Postprandial Hypotension as a Risk Factor for the Development of New Cardiovascular Disease: A Prospective Cohort Study with 36 Month Follow-Up in Community-Dwelling Elderly People


Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Participants
2.2. Evaluation of PPH and Acquisition of Demographic Data
2.3. Surveillance of CVD Development
2.4. Statistical Analysis
3. Results
3.1. Baseline Characteristics
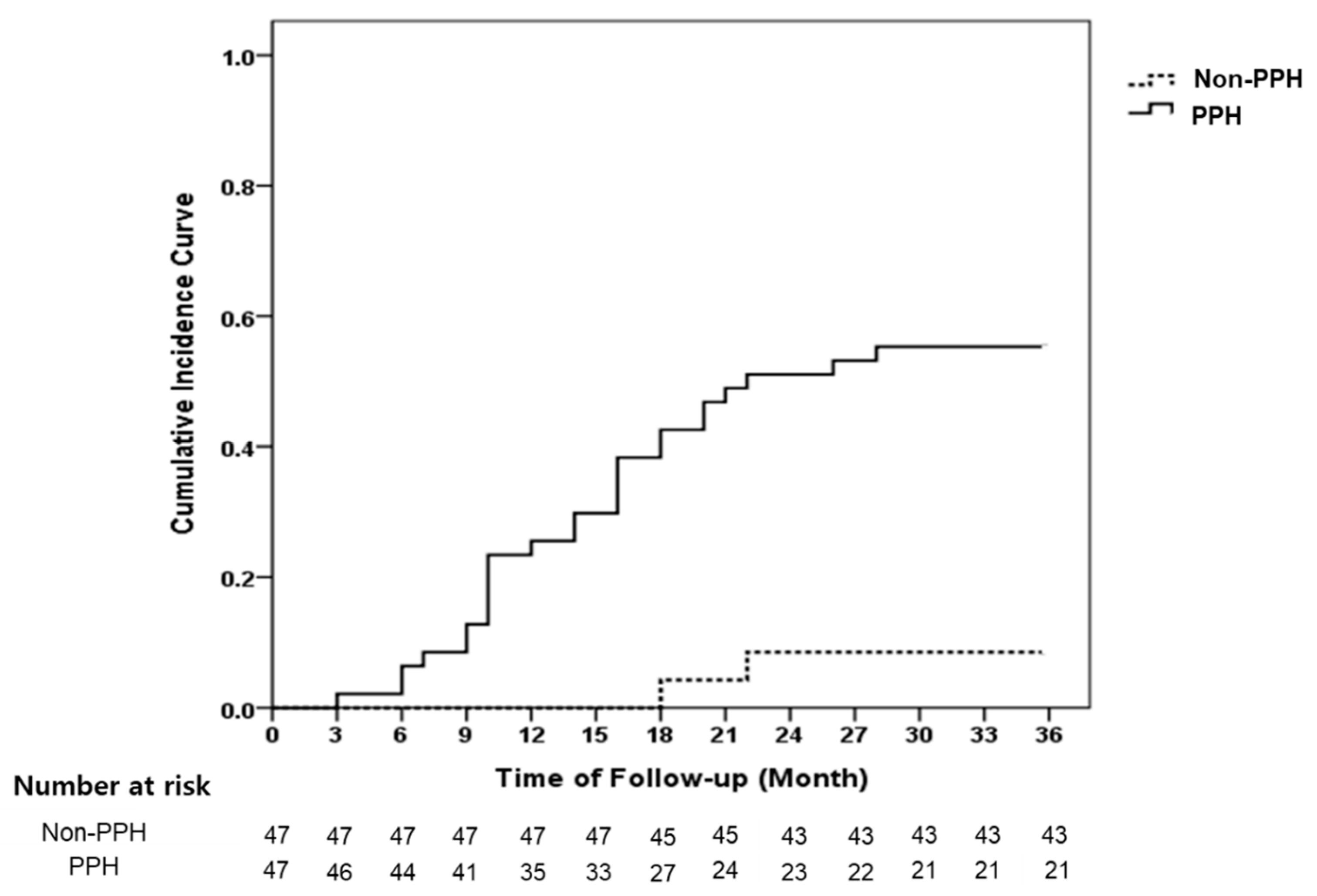
3.2. Incidence of CVD
3.3. Predictive Factors for the Development of New CVD
4. Discussion
5. Conclusions
Funding
Conflicts of Interest
References
- Luciano, G.L.; Brennan, M.J.; Rothberg, M.B. Postprandial hypotension. Am. J. Med. 2010, 123, e1–e6. [Google Scholar] [CrossRef] [PubMed]
- Jansen, R.W.; Lipsitz, L.A. Postprandial hypotension: Epidemiology, pathophysiology, and clinical management. Ann. Intern. Med. 1995, 122, 286–295. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Aronow, W.S.; Ahn, C. Postprandial hypotension in 499 elderly persons in a long-term health care facility. J. Am. Geriatr. Soc. 1994, 42, 930–932. [Google Scholar] [CrossRef] [PubMed]
- Le Couteur, D.G.; Fisher, A.A.; Davis, M.W.; McLean, A.J. Postprandial systolic blood pressure responses of older people in residential care: Association with risk of falling. Gerontology 2003, 49, 260–264. [Google Scholar] [CrossRef] [PubMed]
- Van Orshoven, N.P.; Jansen, P.A.; Oudejans, I.; Schoon, Y.; Oey, P.L. Postprandial hypotension in clinical geriatric patients and healthy elderly: Prevalence related to patient selection and diagnostic criteria. J. Aging Res. 2010, 2010, 243752. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Puisieux, F.; Bulckaen, H.; Fauchais, A.L.; Drumez, S.; Salomez-Granier, F.; Dewailly, P. Ambulatory blood pressure monitoring and postprandial hypotension in elderly persons with falls or syncopes. J. Gerontol. A Biol. Sci. Med. Sci. 2000, 55, M535–M540. [Google Scholar] [CrossRef] [Green Version]
- Lipsitz, L.A.; Ryan, S.M.; Parker, J.A.; Freeman, R.; Wei, J.Y.; Goldberger, A.L. Hemodynamic and autonomic nervous system responses to mixed meal ingestion in healthy young and old subjects and dysautonomic patients with postprandial hypotension. Circulation 1993, 87, 391–400. [Google Scholar] [CrossRef] [Green Version]
- Jang, A.L.; Hwang, S.K.; Kim, D.U. Effects of guar gum ingestion on postprandial blood pressure in older adults. J. Nutr. Health. Aging. 2015, 19, 299–304. [Google Scholar] [CrossRef]
- Fisher, A.A.; Davis, M.W.; Srikusalanukul, W.; Budge, M.M. Postprandial hypotension predicts all-cause mortality in older, low-level care residents. J. Am. Geriatr. Soc. 2005, 53, 1313–1320. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization (WHO). The Top 10 Causes of Death. Available online: https://www.who.int/news-room/fact-sheets/detail/the-top-10-causes-of-death (accessed on 10 September 2019).
- Virtanen, M.; Lallukka, T.; Ervasti, J.; Rahkonen, O.; Lahelma, E.; Pentti, J.; Pietiläinen, O.; Vahtera, J.; Kivimäki, M. The joint contribution of cardiovascular disease and socioeconomic status to disability retirement: A register linkage study. Int. J. Cardiol. 2017, 230, 222–227. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Trahair, L.G.; Horowitz, M.; Jones, K.L. Postprandial hypotension: A systematic review. J. Am. Med. Dir. Assoc. 2014, 15, 394–409. [Google Scholar] [CrossRef] [PubMed]
- Zanasi, A.; Tincani, E.; Evandri, V.; Giovanardi, P.; Bertolotti, M.; Rioli, G. Meal-induced blood pressure variation and cardiovascular mortality in ambulatory hypertensive elderly patients: Preliminary results. J. Hypertens. 2012, 30, 2125–2132. [Google Scholar] [CrossRef] [PubMed]
- Aronow, W.S.; Ahn, C. Association of postprandial hypotension with incidence of falls, syncope, coronary events, stroke, and total mortality at 29-month follow-up in 499 older nursing home residents. J. Am. Geriatr. Soc. 1997, 45, 1051–1053. [Google Scholar] [CrossRef] [PubMed]
- Tabara, Y.; Okada, Y.; Uetani, E.; Nagai, T.; Igase, M.; Kido, T.; Ochi, N.; Ohara, M.; Takita, R.; Kohara, K.; et al. Postprandial hypotension as a risk marker for asymptomatic lacunar infarction. J. Hypertens. 2014, 32, 1084–1090. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kohara, K.; Jiang, Y.; Igase, M.; Takata, Y.; Fukuoka, T.; Okura, T.; Kitami, Y.; Hiwada, K. Postprandial hypotension is associated with asymptomatic cerebrovascular damage in essential hypotensive patients. Hypertension 1999, 33, 565–568. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mancia, G.; Grassi, G. The new European society of hypertension/European society of cardiology (ESH/ESC) guidelines. Ther. Adv. Cardiovasc. Dis. 2008, 2, 5–12. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- World Health Organization (WHO). Cardiovascular Diseases (CVDs). Available online: https://www.who.int/news-room/fact-sheets/detail/cardiovascular-diseases-(cvds) (accessed on 15 September 2019).
- Peitzman, S.J.; Berger, S.R. Postprandial blood pressure decrease in well elderly persons. Arch. Intern. Med. 1989, 149, 286–288. [Google Scholar] [CrossRef] [PubMed]
- Gentilcore, D.; Hausken, T.; Meyer, J.H.; Chapman, I.M.; Horowitz, M.; Jones, K.L. Effects of intraduodenal glucose, fat, and protein on blood pressure, heart rate, and splanchnic blood flow in healthy older subjects. Am. J. Clin. Nutr. 2008, 87, 156–161. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Son, J.T.; Lee, E. Prevalence and risk factors of postprandial hypotension in Korean elderly people. J. Korean Acad. Nurs. 2009, 39, 198–206. [Google Scholar] [CrossRef]


{kind=link}
| Characteristics | Total (n = 94) | PPH (n = 47) | Non-PPH (n = 47) | p-Value |
|---|---|---|---|---|
| Age (years) | 73.1 ± 4.8 | 73.6 ± 4.4 | 72.7 ± 5.1 | 0.355 1 |
| Sex | 0.778 3 | |||
| Male | 15 (16.0) | 8 (17.0) | 7 (14.9) | |
| Female | 79 (84.0) | 39 (83.0) | 40 (85.1) | |
| Body Mass Index (kg/m2) | 23.7 ± 2.5 | 23.8 ± 2.7 | 23.5 ± 2.4 | 0.642 2 |
| Education Level | 0.509 3 | |||
| Elementary School | 67 (71.3) | 36 (76.6) | 31 (66.0) | |
| Middle School | 13 (13.8) | 5 (10.6) | 8 (17.0) | |
| High School | 14 (14.9) | 6 (12.8) | 8 (17.0) | |
| Living Status | 1.000 3 | |||
| Living Alone | 32 (34.0) | 16 (34.0) | 16 (34.0) | |
| With Family or Spouse | 62 (66.0) | 31 (66.0) | 31 (66.0) | |
| Alcohol Drinking | 0.370 3 | |||
| Yes | 13 (13.8) | 5 (10.6) | 8 (17.0) | |
| No | 81 (86.2) | 42 (89.4) | 39 (83.0) | |
| Smoking | 1.000 4 | |||
| Yes | 4 (4.3) | 2 (4.3) | 2 (4.3) | |
| No | 90 (95.7) | 45 (95.7) | 45 (95.7) | |
| Hypertension | 47 (50.0) | 26 (55.3) | 21 (44.7) | 0.302 3 |
| Diabetes Mellitus | 18 (19.1) | 11 (23.4) | 7 (14.9) | 0.294 3 |
| Baseline SBP (mmHg) | 128.6 ± 20.2 | 140.1 ± 17.2 | 117.1 ± 16.1 | <0.001 2 |
| <120 | 34 (36.2) | 6 (12.8) | 28 (59.6) | <0.001 3 |
| ≥120 to <140 | 31 (33.0) | 15 (31.9) | 16 (34.0) | |
| ≥140 | 29 (30.9) | 26 (55.3) | 3 (6.4) | |
| Baseline DBP (mmHg) | 75.2 ± 9.9 | 78.7 ± 7.5 | 71.7 ± 10.9 | <0.001 2 |
| <80 | 64 (68.1) | 23 (48.9) | 41 (87.2) | <0.001 3 |
| ≥80 | 30 (31.9) | 24 (51.1) | 6 (12.8) | |
| Postprandial SBP Change (mmHg) | <0.001 3 | |||
| <10 | 26 (27.7) | 0 (0.0) | 26 (55.3) | |
| ≥10 to <20 | 21 (22.3) | 0 (0.0) | 21 (44.7) | |
| ≥20 | 47 (50.0) | 47 (100.0) | 0 (0.0) | |
| Postprandial DBP Change (mmHg) | <0.001 3 | |||
| <10 | 41 (43.6) | 9 (19.1) | 32 (68.1) | |
| ≥10 | 53 (56.4) | 38 (80.9) | 15 (31.9) |
| Total (n = 94) | CVD (n = 30) | Non-CVD (n = 64) | p-Value | |
|---|---|---|---|---|
| PPH | <0.001 3 | |||
| Yes | 47 (50.0) | 26 (86.7) | 21 (32.8) | |
| No | 47 (50.0) | 4 (13.3) | 43 (67.2) | |
| Age (years) | 73.1 ± 4.8 | 73.0 ± 4.1 | 73.2 ± 5.1 | 0.849 1 |
| Sex | 1.000 4 | |||
| Male | 15 (16.0) | 5 (16.7) | 10 (15.6) | |
| Female | 79 (84.0) | 25 (83.3) | 54 (84.4) | |
| Body mass index (kg/m2) | 23.7 ± 2.5 | 24.5 ± 2.1 | 23.3 ± 2.7 | 0.013 2 |
| Education level | 0.534 4 | |||
| Elementary school | 67 (71.3) | 24 (80.0) | 43 (67.2) | |
| Middle school | 13 (13.8) | 3 (10.0) | 10 (15.6) | |
| High school | 14 (14.9) | 3 (10.0) | 11 (17.2) | |
| Living status | 0.571 3 | |||
| Living alone | 32 (34.0) | 9 (30.0) | 23 (35.9) | |
| With family or spouse | 62 (66.0) | 21 (70.0) | 41 (64.1) | |
| Alcohol drinking | 0.336 4 | |||
| Yes | 13 (13.8) | 6 (20.0) | 7 (10.9) | |
| No | 81 (86.2) | 24 (80.0) | 57 (89.1) | |
| Smoking | 0.590 4 | |||
| Yes | 4 (4.3) | 2 (6.7) | 2 (3.1) | |
| No | 90 (95.7) | 28 (93.3) | 62 (96.9) | |
| Hypertension | 47 (50.0) | 20 (66.7) | 27 (42.2) | 0.027 3 |
| Diabetes mellitus | 18 (19.1) | 9(30.0) | 9 (14.1) | 0.067 3 |
| Baseline SBP (mmHg) | 128.6 ± 20.2 | 139.3 ± 20.9 | 123.6 ± 17.9 | <0.001 2 |
| <120 | 34 (36.2) | 5 (16.7) | 29 (45.3) | <0.001 3 |
| ≥120 to <140 | 31 (33.0) | 7 (23.3) | 24 (37.5) | |
| ≥140 | 29 (30.9) | 18 (60.0) | 11 (17.2) | |
| Baseline DBP (mmHg) | 75.2 ± 9.9 | 79.0 ± 8.6 | 73.4 ± 10.1 | 0.005 2 |
| <80 | 64 (68.1) | 15 (50.0) | 49 (76.6) | 0.010 3 |
| ≥80 | 30 (31.9) | 15 (50.0) | 15 (23.4) | |
| Postprandial SBP change (mmHg) | <0.001 3 | |||
| <10 | 26 (27.7) | 3 (10.0) | 23 (35.9) | |
| ≥10 to <20 | 21 (22.3) | 1 (3.3) | 20 (31.3) | |
| ≥20 | 47 (50.0) | 26 (86.7) | 21 (32.8) | |
| Postprandial DBP change (mmHg) | 0.023 3 | |||
| <10 | 41 (43.6) | 8 (26.7) | 33 (51.6) | |
| ≥10 | 53 (56.4) | 22 (73.3) | 31 (48.4) |
| Characteristic | Univariate | Multivariate | ||||
|---|---|---|---|---|---|---|
| HR | 95% CI | p-Value | HR | 95% CI | p-Value | |
| PPH | 15.97 | 3.80–67.08 | <0.001 | 11.18 | 2.43–51.38 | 0.002 |
| Age (years) | 1.00 | 0.93–1.07 | 0.940 | |||
| Sex (female) | 0.90 | 0.34–2.35 | 0.830 | |||
| BMI (kg/m2) | 1.14 | 1.01–1.29 | 0.030 | 1.10 | 0.96–1.26 | 0.173 |
| Education level (vs. Elementary school) | ||||||
| Middle school | 0.61 | 0.19–2.04 | 0.430 | |||
| High school | 0.57 | 0.17–1.88 | 0.350 | |||
| Living status (Living alone) | 0.80 | 0.37–1.75 | 0.580 | |||
| Alcohol drinking | 1.61 | 0.66–3.95 | 0.300 | |||
| Smoking | 1.77 | 0.42–7.46 | 0.430 | |||
| Hypertension | 4.61 | 1.77–12.05 | 0.002 | 3.26 | 1.22–8.73 | 0.019 |
| Diabetes mellitus | 3.20 | 1.56–6.56 | 0.002 | 1.80 | 0.84–3.89 | 0.132 |
| Baseline SBP (mmHg) | 1.03 | 1.02–1.05 | <0.001 | 1.02 | 0.99–1.05 | 0.148 |
| Baseline DBP (mmHg) | 1.03 | 1.01–1.06 | 0.013 | 0.97 | 0.91–1.02 | 0.245 |
© 2020 by the author. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Jang, A. Postprandial Hypotension as a Risk Factor for the Development of New Cardiovascular Disease: A Prospective Cohort Study with 36 Month Follow-Up in Community-Dwelling Elderly People. J. Clin. Med. 2020, 9, 345. https://doi.org/10.3390/jcm9020345
Jang A. Postprandial Hypotension as a Risk Factor for the Development of New Cardiovascular Disease: A Prospective Cohort Study with 36 Month Follow-Up in Community-Dwelling Elderly People. Journal of Clinical Medicine. 2020; 9(2):345. https://doi.org/10.3390/jcm9020345
Chicago/Turabian StyleJang, Aelee. 2020. "Postprandial Hypotension as a Risk Factor for the Development of New Cardiovascular Disease: A Prospective Cohort Study with 36 Month Follow-Up in Community-Dwelling Elderly People" Journal of Clinical Medicine 9, no. 2: 345. https://doi.org/10.3390/jcm9020345