The Efficacy and Safety of Doripenem in the Treatment of Acute Bacterial Infections—A Systemic Review and Meta-Analysis of Randomized Controlled Trials


Abstract
:1. Introduction
2. Methods
2.1. Study Search and Selection
2.2. Definitions and Outcomes
2.3. Data Analysis
3. Results
3.1. Study Selection and Characteristics
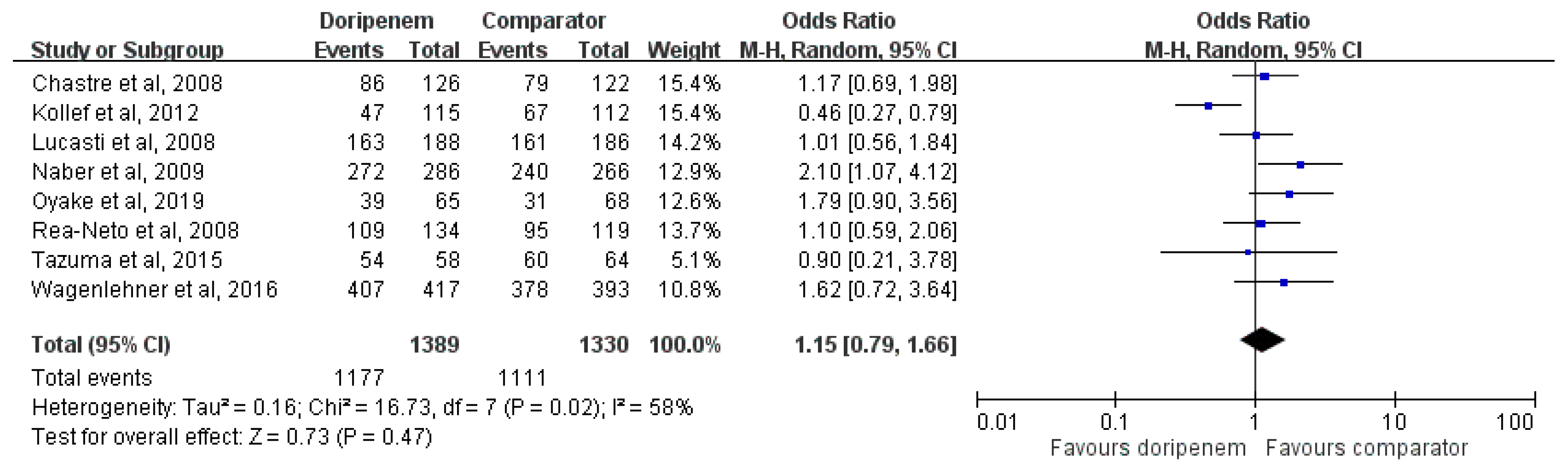
3.2. Clinical Success
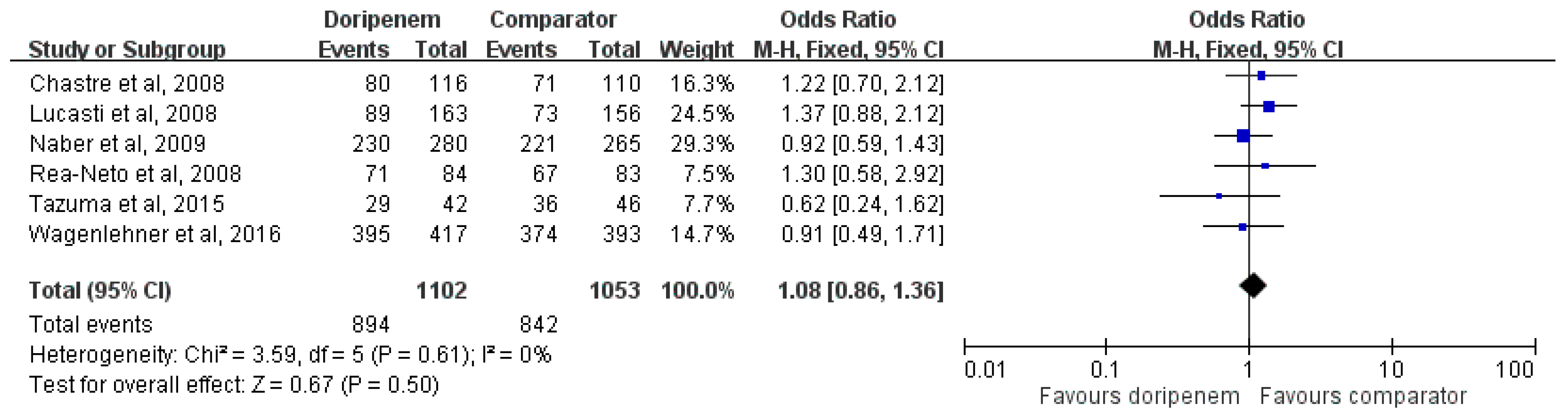
3.3. Microbiological Eradication
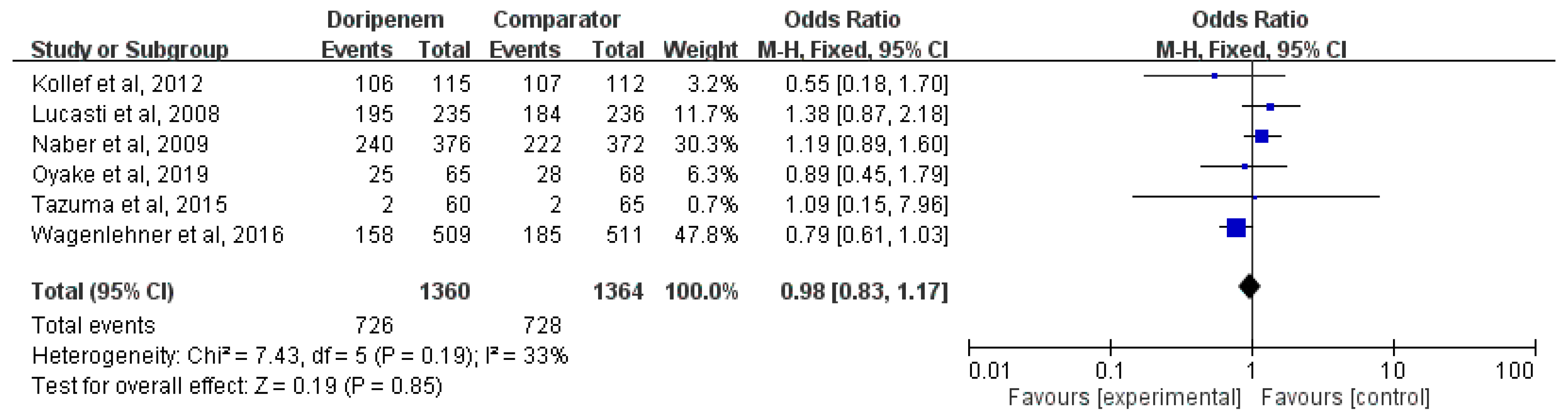
3.4. Adverse Events
4. Discussion
Author Contributions
Conflicts of Interest
Appendix A: List of Terms of the Search Strategy
References
- Kalil, A.C.; Metersky, M.L.; Klompas, M.; Muscedere, J.; Sweeney, D.A.; Palmer, L.B.; Napolitano, L.M.; O’Grady, N.P.; Bartlett, J.G.; Carratalà, J.; et al. Management of adults with hospital-acquired and ventilator-associated pneumonia: 2016 Clinical practice guidelines by the Infectious Diseases Society of America and the American Thoracic Society. Clin. Infect. Dis. 2016, 63, e61–e111. [Google Scholar] [CrossRef] [PubMed]
- Mazzei, T. The pharmacokinetics and pharmacodynamics of the carbapanemes: Focus on doripenem. J. Chemother. 2010, 22, 219–225. [Google Scholar] [CrossRef] [PubMed]
- Castanheira, M.; Jones, R.N.; Livermore, D.M. Antimicrobial activities of doripenem and other carbapenems against Pseudomonas aeruginosa, other nonfermentative bacilli, and Aeromonas spp. Diagn. Microbiol. Infect. Dis. 2009, 63, 426–433. [Google Scholar] [CrossRef] [PubMed]
- Douraghi, M.; Ghalavand, Z.; Nateghi Rostami, M.; Zeraati, H.; Aliramezani, A.; Rahbar, M.; Mohammadzadeh, M.; Ghourchian, S.; Boroumand, M.A.; Abdollahi, A. Comparative in vitro activity of carbapenems against clinical isolates of Acinetobacter baumannii. J. Appl. Microbiol. 2016, 121, 401–407. [Google Scholar] [CrossRef] [PubMed]
- Li, Y.; Lv, Y.; Xue, F.; Zheng, B.; Liu, J.; Zhang, J. Antimicrobial resistance surveillance of doripenem in China. J. Antibiot. Tokyo 2015, 68, 496–500. [Google Scholar] [CrossRef] [PubMed]
- Qu, X.Y.; Hu, T.T.; Zhou, W. A meta-analysis of efficacy and safety of doripenem for treating bacterial infections. Braz. J. Infect. Dis. 2015, 19, 156–162. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wagenlehner, F.M.; Sobel, J.D.; Newell, P.; Armstrong, J.; Huang, X.; Stone, G.G.; Yates, K.; Gasink, L.B. Ceftazidime-avibactam versus doripenem for the treatment of complicated urinary tract infections, including acute pyelonephritis: RECAPTURE, a phase 3 randomized trial program. Clin. Infect. Dis. 2016, 63, 754–762. [Google Scholar] [CrossRef] [PubMed]
- Oyake, T.; Takemasa-Fujisawa, Y.; Sugawara, N.; Mine, T.; Tsukushi, Y.; Hanamura, I.; Fujishima, Y.; Aoki, Y.; Kowata, S.; Ito, S.; et al. Doripenem versus meropenem as first-line empiric therapy of febrile neutropenia in patients with acute leukemia: A prospective, randomized study. Ann. Hematol. 2019, 98, 1209–1216. [Google Scholar] [CrossRef] [PubMed]
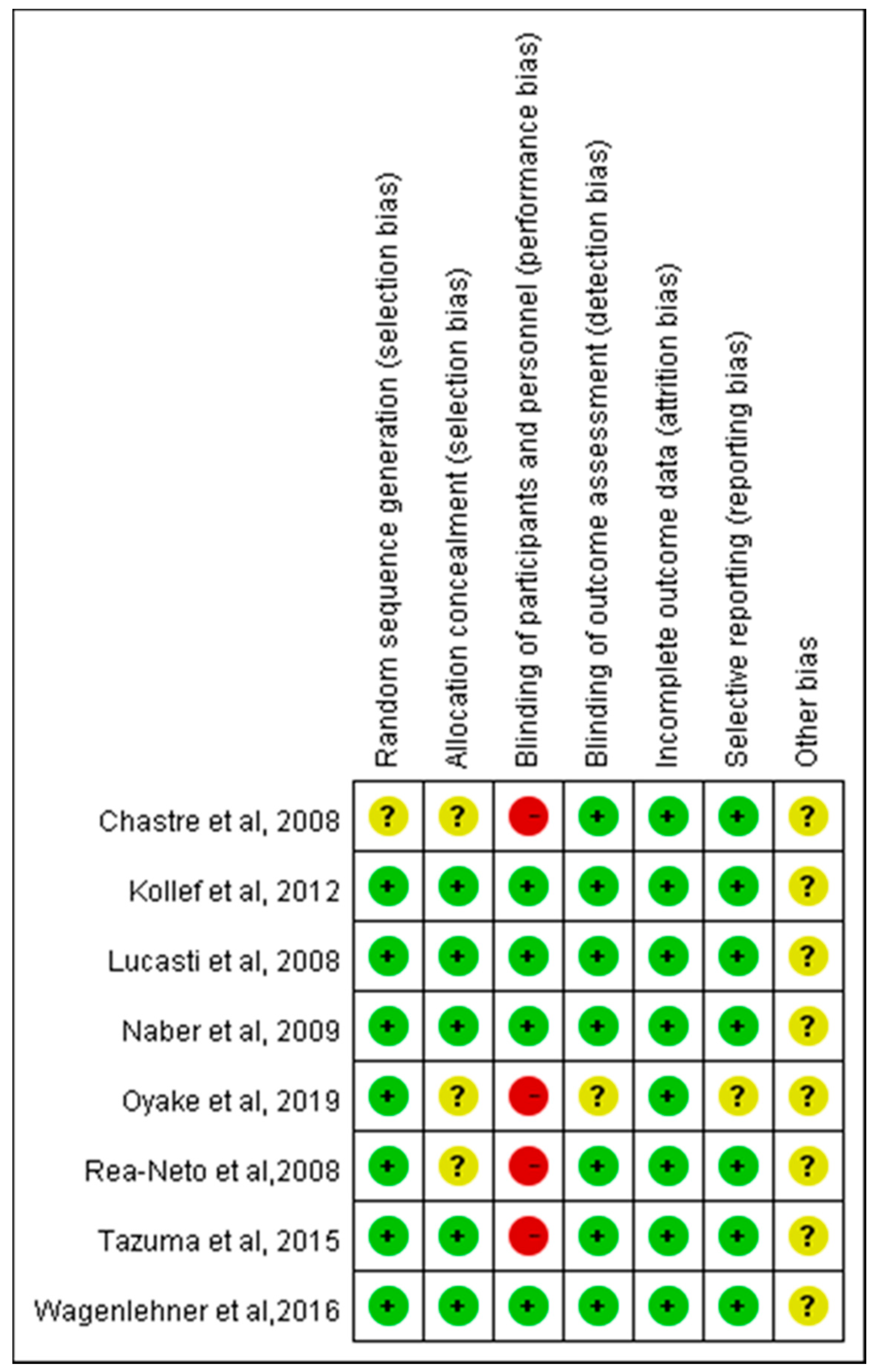
- Higgins, J.P.; Altman, D.G.; Gotzsche, P.C.; Juni, P.; Moher, D.; Oxman, A.D.; Savovic, J.; Schulz, K.F.; Weeks, L.; Sterne, J.A.; et al. The Cochrane Collaboration’s tool for assessing risk of bias in randomised trials. BMJ 2011, 343, d5928. [Google Scholar] [CrossRef]
- Rea-Neto, A.; Niederman, M.; Lobo, S.M.; Schroeder, E.; Lee, M.; Kaniga, K.; Ketter, N.; Prokocimer, P.; Friedland, I. Efficacy and safety of doripenem versus piperacillin/tazobactam in nosocomial pneumonia: A randomized, open-label, multicenter study. Curr. Med. Res. Opin. 2008, 24, 2113–2126. [Google Scholar] [CrossRef] [PubMed]
- Kollef, M.H.; Chastre, J.; Clavel, M.; Restrepo, M.I.; Michiels, B.; Kaniga, K.; Cirillo, I.; Kimko, H.; Redman, R. A randomized trial of 7-day doripenem versus 10-day imipenem-cilastatin for ventilator-associated pneumonia. Crit. Care 2012, 16, R218. [Google Scholar] [CrossRef] [PubMed]
- Chastre, J.; Wunderink, R.; Prokocimer, P.; Lee, M.; Kaniga, K.; Friedland, I. Efficacy and safety of intravenous infusion of doripenem versus imipenem in ventilator-associated pneumonia: A multicenter, randomized study. Crit. Care Med. 2008, 36, 1089–1096. [Google Scholar] [CrossRef] [PubMed]
- Naber, K.G.; Llorens, L.; Kaniga, K.; Kotey, P.; Hedrich, D.; Redman, R. Intravenous doripenem at 500 milligrams versus levofloxacin at 250 milligrams, with an option to switch to oral therapy, for treatment of complicated lower urinary tract infection and pyelonephritis. Antimicrob. Agents Chemother. 2009, 53, 3782–3792. [Google Scholar] [CrossRef] [PubMed]
- Tazuma, S.; Igarashi, Y.; Inui, K.; Ohara, H.; Tsuyuguchi, T.; Ryozawa, S. Clinical efficacy of intravenous doripenem in patients with acute biliary tract infection: A multicenter, randomized, controlled trial with imipenem/cilastatin as comparator. J. Gastroenterol. 2015, 50, 221–229. [Google Scholar] [CrossRef]
- Lucasti, C.; Jasovich, A.; Umeh, O.; Jiang, J.; Kaniga, K.; Friedland, I. Efficacy and tolerability of IV doripenem versus meropenem in adults with complicated intra-abdominal infection: A phase III, prospective, multicenter, randomized, double-blind, noninferiority study. Clin. Ther. 2008, 30, 868–883. [Google Scholar] [CrossRef] [PubMed]
- Kollef, M.H.; Nathwani, D.; Merchant, S.; Gast, C.; Quintana, A.; Ketter, N. Medical resource utilization among patients with ventilator-associated pneumonia: Pooled analysis of randomized studies of doripenem versus comparators. Crit. Care 2010, 14, R84. [Google Scholar] [CrossRef]
- Kongnakorn, T.; Mwamburi, M.; Merchant, S.; Akhras, K.; Caro, J.J.; Nathwani, D. Economic evaluation of doripenem for the treatment of nosocomial pneumonia in the US: Discrete event simulation. Curr. Med. Res. Opin. 2010, 26, 17–24. [Google Scholar] [CrossRef] [PubMed]
- Zilberberg, M.D.; Mody, S.H.; Chen, J.; Shorr, A.F. Cost-effectiveness model of empiric doripenem compared with imipenem-cilastatin in ventilator-associated pneumonia. Surg. Infect. Larchmt 2010, 11, 409–417. [Google Scholar] [CrossRef]
- Drzewiecki, A.; Bulanda, M.; Talaga, K.; Sodo, A.; Adamski, P. Comparison of in vitro activity of doripenem, imipenem and meropenem against clinical isolates of Enterobacteriaceae, Pseudomonas and Acinetobacter in Southern Poland. Pol. Przegl. Chir. 2012, 84, 449–453. [Google Scholar]
- Firsov, A.A.; Gilbert, D.; Greer, K.; Portnoy, Y.A.; Zinner, S.H. Comparative pharmacodynamics and antimutant potentials of doripenem and imipenem with ciprofloxacin-resistant Pseudomonas aeruginosa in an in vitro model. Antimicrob. Agents Chemother. 2012, 56, 1223–1228. [Google Scholar] [CrossRef]
- Wali, N.; Mirza, I.A. Comparative In Vitro Efficacy of doripenem and imipenem against multi-drug resistant Pseudomonas aeruginosa. J. Coll. Physicians Surg. Pak. 2016, 26, 297–301. [Google Scholar] [PubMed]
- Mustafa, M.; Chan, W.M.; Lee, C.; Harijanto, E.; Loo, C.M.; Van Kinh, N.; Anh, N.D.; Garcia, J. A PROspective study on the Usage patterns of Doripenem in the Asia-Pacific region (PROUD study). Int. J. Antimicrob. Agents 2014, 43, 353–360. [Google Scholar] [CrossRef] [PubMed]
- Chao, C.M.; Chen, C.C.; Huang, H.L.; Chuang, Y.C.; Lai, C.C.; Tang, H.J. Clinical experience of patients receiving doripenem-containing regimens for the treatment of healthcare-associated infections. PLoS ONE 2016, 11, e0167522. [Google Scholar] [CrossRef] [PubMed]
- Luyt, C.E.; Aubry, A.; Lu, Q.; Micaelo, M.; Brechot, N.; Brossier, F.; Brisson, H.; Rouby, J.J.; Trouillet, J.L.; Combes, A.; et al. Imipenem, meropenem, or doripenem to treat patients with Pseudomonas aeruginosa ventilator-associated pneumonia. Antimicrob. Agents Chemother. 2014, 58, 1372–1380. [Google Scholar] [CrossRef] [PubMed]
- Muscedere, J.G.; Day, A.; Heyland, D.K. Mortality, attributable mortality, and clinical events as end points for clinical trials of ventilator-associated pneumonia and hospital-acquired pneumonia. Clin. Infect. Dis. 2010, 51 (Suppl. 1), S120–S125. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Reference | RCT Study Design | Duration | Study Population | No. of Patients | Age of the Patients | Dose Regimen | |||
|---|---|---|---|---|---|---|---|---|---|
| Doripenem | Comparator | Doripenem | Comparator | Doripenem | Comparator | ||||
| [10] | Randomized, open-label, multicenter trial | 2004–2006 | Nosocomial pneumonia | 225 | 223 | 57.5 | 59.3 | Doripenem 500 mg every 8 h | Piperacillin/tazobactam 4.5 g every 6 h |
| [15] | Prospective, multicenter, randomized, double-blind | 2004–2006 | Complicated intra-abdominal infection | 237 | 239 | 46.9 | 46.4 | Doripenem 500 mg every 8 h | Meropenem 1.0 g every 8 h |
| [12] | Prospective, multicenter, randomized, open-label trial | 2004–2006 | Ventilator-associated pneumonia | 262 | 263 | 50.7 | 50.3 | Doripenem 500 mg every 8 h | Imipenem/cilastatin 1 g every 8 h or 500 mg every 6 h |
| [13] | Prospective, multicenter, double-blind trial | 2003–2006 | Complicated UTI | 377 | 376 | 51.2 | 51.1 | Doripenem 500 mg every 8 h | Levofloxacin 250 mg everyday |
| [11] | Randomized, double-blind, multicenter trial | 2008–2011 | Ventilator-associated pneumonia | 115 | 112 | 57.5 | 54.6 | Doripenem 1 g every 8 h | Imipenem/cilastatin 1 g every 8 h |
| [14] | Randomized, open-label trial | 2010–2013 | Moderate or severe acute cholangitis or cholecystitis | 62 | 65 | 74 | 73 | Doripenem 500 mg every 8 h | Imipenem/cilastatin 500 mg every 8 h |
| [7] | Randomized, multicenter, double-blind, trials | 2012–2014 | Complicated UTI | 393 | 417 | 53.3 | 51.4 | Doripenem 500 mg every 8 h | Ceftazidime-avibactam 2000 mg/500 mg every 8 h |
| [8] | Randomized, open-label prospective trial | 2011–2013 | Febrile neutropenia in patients with acute leukemia or MDS-refractory anemia with excess blasts | 65 | 68 | 57 | 56 | Doripenem 1 g every 8 h | Meropenem 1.0 g every 8 h |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lai, C.-C.; Cheng, I.-L.; Chen, Y.-H.; Tang, H.-J. The Efficacy and Safety of Doripenem in the Treatment of Acute Bacterial Infections—A Systemic Review and Meta-Analysis of Randomized Controlled Trials. J. Clin. Med. 2019, 8, 958. https://doi.org/10.3390/jcm8070958
Lai C-C, Cheng I-L, Chen Y-H, Tang H-J. The Efficacy and Safety of Doripenem in the Treatment of Acute Bacterial Infections—A Systemic Review and Meta-Analysis of Randomized Controlled Trials. Journal of Clinical Medicine. 2019; 8(7):958. https://doi.org/10.3390/jcm8070958
Chicago/Turabian StyleLai, Chih-Cheng, I-Ling Cheng, Yu-Hung Chen, and Hung-Jen Tang. 2019. "The Efficacy and Safety of Doripenem in the Treatment of Acute Bacterial Infections—A Systemic Review and Meta-Analysis of Randomized Controlled Trials" Journal of Clinical Medicine 8, no. 7: 958. https://doi.org/10.3390/jcm8070958