Incidence and Impact of Acute Kidney Injury after Liver Transplantation: A Meta-Analysis


 , , , , , and
, , , , , and 
Abstract
:1. Introduction
2. Methods
2.1. Search Strategy and Literature Review
2.2. Selection Criteria
2.3. Data Abstraction
2.4. Statistical Analysis
3. Results
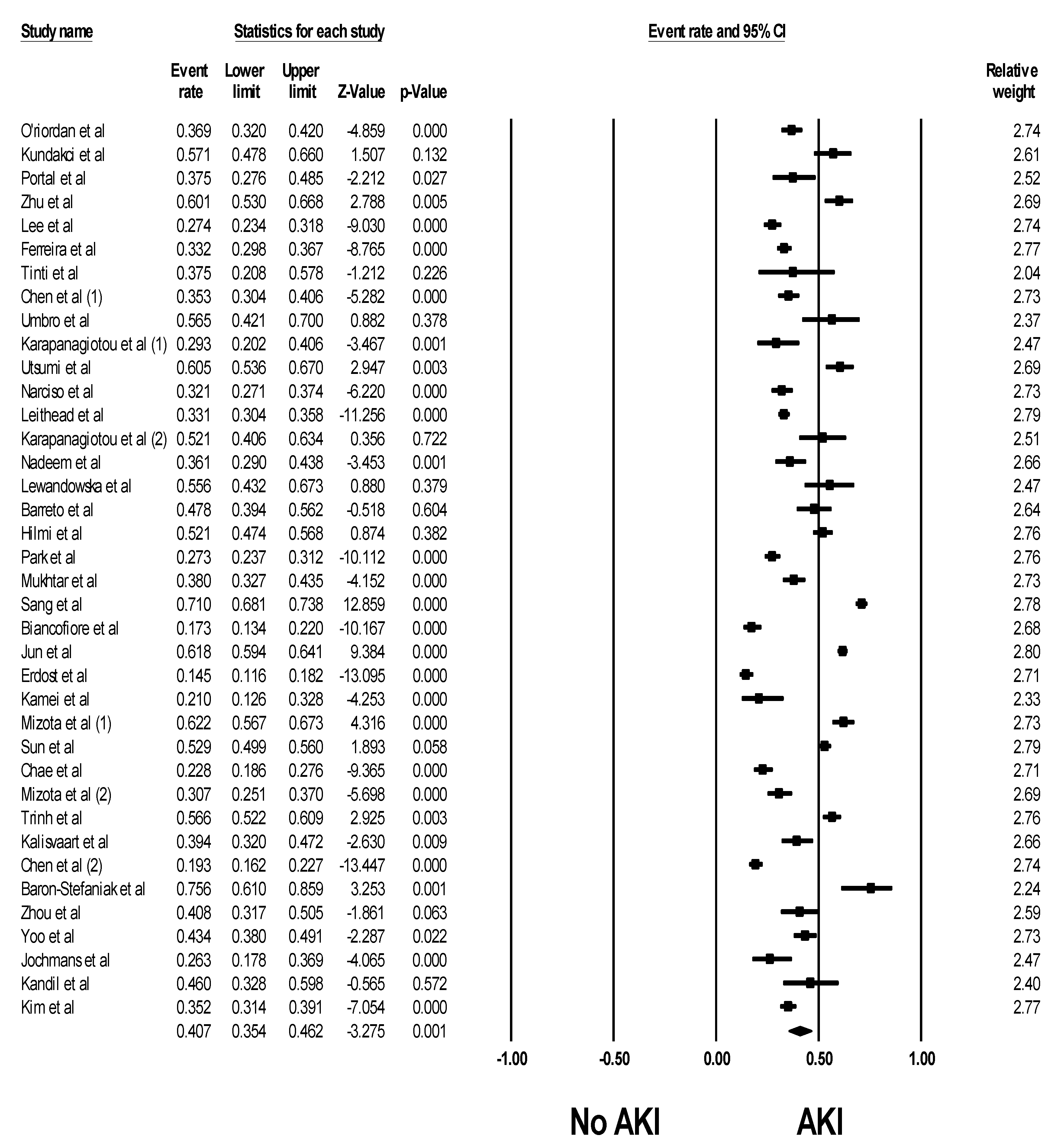
3.1. Incidence of Post-LTx AKI
3.2. Risk Factors for Post-LTx AKI
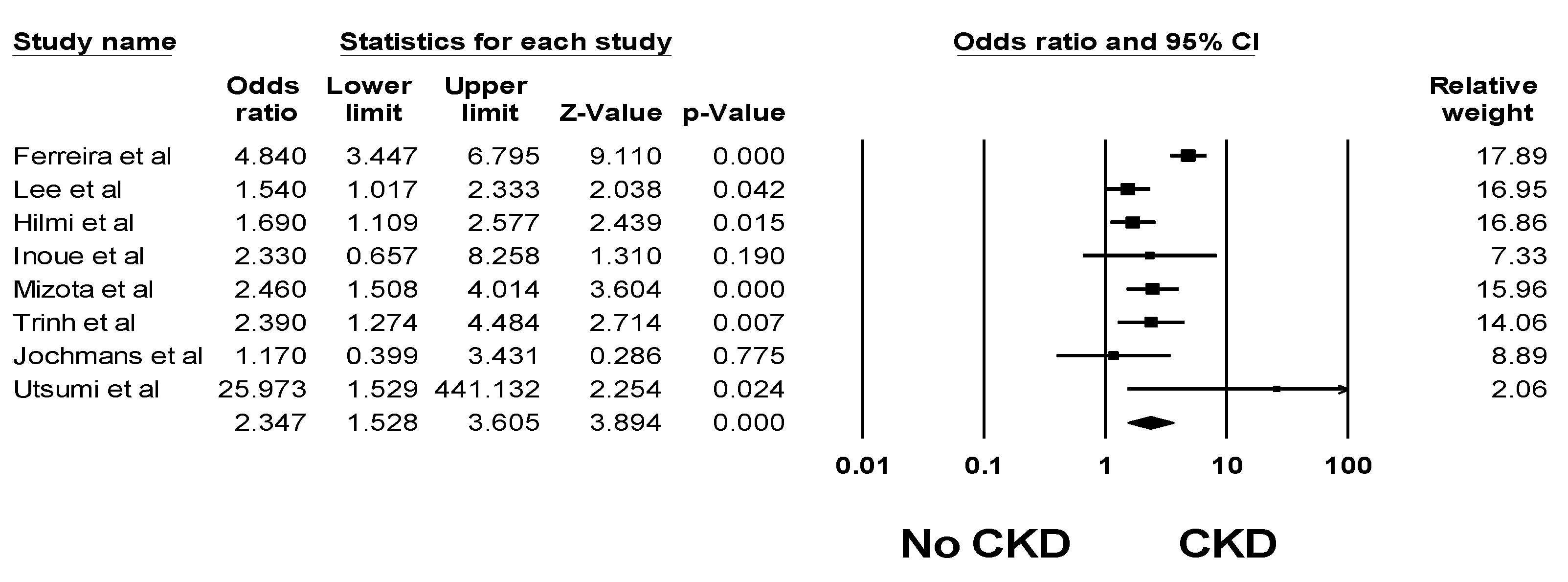
3.3. Impacts of Post-LTx AKI on Patient Outcomes
3.4. Evaluation for Publication Bias
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Acknowledgments
Conflicts of Interest
References
- Gameiro, J.; Agapito Fonseca, J.; Jorge, S.; Lopes, J.A. Acute Kidney Injury Definition and Diagnosis: A Narrative Review. J. Clin. Med. 2018, 7, 307. [Google Scholar] [CrossRef] [PubMed]
- Hoste, E.A.J.; Kellum, J.A.; Selby, N.M.; Zarbock, A.; Palevsky, P.M.; Bagshaw, S.M.; Goldstein, S.L.; Cerdá, J.; Chawla, L.S. Global epidemiology and outcomes of acute kidney injury. Nat. Rev. Nephrol. 2018, 14, 607–625. [Google Scholar] [CrossRef] [PubMed]
- Mehta, R.L.; Burdmann, E.A.; Cerdá, J.; Feehally, J.; Finkelstein, F.; García-García, G.; Godin, M.; Jha, V.; Lameire, N.H.; Levin, N.W.; et al. Recognition and management of acute kidney injury in the International Society of Nephrology 0by25 Global Snapshot: A multinational cross-sectional study. Lancet 2016, 387, 2017–2025. [Google Scholar] [CrossRef]
- Mehta, R.L.; Burdmann, E.A.; Cerdá, J.; Feehally, J.; Finkelstein, F.; García-García, G.; Godin, M.; Jha, V.; Lameire, N.H.; Levin, N.W.; et al. International Society of Nephrology’s 0by25 initiative for acute kidney injury (zero preventable deaths by 2025): A human rights case for nephrology. Lancet 2015, 385, 2616–2643. [Google Scholar] [CrossRef]
- Sawhney, S.; Marks, A.; Fluck, N.; Levin, A.; McLernon, D.; Prescott, G.; Black, C. Post-discharge kidney function is associated with subsequent ten-year renal progression risk among survivors of acute kidney injury. Kidney Int. 2017, 92, 440–452. [Google Scholar] [CrossRef]
- Ponce, D.; Balbi, A. Acute kidney injury: Risk factors and management challenges in developing countries. Int. J. Nephrol. Renov. Dis. 2016, 9, 193–200. [Google Scholar] [CrossRef]
- Pavkov, M.E.; Harding, J.L.; Burrows, N.R. Trends in Hospitalizations for Acute Kidney Injury—United States, 2000–2014. Morb. Mortal. Wkly. Rep. 2018, 67, 289. [Google Scholar] [CrossRef]
- United States Renal Data System. 2017. Available online: https://www.usrds.org/2017/download/v1_c05_AKI_17.pdf (accessed on 15 February 2019).
- Mokdad, A.A.; Lopez, A.D.; Shahraz, S.; Lozano, R.; Mokdad, A.H.; Stanaway, J.; Murray, C.J.; Naghavi, M. Liver cirrhosis mortality in 187 countries between 1980 and 2010: A systematic analysis. BMC Med. 2014, 12, 145. [Google Scholar] [CrossRef] [PubMed]
- McCauley, J.; Van Thiel, D.H.; Starzl, T.E.; Puschett, J.B. Acute and chronic renal failure in liver transplantation. Nephron 1990, 55, 121–128. [Google Scholar] [CrossRef] [PubMed]
- Bilbao, I.; Charco, R.; Balsells, J.; Lazaro, J.L.; Hidalgo, E.; Llopart, L.; Murio, E.; Margarit, C. Risk factors for acute renal failure requiring dialysis after liver transplantation. Clin. Transplant. 1998, 12, 123–129. [Google Scholar]
- Carmona, M.; Álvarez, M.; Marco, J.; Mahíllo, B.; Domínguez-Gil, B.; Núñez, J.R.; Matesanz, R. Global Organ Transplant Activities in 2015. Data from the Global Observatory on Donation and Transplantation (GODT). Transplantation 2017, 101, S29. [Google Scholar] [CrossRef]
- White, S.L.; Hirth, R.; Mahillo, B.; Dominguez-Gil, B.; Delmonico, F.L.; Noel, L.; Chapman, J.; Matesanz, R.; Carmona, M.; Alvarez, M.; et al. The global diffusion of organ transplantation: Trends, drivers and policy implications. Bull. World Health Organ. 2014, 92, 826–835. [Google Scholar] [CrossRef]
- Kim, W.H.; Lee, H.C.; Lim, L.; Ryu, H.G.; Jung, C.W. Intraoperative Oliguria with Decreased SvO Predicts Acute Kidney Injury after Living Donor Liver Transplantation. J. Clin. Med. 2018, 8, 29. [Google Scholar] [CrossRef] [PubMed]
- Hamada, M.; Matsukawa, S.; Shimizu, S.; Kai, S.; Mizota, T. Acute kidney injury after pediatric liver transplantation: Incidence, risk factors, and association with outcome. J. Anesth. 2017, 31, 758–763. [Google Scholar] [CrossRef] [PubMed]
- Nadkarni, G.N.; Chauhan, K.; Patel, A.; Saha, A.; Poojary, P.; Kamat, S.; Patel, S.; Ferrandino, R.; Konstantinidis, I.; Garimella, P.S.; et al. Temporal trends of dialysis requiring acute kidney injury after orthotopic cardiac and liver transplant hospitalizations. BMC Nephrol. 2017, 18, 244. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Barri, Y.M.; Sanchez, E.Q.; Jennings, L.W.; Melton, L.B.; Hays, S.; Levy, M.F.; Klintmalm, G.B. Acute kidney injury following liver transplantation: Definition and outcome. Liver Transplant. 2009, 15, 475–483. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chen, J.; Singhapricha, T.; Hu, K.Q.; Hong, J.C.; Steadman, R.H.; Busuttil, R.W.; Xia, V.W. Postliver transplant acute renal injury and failure by the RIFLE criteria in patients with normal pretransplant serum creatinine concentrations: A matched study. Transplantation 2011, 91, 348–353. [Google Scholar] [CrossRef] [PubMed]
- Hilmi, I.A.; Damian, D.; Al-Khafaji, A.; Planinsic, R.; Boucek, C.; Sakai, T.; Chang, C.C.; Kellum, J.A. Acute kidney injury following orthotopic liver transplantation: Incidence, risk factors, and effects on patient and graft outcomes. Br. J. Anaesth. 2015, 114, 919–926. [Google Scholar] [CrossRef]
- Hilmi, I.A.; Damian, D.; Al-Khafaji, A.; Sakai, T.; Donaldson, J.; Winger, D.G.; Kellum, J.A. Acute kidney injury after orthotopic liver transplantation using living donor versus deceased donor grafts: A propensity score-matched analysis. Liver Transplant. 2015, 21, 1179–1185. [Google Scholar] [CrossRef]
- Sun, K.; Hong, F.; Wang, Y.; Agopian, V.G.; Yan, M.; Busuttil, R.W.; Steadman, R.H.; Xia, V.W. Venovenous Bypass Is Associated With a Lower Incidence of Acute Kidney Injury After Liver Transplantation in Patients with Compromised Pretransplant Renal Function. Anesth. Analg. 2017, 125, 1463–1470. [Google Scholar] [CrossRef]
- Wyatt, C.M.; Arons, R.R. The burden of acute renal failure in nonrenal solid organ transplantation. Transplantation 2004, 78, 1351–1355. [Google Scholar] [CrossRef] [PubMed]
- Sanchez, E.Q.; Gonwa, T.A.; Levy, M.F.; Goldstein, R.M.; Mai, M.L.; Hays, S.R.; Melton, L.B.; Saracino, G.; Klintmalm, G.B. Preoperative and perioperative predictors of the need for renal replacement therapy after orthotopic liver transplantation. Transplantation 2004, 78, 1048–1054. [Google Scholar] [CrossRef] [PubMed]
- Contreras, G.; Garces, G.; Quartin, A.A.; Cely, C.; LaGatta, M.A.; Barreto, G.A.; Roth, D.; Gomez, E. An epidemiologic study of early renal replacement therapy after orthotopic liver transplantation. J. Am. Soc. Nephrol. 2002, 13, 228–233. [Google Scholar]
- Lebron Gallardo, M.; Herrera Gutierrez, M.E.; Seller Perez, G.; Curiel Balsera, E.; Fernandez Ortega, J.F.; Quesada Garcia, G. Risk factors for renal dysfunction in the postoperative course of liver transplant. Liver Transplant. 2004, 10, 1379–1385. [Google Scholar] [CrossRef] [Green Version]
- Alvares-da-Silva, M.R.; Waechter, F.L.; Francisconi, C.F.; Barros, E.; Thome, F.; Traiber, C.; Fonseca, D.L.; Zingani, J.M.; Sampaio, J.A.; Pinto, R.D.; et al. Risk factors for postoperative acute renal failure at a new orthotopic liver transplantation program. Transplant. Proc. 1999, 31, 3050–3052. [Google Scholar] [CrossRef]
- Rossi, A.P.; Vella, J.P. Acute Kidney Disease After Liver and Heart Transplantation. Transplantation 2016, 100, 506–514. [Google Scholar] [CrossRef] [PubMed]
- Kandil, M.A.; Abouelenain, K.M.; Alsebaey, A.; Rashed, H.S.; Afifi, M.H.; Mahmoud, M.A.; Yassen, K.A. Impact of terlipressin infusion during and after live donor liver transplantation on incidence of acute kidney injury and neutrophil gelatinase-associated lipocalin serum levels: A randomized controlled trial. Clin. Transplant. 2017, 31, e13019. [Google Scholar] [CrossRef] [PubMed]
- Jochmans, I.; Meurisse, N.; Neyrinck, A.; Verhaegen, M.; Monbaliu, D.; Pirenne, J. Hepatic ischemia/reperfusion injury associates with acute kidney injury in liver transplantation: Prospective cohort study. Liver Transplant. 2017, 23, 634–644. [Google Scholar] [CrossRef]
- Zhou, Z.Q.; Fan, L.C.; Zhao, X.; Xia, W.; Luo, A.L.; Tian, Y.K.; Wang, X.R. Risk factors for acute kidney injury after orthotopic liver transplantation: A single-center data analysis. J. Huazhong Univ. Sci. Technol. Med. Sci. 2017, 37, 861–863. [Google Scholar] [CrossRef]
- Yoo, S.; Lee, H.J.; Lee, H.; Ryu, H.G. Association Between Perioperative Hyperglycemia or Glucose Variability and Postoperative Acute Kidney Injury After Liver Transplantation: A Retrospective Observational Study. Anesth. Analg. 2017, 124, 35–41. [Google Scholar] [CrossRef]
- O’Riordan, A.; Wong, V.; McQuillan, R.; McCormick, P.A.; Hegarty, J.E.; Watson, A.J. Acute renal disease, as defined by the RIFLE criteria, post-liver transplantation. Am. J. Transplant. 2007, 7, 168–176. [Google Scholar] [CrossRef]
- Xu, X.; Ling, Q.; Wei, Q.; Wu, J.; Gao, F.; He, Z.L.; Zhou, L.; Zheng, S.S. An effective model for predicting acute kidney injury after liver transplantation. Hepatobiliary Pancreat. Dis. Int. 2010, 9, 259–263. [Google Scholar]
- De Ataide, E.C.; Perales, S.R.; Bortoto, J.B.; Peres, M.A.O.; Filho, F.C.; Stucchi, R.S.B.; Udo, E.; Boin, I. Immunomodulation, Acute Renal Failure, and Complications of Basiliximab Use After Liver Transplantation: Analysis of 114 Patients and Literature Review. Transplant. Proc. 2017, 49, 852–857. [Google Scholar] [CrossRef] [PubMed]
- Zongyi, Y.; Baifeng, L.; Funian, Z.; Hao, L.; Xin, W. Risk factors of acute kidney injury after orthotopic liver transplantation in China. Sci. Rep. 2017, 7, 41555. [Google Scholar] [CrossRef] [Green Version]
- Croome, K.P.; Lee, D.D.; Croome, S.; Chadha, R.; Livingston, D.; Abader, P.; Keaveny, A.P.; Taner, C.B. The impact of post-reperfusion syndrome during liver transplantation using livers with significant macrosteatosis. Am. J. Transplant. 2019. [Google Scholar] [CrossRef] [PubMed]
- De Haan, J.E.; Hoorn, E.J.; de Geus, H.R.H. Acute kidney injury after liver transplantation: Recent insights and future perspectives. Best Pract. Res. Clin. Gastroenterol. 2017, 31, 161–169. [Google Scholar] [CrossRef] [PubMed]
- Leithead, J.A.; Armstrong, M.J.; Corbett, C.; Andrew, M.; Kothari, C.; Gunson, B.K.; Muiesan, P.; Ferguson, J.W. Hepatic ischemia reperfusion injury is associated with acute kidney injury following donation after brain death liver transplantation. Transpl. Int. 2013, 26, 1116–1125. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Leithead, J.A.; Rajoriya, N.; Gunson, B.K.; Muiesan, P.; Ferguson, J.W. The evolving use of higher risk grafts is associated with an increased incidence of acute kidney injury after liver transplantation. J. Hepatol. 2014, 60, 1180–1186. [Google Scholar] [CrossRef] [PubMed]
- Lee, S.K.; Park, J.B.; Kim, S.J.; Choi, G.S.; Kim, D.J.; Kwon, C.H.; Joh, J.W. Early postoperative renal dysfunction in the adult living donor liver transplantation. Transplant. Proc. 2007, 39, 1517–1519. [Google Scholar] [CrossRef]
- Kundakci, A.; Pirat, A.; Komurcu, O.; Torgay, A.; Karakayali, H.; Arslan, G.; Haberal, M. Rifle criteria for acute kidney dysfunction following liver transplantation: Incidence and risk factors. Transplant. Proc. 2010, 42, 4171–4174. [Google Scholar] [CrossRef]
- Zhu, M.; Li, Y.; Xia, Q.; Wang, S.; Qiu, Y.; Che, M.; Dai, H.; Qian, J.; Ni, Z.; Axelsson, J.; et al. Strong impact of acute kidney injury on survival after liver transplantation. Transplant. Proc. 2010, 42, 3634–3638. [Google Scholar] [CrossRef] [PubMed]
- Karapanagiotou, A.; Kydona, C.; Dimitriadis, C.; Sgourou, K.; Giasnetsova, T.; Fouzas, I.; Imvrios, G.; Gritsi-Gerogianni, N. Acute kidney injury after orthotopic liver transplantation. Transplant. Proc. 2012, 44, 2727–2729. [Google Scholar] [CrossRef]
- Utsumi, M.; Umeda, Y.; Sadamori, H.; Nagasaka, T.; Takaki, A.; Matsuda, H.; Shinoura, S.; Yoshida, R.; Nobuoka, D.; Satoh, D.; et al. Risk factors for acute renal injury in living donor liver transplantation: Evaluation of the RIFLE criteria. Transpl. Int. 2013, 26, 842–852. [Google Scholar] [CrossRef] [PubMed]
- Romano, T.G.; Schmidtbauer, I.; Silva, F.M.; Pompilio, C.E.; D’Albuquerque, L.A.; Macedo, E. Role of MELD score and serum creatinine as prognostic tools for the development of acute kidney injury after liver transplantation. PLoS ONE 2013, 8, e64089. [Google Scholar] [CrossRef]
- Klaus, F.; Keitel da Silva, C.; Meinerz, G.; Carvalho, L.M.; Goldani, J.C.; Cantisani, G.; Zanotelli, M.L.; Duro Garcia, V.; Keitel, E. Acute kidney injury after liver transplantation: Incidence and mortality. Transplant. Proc. 2014, 46, 1819–1821. [Google Scholar] [CrossRef] [PubMed]
- Kim, J.M.; Jo, Y.Y.; Na, S.W.; Kim, S.I.; Choi, Y.S.; Kim, N.O.; Park, J.E.; Koh, S.O. The predictors for continuous renal replacement therapy in liver transplant recipients. Transplant. Proc. 2014, 46, 184–191. [Google Scholar] [CrossRef]
- Karapanagiotou, A.; Dimitriadis, C.; Papadopoulos, S.; Kydona, C.; Kefsenidis, S.; Papanikolaou, V.; Gritsi-Gerogianni, N. Comparison of RIFLE and AKIN criteria in the evaluation of the frequency of acute kidney injury in post-liver transplantation patients. Transplant. Proc. 2014, 46, 3222–3227. [Google Scholar] [CrossRef] [PubMed]
- Nadeem, A.; Salahuddin, N.; El Hazmi, A.; Joseph, M.; Bohlega, B.; Sallam, H.; Sheikh, Y.; Broering, D. Chloride-liberal fluids are associated with acute kidney injury after liver transplantation. Crit. Care. 2014, 18, 625. [Google Scholar] [CrossRef]
- Yi, Z.; Mayorga, M.E.; Orman, E.S.; Wheeler, S.B.; Hayashi, P.H.; Barritt, A.S.T. Trends in Characteristics of Patients Listed for Liver Transplantation Will Lead to Higher Rates of Waitlist Removal Due to Clinical Deterioration. Transplantation 2017, 101, 2368–2374. [Google Scholar] [CrossRef]
- Orman, E.S.; Barritt, A.S.T.; Wheeler, S.B.; Hayashi, P.H. Declining liver utilization for transplantation in the United States and the impact of donation after cardiac death. Liver Transplant. 2013, 19, 59–68. [Google Scholar] [CrossRef]
- Chuang, F.R.; Lin, C.C.; Wang, P.H.; Cheng, Y.F.; Hsu, K.T.; Chen, Y.S.; Lee, C.H.; Chen, C.L. Acute renal failure after cadaveric related liver transplantation. Transplant. Proc. 2004, 36, 2328–2330. [Google Scholar] [CrossRef]
- Cabezuelo, J.B.; Ramirez, P.; Rios, A.; Acosta, F.; Torres, D.; Sansano, T.; Pons, J.A.; Bru, M.; Montoya, M.; Bueno, F.S.; et al. Risk factors of acute renal failure after liver transplantation. Kidney Int. 2006, 69, 1073–1080. [Google Scholar] [CrossRef] [Green Version]
- Rueggeberg, A.; Boehm, S.; Napieralski, F.; Mueller, A.R.; Neuhaus, P.; Falke, K.J.; Gerlach, H. Development of a risk stratification model for predicting acute renal failure in orthotopic liver transplantation recipients. Anaesthesia 2008, 63, 1174–1180. [Google Scholar] [CrossRef]
- Portal, A.J.; McPhail, M.J.; Bruce, M.; Coltart, I.; Slack, A.; Sherwood, R.; Heaton, N.D.; Shawcross, D.; Wendon, J.A.; Heneghan, M.A. Neutrophil gelatinase--associated lipocalin predicts acute kidney injury in patients undergoing liver transplantation. Liver Transplant. 2010, 16, 1257–1266. [Google Scholar] [CrossRef]
- Lee, J.P.; Heo, N.J.; Joo, K.W.; Yi, N.J.; Suh, K.S.; Moon, K.C.; Kim, S.G.; Kim, Y.S. Risk factors for consequent kidney impairment and differential impact of liver transplantation on renal function. Nephrol. Dial. Transplant. 2010, 25, 2772–2785. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ferreira, A.C.; Nolasco, F.; Carvalho, D.; Sampaio, S.; Baptista, A.; Pessegueiro, P.; Monteiro, E.; Mourao, L.; Barroso, E. Impact of RIFLE classification in liver transplantation. Clin. Transplant. 2010, 24, 394–400. [Google Scholar] [CrossRef] [PubMed]
- Tinti, F.; Umbro, I.; Mecule, A.; Rossi, M.; Merli, M.; Nofroni, I.; Corradini, S.G.; Poli, L.; Pugliese, F.; Ruberto, F.; et al. RIFLE criteria and hepatic function in the assessment of acute renal failure in liver transplantation. Transplant. Proc. 2010, 42, 1233–1236. [Google Scholar] [CrossRef] [PubMed]
- Umbro, I.; Tinti, F.; Mordenti, M.; Rossi, M.; Ianni, S.; Pugliese, F.; Ruberto, F.; Ginanni Corradini, S.; Nofroni, I.; Poli, L.; et al. Model for end-stage liver disease score versus simplified acute physiology score criteria in acute renal failure after liver transplantation. Transplant. Proc. 2011, 43, 1139–1141. [Google Scholar] [CrossRef] [PubMed]
- Narciso, R.C.; Ferraz, L.R.; Mies, S.; Monte, J.C.; dos Santos, O.F.; Neto, M.C.; Rodrigues, C.J.; Batista, M.C.; Durao, M.S., Jr. Impact of acute kidney injury exposure period among liver transplantation patients. BMC Nephrol. 2013, 14, 43. [Google Scholar] [CrossRef]
- Kirnap, M.; Colak, T.; Baskin, E.; Akdur, A.; Moray, G.; Arslan, G.; Haberal, M. Acute renal injury in liver transplant patients and its effect on patient survival. Exp. Clin. Transplant. 2014, 12 (Suppl. 1), 156–158. [Google Scholar]
- Lewandowska, L.; Matuszkiewicz-Rowinska, J.; Jayakumar, C.; Oldakowska-Jedynak, U.; Looney, S.; Galas, M.; Dutkiewicz, M.; Krawczyk, M.; Ramesh, G. Netrin-1 and semaphorin 3A predict the development of acute kidney injury in liver transplant patients. PLoS ONE 2014, 9, e107898. [Google Scholar] [CrossRef]
- Barreto, A.G.; Daher, E.F.; Silva Junior, G.B.; Garcia, J.H.; Magalhaes, C.B.; Lima, J.M.; Viana, C.F.; Pereira, E.D. Risk factors for acute kidney injury and 30-day mortality after liver transplantation. Ann. Hepatol. 2015, 14, 688–694. [Google Scholar] [PubMed]
- Park, M.H.; Shim, H.S.; Kim, W.H.; Kim, H.J.; Kim, D.J.; Lee, S.H.; Kim, C.S.; Gwak, M.S.; Kim, G.S. Clinical Risk Scoring Models for Prediction of Acute Kidney Injury after Living Donor Liver Transplantation: A Retrospective Observational Study. PLoS ONE 2015, 10, e0136230. [Google Scholar] [CrossRef] [PubMed]
- Mukhtar, A.; Mahmoud, I.; Obayah, G.; Hasanin, A.; Aboul-Fetouh, F.; Dabous, H.; Bahaa, M.; Abdelaal, A.; Fathy, M.; El Meteini, M. Intraoperative terlipressin therapy reduces the incidence of postoperative acute kidney injury after living donor liver transplantation. J. Cardiothorac. Vasc. Anesth. 2015, 29, 678–683. [Google Scholar] [CrossRef] [PubMed]
- Sang, B.H.; Bang, J.Y.; Song, J.G.; Hwang, G.S. Hypoalbuminemia within Two Postoperative Days Is an Independent Risk Factor for Acute Kidney Injury Following Living Donor Liver Transplantation: A Propensity Score Analysis of 998 Consecutive Patients. Crit. Care Med. 2015, 43, 2552–2561. [Google Scholar] [CrossRef] [PubMed]
- Wyssusek, K.H.; Keys, A.L.; Yung, J.; Moloney, E.T.; Sivalingam, P.; Paul, S.K. Evaluation of perioperative predictors of acute kidney injury post orthotopic liver transplantation. Anaesth. Intensive Care 2015, 43, 757–763. [Google Scholar] [CrossRef] [PubMed]
- Aksu Erdost, H.; Ozkardesler, S.; Ocmen, E.; Avkan-Oguz, V.; Akan, M.; Iyilikci, L.; Unek, T.; Ozbilgin, M.; Meseri Dalak, R.; Astarcioglu, I. Acute Renal Injury Evaluation After Liver Transplantation: With RIFLE Criteria. Transplant. Proc. 2015, 47, 1482–1487. [Google Scholar] [CrossRef]
- Biancofiore, G.; Bindi, M.L.; Miccoli, M.; Cerutti, E.; Lavezzo, B.; Pucci, L.; Bisa, M.; Esposito, M.; Meacci, L.; Mozzo, R.; et al. Intravenous fenoldopam for early acute kidney injury after liver transplantation. J. Anesth. 2015, 29, 426–432. [Google Scholar] [CrossRef]
- Jun, I.G.; Lee, B.; Kim, S.O.; Shin, W.J.; Bang, J.Y.; Song, J.G.; Song, G.W.; Lee, S.G.; Hwang, G.S. Comparison of acute kidney injury between ABO-compatible and ABO-incompatible living donor liver transplantation: A propensity matching analysis. Liver Transplant. 2016, 22, 1656–1665. [Google Scholar] [CrossRef]
- Inoue, Y.; Soyama, A.; Takatsuki, M.; Hidaka, M.; Kinoshita, A.; Natsuda, K.; Baimakhanov, Z.; Kugiyama, T.; Adachi, T.; Kitasato, A.; et al. Does the development of chronic kidney disease and acute kidney injury affect the prognosis after living donor liver transplantation? Clin. Transplant. 2016, 30, 518–527. [Google Scholar] [CrossRef]
- Erdost, H.A.; Ozkardesler, S.; Akan, M.; Iyilikci, L.; Unek, T.; Ocmen, E.; Dalak, R.M.; Astarcioglu, I. Comparison of the RIFLE, AKIN, and KDIGO Diagnostic Classifications for Acute Renal Injury in Patients Undergoing Liver Transplantation. Transplant. Proc. 2016, 48, 2112–2118. [Google Scholar] [CrossRef] [PubMed]
- Kamei, H.; Onishi, Y.; Nakamura, T.; Ishigami, M.; Hamajima, N. Role of cytokine gene polymorphisms in acute and chronic kidney disease following liver transplantation. Hepatol. Int. 2016, 10, 665–672. [Google Scholar] [CrossRef] [PubMed]
- Mizota, T.; Minamisawa, S.; Imanaka, Y.; Fukuda, K. Oliguria without serum creatinine increase after living donor liver transplantation is associated with adverse post-operative outcomes. Acta Anaesthesiol. Scand. 2016, 60, 874–881. [Google Scholar] [CrossRef] [PubMed]
- Chae, M.S.; Lee, N.; Park, D.H.; Lee, J.; Jung, H.S.; Park, C.S.; Choi, J.H.; Hong, S.H. Influence of oxygen content immediately after graft reperfusion on occurrence of postoperative acute kidney injury in living donor liver transplantation. Medicine 2017, 96, e7626. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mizota, T.; Hamada, M.; Matsukawa, S.; Seo, H.; Tanaka, T.; Segawa, H. Relationship Between Intraoperative Hypotension and Acute Kidney Injury After Living Donor Liver Transplantation: A Retrospective Analysis. J. Cardiothorac. Vasc. Anesth. 2017, 31, 582–589. [Google Scholar] [CrossRef]
- Trinh, E.; Alam, A.; Tchervenkov, J.; Cantarovich, M. Impact of acute kidney injury following liver transplantation on long-term outcomes. Clin. Transplant. 2017, 31, e12863. [Google Scholar] [CrossRef] [PubMed]
- Kalisvaart, M.; de Haan, J.E.; Hesselink, D.A.; Polak, W.G.; Hansen, B.E.; JNM, I.J.; Gommers, D.; Metselaar, H.J.; de Jonge, J. The postreperfusion syndrome is associated with acute kidney injury following donation after brain death liver transplantation. Transpl. Int. 2017, 30, 660–669. [Google Scholar] [CrossRef] [PubMed]
- Chen, X.; Ding, X.; Shen, B.; Teng, J.; Zou, J.; Wang, T.; Zhou, J.; Chen, N.; Zhang, B. Incidence and outcomes of acute kidney injury in patients with hepatocellular carcinoma after liver transplantation. J. Cancer Res. Clin. Oncol. 2017, 143, 1337–1346. [Google Scholar] [CrossRef]
- Baron-Stefaniak, J.; Schiefer, J.; Miller, E.J.; Berlakovich, G.A.; Baron, D.M.; Faybik, P. Comparison of macrophage migration inhibitory factor and neutrophil gelatinase-associated lipocalin-2 to predict acute kidney injury after liver transplantation: An observational pilot study. PLoS ONE 2017, 12, e0183162. [Google Scholar] [CrossRef]
- Paramesh, A.S.; Roayaie, S.; Doan, Y.; Schwartz, M.E.; Emre, S.; Fishbein, T.; Florman, S.; Gondolesi, G.E.; Krieger, N.; Ames, S.; et al. Post-liver transplant acute renal failure: Factors predicting development of end-stage renal disease. Clin. Transplant. 2004, 18, 94–99. [Google Scholar] [CrossRef]
- Lima, E.Q.; Zanetta, D.M.; Castro, I.; Massarollo, P.C.; Mies, S.; Machado, M.M.; Yu, L. Risk factors for development of acute renal failure after liver transplantation. Ren. Fail. 2003, 25, 553–560. [Google Scholar] [CrossRef]
- Leithead, J.A.; Armstrong, M.J.; Corbett, C.; Andrew, M.; Kothari, C.; Gunson, B.K.; Mirza, D.; Muiesan, P.; Ferguson, J.W. Split liver transplant recipients do not have an increased frequency of acute kidney injury. Transpl. Int. 2014, 27, 1125–1134. [Google Scholar] [CrossRef]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. PLoS Med. 2009, 6, e1000097. [Google Scholar] [CrossRef] [PubMed]
- Von Elm, E.; Altman, D.G.; Egger, M.; Pocock, S.J.; Gotzsche, P.C.; Vandenbroucke, J.P. The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement: Guidelines for reporting observational studies. PLoS Med. 2007, 4, e296. [Google Scholar] [CrossRef] [PubMed]
- DerSimonian, R.; Laird, N. Meta-analysis in clinical trials. Control. Clin. Trials 1986, 7, 177–188. [Google Scholar] [CrossRef]
- Higgins, J.P.; Thompson, S.G.; Deeks, J.J.; Altman, D.G. Measuring inconsistency in meta-analyses. BMJ 2003, 327, 557–560. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Easterbrook, P.J.; Berlin, J.A.; Gopalan, R.; Matthews, D.R. Publication bias in clinical research. Lancet 1991, 337, 867–872. [Google Scholar] [CrossRef]
- Hand, W.R.; Whiteley, J.R.; Epperson, T.I.; Tam, L.; Crego, H.; Wolf, B.; Chavin, K.D.; Taber, D.J. Hydroxyethyl starch and acute kidney injury in orthotopic liver transplantation: A single-center retrospective review. Anesth. Analg. 2015, 120, 619–626. [Google Scholar] [CrossRef]
- Caragata, R.; Wyssusek, K.H.; Kruger, P. Acute kidney injury following liver transplantation: A systematic review of published predictive models. Anaesth. Intensive Care 2016, 44, 251–261. [Google Scholar] [CrossRef] [PubMed]
- Agarwal, B.; Shaw, S.; Shankar Hari, M.; Burroughs, A.K.; Davenport, A. Continuous renal replacement therapy (CRRT) in patients with liver disease: Is circuit life different? J. Hepatol. 2009, 51, 504–509. [Google Scholar] [CrossRef]
- Asch, W.S.; Bia, M.J. New Organ Allocation System for Combined Liver-Kidney Transplants and the Availability of Kidneys for Transplant to Patients with Stage 4-5 CKD. Clin. J. Am. Soc. Nephrol. 2017, 12, 848–852. [Google Scholar] [CrossRef]
- Ojo, A.O. Renal disease in recipients of nonrenal solid organ transplantation. Semin. Nephrol. 2007, 27, 498–507. [Google Scholar] [CrossRef] [PubMed]
- Biancofiore, G.; Pucci, L.; Cerutti, E.; Penno, G.; Pardini, E.; Esposito, M.; Bindi, L.; Pelati, E.; Romanelli, A.; Triscornia, S.; et al. Cystatin C as a marker of renal function immediately after liver transplantation. Liver Transplant. 2006, 12, 285–291. [Google Scholar] [CrossRef] [Green Version]
- Huen, S.C.; Parikh, C.R. Predicting acute kidney injury after cardiac surgery: A systematic review. Ann. Thorac. Surg. 2012, 93, 337–347. [Google Scholar] [CrossRef] [PubMed]
- Clajus, C.; Hanke, N.; Gottlieb, J.; Stadler, M.; Weismuller, T.J.; Strassburg, C.P.; Brocker, V.; Bara, C.; Lehner, F.; Drube, J.; et al. Renal comorbidity after solid organ and stem cell transplantation. Am. J. Transplant. 2012, 12, 1691–1699. [Google Scholar] [CrossRef]
- Schlegel, A.; Linecker, M.; Kron, P.; Gyori, G.; De Oliveira, M.L.; Mullhaupt, B.; Clavien, P.A.; Dutkowski, P. Risk Assessment in High- and Low-MELD Liver Transplantation. Am. J. Transplant. 2017, 17, 1050–1063. [Google Scholar] [CrossRef] [PubMed]
- Wadei, H.M.; Lee, D.D.; Croome, K.P.; Mai, M.L.; Golan, E.; Brotman, R.; Keaveny, A.P.; Taner, C.B. Early Allograft Dysfunction After Liver Transplantation Is Associated With Short- and Long-Term Kidney Function Impairment. Am. J. Transplant. 2016, 16, 850–859. [Google Scholar] [CrossRef]
- Leithead, J.A.; Tariciotti, L.; Gunson, B.; Holt, A.; Isaac, J.; Mirza, D.F.; Bramhall, S.; Ferguson, J.W.; Muiesan, P. Donation after cardiac death liver transplant recipients have an increased frequency of acute kidney injury. Am. J. Transplant. 2012, 12, 965–975. [Google Scholar] [CrossRef] [PubMed]
- Jo, S.K.; Rosner, M.H.; Okusa, M.D. Pharmacologic treatment of acute kidney injury: Why drugs haven’t worked and what is on the horizon. Clin. J. Am. Soc. Nephrol. 2007, 2, 356–365. [Google Scholar] [CrossRef]
- Valentino, K.L.; Gutierrez, M.; Sanchez, R.; Winship, M.J.; Shapiro, D.A. First clinical trial of a novel caspase inhibitor: Anti-apoptotic caspase inhibitor, IDN-6556, improves liver enzymes. Int. J. Clin. Pharmacol. Ther. 2003, 41, 441–449. [Google Scholar] [CrossRef]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Study | Year | Country | Procedure/Patients | Number | Deceased Donor | AKI Definition | Incidence | Mortality in AKI |
|---|---|---|---|---|---|---|---|---|
| O’riordan et al. [32] | 2007 | Ireland | Deceased donor orthotopic liver transplant | 350 | 350 (100%) | ARI/ARF; RIFLE Injury and Failure stage within 2 weeks after transplant | ARI/ARF 129/350 (36.9%) Dialysis 68/350 (19.4%) | 1-year mortality 56/129 (43%) |
| Kundakci et al. [41] | 2010 | Turkey | Orthotopic liver transplant | 112 | 75 (67%) | AKI; RIFLE criteria | AKI 64/112 (57.1%) | 1-year mortality 23/64 (36%) |
| Portal et al. [55] | 2010 | UK | Liver transplant | 80 | N/A | AKI; AKIN criteria within 48 hours after transplants | AKI 30/80 (37.5%) | N/A |
| Zhu et al. [42] | 2010 | China | Deceased donor orthotopic liver transplant | 193 | 193 (100%) | AKI; AKIN criteria within 28 days after transplants | AKI 116/193 (60.1%) Dialysis 10/193 (5.2%) | 1-year mortality 30/116 (26%) |
| Lee et al. [56] | 2010 | Korea | Liver transplant | 431 | 99 (23%) | AKI; RIFLE criteria | AKI 118/431 (27.4%) Dialysis 14/431 (3.2%) | N/A |
| Ferreira et al. [57] | 2010 | Portugal | Orthotopic liver transplant | 708 | N/A | AKI; RIFLE criteria within 21 days after transplant | AKI 235/708 (33.2%) Dialysis 73/708 (10.3%) | Mortality 43/235 (18%) |
| Tinti et al. [58] | 2010 | Italy | Deceased donor orthotopic liver transplant | 24 | 24 (100%) | AKI; RIFLE criteria within 15 days after transplant | AKI 9/24 (37.5%) | N/A |
| Chen et al. (1) [18] | 2011 | USA | Liver transplant | 334 | N/A | ARI/ARF; RIFLE Injury and Failure stage within 2 weeks after transplant within 7 days after transplant | ARI/ARF 118/334 (38.3%) | Mortality 13/118 (11%) |
| Umbro et al. [59] | 2011 | Italy | Deceased donor liver transplant | 46 | 46 (100%) | AKI; RIFLE criteria within 7 days after transplant | AKI 26/46 (56.5%) | N/A |
| Karapanagiotou et al. (1) [43] | 2012 | Greece | Orthotopic liver transplant | 75 | N/A | AKI; an increase in SCr 1.5 times above baseline or value > 2.0 mg/dL within 7 days after transplant | AKI 22/75 (29.3%) Dialysis 7/75 (9.3%) | 1-year mortality 11/22 (50%) |
| Utsumi et al. [44] | 2013 | Japan | Living donor liver transplant | 200 | 0 (0%) | AKI; RIFLE criteria within 28 days after transplants | AKI 121/200 (60.5%) ARI/ARF 74/200 (37%) | Hospital mortality AKI 14/121 (12%) ARI/ARF 12/74(16%) 1-year mortality AKI 24/121 (20%) ARI/ARF 22/74 (30%) |
| Narciso et al. [60] | 2013 | Brazil | Liver transplant | 315 | 181 (57%) | AKI; AKIN criteria within 48 hours after transplants | AKI 48 hours: 101/315 (32.1%) 1 week: 255/315 (81%) Hospitalization: 293/315 (93%) Dialysis Any: 48/315 (15.2%) 1 week: 31/315 (9.8%) | Dialysis 28/48 (58%) |
| Leithead et al. [39] | 2014 | UK | Liver transplant | 1152 | 1152 (100%) DCD 112 (10%) | AKI; KDIGO criteria within 7 days after transplants | AKI 381/1152 (33.1%) Dialysis 238/1152 (20.7%) | AKI 152/381 (40%) |
| Karapanagiotou et al. (2) [48] | 2014 | Greece | Liver transplant | 71 | N/A | AKI; RIFLE within 7 days or AKIN criteria within 48 hours | RIFLE AKI 28/71 (39.4%) AKIN AKI 37/71 (52.1%) | 6-month mortality RIFLE AKI 15/28 (54%) AKIN AKI 17/37 (46%) |
| Nadeem et al. [49] | 2014 | Saudi Arabia | Liver transplant | 158 | N/A | AKI; RIFLE criteria within 72 hours after transplants | AKI 57/158 (36.1%) | N/A |
| Lewandowska et al. [62] | 2014 | Poland | Orthotopic liver transplant | 63 | N/A | AKI; RIFLE criteria within 72 hours after transplant | AKI 35/63 (55.6%) | N/A |
| Barreto et al. [63] | 2015 | Brazil | Orthotopic liver transplant | 134 | N/A | AKI; AKIN criteria 2 or 3 within 72 hours after transplants | AKIN stage 2 or 3 64/134 (47.8%) Dialysis 33/134 (24.6%) | N/A |
| Hilmi et al. [19] | 2015 | USA | Deceased donor liver transplant | 424 | 424 (100%) EDC 257 (61%) | AKI; KDIGO criteria within 72 hours after transplant | AKI 221/424 (52.1%) | 30-day mortality 3/221 (1%) |
| Park et al. [64] | 2015 | Korea | Living donor liver transplant | 538 | 0 (0%) | AKI; RIFLE criteria within 30 days after transplant | AKI 147/538 (27.3%) Dialysis 34/538 (6.3%) | Hospital mortality 26/147 (18%) 1-year mortality 29/147 (20%) |
| Mukhtar et al. [65] | 2015 | Egypt | Living donor liver transplant | 303 | 0 (0%) | AKI; AKIN criteria within 96 hours after transplant | AKI 115/303 (38%) Dialysis 28/303 (9.2%) | N/A |
| Sang et al. [66] | 2015 | Korea | Living donor liver transplant | 998 | 0 (0%) | AKI; RIFLE or AKIN criteria within 7 days after transplant | RIFLE AKI 709/998 (71.0%) AKIN AKI 593/998 (59.4%) | RIFLE AKI 79/709 (11%) AKIN AKI 66/593 (11%) |
| Biancofiore et al. [69] | 2015 | Italy | Deceased donor liver transplant | 295 | 295 (100%) | AKI; AKIN criteria within 7 days after transplant | AKIN stage 2 AKI 51/295 (17.3%) | N/A |
| Jun et al. [70] | 2016 | Korea | Living donor liver transplant | 1617 | 0 (0%) | AKI; KDIGO criteria within 7 days after transplant | AKI 999/1617 (61.8%) Dialysis 9/448 (2%) | N/A |
| Erdost et al. [72] | 2016 | Turkey | Liver transplant | 440 | 194 (44%) | AKI; RIFLE, AKIN, KDIGO criteria within 7 days after transplant | RIFLE AKI 35/440 (8.0%) AKIN AKI 63/440 (14.3%) KDIGO AKI 64/440 (14.5%) | 30-day mortality RIFLE AKI 8/35 (23%) AKIN AKI 34/63 (54%) KDIGO AKI 35/64 (55%) |
| Kamei et al. [73] | 2016 | Japan | Liver transplant | 62 | DBD 4 (6%) | AKI; RIFLE injury or failure stage within 4 weeks after transplant | AKI 13/62 (21%) Dialysis 4/62 (6.5%) | N/A |
| Mizota et al. (1) [74] | 2016 | Japan | Living donor liver transplant | 320 | 0 (0%) | AKI; KDIGO criteria within 7 days after transplant | AKI 199/320 (62.2%) | Hospital mortality 39/199 (20%) |
| Sun et al. [21] | 2017 | USA | Liver transplant | 1037 | N/A | AKI; AKIN criteria within 48 hours after transplant | AKI 549/1037 (54.9%) | N/A |
| Chae et al. [75] | 2017 | Korea | Living donor liver transplant | 334 | 0 (0%) | AKI; AKIN criteria within 48 hours after transplant | AKI 76/334 (22.7%) | Hospital mortality 10/76 (13.2%) |
| Mizota et al. (2) [76] | 2017 | Japan | Living donor liver transplant | 231 | 0 (0%) | Severe AKI; KDIGO stage 2 or 3 criteria within 7 days after transplant | Severe AKI 71/231 (30.7%) | Hospital mortality 23/71 (32.4%) |
| Trinh et al. [77] | 2017 | Canada | Deceased donor liver transplant | 491 | 491 (100%) | AKI; KDIGO criteria within 7 days after transplant | AKI 278/491 (56.6%) | N/A |
| Kalisvaart et al. [78] | 2017 | Netherlands | Donation after brain death liver transplant | 155 | 155 (100%) DBD 155 (100%) | AKI; AKIN criteria within 7 days after transplant | AKI 61/155 (39.4%) Dialysis 5/155 (3.2%) | Hospital mortality 9/61 (15%) |
| Chen et al. (2) [79] | 2017 | China | Liver transplant in hepatocellular carcinoma | 566 | N/A | AKI; AKIN criteria within 48 hours after transplant | AKI 109/566 (19.3%) Dialysis 13/566 (2.3%) | 30-day mortality 9/109 (8%) |
| Baron-Stefaniak et al. [80] | 2017 | Austria | Orthotopic liver transplant | 45 | N/A | AKI; KDIGO criteria within 48 hours after transplant | AKI 34/45 (75.6) | N/A |
| Zhou et al. [30] | 2017 | China | Donation after circulatory death orthotopic liver transplant | 103 | 103 (100%) DCD 103 (100%) | AKI; KDIGO criteria within 7 days after transplant | AKI 42/103 (40.8%) CRRT 7/103 (6.8%) | N/A |
| Yoo et al. [31] | 2017 | Korea | Liver transplant | 304 | 84 (28%) | AKI; RIFLE criteria within 7 days after transplant | AKI 132/304 (43.4%) | N/A |
| Jochmans [29] | 2017 | Belgium | Orthotopic liver transplant | 80 | 80 (100%) DCD 13 (16%) DBD 67 (84%) | AKI; RIFLE criteria within 5 days after reperfusion | AKI 21/80 (26.3%) Dialysis 4/80 (5%) | 1-year mortality 2/21 (10%) |
| Kandil et al. [28] | 2017 | Egypt | Living donor liver transplant | 50 | 0 (0%) | AKI; AKIN criteria within 48 hours | AKI 23/50 (46%) | N/A |
| Kim et al. [14] | 2018 | Korea | Living donor liver transplant | 583 | 0 (0%) | AKI; KDIGO criteria within 7 days after transplant | AKI 205/583 (35.2%) | N/A |
| Donor and Graft Factors | Recipient Factors | Surgical and Postoperative Factors |
|---|---|---|
| Cold ischemia time [14,35,78], warm ischemic time [35,39,63,64,66] Small-for-size graft/Graft-recipient body weight ratio [40,44,65,66] Deceased donor [20,47] Graft dysfunction [11,53] DCD [39] ABO incompatibility [70] Lower donor BMI [39] Older donor age [39] | Higher MELD score/MELD-Na [23,39,40,41,42,43,44,45,46,47,48,49,64,67,89] APACHE II25 [43,48,55], Preoperative SCr11 [23,24,25,32,33,34,35] Preoperative BUN [23,24] Preoperative renal dysfunction/ARF [40,43,53] Child-Pugh score [19] SOFA [48] Male sex [42], female sex [19,31] Preoperative hepatic encephalopathy [47] Infection [25,48,71] Hypoalbuminemia [18,53,64,66] Preoperative low hemoglobin [14,72] High body weight, BMI [14,19,39,44,64,66,67,75] Pretransplant hypertension [32,54] Preoperative DM [19,44] Alcoholic liver disease [32] Pretransplant hepatitis B and/or C [54,63] Tumor as indication for transplant [47] Elevated lactate [54,63] Elevated plasma NGAL [55] Hyponatremia [39] Pulmonary hypertension [31] | Intra-operative hypotension, low MAP [24,33,34,54,66,79] Inotrope/vasopressor requirement [18,30,32,48,65], dopamine [35], intra-operative need of noradrenaline [33,67] Duration of treatment with dopamine [53] Blood loss [35,44,47,64,70,71], RBC transfusion [14,18,25,33,39,48,54,65,66,72,89] Need of cryoprecipitate [64] Anesthetic/Operation time [30,64,66,70] Post-reperfusion syndrome [20,64,66,78] SvO2 reduction with oliguria [14], Oxygen content 5 min after graft reperfusion [75] Terlipressin (protective) [65] Venovenous bypass (protective) [21] Postoperative ICU days [23,48] Duration of ventilator support [48] Aminoglycoside use [32] Duration of anhepatic phase [41,79] Intra-operative acidosis [41] Intra-operative urine output [14,24,30,33] Overexposure to calcineurin inhibitor [35,44,64] Need of diuretics [46,75] Chloride-liberal fluid received within the 24 h posttransplant [49] Crystalloid administration [14] Use of 6% HES [89] Mean blood glucose during the day of surgery [64], glucose variability [31] Peak AST occurring at 6 h [29] |
| Study | Outcomes | Confounder Adjustment |
|---|---|---|
| Bilbao et al. [11] | Mortality Dialysis: 6.47 (2.73–15.35) Graft failure Dialysis: 4.11 (1.81–9.32) | None |
| Contreras et al. [24] | Hospital mortality Dialysis: 9.91 (3.45–28.51) ICU LOS Dialysis: 15 ± 13 vs. 7 ± 11 days Hospital LOS Dialysis: 34 ± 27 vs. 19 ± 20 days | None |
| Lebrón Gallardo et al. [25] | Mortality Early renal dysfunction: 2.47 (1.29–4.72) Dialysis: 8.80 (3.65–21.23) | None |
| Sanchez et al. [23] | 1-year mortality Dialysis: 9.07 (5.49–14.97) ICU LOS 2.1 ± 3.0 in no dialysis vs. 8.6 ± 11.6 in hemodialysis vs. 10.5 ± 12.8 days in CRRT | None |
| Wyatt et al. [22] | Mortality ARF without RRT: 8.69 (3.25–23.19) ARF with RRT: 12.07 (3.90–37.32) | Age, sex, race, DM, transplant centers |
| Cabezuelo et al. [53] | ICU LOS ARF: 12.9 ± 7.4 vs. 7.2 ± 4.0 days | N/A |
| O’Riordan et al. [32] | 1-year mortality ARF: 2.6 (1.5–4.5) Hospital LOS 39.3 ± 79.5 in no ARI/ARF vs. 53.3 ± 72.8 in ARI vs. 73.0 ± 129.8 days in ARF | DM, pretransplant, SCr, PBC, inotrope use, CMV infection/disease, rejection |
| Lee et al. [40] | Hospital LOS Renal dysfunction: 75 ± 144 vs. 45.2 ± 34.5 days | N/A |
| Rueggeberg et al. [54] | 1-year mortality AKI: 10.93 (3.64–32.83) | None |
| Barri et al. [17] | 2-year mortality AKI: 2.33 (1.53–3.53) 2-year graft failure AKI: 2.56 (1.73–3.78) ICU LOS AKI: 8 ± 19 vs. 3 ± 5 days Hospital LOS AKI: 20 ± 24 vs. 11 ± 10 days | None |
| Kundakci et al. [41] | 1-year mortality AKI: 6.73 (2.15–21.06) | None |
| Zhu et al. [42] | 1-year mortality AKI: 12.1 (1.57–93.54) ICU LOS AKI: 6 (4–9) vs. 4 (3–5) days Hospital LOS AKI: 29 (16–47) vs. 29 (20–48) days | Hypertension, infection and APACHE II |
| Ferreira et al. [57] | Mortality AKI: 0.73 (0.59–1.08) CKD AKI: 4.84 (3.45–6.80) | None |
| Lee et al. [56] | CKD AKI: 1.54 (1.02–2.34) | Age, sex, period of transplant, BMI, pretransplant DM, pretransplant hypertension, history of cardiovascular disease, donor type, underlying liver disease, HBV-related liver disease, hepatocellular carcinoma, use of adefovir, calcineurin inhibitors, purine metabolism inhibitors, acute rejection, pretransplant hemoglobin, pretransplant GFR, pretransplant proteinuria, hepatorenal syndrome, Child-Pugh score, MELD score |
| Chen et al. [18] | 1-year mortality ARI/ARF: 2.79 (0.96–8.12) 1-year graft failure ARI/ARF: 1.91 (0.89–4.09) Hospital LOS 21.8 ± 22.1 in no ARI/ARF vs. 24 ± 25 in ARI and 37 ± 49 days in ARF | None |
| Karapanagiotou et al. [43] | 1-year mortality 9.61 (1.48–62.55) | Infection, hemorrhage, MELD, APACHE score |
| Utsumi et al. [44] | Hospital mortality AKI: 5.04 (1.11–22.81) ARI/ARF: 5.90 (1.83–19.06) 1-year mortality AKI: 9.53 (2.18–41.56) ARI/ARF: 12.90 (4.24–39.30) CKD AKI: 15/107 (14%) vs. 0/77 (0%) ARI/ARF: 35.29 (4.51–275.82) Hospital LOS ARI/ARF: 101.5 ± 68.8 vs. 69.7 ± 48.5 days | None |
| Narciso et al. [60] | Mortality Dialysis: 6.7 (3.49–12.96) | None |
| Romano et al. [45] | Hospital mortality AKI: 1.88 (0.76–4.65) | None |
| Leithead et al. [39] | Mortality 1.71 (1.35–2.17) | Age, sex, MELD score, eGFR, DM |
| Klaus et al. [46] | Mortality AKI: 5.11 (1.39–18.71) Dialysis:14.4 (4.60–45.09) | None |
| Kim et al. [47] | 1-year mortality Dialysis: 56.5 (12.32–259.20) | None |
| Karapanagiotou et al. [48] | 6-month mortality RIFLE: 3.08 (1.09–1.95) AKIN: 9.34 (1.20–15.69) ICU LOS RIFLE: 15.44 ± 15.41 vs. 8.65 ± 12.59 days AKIN: 13.75 ± 14.53 vs. 9.1 ± 13.08 days | Vasopressor use, RBC transfusion |
| Nadeem et al. [49] | ICU LOS AKI: 13.4 ± 19 vs. 5.5 ± 4.7 days | N/A |
| Kirnap et al. [61] | Mortality AKI: 1.85 (0.65–5.23) ICU LOS AKI: 10 ± 8 vs. 3 ± 2 days Hospital LOS AKI: 26 ± 70 vs. 16 ± 7 days | None |
| Barreto et al. [63] | Hospital mortality AKIN stage 2 or 3: 4.3 (1.3–14.6) | None |
| Hilmi et al. [19] | 30-day mortality AKI: 3/221(1.4%) vs. 0/203 (0%) CKD AKI: 1.69 (1.11–2.58) | None |
| Park et al. [64] | Hospital mortality 3.44 (1.89–6.25) 1-year mortality AKI: 1.57 (0.95–2.58) ICU LOS 6 (6–7) in no AKI vs. 6 (6–9) in Risk vs. 7 (6–18) in Injury vs. 11 (10–85) in Failure group Hospital LOS 29 (23–42) in no AKI vs. 31 (21–43) in Risk vs. 33 (26–47) in Injury vs. 46 (16–108) in Failure group | None |
| Mukhtar et al. [65] | Mortality AKI: 2.1 (1.18–4.0) | Graft weight to recipient body weight ratio, baseline creatinine, MELD score, DM, Terlipressin use, massive transfusion, vasopressor use |
| Sang et al. [66] | Mortality RIFLE AKI: 2.29 (1.29–4.05) AKIN AKI: 1.69 (1.06–2.67) | None |
| Wyssusek et al. [67] | Mortality AKI: 3.23 (0.43–24.27) | None |
| Jun et al. [70] | Mortality AKI: 0.36 (0.09–1.43) | ABO incompatibility, MELD score, hypertension, coronary artery disease, age, post-reperfusion syndrome, vasopressor, crystalloid, RBC transfusion, FFP transfusion, operation time, cold ischemic time |
| Inoue et al. [71] | 1-year mortality AKI: 4.54 (1.27–16.32) CKD AKI: 2.33 (0.66–8.29) | None |
| Mizota et al. [74] | Hospital mortality AKI: 2.53 (1.23–5.22) CKD AKI: 2.46 (1.51–4.02) | Age, MELD score, blood type incompatibility, re-transplantation |
| Erdost et al. [72] | 30-day mortality RIFLE AKI: 4.15 (1.72–10.00) AKIN AKI: 440.83 (58.24–3336.87) KDIGO AKI: 35/64 (55%) vs. 0/376 | None |
| Chae et al. [75] | Hospital mortality AKI: 1.63 (0.73–3.60) ICU LOS AKI: 7 (6–8) vs. 7 (5–7) days Hospital LOS AKI: 28 (22–39) vs. 23 (21–31) days | None |
| Mizota et al. [76] | Hospital mortality Severe AKI: 3.56 (1.78–7.09) | None |
| Trinh et al. [77] | Mortality AKI: 1.41 (1.03–1.92) CKD stage 4–5 AKI: 2.39 (1.27–4.47) | Age, sex, MELD score, baseline eGFR, ATG induction, pretransplant hypertension and DM |
| Kalisvaart et al. [78] | Hospital mortality AKI: 7.96 (1.66–38.25) ICU LOS AKI: 3 (2–5) vs. 2 (2–3) days Hospital LOS AKI: 24 (19–35) vs. 17 (14–27) days | None |
| Nadkarni et al. [16] | Hospital mortality Dialysis: 2.00 (1.55–2.59) | Not specified |
| Chen et al. [79] | 30-day mortality AKI: 4.05 (1.02–16.18) | ALP, MELD score, operation time, blood transfusion |
| Zongyi et al. [35] | 1-year mortality RIFLE failure stage AKI: 12.25 (8.99–16.70) 1-year graft failure RIFLE failure stage AKI: 11.73 (8.57–16.06) Hospital LOS RIFLE failure stage AKI: 16 (6–34.5) vs. 25 (18–35) days | None |
| Zhou et al. [30] | 14-day mortality AKI: 3.35 (0.94–11.98) Hospital LOS AKI: 28.13 ± 20.04 vs. 26.16 ± 11.91 days | None |
| Jochmans et al. [29] | 1-year mortality AKI: 6.11 (0.52–71.16) 1-year graft failure AKI: 2.54 (0.61–10.55) CKD AKI:1.17 (0.40–3.44) ICU LOS AKI: 4 (3–9) vs. 2 (2–4) Hospital LOS AKI: 23 (17–46) vs. 16 (13–26) | None |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Thongprayoon, C.; Kaewput, W.; Thamcharoen, N.; Bathini, T.; Watthanasuntorn, K.; Lertjitbanjong, P.; Sharma, K.; Salim, S.A.; Ungprasert, P.; Wijarnpreecha, K.; et al. Incidence and Impact of Acute Kidney Injury after Liver Transplantation: A Meta-Analysis. J. Clin. Med. 2019, 8, 372. https://doi.org/10.3390/jcm8030372
Thongprayoon C, Kaewput W, Thamcharoen N, Bathini T, Watthanasuntorn K, Lertjitbanjong P, Sharma K, Salim SA, Ungprasert P, Wijarnpreecha K, et al. Incidence and Impact of Acute Kidney Injury after Liver Transplantation: A Meta-Analysis. Journal of Clinical Medicine. 2019; 8(3):372. https://doi.org/10.3390/jcm8030372
Chicago/Turabian StyleThongprayoon, Charat, Wisit Kaewput, Natanong Thamcharoen, Tarun Bathini, Kanramon Watthanasuntorn, Ploypin Lertjitbanjong, Konika Sharma, Sohail Abdul Salim, Patompong Ungprasert, Karn Wijarnpreecha, and et al. 2019. "Incidence and Impact of Acute Kidney Injury after Liver Transplantation: A Meta-Analysis" Journal of Clinical Medicine 8, no. 3: 372. https://doi.org/10.3390/jcm8030372