The Effect of (Poly)phenol-Rich Interventions on Cognitive Functions and Neuroprotective Measures in Healthy Aging Adults: A Systematic Review and Meta-Analysis

 , , , , , , , ,
, , , , , , , ,
Abstract
:1. Introduction.
2. Method
2.1. Data Sources and Search Strategy
2.2. Inclusion and Exclusion Criteria
2.3. Study Selection
2.4. Data Extraction
2.5. Quality Assessment
2.6. Statistical Analysis
3. Results
3.1. Study Selection and Characteristics
3.1.1. Study Selection
3.1.2. Study Characteristics
3.2. Subject Characteristics
3.3. Study Design and Supplement Administration
3.4. Methodological Quality of Studies
3.5. Effect of (Poly)Phenol-Rich Supplementation on Cognitive Functions of Older Adults
3.6. Effect of (Poly)Phenol-Rich Supplementation on Brain Parameters of Older Adults
3.7. Meta-Analysis Results
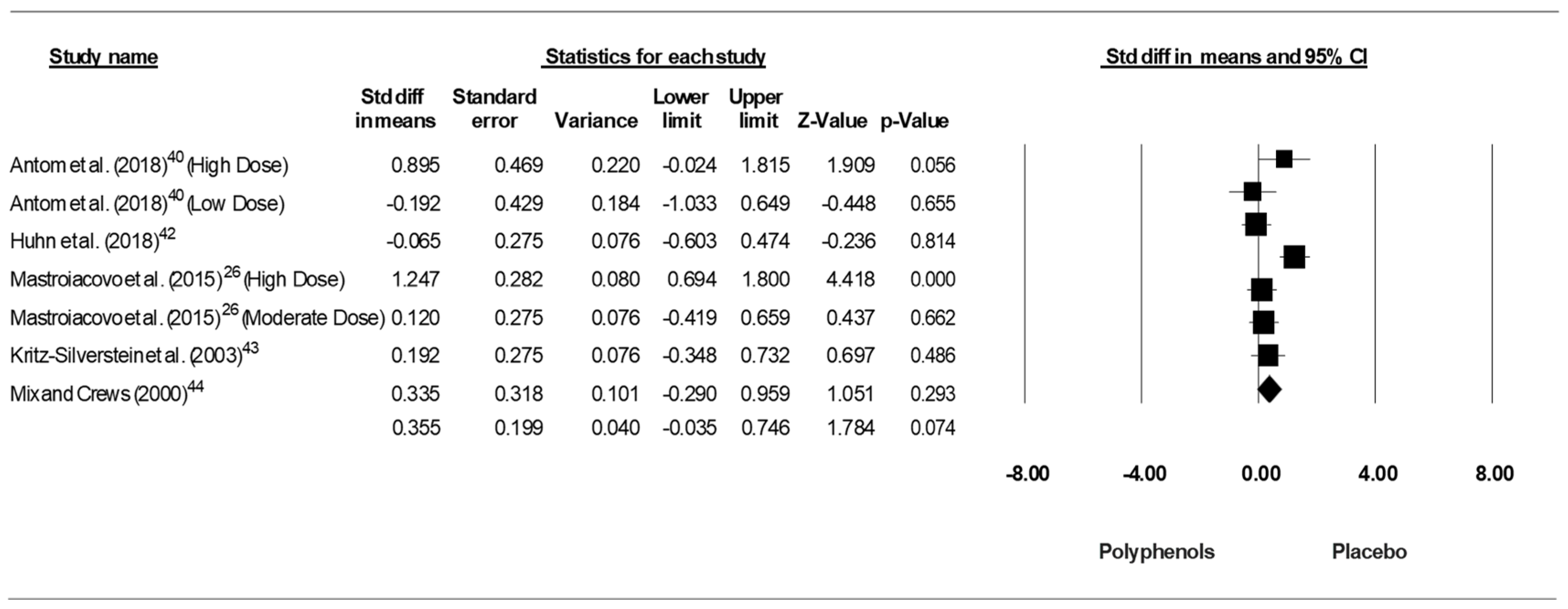
3.7.1. Trail Making Test-A
3.7.2. Trail Making Test-B
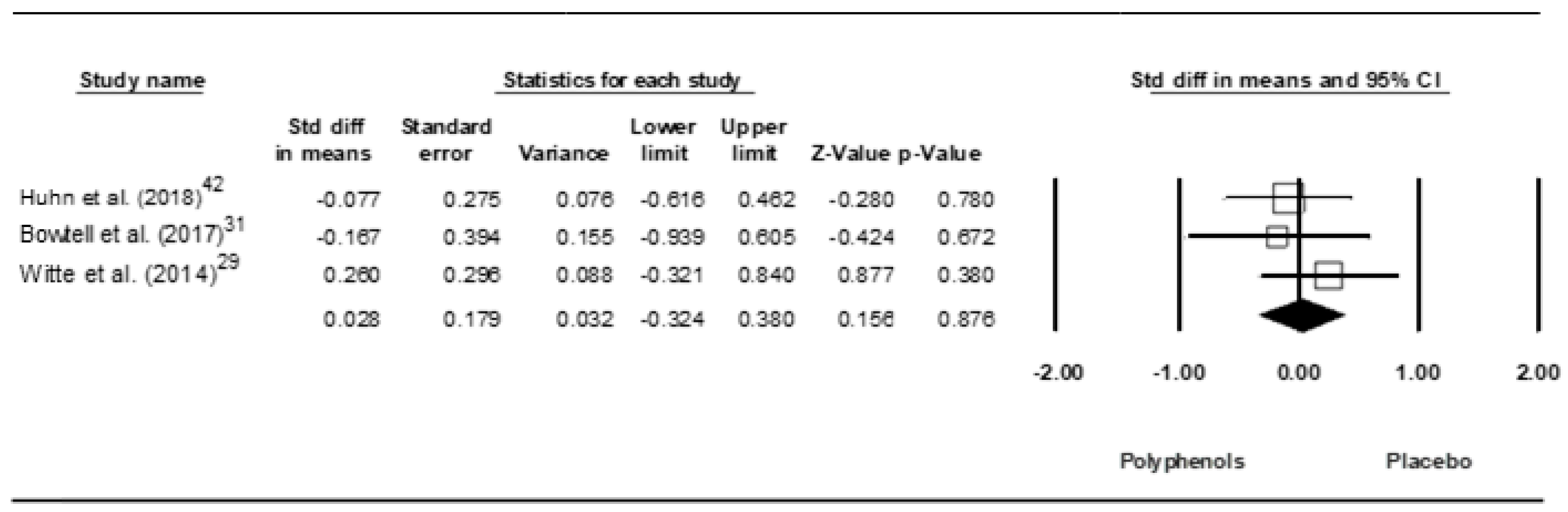
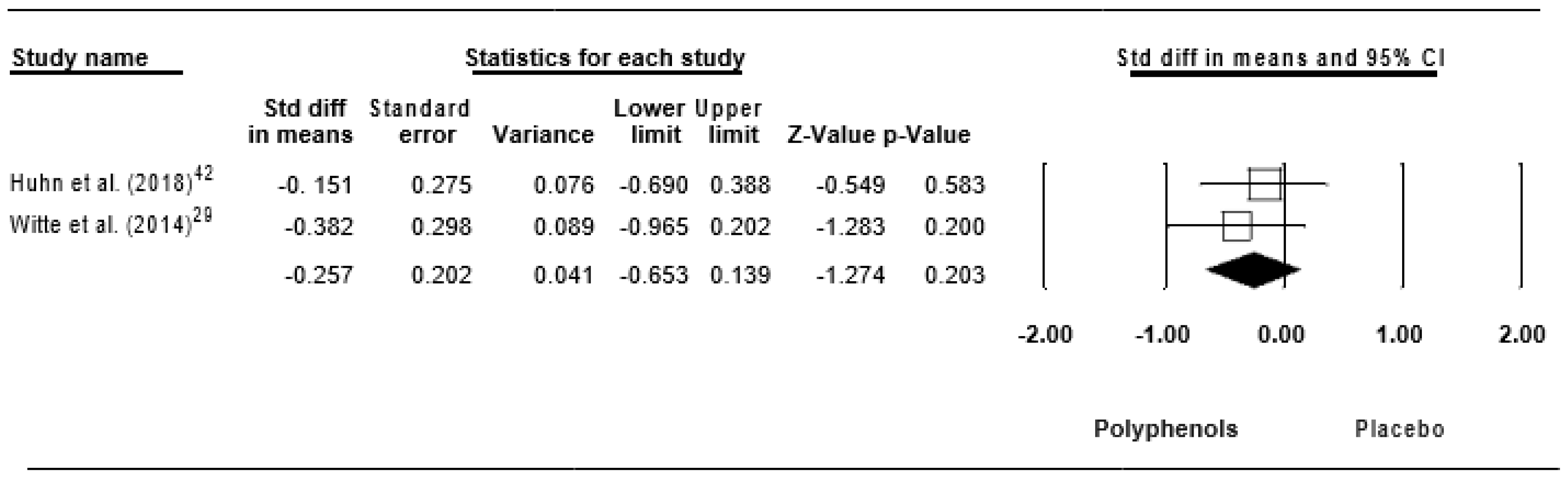
3.7.3. Brain-Derived Neurotrophic Factor
3.7.4. High-Sensitivity C-reactive Protein
3.7.5. Interleukin-6
3.7.6. Tumor Necrosis Factor alpha
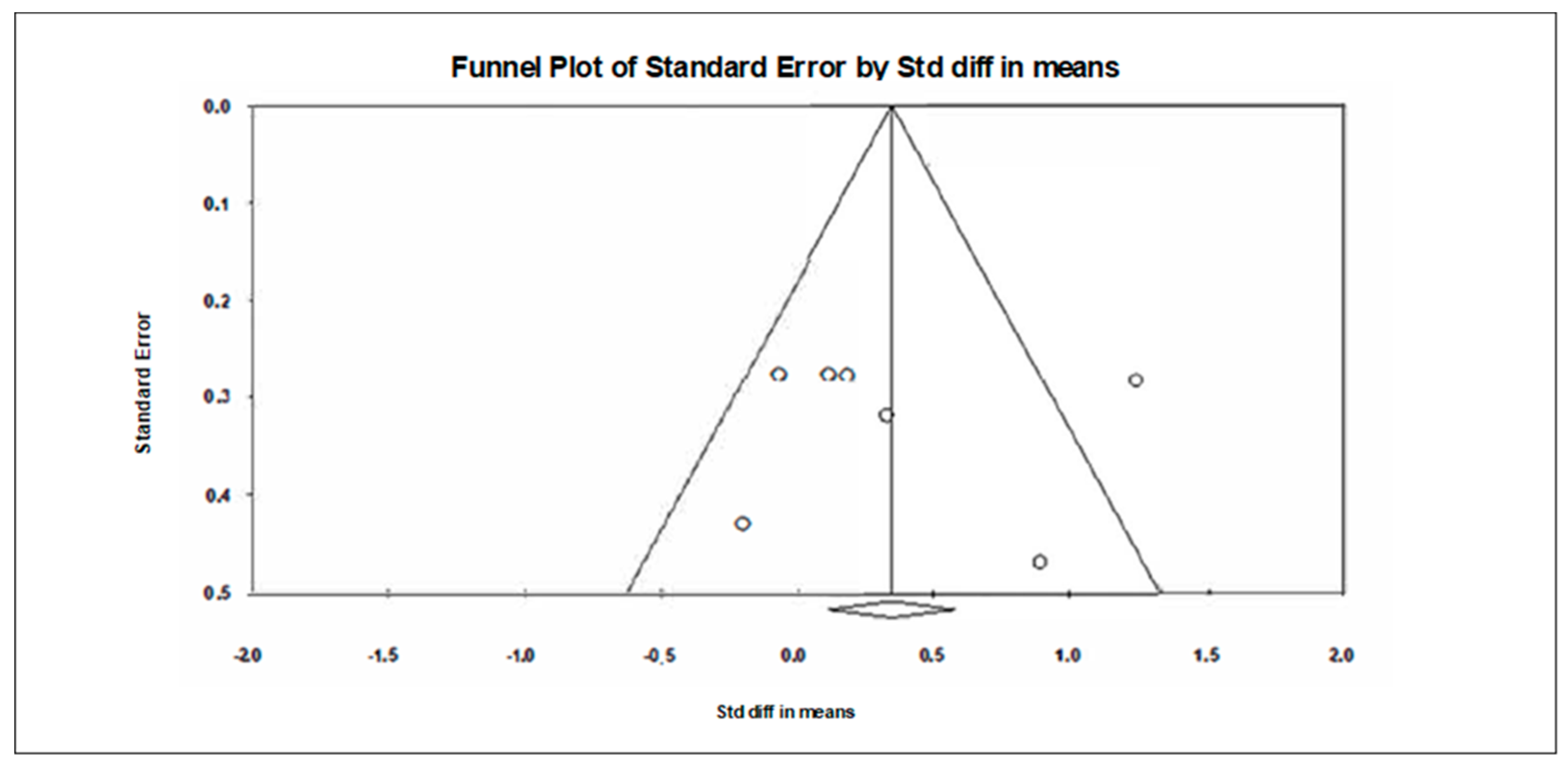
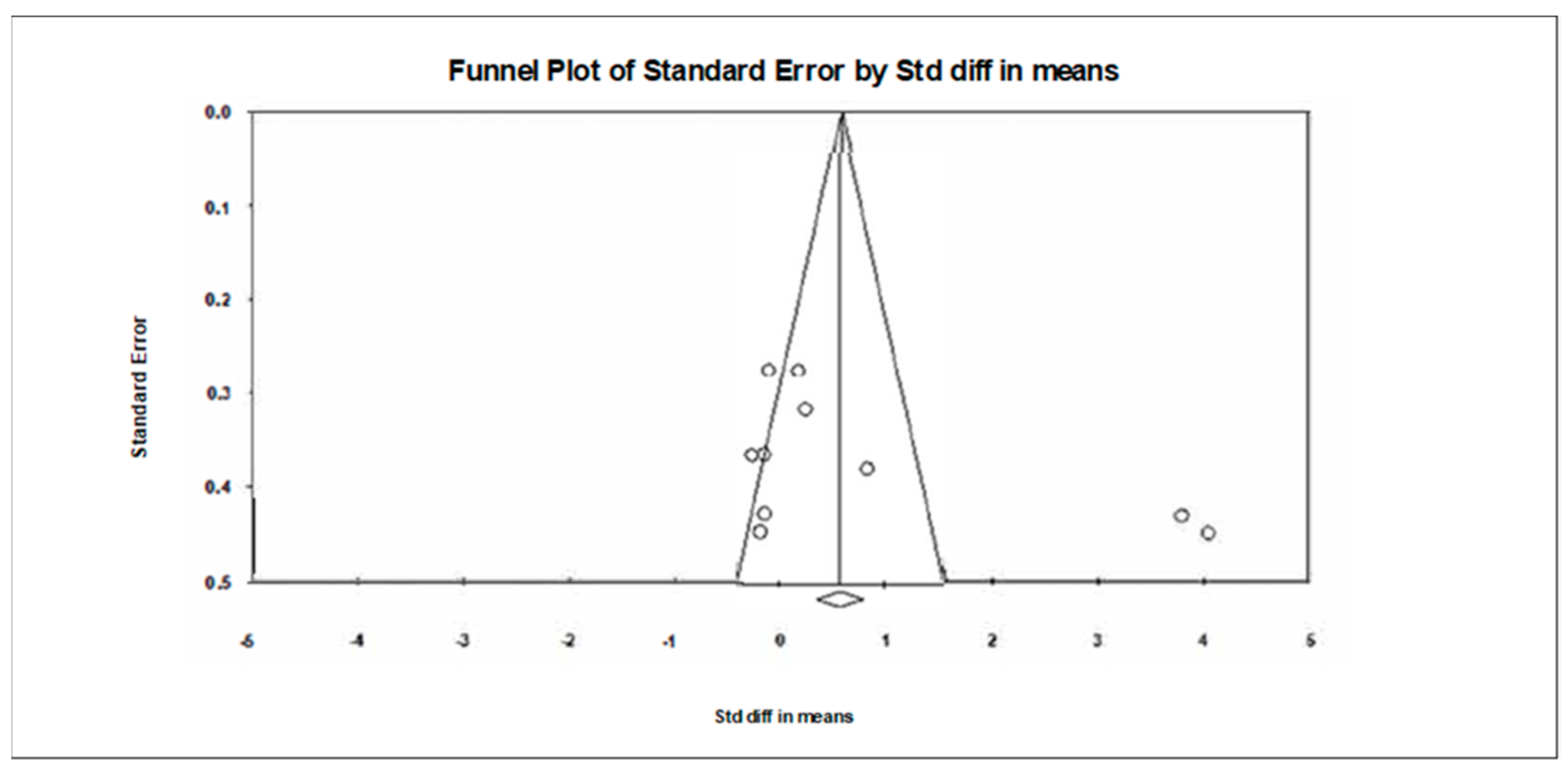
3.8. Sensitivity and Cumulative Meta-Analyses
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- World Health Organization (WHO). World Report on Ageing and Health. 2018. Available online: https://www.who.int/news-room/fact-sheets/detail/ageing-and-health (accessed on 22 December 2019).
- Pluvinage, J.V.; Wyss-Coray, T. Systemic factors as mediators of brain homeostasis, ageing and neurodegeneration. Nat Rev Neurosci. 2020, 1–10. [Google Scholar] [CrossRef]
- Murman, D.L. The Impact of Age on Cognition. Semin. Hear. 2015, 36, 111–121. [Google Scholar] [CrossRef]
- Gazzaley, A.; Sheridan, M.A.; Cooney, J.W.; D’Esposito, M. Age-related deficits in component processes of working memory. Neuropsychology 2007, 21, 532–539. [Google Scholar] [CrossRef] [Green Version]
- Small, B.J.; Fratiglioni, L.; Viitanen, M.; Winblad, B.; Bäckman, L. The course of cognitive impairment in preclinical Alzheimer disease: Three- and 6-year follow-up of a population-based sample. Arch Neurol. 2000, 57, 839–844. [Google Scholar] [CrossRef] [Green Version]
- Kramer, A.F.; Erickson, K.I.; Colcombe, S.J. Exercise, cognition, and the aging brain. J. Appl. Physiol. 2006, 101, 1237–1242. [Google Scholar] [CrossRef]
- Asha Devi, S.; Satpati, A. Oxidative Stress and the Brain: An Insight into Cognitive Aging. In Topics in Biomedical Gerontology; Rath, P., Sharma, R., Prasad, S., Eds.; Springer: Singapore, 2017; pp. 123–140. [Google Scholar]
- Legdeur, N.; Heymans, M.W.; Comijs, H.C.; Huisman, M.; Maier, A.B.; Visser, P.J. Age dependency of risk factors for cognitive decline. BMC Geriatr. 2018, 18, 187. [Google Scholar] [CrossRef]
- Floyd, R.A.; Hensley, K. Oxidative stress in brain aging. Implications for therapeutics of neurodegenerative diseases. Neurobiol. Aging 2002, 23, 795–807. [Google Scholar] [CrossRef]
- Jolitha, A.B.; Subramanyam, M.V.V.; Asha Devi, S. Modification by vitamin E and exercise of oxidative stress in regions of aging rat brain: Studies on superoxide dismutase isoenzymes and protein oxidation status. Exp. Geront. 2006, 41, 753–763. [Google Scholar] [CrossRef]
- Bratic, A.; Larsson, N. The role of mitochondria in aging. J. Clin. Investig. 2013, 123, 951–957. [Google Scholar] [CrossRef] [Green Version]
- Siqueira, I.R.; Fochesatto, C.; de Andrade, A.; Santos, M.; Hagen, M.; Bello-Klein, A.; Netto, C.A. Total antioxidant capacity is impaired in different structures from aged rat brain. Int. J. Dev. Neurosci. 2005, 23, 663–671. [Google Scholar] [CrossRef]
- Hasan, M.; Tripathi, S.; Mahdi, A.A.; Mitra, K.; Negi, M.P.L. Lipofuscin, lipid peroxidation and antioxidant status in discrete regions of the aged rat brain. Proc. Indian Natl. Acad. Sci. 2009, 75, 173–181. [Google Scholar]
- Halliwell, B. Free radicals and antioxidants: Updating a personal view. Nutr. Rev. 2012, 70, 257–265. [Google Scholar] [CrossRef]
- Pesce, M.; Tatangelo, R.; La Fratta, I.; Rizzuto, A.; Campagna, G.; Turli, C.; Ferrone, A.; Franceschelli, S.; Speranza, L.; Patruno, A.; et al. Aging-Related Oxidative Stress: Positive Effect of Memory Training. Neuroscience 2018, 370, 246–255. [Google Scholar] [CrossRef]
- Heneka, M.T.; Carson, M.J.; El Khoury, J.; Landreth, G.E.; Brosseron, F.; Feinstein, D.L.; Jacobs, A.H.; Wyss-Coray, T.; Vitorica, J.; Ransohoff, R.M.; et al. Neuroinflammation in Alzheimer’s disease. Lancet Neurol. 2015, 14, 388–405. [Google Scholar] [CrossRef] [Green Version]
- Kinney, J.W.; Bemiller, S.M.; Murtishaw, A.S.; Leisgang, A.M.; Salazar, A.M.; Lamb, B.T. Inflammation as a central mechanism in Alzheimer’s disease. Alzheimers Dement 2018, 4, 575–590. [Google Scholar] [CrossRef]
- Solleiro-Villavicencio, H.; Rivas-Arancibia, S. Effect of Chronic Oxidative Stress on Neuroinflammatory Response Mediated by CD4+T Cells in Neurodegenerative Diseases. Front Cell Neurosci. 2018, 12, 114. [Google Scholar] [CrossRef] [Green Version]
- Vauzour, D.; Camprubi-Robles, M.; Miquel-Kergoat, S.; Andres-Lacueva, C.; Bánáti, D.; Barberger-Gateau, P.; Bowman, G.L.; Caberlotto, L.; Clarke, R.; Hogervorst, E.; et al. Nutrition for the ageing brain: Towards evidence for an optimal diet. Ageing Res. Rev. 2017, 35, 222–240. [Google Scholar] [CrossRef] [Green Version]
- Vauzour, D. Dietary polyphenols as modulators of brain functions: Biological actions and molecular mechanisms underpinning their beneficial effects. Oxid. Med. Cell. Longev. 2012, 914273. [Google Scholar] [CrossRef] [Green Version]
- Hussain, M.B.; Hassan, S.; Waheed, M.; Javed, A.; Farooq, M.A.; Tahir, A. Bioavailability and Metabolic Pathway of Phenolic Compounds. 5. In Plant Physiological Aspects of Phenolic Compounds; Marcos, S.-H., Rosario, G.-M., Mariana, P.-T., Eds.; IntechOpen: Rijeka, Croatia, 2019. [Google Scholar]
- Ammar, A.; Bailey, S.J.; Chtourou, H.; Trabelsi, K.; Turki, M.; Hökelmann, A.; Souissi, N. Effects of pomegranate supplementation on exercise performance and post-exercise recovery: A systematic review. Br. J. Nutr. 2018, 20, 1201–1216. [Google Scholar] [CrossRef] [Green Version]
- Ammar, A.; Turki, M.; Chtourou, H.; Hammouda, O.; Trabelsi, K.; Kallel, C.; Abdelkarim, O.; Hoekelmann, A.; Bouaziz, M.; Ayadi, F.; et al. Pomegranate Supplementation Accelerates Recovery of Muscle Damage and Soreness and Inflammatory Markers after a Weightlifting Training Session. PLoS ONE 2016, 11, e0160305. [Google Scholar] [CrossRef] [Green Version]
- Ammar, A.; Turki, M.; Hammouda, O.; Chtourou, H.; Trabelsi, K.; Bouaziz, M.; Abdelkarim, O.; Hoekelmann, A.; Ayadi, F.; Souissi, N.; et al. Effects of Pomegranate Juice Supplementation on Oxidative Stress Biomarkers Following Weightlifting Exercise. Nutrients 2017, 9, 819. [Google Scholar] [CrossRef] [Green Version]
- Fraga, C.G.; Croft, K.D.; Kennedy, D.O.; Tomás-Barberán, F.A. The effects of polyphenols and other bioactives on human health. Food Funct. 2019, 10, 514–528. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mastroiacovo, D.; Kwik-Uribe, C.; Grassi, D.; Necozione, S.; Raffaele, A.; Pistacchio, L.; Righetti, R.; Bocale, R.; Lechiara, M.C.; Marini, C.; et al. Cocoa flavanol consumption improves cognitive function, blood pressure control, and metabolic profile in elderly subjects: The Cocoa, Cognition, and Aging (CoCoA) Study--a randomized controlled trial. Am. J. Clin. Nutr. 2015, 101, 538–548. [Google Scholar] [CrossRef]
- Whyte, A.R.; Cheng, N.; Fromentin, E.; Williams, C.M. A Randomized, Double-Blinded, Placebo-Controlled Study to Compare the Safety and Efficacy of Low Dose Enhanced Wild Blueberry Powder and Wild Blueberry Extract (ThinkBlue™) in Maintenance of Episodic and Working Memory in Older Adults. Nutrients 2018, 10, 660. [Google Scholar] [CrossRef] [Green Version]
- Wightman, E.L.; Jackson, P.A.; Khan, J.; Forster, J.; Heiner, F.; Feistel, B.; Suarez, C.G.; Pischel, I.; Kennedy, D.O. The Acute and Chronic Cognitive and Cerebral Blood Flow Effects of a Sideritisscardica (Greek Mountain Tea) Extract: A Double Blind, Randomized, Placebo Controlled, Parallel Groups Study in Healthy Humans. Nutrients 2018, 10, 955. [Google Scholar] [CrossRef] [Green Version]
- Witte, A.V.; Kerti, L.; Margulies, D.S.; Flöel, A. Effects of resveratrol on memory performance, hippocampal functional connectivity, and glucose metabolism in healthy older adults. J. Neurosci. 2014, 34, 7862–7870. [Google Scholar] [CrossRef] [Green Version]
- Lamport, D.J.; Pal, D.; Moutsiana, C.; Field, D.T.; Williams, C.M.; Spencer, J.P.; Butler, L.T. The effect of flavanol-rich cocoa on cerebral perfusion in healthy older adults during conscious resting state: A placebo controlled, crossover, acute trial. Psychopharmacology 2015, 232, 3227–3234. [Google Scholar] [CrossRef] [Green Version]
- Bowtell, J.L.; Aboo-Bakkar, Z.; Conway, M.E.; Adlam, A.R.; Fulford, J. Enhanced task-related brain activation and resting perfusion in healthy older adults after chronic blueberry supplementation. Appl. Physiol. Nutr. Metab. 2017, 42, 773–779. [Google Scholar] [CrossRef]
- Ho, K.K.; Ferruzzi, M.G.; Wightman, J.D. Potential health benefits of (poly) phenols derived from fruit and 100% fruit juice. Nutr. Rev. 2020, 78, 145–174. [Google Scholar] [CrossRef]
- Cui, C.; Birru, R.L.; Snitz, B.E.; et al. Effects of soy isoflavones on cognitive function: A systematic review and meta-analysis of randomized controlled trials. Nutr. Rev. 2020, 78, 134–144. [Google Scholar] [CrossRef]
- Holland, T.M.; Agarwal, P.; Wang, Y.; Leurgans, S.E.; Bennett, D.A.; Booth, S.L.; Morris, M.C. Dietary flavonols and risk of Alzheimer dementia. Neurology 2020, 10. [Google Scholar] [CrossRef]
- Gleason, C.E.; Carlsson, C.M.; Barnet, J.H.; Meade, S.A.; Setchell, K.D.; Atwood, C.S.; Johnson, S.C.; Ries, M.L.; Asthana, S. A preliminary study of the safety, feasibility and cognitive efficacy of soy isoflavone supplements in older men and women. Age Ageing 2009, 38, 86–93. [Google Scholar] [CrossRef] [Green Version]
- Howes, J.B.; Bray, K.; Lorenz, L.; Smerdely, P.; Howes, L.G. The effects of dietary supplementation with isoflavones from red clover on cognitive function in postmenopausal women. Climacteric 2004, 7, 70–77. [Google Scholar] [CrossRef]
- Marsh, C.E.; Carter, H.H.; Guelfi, K.J.; Smith, K.J.; Pike, K.E.; Naylor, L.H.; Green, D.J. Brachial and cerebrovascular functions are enhanced in postmenopausal women after ingestion of chocolate with a high concentration of cocoa. J. Nutr. 2017, 147, 1686–1692. [Google Scholar] [CrossRef]
- Rosenberg, A.; Mangialasche, F.; Ngandu, T.; Solomon, A.; Kivipelto, M. Multidomain Interventions to Prevent Cognitive Impairment, Alzheimer’s Disease, and Dementia: From FINGER to World-Wide FINGERS. J. Prev. Alzheimers Dis. 2019, 1–8. [Google Scholar] [CrossRef]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. J. Clin. Epidemiol. 2009, 62, 1006–1012. [Google Scholar] [CrossRef]
- Anton, S.D.; Ebner, N.; Dzierzewski, J.M.; Zlatar, Z.Z.; Gurka, M.J.; Dotson, V.M.; Kirton, J.; Mankowski, R.T.; Marsiske, M.; Manini, T.M. Effects of 90 Days of Resveratrol Supplementation on Cognitive Function in Elders: A Pilot Study. J. Altern. Complementary Med. 2018, 24, 725–732. [Google Scholar] [CrossRef]
- Bensalem, J.; Dudonné, S.; Etchamendy, N.; Pellay, H.; Amadieu, C.; Gaudout, D.; Dubreuil, S.; Marie-Eve Paradis, M.E.; Pomerleau, S.; Capuron, L. Polyphenols from Grape and Blueberry Improve Episodic Memory in Healthy Elderly with Lower Level of Memory Performance: A Bicentric Double-Blind, Randomized, Placebo-Controlled Clinical Study. J. Gerontol. 2019, 74, 996–1007. [Google Scholar] [CrossRef]
- Huhn, S.; Beyer, F.; Zhang, R.; Lampe, L.; Grothe, J.; Kratzsch, J.; Willenberg, A.; Breitfeld, J.; Kovacs, P.; Stumvoll, M.; et al. Effects of resveratrol on memory performance, hippocampus connectivity and microstructure in older adults—A randomized controlled trial. NeuroImage 2018, 174, 177–190. [Google Scholar] [CrossRef]
- Kritz-Silverstein, D.; Von Mühlen, D.; Barrett-Connor, E.; Bressel, M.A.B. Isoflavones and cognitive function in older women: theSOy and Postmenopausal Health in Aging (SOPHIA) Study. Menopause 2003, 10, 196–202. [Google Scholar] [CrossRef]
- Mix, J.A.; Crews, W.D. An Examination of the Efficacy of Ginkgo biloba Extract EGb 761 on the Neuropsychologic Functioning of Cognitively Intact Older Adults. J. Altern. Complementary Med. 2000, 6, 219–229. [Google Scholar] [CrossRef] [PubMed]
- Sorond, F.A.; Lipsitz, L.A.; Hollenberg, N.K.; Fisher, N.D. Cerebral blood flow response to flavanol-rich cocoa in healthy elderly humans. Neuropsychiatr. Dis. Treat. 2008, 4, 433–440. [Google Scholar] [PubMed]
- Maher, C.G.; Sherrington, C.; Herbert, R.D.; Moseley, A.M.; Elkins, M. Reliability of the PEDro scale for rating quality of randomized controlled trials. Phys. Ther. 2003, 83, 713. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Verhagen, A.P.; de Vet, H.C.; de Bie, R.A.; Kessels, A.G.; Boers, M.; Bouter, L.M.; Knipschild, P.G. The delphi list: A criteria list for quality assessment of randomized clinical trials for conducting systematic reviews developed by delphi consensus. J. Clin. Epidemiol. 1998, 51, 1235. [Google Scholar] [CrossRef] [Green Version]
- Moseley, A.M.; Herbert, R.D.; Maher, C.G.; Sherrington, C.; Elkins, M.R. Reported quality of randomized controlled trials of physiotherapy interventions has improved over time. J. Clin. Epidemiol. 2011, 64, 594–601. [Google Scholar] [CrossRef]
- Higgins, J.; Green, S. Cochrane Handbook for Systematic Reviews of Interventions. Version 5.1.0. Available online: http//www.cochrane-handbook.orb (accessed on 1 March 2011).
- Hadi, A.; Najafgholizadeh, A.; Aydenlu, E.S.; Shafiei, Z.; Pirivand, F.; Golpour, S.; Pourmasoumi, M. Royal jelly is an effective and relatively safe alternative approach to blood lipid modulation: A meta-analysis. J. Funct. Foods 2018, 41, 202–209. [Google Scholar] [CrossRef]
- Hopkins, W.G.; Marshall, S.W.; Batterham, A.M.; Hanin, J. Progressive statistics for studies in sports medicine and exercise science. Med. Sci. Sports Exerc. 2009, 41, 3–13. [Google Scholar] [CrossRef] [Green Version]
- Morris, S.B. Estimating Effect Sizes FromPretest-Posttest-Control Group Designs. Organ. Res. Methods 2008, 11, 364–386. [Google Scholar] [CrossRef]
- Higgins, J.P.; Thompson, S.G.; Deeks, J.J.; Altman, D.G. Measuring inconsistency in meta-analyses. BMJ 2003, 327, 557–560. [Google Scholar] [CrossRef] [Green Version]
- Begg, C.B.; Mazumdar, M. Operating characteristics of a rank correlation test for publication bias. Biometrics 1994, 50, 1088–1101. [Google Scholar] [CrossRef]
- Egger, M.; Smith, G.D.; Schneider, M.; Minder, C. Bias in meta-analysis detected by a simple, graphical test. Br. Med. J. 1997, 315, 629–634. [Google Scholar] [CrossRef] [Green Version]
- Duval, S.; Tweedie, R. Trim and fill: A simple funnel-plot-based method of testing and adjusting for publication bias in meta-analysis. Biometrics 2000, 56, 455–463. [Google Scholar] [CrossRef] [PubMed]
- Figueira, I.; Menezes, R.; Macedo, D.; Costa, I.; Dos Santos, C.N. Polyphenols Beyond Barriers: A Glimpse into the Brain. Curr. Neuropharmacol. 2017, 15, 562–594. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- González-Fuentes, J.; Selva, J.; Moya, C.; Castro-Vázquez, L.; Lozano, M.V.; Marcos, P.; Plaza-Oliver, M.; Rodriguez-Robledo, V.; Santander-Ortega, M.J.; Villaseca-González, N.; et al. Neuroprotective natural molecules, from food to brain. Front. Neurosci. 2018, 12, 721. [Google Scholar] [CrossRef] [Green Version]
- Rein, M.J.; Renouf, M.; Cruz-Hernandez, C.; Actis-Goretta, L.; Thakkar, S.K.; da Silva Pinto, M. Bioavailability of bioactive food compounds: A challenging journey to bioefficacy. Br. J. Clin. Pharmacol. 2013, 75, 588–602. [Google Scholar] [CrossRef] [Green Version]
- D’Archivio, M.; Filesi, C.; Varì, R.; Scazzocchio, B.; Masella, R. Bioavailability of the polyphenols: Status and controversies. Int. J. Mol. Sci. 2010, 11, 1321–1342. [Google Scholar] [CrossRef]
- Manach, C.; Scalbert, A.; Morand, C.; Rémésy, C.; Jiménez, L. Polyphenols: Food sources and bioavailability. Am. J. Clin. Nutr. 2004, 79, 727–747. [Google Scholar] [CrossRef] [Green Version]
- Manach, C.; Williamson, G.; Morand, C.; Scalbert, A.; Remesy, C. Bioavailability and bioefficacy of polyphenols in humans. I. Review of 97 bioavailability studies. Am. J. Clin. Nutr. 2005, 81 (Suppl. 1), 230S–242S. [Google Scholar] [CrossRef] [Green Version]
- González-Gallego, J.; García, M.V.; Sánchez-Campos, S.; Tuñó, M.J. Fruit polyphenols, immunity and inflammation. Br. J. Nutr. 2010, 104 (Suppl. 3), S15–S27. [Google Scholar] [CrossRef] [Green Version]
- Spencer, J.P.; Vafeiadou, K.; Williams, R.J.; Vauzour, D. Neuroinflammation: Modulation by flavonoids and mechanisms of action. Mol. Asp. Med. 2012, 33, 83–97. [Google Scholar] [CrossRef]
- Kao, T.K.; Ou, Y.C.; Raung, S.L.; Lai, C.Y.; Liao, S.L.; Chen, C.J. Inhibition of nitric oxide production by quercetin in endotoxin/cytokine-stimulated microglia. Life Sci. 2010, 86, 315–321. [Google Scholar] [CrossRef] [PubMed]
- Kelley, D.S.; Rasooly, R.; Jacob, R.A.; Kader, A.A.; Mackey, B.E. Consumption of bing sweet cherries lowers circulating concentrations of inflammation markers in healthy men and women. J. Nutr. 2006, 136, 981. [Google Scholar] [CrossRef] [PubMed]
- Urbaniak, A.; Basta, P.; Ast, K.; Wołoszyn, A.; Kuriańska–Wołoszyn, J.; Latour, E.; Skarpańska–Stejnborn, A. The impact of supplementation with pomegranate fruit (Punicagranatum L.) juice on selected antioxidant parameters and markers of iron metabolism in rowers. J. Int. Soc. Sports Nutr. 2018, 15, 35. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Huebbe, P.; Giller, K.; de Pascual-Teresa, S.; Arkenau, A.; Adolphi, B.; Portius, S.; Arkenau, C.N.; Rimbach, G. Effects of blackcurrant-based juice on atherosclerosis-related biomarkers in cultured macrophages and in human subjects after consumption of a high-energy meal. Br. J. Nutr. 2012, 108, 234–244. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vafeiadou, K.; Vauzour, D.; Lee, H.Y.; Rodriguez-Mateos, A.; Williams, R.J.; Spencer, J.P.E. The citrus flavanone naringenin inhibits inflammatory signalling in glial cells and protects against neuroinflammatory injury. Arch. Biochem. Biophys. 2009, 484, 100–109. [Google Scholar] [CrossRef] [PubMed]
- Abramov, A.Y.; Jacobson, J.; Wientjes, F.; Hothersall, J.; Canevari, L.; Duchen, M.R. Expression and modulation of an NADPH oxidase in mammalian astrocytes. J. Neurosci. 2005, 25, 9176–9184. [Google Scholar] [CrossRef]
- Fisher, N.D.; Hollenberg, N.K. Aging and vascular responses to flavanol-rich cocoa. J. Hypertens 2006, 24, 1575–1580. [Google Scholar] [CrossRef] [Green Version]
- Fisher, N.D.; Hughes, M.; Gerhard-Herman, M.; Hollenberg, N.K. Flavanol-rich cocoa induces nitric-oxide-dependent vasodilation in healthy humans. J. Hypertens 2003, 21, 2281–2286. [Google Scholar] [CrossRef]
- Scalbert, A.; Manach, C.; Morand, C.; Rémésy, C.; Jiménez, L. Dietary polyphenols and the prevention of diseases. Crit. Rev. Food Sci. Nutr. 2005, 45, 287–306. [Google Scholar] [CrossRef]
- Hellsten, Y.; Nyberg, M.; Jensen, L.G.; Mortensen, S.P. Vasodilator interactions in skeletal muscle blood flow regulation. J. Physiol. 2012, 590, 6297–6305. [Google Scholar] [CrossRef]
- Ignarro, L.J.; Byrns, R.E.; Sumi, D.; de Nigris, F.; Napoli, C. Pomegranate juice protects nitric oxide against oxidative destruction and enhances the biological actions of nitric oxide. Nitric Oxide 2006, 15, 93–102. [Google Scholar] [CrossRef] [PubMed]
- Nehlig, A. The neuroprotective effects of cocoa flavanol and its influence on cognitive performance. Br. J. Clin. Pharm. 2012, 75, 716–727. [Google Scholar] [CrossRef] [PubMed]
- Luh, W.M.; Wong, E.C.; Bandettini, P.A.; Ward, B.D.; Hyde, J.S. Comparison of simultaneously measured perfusion and BOLD signalincreases during brain activation with T (1)-based tissue identification. MagnReson Med. 2000, 44, 137–143. [Google Scholar] [CrossRef]
- Kim, S.G.; Duong, T.Q. Mapping cortical columnar structures using fMRI. Physiol. Behav. 2002, 77, 641–644. [Google Scholar] [CrossRef]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Parameter | Inclusion Criterion |
|---|---|
| Participants | Aging adults (55 years old and over) |
| Intervention | Acute and/or chronic (poly)phenols-rich supplementation |
| Comparison | Any |
| Outcome | Cognitive functions (e.g., overall cognition, psychomotor performance, executive function, processing speed, attention, language, verbal memory, and visual memory) and neuroprotective measures (e.g., brain perfusion, brain activity, cerebral hemodynamics, cerebral blood flow (CBF), neuroplasticity, and neuroinflammation) |
| Study design | Randomized controlled trial |
| Authors | Study Design | Treatment | Phenolyc Content | Dose | Duration | Washout | Study Population | Effect on Cognitive Functions | Assessing Methods (e.g., Cognitive Battery Test) |
|---|---|---|---|---|---|---|---|---|---|
| Antom et al. (2018) [40] | Double-blind, phase II, randomized, placebo-controlled pilot study | Resveratrol | Not mentioned | Low dose: 300 mg/day; high dose: 1000 mg/day | Chronic: 90 Days | N/A | n = 32 (10 PLA, 12 low dose, 10 high dose); sedentary older adults, mean age: 73.34 ± 7.02 years old (65–93 years) | ↑ significantly improves psychomotor speed on the TMT-A using 1000 mg/day; ↔ nonsignificant effect on the other cognitive functions (visual attention, working memory, verbal fluency, and semantic memory) | Trail Making Test (TMT) assessing executive functions: TMT-A = information processing speed, digits forward and backward (auditory attention: forward) and working memory (backward), digit symbol substitution test (attention and processing speed), Erikson–Flanker task (executive function by measuring response inhibition), controlled oral word association (verbal fluency), Hopkins Verbal Learning Test-Revised: HVLT (verbal learning, recognition memory, and recall), and task switching (accuracy and reaction time) |
| Bensalem et al. (2019) [41] | Bicentric, randomized, double-blind, placebo-controlled trial | polyphenol-rich extract from grape and blueberry (PEGB) | 258 mg flavonoids/day | 600 mg/day: 2 capsules (each one contains 300 mg PEGB)/day | chronic: 24 weeks | N/A | n = 190 (92 PEGB group, 98 PLA group), healthy elderly subjects, mean age: 64.66 ± 2.91 years old (60–70 years) | ↑ significantly improves VRM-free recall; ↔ nonsignificant effect on the other cognitive functions (PAL, VRMR, SSP, and reverse SSP) | Cambridge Neuropsychological Test Automated Battery (CANTAB): Paired Associate Learning (PAL) test (visuospatial learning and episodic memory); verbal recall memory: VRM (episodic RM using VRM-free recall (VRMFR) and VR recognition memory using (VRMR) and working memory using the Special Span (SSP) and the reverse SSP tests |
| Bowtell et al. (2017) [31] | Randomized, double-blind, placebo-controlled parallel trial | Anthocyanin-rich blueberry concentrate | 387 mg anthocyanidins/day | 30 mL blueberry concentrate (diluted to 240 mL total volume with tap water); 387 mg anthocyanidins/day | chronic: 12 weeks | N/A | n = 26 (12 blueberry, 14 PLA), older adults, mean age: blueberry group = 67.5 ± 0.9, PLA group = 69 ± 0.9 | ↑ significantly improves working memory performance during 2 back cognitive task; nonsignificant improvement during 1 back cognitive task; ↔ nonsignificant effect on the other cognitive functions | The cognitive battery of tests (CogStateLtd.): detection task (psychomotor function), the Groton maze timed chase test (speed of visual processing), the Groton maze learning test with a delayed recall component (executive function and delayed record), identification task (attention), international shopping list task with delayed recall (verbal learning and delayed recall), 1-back and 2-back memory tasks (working memory). The speed and accuracy of responses were quantified. |
| Gleason et al. (2009) [35] | Double-blind, randomized, placebo-controlled, parallel-group pilot study | Purified glycosidic isoflavones | 100 mg isoflavones | 100 mg soy-isoflavones/day | chronic: 6 months | N/A | n = 30, (15 isoflavones, 15 PLA), older adults: mean age: isoflavone group = 73 ± 7.9, PLA group: 74.3 ± 6.3, (range: 62–89 years) | ↑ significantly improves cognitive performances on 2 tests of verbal and visuospatial memory (Rey complex figure and visual spatial learning tests), verbal/language fluency test, and visual-motor function tests; ↔ nonsignificant effect on two tests of verbal learning and recall (Buschke Selective Reminding Test and Paragraph Recall Test), language (Boston Naming test), one test of executive function (mazes); ↓ significantly decreases performance during two tests of executive functions (Trail Making Test part B TMT-B and Stroop Color-Word test) | Battery of neuropsychological measures: verbal and visuospatial memory (Buschke Selective Reminding test, Paragraph Recall, Rey Complex Figure test, Visual Spatial Learning test); language (Boston Naming test); language fluency (FAS, animal fluency); visual-motor function (Rey Complex Figure test copy, Grooved Pegboard), and executive function (Stroop Color Word test, Mazes, TMT-B = cognitive flexibility) |
| Howes et al. (2004) [36] | Double blind, randomized, placebo-controlled, counterbalanced trial | Isoflavone-rich extract from red clover | 25 mg of formononetin, 2.5 mg of biochanin and <1 mg of genistein and daidzein | Two tablets/day (~55 mg isoflavone/day) | chronic: 6 months | 1 month | n = 30, (15 isoflavones, 15 PLA), older women, mean age: isoflavones group = 68.5 ± 6.6 years; placebo group = 67.7 ± 5.5 years | ↑ significantly improves cognitive performance during block design test (a test of visual-spatial intelligence); ↔ nonsignificant effect on the other tests; ↓ significantly decreases performances during digit recall and verbal memory 2 tests (all not significant if correction to multiple comparisons is made) | Tests of speed of information processing (trail A and digit symbol); tests of memory (memory 1 and 2, verbal memory 1 and 2, and visual memory 1 and 2); tests of verbal ability (Boston naming test, FAS test, animal naming test, and similarities naming test); tests of frontal cortex function (arithmetic test, trail B test, and block design test); digit recall |
| Huhn et al. (2018) [42] | Double-blind, randomized controlled trial | Resveratrol | 200 mg resveratrol/day | Two pills of 100 mg resveratrol per day (total daily dose/day = 200 mg/day) | chronic: 26 weeks | N/A | n = 60 (30 resveratrol group, 30 PLA), elderly participants, range age: 60–79 years | nonsignificant improvement on pattern recognition memory; ↔ nonsignificant effect on verbal memory performance | Verbal memory performance (learning ability, delayed recall, rate of forgetting, and recognition) were assessed using the German version of the California Verbal Learning Task (CVLT); attention and mental flexibility were assessed using the TMT-A and TMT-B. Pattern recognition performance was assessed with the ModBent task |
| Kritz-Silverstein et al. (2003) [43] | Double-blind, randomized, placebo-controlled trial | Soy-extracted isoflavones | 110 mg total isoflavones/day | Two pills of 55 mg of soy-extracted isoflavones per day (total daily dose = 110 mg/day) | chronic: 6 months | N/A | n = 53 (27 treatment, 26 PLA), older women, mean age: treatment group = 60 ± 4, PLA: 62 ± 6 | ↑ significantly improves category fluency verbal memory performance; nonsignificant improvement on trail B and the immediate and delayed logical memory and recall test; ↔ nonsignificant effect on trail A | Cognitive function tests: trails A and B (assess visuomotor tracking and attention), category fluency (assess verbal memory), and logical memory and recall tests (a paragraph recall test assessing immediate and delayed verbal memory). |
| Marsh et al. (2017) [37] | Counterbalanced within-subject crossover design | Chocolate with a high concentration of polyphenols-rich cocoa | Total polyphenols: ≈85 mg: white chocolate, 200 mg: milk chocolate, 395 mg: Dark chocolate | 84 g dark chocolate (80% cacao), 87 g milk chocolate (35% cacao), or 85 g white chocolate (0% cacao) per daily | Acute | 1 week | n = 12 (counterbalanced design), older women, mean age: 57.3 ± 5.3 y) | ↔ nonsignificant effect on any of the assessed cognitive functions | 7 CogState measures: verbal memory, psychomotor memory, visual attention, working memory (one back), working memory (two back), visual memory, and verbal recall memory |
| Mastroiacovo et al. (2015) [26] | Double-blind, controlled, parallel-arm study | Cocoa flavanol drinks (high, moderate, and low flavanol contents) | Total flavanols: high flavanol drink (993 mg), moderate flavanols drink (520 mg), low flavanols drink (48 mg) | 250 mL drink with high, moderate, or low flavanol content/day | chronic: 8 weeks | N/A | n = 90 (30 for each study’s arm), older adults, age > 60 years old | ↑ significant improvement in performance of TMT-A and TMT-B and overall cognitive performance “z score” after consumption of the high and the intermediate flavanol drinks; ↑significant improvement in the Verbal Fluency Test (VFT) score using the high flavanols drink; ↔ nonsignificant effect on Mini-Mental State Examination (MMSE) | Mini-Mental State Examination (MMSE); TMT-A and TMT-B; the Verbal Fluency Test (VFT); and overall cognitive function (z score) |
| Mix & Crews. (2000) [44] | Double-blind, fixed-dose, placebo-controlled, parallel-group design | Ginkgo biloba extract EGb 761 | Not mentioned | 180 mg/day | 6 weeks | N/A | n = 48 (n of each arm: not mentioned), older adults, age range: 55–86 years old | ↑ significant improvement on one task assessing speed of processing abilities (i.e., color-naming task of the Stroop Color and Word Test); nonsignificant improvement in the majorities of the remaining tasks that involved a timed, speed of processing component (e.g., trail making test A and B); ↔ nonsignificant effect on the four objective memory measures (i.e., logical memory I and II and visual reproduction I and II) | Stroop Color and Word Test, TMT-A and TMT-B, Wechsler Memory Scale—Revised (WMS-R), Logical Memory I and II (LM I and II), and Visual Reproduction I and II subtests (VR I and II) |
| Whyte et al. (2018) [27] | Randomized, double blinded, placebo-controlled trial | 1000 mg capsules of wild blueberry (WB): WBP500WBP1000 and WBE111 (purified WB extract) | Total polyohenol contents: WBP500 (35 mg/capsule) powder); WBP1000 (70 mg/capsule); WBE111 (50 mg/capsule) | 1 daily dose of either WBP500, WBP1000, or WBE111 | Chronic intervention (3 and 6 months) | N/A | n = 122 (30 PLA, 30 WBP500, 31 WBP1000, and 31 WBE111), older adults, mean age: 71 ± 4 years old (65–80 years) | ↑ significant improvement of verbal and short-term spatial episodic memory performances with better delayed word recognition during the RAVLT and better recall of sequences during the Corsi Block task following WBE111 at 3 months compared to PLA, ↔ nonsignificant effect on working memory and executive function at 3 months follow-up ↔ nonsignificant effect for all cognitive performance at 6 months follow-up | Battery of cognitive tasks targeting episodic memory (verbal episodic memory using the Rey’s Auditory Verbal Learning task (RAVLT), visual episodic memory using an object recognition task, and short-term spatial episodic memory using the Corsi Blocks task), working memory (using serial subtractions and Sternberg memory scanning tasks), and executive function (using the Modified Attention Network Task (MANT) and Stroop task) |
| Wightman et al. (2018) [28] | Double blind, randomized, placebo controlled, parallel groups study | Polyphenol-rich Greek mountain tea (Sideritis scardica) | Potal phenolic content = 6.25% of the 20% Greek mountain tee extract | 475 or 950 mg of Greek mountain tea daily | Acute and chrnic (4 weeks) | N/A | n = 140 (n of each arm: not mentioned), older adults, mean age 60.3 years old | Acute and chronic effects of the Greek mountain tea with ↑ significant improvement in working memory (fewer false alarm during RVIP test) and higher episodic memory accuracy (during the picture recognition task) using the higher (950 mg) dose; ↑ significant improvement in speed of attention (derived from reaction time during numerical working memory, choice reaction time, and RVIP tasks) using both intermediate (475 mg) and high doses (950 mg) compared to active Ginko control (240 mg) | Cognitive function tests battery (www.cognitivetesting.co.uk) assessing accuracy and speed of attention (choice reaction time test), working memory (numerical working memory task, Serial 3s and 7s tasks, and Rapid Visual Information Processing (RVIP) task), and episodic memory (delayed word recall, delayed name/face recall, delayed picture recognition, and delayed word recognition tasks) performances |
| Witte et al. (2014) [29] | Double blind, randomized, placebo controlled, parallel groups study | Resveratrol | Not mentioned | 200 mg/d | 26 weeks | N/A | n = 46 (23 resveratrol, 23 PLA), older female, mean age: resveratrol group = 65 ± 7 years old, PLA = 64 ± 5 years old | ↑ significant improvement on retention ability; nonsignificant improvement on delayed recall and recognition, ↔ nonsignificant effect on learning ability using AVLT | Memory performance (i.e., retention, delayed recall, and recognition) and learning ability were assessed using the Auditory Verbal Learning Test (AVLT) |
| Authors | Study Design | Treatment | Phenolyc Content | Dose | Duration | Washout | Study Population | Effect on Neuroprotective Measures | Assessing Methods (e.g., Cognitive Battery Test) |
|---|---|---|---|---|---|---|---|---|---|
| Bowtell et al. (2017) [31] | Randomized, double-blind, placebo-controlled parallel trial | Anthocyanin-rich blueberry concentrate | 387 mg anthocyanidins/day | 30 mL blueberry concentrate (diluted to 240 mL total volume with tap water); 387 mg anthocyanidins/day | chronic: 12 weeks | N/A | n = 26 (12 blueberry, 14 PLA), older adults, mean age: blueberry group = 67.5 ± 0.9, PLA group = 69 ± 0.9 | ↑ significantly improves task-related brain activation and increases resting regional grey matter perfusion in the parietal and occipital lobes; ↔ nonsignificant effect on BDNF and hs-CRP | 1.5 T MRI scanner during numerical Stroop test to quantify task-related activation; Arterial Spin Labelling Magnetic Resonance Imaging (ASL MRI) technique to determine quantitative resting brain perfusion; blood parameters (BDNF, hs-CRP) |
| Huhn et al. (2018) [42] | Double-blind, randomized controlled trial | Resveratrol | 200 mg resveratrol/day | Two pills of 100 mg resveratrol per day (total daily dose/day = 200 mg/day) | chronic: 26 weeks | N/A | n = 60 (30 resveratrol group, 30 PLA), elderly participants, range age: 60–79 years | ↔ nonsignificant effect on hippocampus subfield volumes, mean weighted image diffusivity, and hippocampus connectivity; ↔ nonsignificant effect on BDNF, hs-CRP, TNF-α, and IL-6 | Anatomical MRI for hippocampal volumetry was acquired at a Siemens Magnetom 7 Tesla system; blood parameters (BDNF, hs-CRP, IL-6, and TNF-α) |
| Lamport et al. (2015) [30] | Randomized, counterbalanced double-blind, crossover trial | Cocoa flavanols | High flavanol drink (494 mg), low flavanols drink (29 mg) | 330 mL containing high or low flavanols content daily | Acute | 1 week | n = 18 (counterbalanced) older adults, mean age: 61 ± 5 years old (55–65 years) | ↑ significantly increases regional CBF in the anterior cingulate cortex and central opercular cortex | Arterial Spin Labelling Functional Magnetic Resonance Imaging (ASL fMRI) to assess resting regional perfusion |
| Marsh et al. (2017) [37] | Counterbalanced within-subject crossover design | Chocolate with a high concentration of polyphenols-rich cocoa | Total polyphenols: ≈85 mg: white chocolate, 200 mg: milk chocolate, 395 mg: dark chocolate | 84 g dark chocolate (80% cacao), 87 g milk chocolate (35% cacao), or 85 g white chocolate (0% cacao) per daily | Acute | 1 week | n = 12 (counterbalanced design), older women, mean age: 57.3 ± 5.3 y) | ↓ significantly decreases CBF responses (i.e., middle cerebral artery velocity and cerebrovascular conductance) during the cognitive tasks using milk and dark chocolate; ↔ nonsignificant effect on mean arterial pressure | Transcranial Doppler (TCD) (Spencer Technologies) to assess cerebral blood flow velocity (CBFv) responses to a computerized cognitive assessment battery (CogState) |
| Sorond et al. (2008) [45] | Randomized, double-blind, parallel arm trial | Cocoa flavanol drink (flavanol-rich cocoa (FRC) and flavanol-poor cocoa (FPC)) | 450 mg flavanol cocoa in each 450 mg FRC packet drink and 18.2 mg flavanol cocoa in each 450 mg FPC drink packet | 2 packets daily (900 mg/day) | 1 and 2 weeks | N/A | n = 21 (n of each arm: not mentioned), healthy elderly volunteers, mean age = 72 ± 6 years old, (59–83 years) | ↑ significantly increases mean Blood Flow Velocity (MFV) with 8% ± 4% during the first week and 10% ± 4% during the two weeks, ↔ nonsignificant effect on cerebrovascular resistance (CVR) and cerebral vasoreactivity (VR) | Transcranial Doppler (TCD) ultrasonography; outcome: Mean Blood Flow Velocity (MBFV), cerebrovascular resistance (CVR), and cerebral vasoreactivity (VR) in the middle cerebral artery (MCA) |
| Wightman et al. (2018) [28] | Double Blind, randomized, placebo controlled, parallel groups study | Polyphenol-rich Greek mountain tea (Sideritis scardica) | Total phenolic content = 6.25% of the 20% Greek mountain tee extract | 475 or 950 mg of Greek mountain tea daily | Acute and chronic (4 weeks) | N/A | n = 57 (n of each arm: not mentioned), older adults, mean age 60.3 years old | The acute ingestion of the Grek mountain tea during completion of cognitively demanding tasks: ↑ significantly improves oxygenated haemoglobin (HbO) and oxygen saturation (Ox%) in the prefrontal cortex using both intermediate (475 mg) and high dose (950 mg) compared to active Ginko control (240 mg), and ↑ significantly improves total (THb) and deoxygenated (Hb) haemoglobin only using the high dose (950 mg) compared to active Ginko control (240 mg); ↔ no significant effect of the chronic ingestion at day 28 | Near-Infrared Spectroscopy (NIRS) during completion of cognitive task to assess cerebral hemodynamics/blood flow including total hemoglobin (total-Hb), oxygenated hemoglobin (oxy-Hb), deoxygenated hemoglobin (deoxy-Hb), and oxygen saturation (Ox%) in the prefrontal cortex |
| Witte et al. (2014) [29] | Double blind, randomized, placebo controlled, parallel groups study | Resveratrol | Not mentioned | 200 mg/day | 26 weeks | N/A | n = 46 (23 resveratrol, 23 PLA), older female, mean age: resveratrol group = 65 ± 7 years old, PLA = 64 ± 5 years old | ↑significantly improves hippocampal functional connectivity (FC); ↔ nonsignificant effect on total gray matter volume or in the volume or microstructure of the hippocampus, ↔ nonsignificant effect on BDNF, Hs-CRP, and IL-6. | Neuroimaging (MRI 3 tesla) to assess volume, microstructure, and functional connectivity (FC) of the hippocampus; blood parameters (BDNF, hs-CRP, IL-6, and TNF-α) |
| Items | Antom et al. (2018) [40] | Bensalem et al. (2019) [41] | Bowtell et al. (2017) [31] | Gleason et al. (2009) [35] | Howes et al. (2004) [36] | Huhn et al. (2018) [42] | Kritz-Silverstein et al. (2003) [43] | Lamport et al. (2015) [30] | Marsh et al. (2017) [37] | Mastroiacovo et al. (2015) [26] | Mix and Crews (2000) [44] | Sorond et al. (2008) [45] | Whyte et al. (2018) [27] | Wightman et al. (2018) [28] | Witte et al. (2014) [29] | |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 11 | Eligibility criteria were specified. | + | + | + | + | + | + | + | + | + | + | + | + | + | + | + |
| 22 | Subjects were randomly allocated to groups (in a crossover study, subjects were randomly allocated an order in which treatments were received). | + | + | + | + | + | + | + | + | + | + | + | + | + | + | + |
| 33 | Allocation was concealed. | - | + | + | + | + | + | + | + | - | + | + | + | + | + | + |
| 44 | The groups were similar at baseline regarding the most important prognostic indicators. | + | + | + | + | + | + | + | + | + | + | + | + | + | + | + |
| 55 | There was blinding of all subjects. | + | + | + | + | + | + | + | + | + | + | + | + | + | + | + |
| 66 | There was blinding of all therapists who administered the therapy. | + | + | + | + | + | + | + | + | - | + | + | + | + | + | + |
| 77 | There was blinding of all assessors who measured at least one key outcome. | - | - | - | - | - | - | - | - | - | - | - | - | - | - | - |
| 88 | Measures of at least one key outcome were obtained from more than 85% of the subjects initially allocated to groups. | + | + | + | + | + | + | + | + | + | + | + | + | + | + | + |
| 99 | All subjects for whom outcome measures were available received the treatment or control condition as allocated or, where this was not the case, data for at least one key outcome was analysed by “intention to treat”. | + | + | + | + | + | + | + | + | + | + | + | + | + | + | + |
| 110 | The results of between-group statistical comparisons are reported for at least one key outcome. | + | + | + | + | + | + | + | + | + | + | + | + | + | + | + |
| 111 | The study provides both point measures and measures of variability for at least one key outcome. | + | + | + | + | + | + | + | + | + | + | + | + | + | + | + |
| Total score | 8 | 9 | 9 | 9 | 9 | 9 | 9 | 9 | 7 | 9 | 9 | 9 | 9 | 9 | 9 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ammar, A.; Trabelsi, K.; Müller, P.; Bouaziz, B.; Boukhris, O.; Glenn, J.M.; Bott, N.; Driss, T.; Chtourou, H.; Müller, N.; et al. The Effect of (Poly)phenol-Rich Interventions on Cognitive Functions and Neuroprotective Measures in Healthy Aging Adults: A Systematic Review and Meta-Analysis. J. Clin. Med. 2020, 9, 835. https://doi.org/10.3390/jcm9030835
Ammar A, Trabelsi K, Müller P, Bouaziz B, Boukhris O, Glenn JM, Bott N, Driss T, Chtourou H, Müller N, et al. The Effect of (Poly)phenol-Rich Interventions on Cognitive Functions and Neuroprotective Measures in Healthy Aging Adults: A Systematic Review and Meta-Analysis. Journal of Clinical Medicine. 2020; 9(3):835. https://doi.org/10.3390/jcm9030835
Chicago/Turabian StyleAmmar, Achraf, Khaled Trabelsi, Patrick Müller, Bassem Bouaziz, Omar Boukhris, Jordan M Glenn, Nick Bott, Tarak Driss, Hamdi Chtourou, Notger Müller, and et al. 2020. "The Effect of (Poly)phenol-Rich Interventions on Cognitive Functions and Neuroprotective Measures in Healthy Aging Adults: A Systematic Review and Meta-Analysis" Journal of Clinical Medicine 9, no. 3: 835. https://doi.org/10.3390/jcm9030835