Effect of Diabetes Mellitus on Acute Kidney Injury after Minimally Invasive Partial Nephrectomy: A Case-Matched Retrospective Analysis

Abstract
:1. Introduction
2. Material and Methods
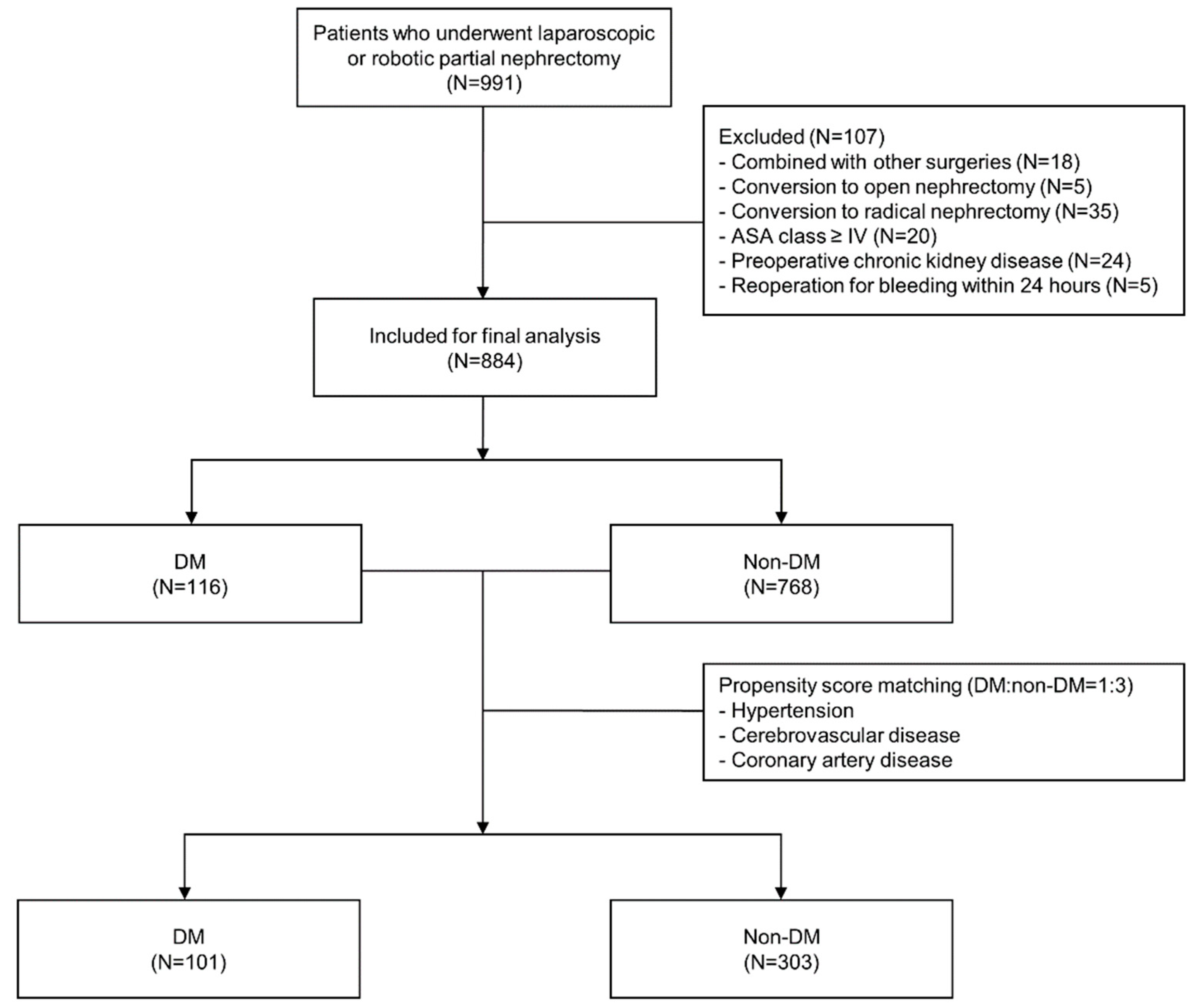
2.1. Patients
2.2. Data Collection
2.3. Primary and Secondary Outcomes
2.4. Statistical Analysis
3. Results
4. Discussion
Author Contributions
Funding
Conflicts of Interest
References
- Lau, W.K.; Blute, M.L.; Weaver, A.L.; Torres, V.E.; Zincke, H. Matched comparison of radical nephrectomy vs nephron-sparing surgery in patients with unilateral renal cell carcinoma and a normal contralateral kidney. Mayo Clin. Proc. 2000, 75, 1236–1242. [Google Scholar] [CrossRef] [PubMed]
- Suer, E.; Burgu, B.; Gokce, M.I.; Turkolmez, K.; Beduk, Y.; Baltaci, S. Comparison of radical and partial nephrectomy in terms of renal function: A retrospective cohort study. Scand. J. Urol. Nephrol. 2011, 45, 24–29. [Google Scholar] [CrossRef]
- Rajan, S.; Babazade, R.; Govindarajan, S.R.; Pal, R.; You, J.; Mascha, E.J.; Khanna, A.; Yang, M.; Marcano, F.D.; Singh, A.K.; et al. Perioperative factors associated with acute kidney injury after partial nephrectomy. Br. J. Anaesth. 2016, 116, 70–76. [Google Scholar] [CrossRef]
- Zhang, Z.; Zhao, J.; Dong, W.; Remer, E.; Li, J.; Demirjian, S.; Zabell, J.; Campbell, S.C. Acute kidney injury after partial nephrectomy: Role of parenchymal mass reduction and ischemia and impact on subsequent functional recovery. Eur. Urol. 2016, 69, 745–752. [Google Scholar] [CrossRef] [PubMed]
- Rosen, D.C.; Kannappan, M.; Paulucci, D.J.; Beksac, A.T.; Attallah, K.; Abaza, R.; Eun, D.D.; Bhandari, A.; Hemal, A.K.; Porter, J.; et al. Reevaluating warm ischemia time as a predictor of renal function outcomes after robotic partial nephrectomy. Urology 2018, 120, 156–161. [Google Scholar] [CrossRef]
- Lee, B.; Lee, S.Y.; Kim, N.Y.; Rha, K.H.; Choi, Y.D.; Park, S.; Kim, S.Y. Effect of ulinastatin on postoperative renal function in patients undergoing robot-assisted laparoscopic partial nephrectomy: A randomized trial. Surg. Endosc. 2017, 31, 3728–3736. [Google Scholar] [CrossRef]
- National Kidney, F. Kdoqi clinical practice guideline for diabetes and ckd: 2012 update. Am. J. Kidney Dis. 2012, 60, 850–886. [Google Scholar]
- Girman, C.J.; Kou, T.D.; Brodovicz, K.; Alexander, C.M.; O’Neill, E.A.; Engel, S.; Williams-Herman, D.E.; Katz, L. Risk of acute renal failure in patients with type 2 diabetes mellitus. Diabet. Med. 2012, 29, 614–621. [Google Scholar] [CrossRef] [PubMed]
- Wang, Y.; Bellomo, R. Cardiac surgery-associated acute kidney injury: Risk factors, pathophysiology and treatment. Nat. Rev. Nephrol. 2017, 13, 697–711. [Google Scholar] [CrossRef]
- Kheterpal, S.; Tremper, K.K.; Heung, M.; Rosenberg, A.L.; Englesbe, M.; Shanks, A.M.; Campbell, D.A., Jr. Development and validation of an acute kidney injury risk index for patients undergoing general surgery: Results from a national data set. Anesthesiology 2009, 110, 505–515. [Google Scholar] [CrossRef] [PubMed]
- Pourafkari, L.; Arora, P.; Porhomayon, J.; Dosluoglu, H.H.; Arora, P.; Nader, N.D. Acute kidney injury after non-cardiovascular surgery: Risk factors and impact on development of chronic kidney disease and long-term mortality. Curr. Med. Res. Opin. 2018, 34, 1829–1837. [Google Scholar] [CrossRef] [PubMed]
- Lane, B.R.; Babineau, D.C.; Poggio, E.D.; Weight, C.J.; Larson, B.T.; Gill, I.S.; Novick, A.C. Factors predicting renal functional outcome after partial nephrectomy. J. Urol. 2008, 180, 2363–2368. [Google Scholar] [CrossRef] [PubMed]
- Volpe, A.; Blute, M.L.; Ficarra, V.; Gill, I.S.; Kutikov, A.; Porpiglia, F.; Rogers, C.; Touijer, K.A.; Van Poppel, H.; Thompson, R.H. Renal ischemia and function after partial nephrectomy: A collaborative review of the literature. Eur. Urol. 2015, 68, 61–74. [Google Scholar] [CrossRef]
- Schmid, M.; Krishna, N.; Ravi, P.; Meyer, C.P.; Becker, A.; Dalela, D.; Sood, A.; Chun, F.K.; Kibel, A.S.; Menon, M.; et al. Trends of acute kidney injury after radical or partial nephrectomy for renal cell carcinoma. Urol. Oncol. 2016, 34, 293.e1–293.e10. [Google Scholar] [CrossRef] [PubMed]
- Schmid, M.; Abd-El-Barr, A.E.; Gandaglia, G.; Sood, A.; Olugbade, K., Jr.; Ruhotina, N.; Sammon, J.D.; Varda, B.; Chang, S.L.; Kibel, A.S.; et al. Predictors of 30-day acute kidney injury following radical and partial nephrectomy for renal cell carcinoma. Urol. Oncol. 2014, 32, 1259–1266. [Google Scholar] [CrossRef]
- Jeong, W.; Park, S.Y.; Lorenzo, E.I.; Oh, C.K.; Han, W.K.; Rha, K.H. Laparoscopic partial nephrectomy versus robot-assisted laparoscopic partial nephrectomy. J Endourol. 2009, 23, 1457–1460. [Google Scholar] [CrossRef] [PubMed]
- Mehta, R.L.; Kellum, J.A.; Shah, S.V.; Molitoris, B.A.; Ronco, C.; Warnock, D.G.; Levin, A. Acute kidney injury network: Report of an initiative to improve outcomes in acute kidney injury. Crit Care. 2007, 11, R31. [Google Scholar] [CrossRef] [PubMed]
- Weight, C.J.; Larson, B.T.; Fergany, A.F.; Gao, T.; Lane, B.R.; Campbell, S.C.; Kaouk, J.H.; Klein, E.A.; Novick, A.C. Nephrectomy induced chronic renal insufficiency is associated with increased risk of cardiovascular death and death from any cause in patients with localized ct1b renal masses. J. Urol. 2010, 183, 1317–1323. [Google Scholar] [CrossRef]
- Cho, A.; Lee, J.E.; Kwon, G.Y.; Huh, W.; Lee, H.M.; Kim, Y.G.; Kim, D.J.; Oh, H.Y.; Choi, H.Y. Post-operative acute kidney injury in patients with renal cell carcinoma is a potent risk factor for new-onset chronic kidney disease after radical nephrectomy. Nephrol. Dial. Transplant. 2011, 26, 3496–3501. [Google Scholar] [CrossRef] [PubMed]
- Zaher Bahouth, E.S.; Nativ, O.; Halachmi, S.; Moskovitz, B.; Abassi, Z.; Nativ, O. Relationship between clinical factors and the occurrence of post-operative acute kidney injury in patients undergoing nephron-sparing surgery. JMCM 2018, 1, 47–50. [Google Scholar]
- Nativ, O.; Bahouth, Z.; Sabo, E.; Halachmi, S.; Moskovitz, B.; Hellou, E.G.; Abassi, Z.; Nativ, O. Method used for tumor bed closure (suture vs. Sealant), ischemia time and duration of surgery are independent predictors of post-nephron sparing surgery acute kidney injury. Urol. Int. 2018, 101, 184–189. [Google Scholar] [CrossRef] [PubMed]
- Nakazawa, J.; Isshiki, K.; Sugimoto, T.; Araki, S.; Kume, S.; Yokomaku, Y.; Chin-Kanasaki, M.; Sakaguchi, M.; Koya, D.; Haneda, M.; et al. Renoprotective effects of asialoerythropoietin in diabetic mice against ischaemia-reperfusion-induced acute kidney injury. Nephrology 2010, 15, 93–101. [Google Scholar] [CrossRef] [PubMed]
- Peng, J.; Li, X.; Zhang, D.; Chen, J.K.; Su, Y.; Smith, S.B.; Dong, Z. Hyperglycemia, p53, and mitochondrial pathway of apoptosis are involved in the susceptibility of diabetic models to ischemic acute kidney injury. Kidney Int. 2015, 87, 137–150. [Google Scholar] [CrossRef] [PubMed]
- Shi, H.; Patschan, D.; Epstein, T.; Goligorsky, M.S.; Winaver, J. Delayed recovery of renal regional blood flow in diabetic mice subjected to acute ischemic kidney injury. Am. J. Physiol. Renal Physiol. 2007, 293, F1512–F1517. [Google Scholar] [CrossRef] [PubMed]
- Funahashi, Y.; Hattori, R.; Yamamoto, T.; Kamihira, O.; Kato, K.; Gotoh, M. Ischemic renal damage after nephron-sparing surgery in patients with normal contralateral kidney. Eur. Urol. 2009, 55, 209–215. [Google Scholar] [CrossRef] [PubMed]
- Porpiglia, F.; Fiori, C.; Bertolo, R.; Angusti, T.; Piccoli, G.B.; Podio, V.; Russo, R. The effects of warm ischaemia time on renal function after laparoscopic partial nephrectomy in patients with normal contralateral kidney. World J. Urol. 2012, 30, 257–263. [Google Scholar] [CrossRef] [PubMed]
- Bell, S.; Dekker, F.W.; Vadiveloo, T.; Marwick, C.; Deshmukh, H.; Donnan, P.T.; Van Diepen, M. Risk of postoperative acute kidney injury in patients undergoing orthopaedic surgery—development and validation of a risk score and effect of acute kidney injury on survival: Observational cohort study. BMJ 2015, 351, h5639. [Google Scholar] [CrossRef]
- Park, K.M.; Kim, J.I.; Ahn, Y.; Bonventre, A.J.; Bonventre, J.V. Testosterone is responsible for enhanced susceptibility of males to ischemic renal injury. J. Biol. Chem. 2004, 279, 52282–52292. [Google Scholar] [CrossRef]
- Muller, V.; Losonczy, G.; Heemann, U.; Vannay, A.; Fekete, A.; Reusz, G.; Tulassay, T.; Szabo, A.J. Sexual dimorphism in renal ischemia-reperfusion injury in rats: Possible role of endothelin. Kidney Int. 2002, 62, 1364–1371. [Google Scholar] [CrossRef]
- Tanaka, R.; Tsutsui, H.; Ohkita, M.; Takaoka, M.; Yukimura, T.; Matsumura, Y. Sex differences in ischemia/reperfusion-induced acute kidney injury are dependent on the renal sympathetic nervous system. Eur. J. Pharmacol. 2013, 714, 397–404. [Google Scholar] [CrossRef]
- Halkos, M.E.; Puskas, J.D.; Lattouf, O.M.; Kilgo, P.; Kerendi, F.; Song, H.K.; Guyton, R.A.; Thourani, V.H. Elevated preoperative hemoglobin a1c level is predictive of adverse events after coronary artery bypass surgery. J. Thorac. Cardiovasc. Surg. 2008, 136, 631–640. [Google Scholar] [CrossRef]
- Morgan, C.J. Reducing bias using propensity score matching. J. Nucl. Cardiol. 2018, 25, 404–406. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variables | Univariate | Multivariate | ||
|---|---|---|---|---|
| OR (95% CI) | P value | OR (95% CI) | P value | |
| Age, year | 0.99 (0.98–1.01) | 0.292 | ||
| Male sex | 3.84 (2.51–5.87) | <0.001 | 4.57 (2.40–8.72) | <0.001 |
| Body mass index, kg/m2 | 1.02 (0.99–1.05) | 0.151 | ||
| ASA physical status | ||||
| I | 1 | |||
| II | 0.95 (0.66–1.36) | 0.772 | ||
| III | 1.39 (0.74–2.63) | 0.309 | ||
| Co-morbidities | ||||
| Diabetes mellitus | 2.56 (1.68–3.92) | <0.001 | 2.85 (1.71–4.74) | <0.001 |
| Hypertension | 1.39 (0.99–1.95) | 0.056 | 1.10 (0.73–1.65) | 0.654 |
| Cerebrovascular disease | 1.19 (0.43–3.27) | 0.738 | ||
| Coronary artery disease | 2.20 (0.92–5.28) | 0.077 | 1.39 (0.52–3.69) | 0.507 |
| Preoperative lab value | ||||
| Creatinine, mg/dL | 7.07 (2.78–18.03) | <0.001 | 0.79 (0.20–3.09) | 0.734 |
| Hematocrit, % | 1.06 (1.02–1.10) | 0.002 | 1.00 (0.95–1.05) | 0.912 |
| Hemoglobin A1c | ||||
| ≤7% | 1 | |||
| >7% | 1.63 (0.76–3.50) | 0.214 | ||
| Type of operation | ||||
| Laparoscopic | 1 | |||
| Robotic | 0.98 (0.67–1.44) | 0.907 | ||
| Operation time, 60 min increase | 1.44 (1.30–1.61) | <0.001 | 1.26 (1.08–1.47) | 0.003 |
| Warm ischemia time | ||||
| ≤25 min | 1 | 1 | ||
| >25 min | 3.25 (2.30–4.58) | <0.001 | 2.81 (1.92–4.10) | <0.001 |
| Intraoperative I & O | ||||
| Fluid input, 500 mL increase | 1.46 (1.30–1.65) | <0.001 | 1.09 (0.91–1.31) | 0.349 |
| Colloid administration | 1.22 (0.88–1.70) | 0.238 | ||
| RBC transfusion | 2.61 (1.28–5.32) | 0.008 | 1.72 (0.71–4.19) | 0.230 |
| Urine output, 100 mL increase | 1.06 (1.02–1.10) | 0.002 | 1.06 (1.02–1.11) | 0.008 |
| Blood loss, 300 mL increase | 1.55 (1.33–1.80) | <0.001 | ||
| Variables | After Case Matching (N = 404) | Before Case Matching (N = 884) | ||||
|---|---|---|---|---|---|---|
| DM (N = 101) | Non–DM (N = 303) | P value | DM (N = 116) | Non–DM (N = 768) | P value | |
| Age, year | 58.7 (9.2) | 58.8 (9.6) | 0.887 | 60.0 (9.8) | 51.5 (12.5) | <0.001 |
| Male sex | 69 (68%) | 182 (60%) | 0.139 | 78 (67%) | 472 (61%) | 0.231 |
| Body mass index, kg/m2 | 26.8 (11.7) | 25.0 (3.2) | 0.131 | 26.6 (11.0) | 24.6 (3.6) | 0.065 |
| ASA physical status | <0.001 | <0.001 | ||||
| I | 0 | 49 (16%) | 0 | 295 (38%) | ||
| II | 91 (90%) | 223 (74%) | 100 (86%) | 427 (56%) | ||
| III | 10 (10%) | 31 (10%) | 16 (14%) | 46 (6%) | ||
| Co-morbidities | ||||||
| DM with oral medication | 98 (97%) | 113 (97%) | ||||
| DM with insulin | 3 (3%) | 3 (3%) | ||||
| Hypertension | 68 (67%) | 206 (68%) | 0.902 | 83 (72%) | 234 (30%) | <0.001 |
| Cerebrovascular disease | 4 (4%) | 13 (4%) | >0.999 | 7 (6%) | 15 (2%) | 0.018 |
| Coronary artery disease | 4 (4%) | 6 (2%) | 0.276 | 8 (7%) | 15 (2%) | 0.006 |
| Preoperative lab value | ||||||
| Creatinine, mg/dL | 0.8 (0.2) | 0.8 (0.2) | 0.821 | 0.8 (0.2) | 0.8 (0.2) | 0.530 |
| Hematocrit, % | 42.2 (5.1) | 42.2 (4.5) | 0.988 | 41.9 (5.1) | 42.4 (4.4) | 0.262 |
| Hemoglobin A1c, % | 7.3 (1.3) | 7.3 (1.4) | ||||
| Type of operation | 0.604 | 0.478 | ||||
| Laparoscopic | 29 (29%) | 79 (26%) | 31 (27%) | 182 (24%) | ||
| Robotic | 72 (71%) | 224 (74%) | 85 (73%) | 586 (76%) | ||
| Operation time, min | 289.5 (78.3) | 287.5 (98.0) | 0.838 | 288.2 (78.2) | 284.9 (91.2) | 0.676 |
| Warm ischemia time | 0.952 | 0.511 | ||||
| ≤25 min | 64 (63%) | 191 (63%) | 72 (62%) | 452 (59%) | ||
| >25 min | 37 (37%) | 112 (37%) | 44 (38%) | 316 (41%) | ||
| Intraoperative I & O | ||||||
| Fluid input, mL | 1793.5 (652.6) | 1845.2 (658.8) | 0.494 | 1812.9 (640.1) | 1853.6 (652.8) | 0.531 |
| Patients administered with colloid, n | 44 (44%) | 125 (41%) | 0.684 | 51 (44%) | 326 (42%) | 0.758 |
| Patients transfused with RBC, n | 7 (7%) | 9 (3%) | 0.135 | 10 (9%) | 24 (3%) | 0.009 |
| Urine output, mL | 583.7 (361.4) | 563.7 (393.7) | 0.652 | 609.6 (442.3) | 593.9 (422.1) | 0.710 |
| Blood loss, mL | 286.4 (337.7) | 254.9 (303.4) | 0.380 | 294.3 (336.8) | 245.0 (288.6) | 0.137 |
| Variables | DM (N = 101) | Non–DM (N = 303) | ||||||
|---|---|---|---|---|---|---|---|---|
| Univariate | Multivariate | Univariate | Multivariate | |||||
| OR (95% CI) | P-value | OR (95% CI) | P-value | OR (95% CI) | P-value | OR (95% CI) | P-value | |
| Age, year | 1.00 (0.96–1.05) | 0.947 | 0.99 (0.96–1.03) | 0.581 | ||||
| Male sex | 10.87 (2.41–49.18) | 0.002 | 19.58 (2.47–155.35) | 0.005 | 4.89 (2.00–11.99) | 0.001 | 4.52 (1.32–15.48) | 0.016 |
| Body mass index, kg/m2 | 0.99 (0.96–1.04) | 0.973 | 1.06 (0.96–1.17) | 0.236 | ||||
| ASA physical status | ||||||||
| I | 1 | |||||||
| II | 1 | 0.51 (0.24–1.12) | 0.093 | |||||
| III | 2.50 (0.67–9.36) | 0.174 | 0.38 (0.10–1.51) | 0.170 | ||||
| Co-morbidities | ||||||||
| Hypertension | 2.03 (0.77–5.35) | 0.154 | 1.10 (0.55–2.22) | 0.787 | ||||
| Cerebrovascular disease | 0.74 (0.07–7.45) | 0.802 | 1.10 (0.24–5.16) | 0.900 | ||||
| Coronary artery disease | 7.39 (0.74–74.13) | 0.089 | 10.41 (0.79–136.42) | 0.074 | 0.45 (0.02 –10.23) | 0.616 | 0.39 (0.02–9.25) | 0.557 |
| Preoperative lab value | ||||||||
| Creatinine, mg/dL | 21.28 (1.36–332.47) | 0.029 | 5.46 (0.14–219.15) | 0.367 | 7.37 (1.26–43.09) | 0.027 | 0.25 (0.02–3.50) | 0.301 |
| Hematocrit, % | 1.08 (0.99–1.18) | 0.090 | 0.94 (0.83–1.08) | 0.391 | 1.09 (1.02–1.18) | 0.017 | 1.04 (0.95–1.13) | 0.418 |
| Hemoglobin A1c | ||||||||
| ≤7% | 1 | |||||||
| >7% | 2.11 (0.89–5.01) | 0.090 | 4.59 (1.47–14.36) | 0.009 | ||||
| Type of operation | ||||||||
| Laparoscopic | 1 | 1 | ||||||
| Robotic | 1.57 (0.59–4.19) | 0.367 | 1.03 (0.49–2.16) | 0.937 | ||||
| Operation time, 60 min increase | 1.35 (0.97–1.88) | 0.077 | 1.24 (0.75–2.05) | 0.408 | 1.45 (1.21–1.74) | <0.001 | 1.18 (0.90–1.56) | 0.235 |
| Warm ischemia time | ||||||||
| ≤25 min | 1 | 1 | 1 | 1 | ||||
| >25 min | 2.49 (1.04–5.94) | 0.040 | 3.57 (1.17–10.94) | 0.026 | 3.09 (1.59–6.01) | 0.001 | 2.56 (1.24–5.26) | 0.011 |
| Intraoperative I & O | ||||||||
| Fluid input, 500 mL increase | 1.31 (0.95–1.81) | 0.101 | 0.93 (0.60–1.44) | 0.752 | 1.63 (1.29–2.05) | <0.001 | 1.21 (0.87–1.68) | 0.251 |
| Colloid administration | 1.33 (0.57–3.10) | 0.516 | 0.92 (0.48–1.78) | 0.805 | ||||
| RBC transfusion | 1.77 (0.37–8.42) | 0.474 | 4.28 (0.40–46.09) | 0.230 | 5.23 (1.35–20.33) | 0.017 | 5.13 (0.96–27.42) | 0.056 |
| Urine output, 100 mL increase | 0.91 (0.80–1.05) | 0.185 | 1.07 (0.99–1.15) | 0.097 | ||||
| Blood loss, 300 mL increase | 1.58 (1.07–2.33) | 0.023 | 1.56 (1.20–2.04) | 0.001 | ||||
| Total patients, n | AKI incidence, n (%) | OR (95% CI) | P value | |
|---|---|---|---|---|
| Non-DM female | 121 | 8 (6.6%) | 1 | |
| DM female | 32 | 2 (6.3%) | 0.95 (0.16–5.59) | 0.958 |
| Non-DM male | 182 | 37 (20.3%) | 4.12 (1.32–12.86) | 0.015 |
| DM male | 69 | 29 (42.0%) | 14.46 (4.62–45.25) | <0.001 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kim, N.Y.; Hong, J.H.; Koh, D.H.; Lee, J.; Nam, H.J.; Kim, S.Y. Effect of Diabetes Mellitus on Acute Kidney Injury after Minimally Invasive Partial Nephrectomy: A Case-Matched Retrospective Analysis. J. Clin. Med. 2019, 8, 468. https://doi.org/10.3390/jcm8040468
Kim NY, Hong JH, Koh DH, Lee J, Nam HJ, Kim SY. Effect of Diabetes Mellitus on Acute Kidney Injury after Minimally Invasive Partial Nephrectomy: A Case-Matched Retrospective Analysis. Journal of Clinical Medicine. 2019; 8(4):468. https://doi.org/10.3390/jcm8040468
Chicago/Turabian StyleKim, Na Young, Jung Hwa Hong, Dong Hoon Koh, Jongsoo Lee, Hoon Jae Nam, and So Yeon Kim. 2019. "Effect of Diabetes Mellitus on Acute Kidney Injury after Minimally Invasive Partial Nephrectomy: A Case-Matched Retrospective Analysis" Journal of Clinical Medicine 8, no. 4: 468. https://doi.org/10.3390/jcm8040468