Forecasting COVID-19-Associated Hospitalizations under Different Levels of Social Distancing in Lombardy and Emilia-Romagna, Northern Italy: Results from an Extended SEIR Compartmental Model

 , ,
, ,  ,
, 
Abstract
1. Introduction
2. Experimental Section
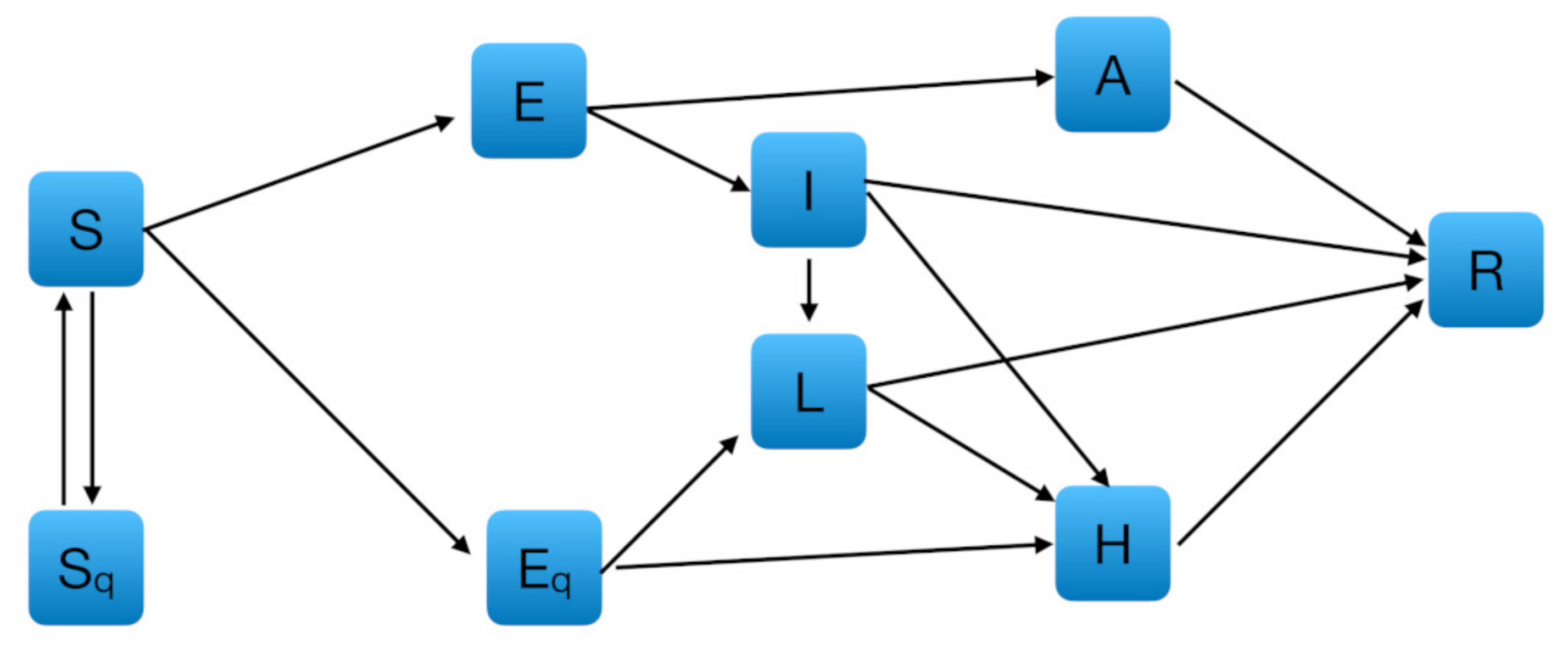
2.1. Model Specification
2.2. Formulation of the Model
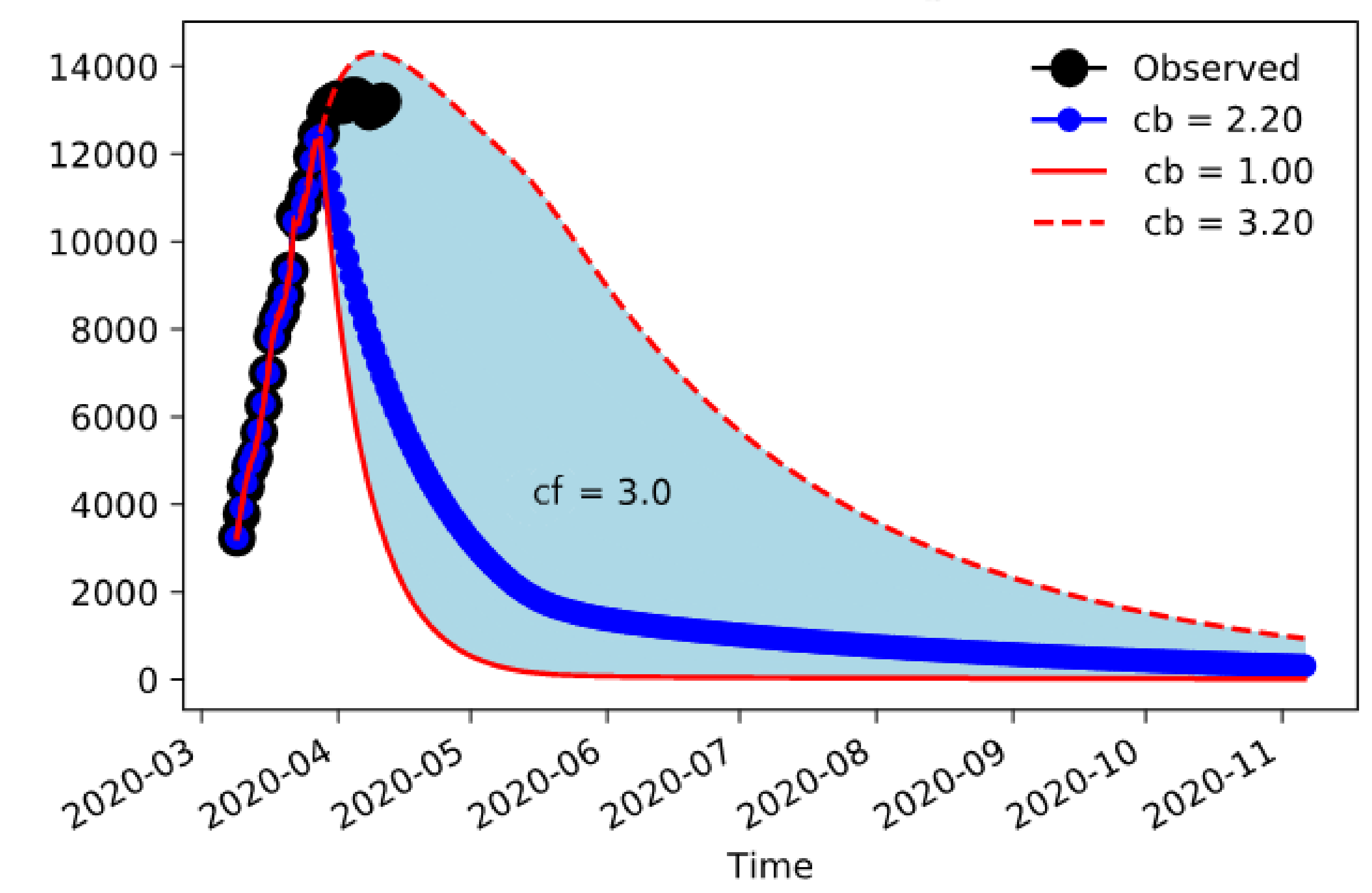
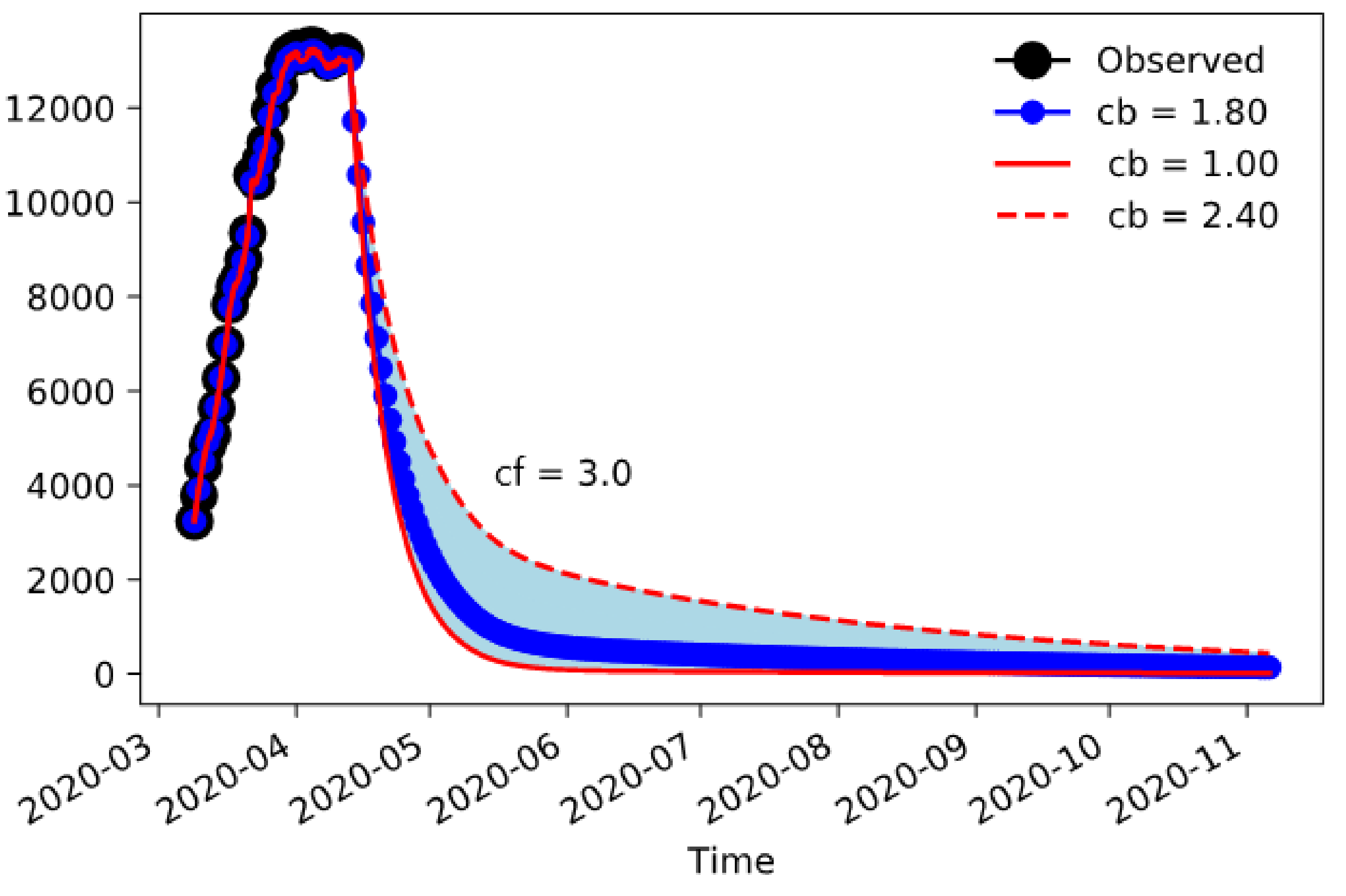
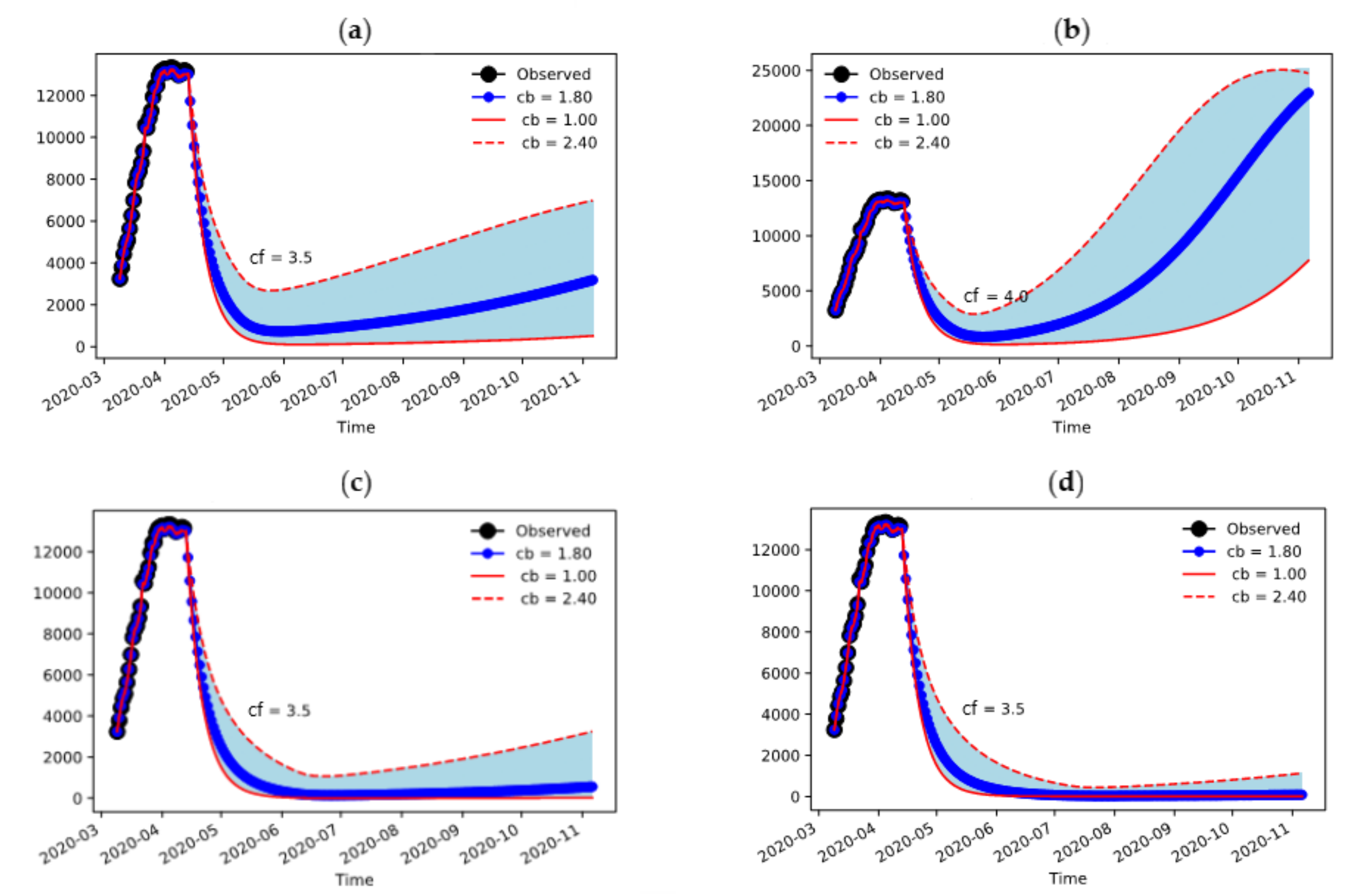
3. Results
Sensitivity Analysis on Initial Conditions and Parameters
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- Coronavirus Confirmed as Pandemic. Available online: https://www.bbc.com/news/world-51839944 (accessed on 17 April 2020).
- Wu, Z.; McGoogan, J.M. Characteristics of and Important Lessons from the Coronavirus Disease 2019 (COVID-19) Outbreak in China: Summary of a Report of 72314 Cases from the Chinese Center for Disease Control and Prevention. JAMA 2020, 323, 1239–1242. [Google Scholar] [CrossRef] [PubMed]
- Coronavirus Disease (COVID-19) Pandemic. Available online: https://www.who.int/emergencies/diseases/novel-coronavirus-2019 (accessed on 17 April 2020).
- Grasselli, G.; Zangrillo, A.; Zanella, A.; Antonelli, M.; Cabrini, L.; Castelli, A.; Cereda, D.; Coluccello, A.; Foti, G.; Fumagalli, R.; et al. Baseline Characteristics and Outcomes of 1591 Patients Infected With SARS-CoV-2 Admitted to ICUs of the Lombardy Region, Italy. JAMA 2020, 323, 1574–1581. [Google Scholar] [CrossRef] [PubMed]
- Onder, G.; Rezza, G.; Brusaferro, S. Case-Fatality Rate and Characteristics of Patients Dying in Relation to COVID-19 in Italy. JAMA 2020, in press. [Google Scholar] [CrossRef] [PubMed]
- Dati COVID-19 Italia. Available online: https://github.com/pcm-dpc/COVID-19/tree/master/schede-riepilogative (accessed on 17 April 2020).
- Presidenza del Consiglio dei Ministri. Ulteriori disposizioni attuative del decreto-legge 23 febbraio 2020, n. 6, recante misure urgenti in materia di contenimento e gestione dell’emergenza epidemiologica da COVID-19. (20A01522). Gazz. Uff. Della Repubb. Ital. 2020, 59, 3–6. [Google Scholar]
- Zhou, F.; Yu, T.; Du, R.; Fan, G.; Liu, Y.; Liu, Z.; Xiang, J.; Wang, Y.; Song, B.; Gu, X.; et al. Clinical course and risk factors for mortality of adult inpatients with COVID-19 in Wuhan, China: A retrospective cohort study. Lancet 2020, 395, 1054–1062. [Google Scholar] [CrossRef]
- Coronavirus: Corsa Contro il Tempo Regioni per Terapie Intensive. Available online: http://www.regioni.it/news/2020/03/20/coronavirus-corsa-contro-il-tempo-regioni-per-terapie-intensive-607711/ (accessed on 17 April 2020).
- Hethcote, H.W. The Mathematics of infectious diseases. SIAM Rev. 2000, 42, 599–653. [Google Scholar] [CrossRef]
- Walters, C.E.; Meslé, M.M.I.; Hall, I.M. Modelling the global spread of diseases : A review of current practice and capability. Epidemics 2018, 25, 1–8. [Google Scholar] [CrossRef]
- Kermack, W.; McKendrick, A. Contributions to the mathematical theory of epidemics—I. Bull. Math. Biol. 1991, 53, 33–55. [Google Scholar] [CrossRef]
- Apolloni, A.; Poletto, C.; Ramasco, J.J.; Jensen, P.; Colizza, V. Metapopulation epidemic models with heterogeneous mixing and travel behaviour. Theor. Biol. Med. Model. 2014, 11, 3. [Google Scholar] [CrossRef]
- Vaidya, N.K.; Morgan, M.; Jones, T.; Miller, L.; Lapin, S.; Schwartz, E.J. Modelling the epidemic spread of an H1N1 influenza outbreak in a rural university town. Epidemiol. Infect. 2015, 143, 1610–1620. [Google Scholar] [CrossRef]
- Chen, T.M.; Rui, J.; Wang, Q.P.; Zhao, Z.Y.; Cui, J.A.; Yin, L. A mathematical model for simulating the phase-based transmissibility of a novel coronavirus. Infect. Dis. Poverty 2020, 9, 24. [Google Scholar] [CrossRef] [PubMed]
- Cooley, P.; Brown, S.; Cajka, J.; Chasteen, B.; Ganapathi, L.; Grefenstette, J.; Hollingsworth, C.R.; Lee, B.Y.; Levine, B.; Wheaton, W.D.; et al. The role of subway travel in an influenza epidemic: A New York city simulation. J. Urban Health 2011, 88, 982–995. [Google Scholar] [CrossRef] [PubMed]
- Ferguson, N.M.; Cummings, D.A.T.; Fraser, C.; Cajka, J.C.; Cooley, P.C.; Burke, D.S. Strategies for mitigating an influenza pandemic. Nature 2006, 442, 448–452. [Google Scholar] [CrossRef]
- Shi, P.; Keskinocak, P.; Swann, J.L.; Lee, B.Y. The impact of mass gatherings and holiday traveling on the course of an influenza pandemic: A computational model. BMC Public Health 2010, 10, 778. [Google Scholar] [CrossRef] [PubMed]
- Meyers, L.A.; Pourbohloul, B.; Newman, M.E.J.; Skowronski, D.M.; Brunham, R.C. Network theory and SARS: Predicting outbreak diversity. J. Theor. Biol. 2005, 232, 71–81. [Google Scholar] [CrossRef] [PubMed]
- Hunter, E.; MacNamee, B.; Kelleher, J.D. A comparison of agent-based models and equation based models for infectious disease epidemiology. CEUR Workshop Proc. 2018, 2259, 33–44. [Google Scholar]
- Ajelli, M.; Gonçalves, B.; Balcan, D.; Colizza, V.; Hu, H.; Ramasco, J.J.; Merler, S.; Vespignani, A. Comparing large-scale computational approaches to epidemic modeling: Agent-based versus structured metapopulation models. BMC Infect. Dis. 2010, 10, 190. [Google Scholar] [CrossRef]
- Tang, B.; Wang, X.; Li, Q.; Bragazzi, N.L.; Tang, S.; Xiao, Y.; Wu, J. Estimation of the Transmission Risk of the 2019-nCoV and Its Implication for Public Health Interventions. J. Clin. Med. 2020, 9, 462. [Google Scholar] [CrossRef]
- Tang, B.; Bragazzi, N.L.; Li, Q.; Tang, S.; Xiao, Y.; Wu, J. An updated estimation of the risk of transmission of the novel coronavirus (2019-nCov). Infect. Dis. Model. 2020, 5, 248–255. [Google Scholar] [CrossRef]
- Lauer, S.A.; Grantz, K.H.; Bi, Q.; Jones, F.K.; Zheng, Q.; Meredith, H.R.; Azman, A.S.; Reich, N.G.; Lessler, J. The Incubation Period of Coronavirus Disease 2019 (COVID-19) From Publicly Reported Confirmed Cases: Estimation and Application. Ann. Intern. Med. 2020, in press. [Google Scholar] [CrossRef]
- Hoke, J.E.; Anthes, R.A. The Initialization of Numerical Models by a Dynamic-Initialization Technique. Mon. Weather Rev. 1976, 104, 1551–1556. [Google Scholar] [CrossRef]
- Lei, L.; Hacker, J.P. Nudging, ensemble, and nudging ensembles for data assimilation in the presence of model error. Mon. Weather Rev. 2015, 143, 2600–2610. [Google Scholar] [CrossRef]
- Così il Coronavirus ha Fatto Collassare il Sistema Sanitario Lombardo. Available online: https://www.ilsecoloxix.it/italia-mondo/cronaca/2020/03/29/news/cosi-il-coronavirus-ha-fatto-collassare-il-sistema-sanitario-lombardo-1.38653328 (accessed on 17 April 2020).
- Ricci, A.; Longo, F. Modelli innovativi a confronto: Lombardia ed Emilia-Romagna. Salute e Territorio 2012, 201, 317–328. [Google Scholar]
- Regions for Health Network. Emilia-Romagna Region, Italy. Available online: http://www.euro.who.int/__data/assets/pdf_file/0005/373388/rhn-emilia-romagna-eng.pdf?ua=1 (accessed on 17 April 2020).
- Analisi dei Modelli Organizzativi di Risposta al Covid-19. Focus su Lombardia, Veneto, Emilia-Romagna, Piemonte e Lazio. Available online: https://altems.unicatt.it/altems-ALTEMS-COVID19_IstantReport2-report.pdf (accessed on 17 April 2020).






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Parameter | Value | Definition |
|---|---|---|
| 2.1011 × 10–8 | Probability of transmission per contact | |
| 1.8887 × 10–7 | Quarantined rate of exposed individuals | |
| 1/7 | Transition rate of exposed individuals to the infected class | |
| 1/14 | Rate at which the quarantined uninfected contacts are released into the wider community | |
| 0.86834 | Probability of having symptoms among infected individuals | |
| 0.1259 | Transition rate of quarantined exposed individuals to the hospitalized infected class | |
| 0.33029 | Recovery rate of symptomatic infected individuals | |
| 0.13978 | Recovery rate of asymptomatic infected individuals | |
| 0.11624 | Recovery rate of hospitalized infected individuals | |
| 1.7826 × 10–5 | Disease induced death rate | |
| 0.05 | Infected rate of asymptomatic/symptomatic | |
| 0.2000 | Rate of home isolation for infected individuals | |
| 0.2000 | Rate of home isolation for quarantined exposed individuals | |
| 0.13978 | Recovery rate for isolated infected individuals | |
| 0.2000 | Hospitalization rate for isolated infected individuals |
| Definition | Prevalent Cases | Source/Calculation | |
|---|---|---|---|
| Lombardy | Emilia-Romagna | ||
| Resident on 31 October 2019 (P) | 10,085,021 | 4,468,023 | Istat estimate |
| Deaths (D) | 333 | 70 | Civil protection |
| Hospitalized (H) | 3242 | 666 | Civil protection |
| Isolated infected (L) | 1248 | 620 | Civil protection |
| Known infected (H + L + D) | 4823 | 1356 | Civil protection |
| Undetected infected (A + I) | 48,230 | 13,560 | (H + L + D) × 10 a |
| Undetected asymptomatic infected (A) | 32,153 | 9040 | (A + I) × 2/3 b |
| Undetected symptomatic infected (I) | 16,077 | 4520 | (A + I) × 1/3 |
| Tests (T) | 20,135 | 4906 | Civil protection |
| Quarantined (Q) | 15,312 | 3550 | T − (H + L+ D) |
| Quarantined exposed (Eq) | 24 | 6 | Q × 0.0016 c |
| Quarantined susceptible (Sq) | 15,288 | 3544 | Q × 0.9984 c |
| Unknown exposed (E) | 2212 | 513 | Eq × 90.277 c |
| Recovered (R) | 646 | 30 | Civil protection |
| Susceptible (S) | 10,013,798 | 4,449,014 | P – Q – E – H – L –D – A – I – R |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Reno, C.; Lenzi, J.; Navarra, A.; Barelli, E.; Gori, D.; Lanza, A.; Valentini, R.; Tang, B.; Fantini, M.P. Forecasting COVID-19-Associated Hospitalizations under Different Levels of Social Distancing in Lombardy and Emilia-Romagna, Northern Italy: Results from an Extended SEIR Compartmental Model. J. Clin. Med. 2020, 9, 1492. https://doi.org/10.3390/jcm9051492
Reno C, Lenzi J, Navarra A, Barelli E, Gori D, Lanza A, Valentini R, Tang B, Fantini MP. Forecasting COVID-19-Associated Hospitalizations under Different Levels of Social Distancing in Lombardy and Emilia-Romagna, Northern Italy: Results from an Extended SEIR Compartmental Model. Journal of Clinical Medicine. 2020; 9(5):1492. https://doi.org/10.3390/jcm9051492
Chicago/Turabian StyleReno, Chiara, Jacopo Lenzi, Antonio Navarra, Eleonora Barelli, Davide Gori, Alessandro Lanza, Riccardo Valentini, Biao Tang, and Maria Pia Fantini. 2020. "Forecasting COVID-19-Associated Hospitalizations under Different Levels of Social Distancing in Lombardy and Emilia-Romagna, Northern Italy: Results from an Extended SEIR Compartmental Model" Journal of Clinical Medicine 9, no. 5: 1492. https://doi.org/10.3390/jcm9051492
APA StyleReno, C., Lenzi, J., Navarra, A., Barelli, E., Gori, D., Lanza, A., Valentini, R., Tang, B., & Fantini, M. P. (2020). Forecasting COVID-19-Associated Hospitalizations under Different Levels of Social Distancing in Lombardy and Emilia-Romagna, Northern Italy: Results from an Extended SEIR Compartmental Model. Journal of Clinical Medicine, 9(5), 1492. https://doi.org/10.3390/jcm9051492