Risk and Prognostic Factors in Very Old Patients with Sepsis Secondary to Community-Acquired Pneumonia

 ,
,  ,
,  ,
, 
Abstract
1. Introduction
2. Methods
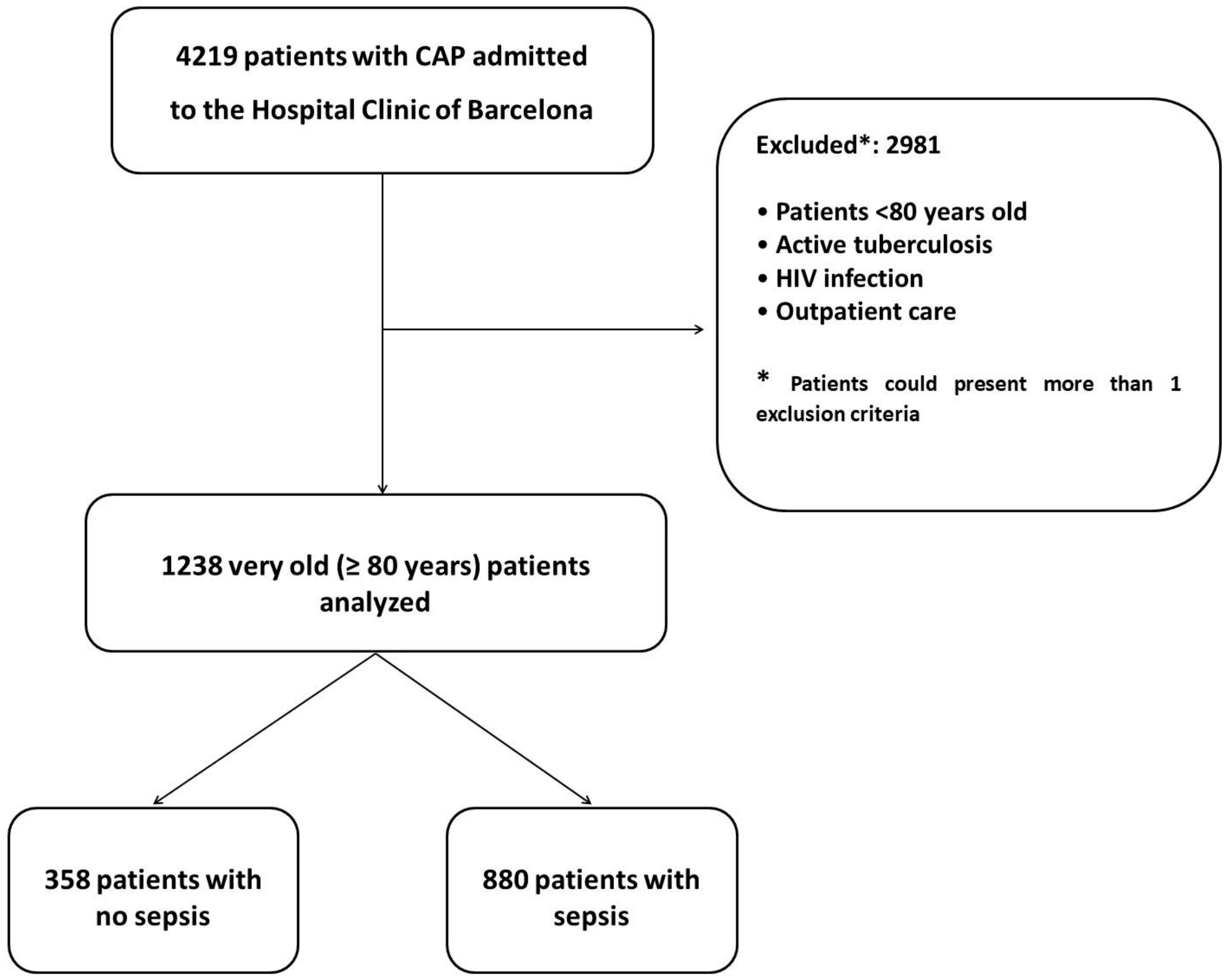
2.1. Study Design and Patients
2.2. Definitions
2.3. Data Collection, Evaluation, and Microbiological Diagnosis
2.4. Outcomes
2.5. Statistical Analysis
3. Results
3.1. Overall Population
3.2. Comparison of Very Old Patients With and Without Sepsis
3.3. Risk Factors for Sepsis
3.4. Outcomes of Very Old Septic and Non-Septic Patients
3.5. Factors Associated with 30-Day Mortality in Patients with Sepsis
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Acknowledgments
Conflicts of Interest
References
- Chalmers, J.; Campling, J.; Ellsbury, G.; Hawkey, P.M.; Madhava, H.; Slack, M. Community-acquired pneumonia in the United Kingdom: A call to action. Pneumonia (Nathan) 2017, 9, 15. [Google Scholar] [CrossRef] [PubMed]
- Cillóniz, C.; Rodríguez-Hurtado, D.; Torres, A. Characteristics and Management of Community-Acquired Pneumonia in the Era of Global Aging. Med. Sci. (Basel) 2018, 6, 35. [Google Scholar] [CrossRef] [PubMed]
- Fernández-Sabé, N.; Carratalà, J.; Rosón, B.; Dorca, J.; Verdaguer, R.; Manresa, F.; Gudiol, F. Community-acquired pneumonia in very elderly patients: Causative organisms, clinical characteristics, and outcomes. Med. (Baltim.) 2003, 82, 159–169. [Google Scholar] [CrossRef] [PubMed]
- World Population Prospects: The 2017 Revision|Multimedia Library-United Nations Department of Economic and Social Affairs. Available online: https://www.un.org/development/desa/publications/world-population-prospects-the-2017-revision.html (accessed on 9 February 2018).
- Flaatten, H.; de Lange, D.W.; Artigas, A.; Bin, D.; Moreno, R.; Christensen, S.; Joynt, G.M.; Bagshaw, S.M.; Sprung, C.L.; Benoit, D.; et al. The status of intensive care medicine research and a future agenda for very old patients in the ICU. Intensiv. Care Med. 2017, 43, 1319–1328. [Google Scholar] [CrossRef] [PubMed]
- Bagshaw, S.M.; Webb, S.A.R.; Delaney, A.; George, C.; Pilcher, D.; Hart, G.K.; Bellomo, R. Very old patients admitted to intensive care in Australia and New Zealand: A multi-centre cohort analysis. Crit. Care 2009, 13, R45. [Google Scholar] [CrossRef] [PubMed]
- Muessig, J.M.; Masyuk, M.; Nia, A.M.; Franz, M.; Kabisch, B.; Kelm, M.; Jung, C. Are we ever too old? Characteristics and outcome of octogenarians admitted to a medical intensive care unit. Med. (Baltim.) 2017, 96, e7776. [Google Scholar] [CrossRef] [PubMed]
- Lerolle, N.; Trinquart, L.; Bornstain, C.; Tadié, J.-M.; Imbert, A.; Diehl, J.-L.; Fagon, J.-Y.; Guérot, E. Increased intensity of treatment and decreased mortality in elderly patients in an intensive care unit over a decade. Crit. Care Med. 2010, 38, 59–64. [Google Scholar] [CrossRef]
- Montull, B.; Menéndez, R.; Torres, A.; Reyes, S.; Méndez, R.; Zalacaín, R.; Capelastegui, A.; Rajas, O.; Borderías, L.; Martin-Villasclaras, J.; et al. Predictors of Severe Sepsis among Patients Hospitalized for Community-Acquired Pneumonia. PLoS ONE 2016, 11, e0145929. [Google Scholar] [CrossRef]
- Singer, M.; Deutschman, C.S.; Seymour, C.W.; Shankar-Hari, M.; Annane, D.; Bauer, M.; Bellomo, R.; Bernard, G.R.; Chiche, J.-D.; Coopersmith, C.M.; et al. The Third International Consensus Definitions for Sepsis and Septic Shock (Sepsis-3). JAMA 2016, 315, 801–810. [Google Scholar] [CrossRef]
- Martin-Loeches, I.; Guia, M.C.; Vallecoccia, M.S.; Suarez, D.; Ibarz, M.; Irazabal, M.; Ferrer, R.; Artigas, A. Risk factors for mortality in elderly and very elderly critically ill patients with sepsis: A prospective, observational, multicenter cohort study. Ann. Intensiv. Care 2019, 9, 26. [Google Scholar] [CrossRef]
- Canaday, D.H.; Jump, R.L.P. Aging has unique effects on the risks, presentation, diagnosis, treatment and prognosis of infectious diseases. Infect. Dis. Clin. N. Am. 2017, 31, xiii–xv. [Google Scholar] [CrossRef]
- Polverino, E.; Torres, A.; Menendez, R.; Cillóniz, C.; Valles, J.M.; Capelastegui, A.; Marcos, M.A.; Alfageme, I.; Zalacain, R.; Almirall, J.; et al. Microbial aetiology of healthcare associated pneumonia in Spain: A prospective, multicentre, case-control study. Thorax 2013, 68, 1007–1014. [Google Scholar] [CrossRef] [PubMed]
- Mandell, L.A.; Wunderink, R.G.; Anzueto, A.; Bartlett, J.G.; Campbell, G.D.; Dean, N.C.; Dowell, S.F.; File, T.M.; Musher, D.M.; Niederman, M.S.; et al. Infectious Diseases Society of America/American Thoracic Society consensus guidelines on the management of community-acquired pneumonia in adults. Clin. Infect. Dis. 2007, 44 (Suppl. 2), S27–S72. [Google Scholar] [CrossRef] [PubMed]
- Torres, A.; Barberán, J.; Falguera, M.; Menéndez, R.; Molina, J.; Olaechea, P.; Rodríguez, A. Grupo de la Guía Multidisciplinar para el Manejo de la Neumonía Adquirida en la Comunidad (Multidisciplinary guidelines for the management of community-acquired pneumonia). Med. Clin. (Barc.) 2013, 140, 223.e1–223.e19. [Google Scholar]
- ARDS Definition Task Force; Ranieri, V.M.; Rubenfeld, G.D.; Thompson, B.T.; Ferguson, N.D.; Caldwell, E.; Fan, E.; Camporota, L.; Slutsky, A.S. Acute respiratory distress syndrome: The Berlin Definition. JAMA 2012, 307, 2526–2533. [Google Scholar] [PubMed]
- Vincent, J.L.; Moreno, R.; Takala, J.; Willatts, S.; De Mendonça, A.; Bruining, H.; Reinhart, C.K.; Suter, P.M.; Thijs, L.G. The SOFA (Sepsis-related Organ Failure Assessment) score to describe organ dysfunction/failure. On behalf of the Working Group on Sepsis-Related Problems of the European Society of Intensive Care Medicine. Intensiv. Care Med. 1996, 22, 707–710. [Google Scholar] [CrossRef]
- Fine, M.J.; Auble, T.E.; Yealy, D.M.; Hanusa, B.H.; Weissfeld, L.A.; Singer, D.E.; Coley, C.M.; Marrie, T.J.; Kapoor, W.N. A prediction rule to identify low-risk patients with community-acquired pneumonia. N. Engl. J. Med. 1997, 336, 243–250. [Google Scholar] [CrossRef]
- Lim, W.S.; van der Eerden, M.M.; Laing, R.; Boersma, W.G.; Karalus, N.; Town, G.I.; Lewis, S.A.; Macfarlane, J.T. Defining community acquired pneumonia severity on presentation to hospital: An international derivation and validation study. Thorax 2003, 58, 377–382. [Google Scholar] [CrossRef]
- Rhodes, A.; Evans, L.E.; Alhazzani, W.; Levy, M.M.; Antonelli, M.; Ferrer, R.; Kumar, A.; Sevransky, J.E.; Sprung, C.L.; Nunnally, M.E.; et al. Surviving Sepsis Campaign: International Guidelines for Management of Sepsis and Septic Shock: 2016. Intensiv. Care Med. 2017, 43, 304–377. [Google Scholar] [CrossRef]
- Bellomo, R.; Ronco, C.; Kellum, J.A.; Mehta, R.L.; Palevsky, P. Acute Dialysis Quality Initiative workgroup Acute renal failure-definition, outcome measures, animal models, fluid therapy and information technology needs: The Second International Consensus Conference of the Acute Dialysis Quality Initiative (ADQI) Group. Crit. Care 2004, 8, R204–R212. [Google Scholar] [CrossRef]
- Cillóniz, C.; Ewig, S.; Polverino, E.; Marcos, M.A.; Esquinas, C.; Gabarrús, A.; Mensa, J.; Torres, A. Microbial aetiology of community-acquired pneumonia and its relation to severity. Thorax 2011, 66, 340–346. [Google Scholar] [CrossRef] [PubMed]
- Cillóniz, C.; Polverino, E.; Ewig, S.; Aliberti, S.; Gabarrús, A.; Menéndez, R.; Mensa, J.; Blasi, F.; Torres, A. Impact of age and comorbidity on cause and outcome in community-acquired pneumonia. Chest 2013, 144, 999–1007. [Google Scholar] [CrossRef]
- Hosmer, D.W.; Lemesshow, S.T.J. Applied logistic regression. D. W. Hosmer and S.; Lemeshow, Wiley, New York, 1989. No. of pages: Xiii + 307. Price: £36.00. Stat. Med. 1991, 10, 1162–1163. [Google Scholar]
- Collett, D. Modelling Binary Data; Chapman and Hall: London, UK, 1991; ISBN 0-412-38800-6. [Google Scholar]
- McCullagh, P.; Nelder, J.A. Generalized Linear Models, 2nd ed.; CRC Press: Boca Raton, FL, USA, 1989; ISBN 978-0-412-31760-6. [Google Scholar]
- Thoemmes, F.; Ong, A.D. A Primer on Inverse Probability of Treatment Weighting and Marginal Structural Models. Emerg. Adulthood 2016, 4, 40–59. [Google Scholar] [CrossRef]
- Brookhart, M.A.; Schneeweiss, S.; Rothman, K.J.; Glynn, R.J.; Avorn, J.; Stürmer, T. Variable selection for propensity score models. Am. J. Epidemiol. 2006, 163, 1149–1156. [Google Scholar] [CrossRef]
- Multivariate Statistical Modelling Based on Generalized Linear Models|Ludwig Fahrmeir|Springer. Available online: https://www.springer.com/us/book/9780387951874 (accessed on 13 November 2018).
- Huang, C.-T.; Chuang, Y.-C.; Tsai, Y.-J.; Ko, W.-J.; Yu, C.-J. High Mortality in Severe Sepsis and Septic Shock Patients with Do-Not-Resuscitate Orders in East Asia. PLoS ONE 2016, 11, e0159501. [Google Scholar] [CrossRef] [PubMed]
- Efron, B.; Tibshirani, R.J. An Introduction to the Bootstrap; CRC Press: Boca Raton, FL, USA, 1994; ISBN 978-0-412-04231-7. [Google Scholar]
- Sterne, J.A.C.; White, I.R.; Carlin, J.B.; Spratt, M.; Royston, P.; Kenward, M.G.; Wood, A.M.; Carpenter, J.R. Multiple imputation for missing data in epidemiological and clinical research: Potential and pitfalls. BMJ 2009, 338, b2393. [Google Scholar] [CrossRef]
- Valencia, M.; Badia, J.R.; Cavalcanti, M.; Ferrer, M.; Agustí, C.; Angrill, J.; García, E.; Mensa, J.; Niederman, M.S.; Torres, A. Pneumonia severity index class v patients with community-acquired pneumonia: Characteristics, outcomes, and value of severity scores. Chest 2007, 132, 515–522. [Google Scholar] [CrossRef]
- Ferrer, M.; Travierso, C.; Cilloniz, C.; Gabarrus, A.; Ranzani, O.T.; Polverino, E.; Liapikou, A.; Blasi, F.; Torres, A. Severe community-acquired pneumonia: Characteristics and prognostic factors in ventilated and non-ventilated patients. PLoS ONE 2018, 13, e0191721. [Google Scholar] [CrossRef]
- Simonetti, A.F.; Viasus, D.; Garcia-Vidal, C.; Carratalà, J. Management of community-acquired pneumonia in older adults. Adv. Infect. Dis. 2014, 2, 3–16. [Google Scholar] [CrossRef]
- Sinapidis, D.; Kosmas, V.; Vittoros, V.; Koutelidakis, I.M.; Pantazi, A.; Stefos, A.; Katsaros, K.E.; Akinosoglou, K.; Bristianou, M.; Toutouzas, K.; et al. Progression into sepsis: An individualized process varying by the interaction of comorbidities with the underlying infection. BMC Infect. Dis. 2018, 18, 242. [Google Scholar] [CrossRef]
- Torres, A.; Peetermans, W.E.; Viegi, G.; Blasi, F. Risk factors for community-acquired pneumonia in adults in Europe: A literature review. Thorax 2013, 68, 1057–1065. [Google Scholar] [CrossRef] [PubMed]
- Ochoa-Gondar, O.; Vila-Córcoles, A.; de Diego, C.; Arija, V.; Maxenchs, M.; Grive, M.; Martin, E.; Pinyol, J.L. EVAN-65 Study Group The burden of community-acquired pneumonia in the elderly: The Spanish EVAN-65 study. BMC Public Health 2008, 8, 222. [Google Scholar] [CrossRef] [PubMed]
- Amaro, R.; Sellarés, J.; Polverino, E.; Cillóniz, C.; Ferrer, M.; Fernández-Barat, L.; Mensa, J.; Niederman, M.S.; Torres, A. Antibiotic therapy prior to hospital admission is associated with reduced septic shock and need for mechanical ventilation in patients with community-acquired pneumonia. J. Infect. 2017, 74, 442–449. [Google Scholar] [CrossRef] [PubMed]
- Filbin, M.R.; Lynch, J.; Gillingham, T.D.; Thorsen, J.E.; Pasakarnis, C.L.; Nepal, S.; Matsushima, M.; Rhee, C.; Heldt, T.; Reisner, A.T. Presenting Symptoms Independently Predict Mortality in Septic Shock: Importance of a Previously Unmeasured Confounder. Crit. Care Med. 2018, 46, 1592–1599. [Google Scholar] [CrossRef] [PubMed]
- Álvaro-Meca, A.; Jiménez-Sousa, M.A.; Micheloud, D.; Sánchez-Lopez, A.; Heredia-Rodríguez, M.; Tamayo, E.; Resino, S. Group of Biomedical Research in Critical Care Medicine (BioCritic) Epidemiological trends of sepsis in the twenty-first century (2000–2013): An analysis of incidence, mortality, and associated costs in Spain. Popul. Health Metr. 2018, 16, 4. [Google Scholar] [CrossRef] [PubMed]
- Angus, D.C.; Linde-Zwirble, W.T.; Lidicker, J.; Clermont, G.; Carcillo, J.; Pinsky, M.R. Epidemiology of severe sepsis in the United States: Analysis of incidence, outcome, and associated costs of care. Crit. Care Med. 2001, 29, 1303–1310. [Google Scholar] [CrossRef] [PubMed]
- Roch, A.; Wiramus, S.; Pauly, V.; Forel, J.-M.; Guervilly, C.; Gainnier, M.; Papazian, L. Long-term outcome in medical patients aged 80 or over following admission to an intensive care unit. Crit. Care 2011, 15, R36. [Google Scholar] [CrossRef] [PubMed]
- Nasa, P.; Juneja, D.; Singh, O. Severe sepsis and septic shock in the elderly: An overview. World J. Crit. Care Med. 2012, 1, 23–30. [Google Scholar]
- Van Vught, L.A.; Scicluna, B.P.; Hoogendijk, A.J.; Wiewel, M.A.; Klein Klouwenberg, P.M.C.; Cremer, O.L.; Horn, J.; Nürnberg, P.; Bonten, M.M.J.; Schultz, M.J.; et al. Association of diabetes and diabetes treatment with the host response in critically ill sepsis patients. Crit. Care 2016, 20, 252. [Google Scholar] [CrossRef]
- Graham, B.B.; Keniston, A.; Gajic, O.; Trillo Alvarez, C.A.; Medvedev, S.; Douglas, I.S. Diabetes mellitus does not adversely affect outcomes from a critical illness. Crit. Care Med. 2010, 38, 16–24. [Google Scholar] [CrossRef]
- Krinsley, J.S. Moving closer to untangling a sweet web: Hyperglycemia, diabetic status, and mortality in the critically ill. Crit. Care Med. 2010, 38, 295–296. [Google Scholar] [CrossRef] [PubMed]
- Walkey, A.J.; Weinberg, J.; Wiener, R.S.; Cooke, C.R.; Lindenauer, P.K. Association of Do-Not-Resuscitate Orders and Hospital Mortality Rate Among Patients with Pneumonia. JAMA Intern. Med. 2016, 176, 97–104. [Google Scholar] [CrossRef] [PubMed][Green Version]


{kind=link}
| Sepsis | |||
|---|---|---|---|
| Variable | No (N = 358) | Yes (N = 880) | P-Value |
| Age, mean (SD), years | 86.6 (5.0) | 85.9 (4.5) | 0.030 |
| Male sex, n (%) | 155 (43) | 531 (60) | <0.001 |
| Current smoker, n (%) | 10 (3) | 45 (5) | 0.081 |
| Current alcohol user, n (%) | 19 (6) | 57 (7) | 0.47 |
| Previous antibiotic in last week, n (%) | 98 (30) | 190 (23) | 0.020 |
| Influenza vaccine, n (%) | 184 (63) | 468 (64) | 0.89 |
| Pneumococcal vaccine, n (%) | 72 (25) | 185 (25) | >0.99 |
| Previous inhaled corticosteroids, n (%) | 62 (18) | 185 (22) | 0.19 |
| Previous systemic corticosteroids, n (%) | 12 (3) | 43 (5) | 0.24 |
| Fever, n (%) | 231 (69) | 569 (66) | 0.72 |
| Pleuritic pain, n (%) | 91 (27) | 177 (21) | 0.021 |
| Dyspnea, n (%) | 261 (76) | 662 (77) | 0.78 |
| Cough, n (%) | 236 (69) | 637 (74) | 0.056 |
| Altered mental status, n (%) | 64 (19) | 295 (34) | 0.001 |
| Prior pneumonia (last year), n (%) | 33 (10) | 131 (16) | 0.011 |
| Comorbidities, n (%) a | 275 (78) | 710 (81) | 0.28 |
| Chronic respiratory disease | 127 (38) | 344 (40) | 0.42 |
| Chronic cardiovascular disease | 67 (19) | 191 (22) | 0.28 |
| Diabetes mellitus | 70 (20) | 241 (28) | 0.007 |
| Neurologic chronic disease | 123 (36) | 266 (31) | 0.085 |
| Chronic renal disease | 22 (6) | 113 (13) | 0.001 |
| Chronic liver disease | 12 (3) | 25 (3) | 0.58 |
| Nursing home resident, n (%) | 71 (20) | 156 (18) | 0.36 |
| Dyspnea, n (%) | 261 (76) | 662 (77) | 0.78 |
| Pleuritic pain, n (%) | 91 (27) | 177 (21) | 0.021 |
| Respiratory rate, median (IQR), breaths/min | 24 (20; 30) | 25 (22; 32) | 0.017 |
| C-reactive protein, median (IQR), mg/dL | 16.2 (8.5; 24.4) | 16.2 (7.4; 25.9) | 0.95 |
| Lymphocytes, median (IQR), cell/mm3 | 1002 (621; 1560) | 888 (510; 1316) | 0.002 |
| Neuthophils, median (IQR), cell/mm3 | 9840 (6708; 14,130) | 10,218 (6596;15,136) | 0.37 |
| PSI score, median (IQR) | 107 (91; 127) | 123.5 (104; 145) | <0.001 |
| PSI risk class IV–V, n (%) b | 77 (78) | 507 (92) | <0.001 |
| Severe CAP, n (%) | 21 (11) | 288 (45) | <0.001 |
| Bacteremia, n (%) c | 19 (9) | 79 (13) | 0.086 |
| Pleural effusion, n (%) | 42 (13) | 110 (13) | 0.90 |
| Multilobar appearance on CXR, n (%) | 74 (21) | 203 (23) | 0.36 |
| Septic shock at admission, n (%) | 0 (0) | 61 (7) | <0.001 |
| Do-not-resuscitate order, n (%) | 59 (18) | 148 (18) | 0.96 |
| Empiric antibiotic therapy, n (%) | - | - | - |
| Monotherapy | 145 (41) | 310 (36) | 0.072 |
| Fluoroquinolones | 91 (26) | 187 (21) | 0.10 |
| β-lactams | 53 (15) | 120 (14) | 0.57 |
| Other therapy | 1 (0.3) | 3 (0.3) | >0.99 |
| Combination therapies | 208 (59) | 561 (64) | 0.072 |
| β-lactams plus macrolides | 105 (30) | 255 (29) | 0.87 |
| β-lactams plus fluoroquinolones | 70 (20) | 227 (26) | 0.021 |
| Other combination therapies | 33 (9) | 79 (9) | 0.88 |
| Appropriate empiric treatment, n (%) | 339 (97) | 817 (96) | 0.57 |
| Univariate a | Multivariable b,c | |||||
|---|---|---|---|---|---|---|
| Variable | OR | 95% CI | P-Value | OR | 95% CI | P-Value |
| Male sex | 1.97 | 1.54 to 2.53 | <0.001 | 1.87 | 1.46 to 2.41 | <0.001 |
| Smoking status d | - | - | <0.001 | - | - | - |
| Never smoker | 1.00 | - | - | - | - | - |
| Current smoker | 2.00 | 1.02 to 3.94 | 0.044 | - | - | - |
| Ex-smoker | 1.58 | 1.21 to 2.06 | 0.001 | - | - | - |
| Previous antibiotic in last week | 0.70 | 0.53 to 0.92 | 0.010 | 0.71 | 0.54 to 0.94 | 0.016 |
| Chronic renal disease | 2.30 | 1.43 to 3.69 | 0.001 | 2.08 | 1.29 to 3.37 | 0.003 |
| Diabetes mellitus | 1.52 | 1.13 to 2.04 | 0.006 | 1.42 | 1.05 to 1.92 | 0.024 |
| Neurological chronic disease | 0.79 | 0.61 to 1.02 | 0.074 | - | - | - |
| Sepsis | |||
|---|---|---|---|
| Variable | No (N = 358) | Yes (N = 880) | P-Value |
| Length of hospital stay, median (IQR), days | 7 (6; 11) | 8 (6; 13) | 0.005 |
| In-hospital mortality, n (%) | 32 (9) | 129 (15) | 0.006 |
| 30-day mortality, n (%) | 40 (11) | 134 (15) | 0.062 |
| One-year mortality, n (%) | 56 (16) | 190 (22) | 0.013 |
| ICU admission, n (%) | 17 (5) | 119 (14) | <0.001 |
| ICU mortality, n (%) a | 1 (6) | 20 (17) | 0.47 |
| Mechanical ventilation, n (%) b | - | - | <0.001 |
| Not ventilated | 237 (99) | 582 (89) | <0.001 |
| Non-invasive | 1 (0.4) | 38 (6) | <0.001 |
| Invasive | 2 (1) | 34 (5) | 0.003 |
| Univariate a | Multivariable b | |||||
|---|---|---|---|---|---|---|
| Variable | OR | 95% CI | P-Value | OR | 95% CI | P-Value |
| Chronic renal disease | 2.60 | 1.40 to 4.83 | 0.003 | 2.57 | 1.35 to 4.89 | 0.004 |
| Diabetes mellitus | 0.49 | 0.22 to 0.88 | 0.021 | 0.44 | 0.21 to 0.89 | 0.023 |
| Neurologic chronic disease | 2.68 | 1.60 to 4.50 | <0.001 | 2.80 | 1.62 to 4.85 | <0.001 |
| Nursing home | 2.19 | 1.21 to 3.94 | <0.001 | - | - | - |
| PSI risk class IV–V | 4.09 | 0.98 to 17.0 | 0.054 | - | - | - |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cillóniz, C.; Dominedò, C.; Ielpo, A.; Ferrer, M.; Gabarrús, A.; Battaglini, D.; Bermejo-Martin, J.; Meli, A.; García-Vidal, C.; Liapikou, A.; et al. Risk and Prognostic Factors in Very Old Patients with Sepsis Secondary to Community-Acquired Pneumonia. J. Clin. Med. 2019, 8, 961. https://doi.org/10.3390/jcm8070961
Cillóniz C, Dominedò C, Ielpo A, Ferrer M, Gabarrús A, Battaglini D, Bermejo-Martin J, Meli A, García-Vidal C, Liapikou A, et al. Risk and Prognostic Factors in Very Old Patients with Sepsis Secondary to Community-Acquired Pneumonia. Journal of Clinical Medicine. 2019; 8(7):961. https://doi.org/10.3390/jcm8070961
Chicago/Turabian StyleCillóniz, Catia, Cristina Dominedò, Antonella Ielpo, Miquel Ferrer, Albert Gabarrús, Denise Battaglini, Jesús Bermejo-Martin, Andrea Meli, Carolina García-Vidal, Adamanthia Liapikou, and et al. 2019. "Risk and Prognostic Factors in Very Old Patients with Sepsis Secondary to Community-Acquired Pneumonia" Journal of Clinical Medicine 8, no. 7: 961. https://doi.org/10.3390/jcm8070961
APA StyleCillóniz, C., Dominedò, C., Ielpo, A., Ferrer, M., Gabarrús, A., Battaglini, D., Bermejo-Martin, J., Meli, A., García-Vidal, C., Liapikou, A., Singer, M., & Torres, A. (2019). Risk and Prognostic Factors in Very Old Patients with Sepsis Secondary to Community-Acquired Pneumonia. Journal of Clinical Medicine, 8(7), 961. https://doi.org/10.3390/jcm8070961