; Salim, S.A.; Ungprasert, P.; Lertjitbanjong, P.; Aeddula, N.R.; Torres-Ortiz, A.; et al. Acute Kidney Injury in Patients Undergoing Total Hip Arthroplasty: A Systematic Review and Meta-Analysis. J. Clin. Med. 2019, 8, 66. https://doi.org/10.3390/jcm8010066
Thongprayoon C, Kaewput W, Thamcharoen N, Bathini T, Watthanasuntorn K, Salim SA, Ungprasert P, Lertjitbanjong P, Aeddula NR, Torres-Ortiz A, et al. Acute Kidney Injury in Patients Undergoing Total Hip Arthroplasty: A Systematic Review and Meta-Analysis. Journal of Clinical Medicine. 2019; 8(1):66. https://doi.org/10.3390/jcm8010066
Chicago/Turabian StyleThongprayoon, Charat, Wisit Kaewput, Natanong Thamcharoen, Tarun Bathini, Kanramon Watthanasuntorn, Sohail Abdul Salim, Patompong Ungprasert, Ploypin Lertjitbanjong, Narothama Reddy Aeddula, Aldo Torres-Ortiz, and et al. 2019. "Acute Kidney Injury in Patients Undergoing Total Hip Arthroplasty: A Systematic Review and Meta-Analysis" Journal of Clinical Medicine 8, no. 1: 66. https://doi.org/10.3390/jcm8010066