
Access to Human Health Benefits of Forests in Rural Low and Middle-Income Countries: A Literature Review and Conceptual Framework

1
Duke University Marine Lab, Nicholas School of the Environment, Duke University, Beaufort, NC 28516, USA
2
School of the Environment, University of Toronto, Toronto, ON M5S 3E8, Canada
Challenges 2024, 15(1), 12; https://doi.org/10.3390/challe15010012
Submission received: 31 January 2024
/
Revised: 22 February 2024
/
Accepted: 28 February 2024
/
Published: 29 February 2024
(This article belongs to the Section Planetary Health)
{kind=link}
{kind=link}
Abstract
:Forests are increasingly recognized for their beneficial roles in human health. However, there is a debate on how forest health benefits can be accessed equitably, particularly by vulnerable forest-dependent rural communities in low- and middle-income countries (LMICs). Access to forest health benefits is determined by a range of interconnected means, including property rights, as well as natural, physical, human, social, and financial capital. This paper presents a literature review of the roles of means of access in shaping human health effects of forests. Evidence suggests that variations in these means of access are associated with varying ability to access forest health benefits. However, existing evidence is thin, mixed, and weak. A conceptual model is then developed to provide a framework for understanding how means of access moderate the effects of forests on health in rural LMICs to guide the generation of strong evidence. The multiple interconnected factors moderating the health effects of forests at the core of the conceptual framework promote the multisectoral and transdisciplinary approaches needed to enhance equitable access to forest health benefits.
1. Introduction
Forests have been increasingly recognized for their beneficial contribution to human health [1], in addition to their established roles in biodiversity conservation [2], climate change mitigation [3], and poverty alleviation [4]. Though forests are linked to some negative health outcomes, the effects of forests on human health are overwhelmingly beneficial [5]. Existing evidence, however, predominantly focuses on the psychological and physiological health benefits of recreational exposure to or experience of forests or greenspaces in urban communities in high-income countries. Evidence from rural low- and middle-income countries (LMICs) is scarce [5]. Yet, rural communities in LMICs are highly dependent on health benefits from natural resources because of limited access to health services and infrastructure [6]. Furthermore, the rates of forest degradation and deforestation are high in the rural areas of LMICs [7]. There is therefore a debate on how such communities can sustainably and equitably derive or enhance forest health benefits. The mere availability of forest resources does not necessarily translate into beneficial human health outcomes. Access to forest health benefits (e.g., forest food, improved water quality) is a requisite for these resources to have beneficial health impacts. To contribute to the debate, this paper discusses a constellation of interconnected factors that influence access to forest health benefits in rural communities in LMICs.
Access is defined as the “ability to derive benefits from things” [8]. There are many studies researching factors determining access to health benefits of forests and urban greenspaces in high-income countries. Examples of such factors include distance to forests or greenspaces, weather, safety, occupation, lifestyle, time availability, and relatedness to nature [9,10,11]. While there may be cases where some of these factors can also determine access to forest health benefits in LMICs (e.g., in urban areas [12]), conclusions from studies in high-income countries cannot be easily extended to rural communities in LMICs because of differences in social-ecological contexts [13]. In rural LMICs, factors determining access to forest benefits include means, such as property rights [14] and capital (natural, physical, human, social, financial) [15,16,17]. Property rights are well-acknowledged means to gain, maintain, or control access to forest benefits. However, property rights alone do not guarantee access. Through negotiation, cooperation, competition, or conflict, people who have no property rights can still have access to forest benefits [18]. Other contextual factors, such as natural, physical, human, social, and financial capital, mediate or operate parallel to property rights to constrain or enable people to derive benefits from forest resources [15,16,17]. While the roles of these means of access (property rights and capital) in shaping human wellbeing benefits from forests are relatively well characterized in rural LMICs, human health is rarely considered as an outcome.
The paucity of evidence on how means of access alter the effects of forests on human health in rural LMIC context limits the application of forest-based interventions involving property rights or capital as nature-based solutions in public health. Such evidence is needed to design forest conservation programs that will improve human health outcomes for some of the world’s most vulnerable communities highly dependent on rapidly shrinking forest resources. A conceptual model that provides a framework for understanding how means of access (property rights and capital) shape people’s ability to derive health forest benefits is therefore needed. A conceptual framework should also provide guidance on how to generate strong evidence on how forests and means of access interact to affect human health outcomes. This paper presents such a conceptual framework based on a review of the current state of knowledge on property rights and capital as means of access to forest health benefits in the rural communities of LMICs and a discussion of existing conceptual frameworks linking forests and human health. The findings of the review are first summarized. The paper then discusses existing conceptual frameworks and describes the newly developed one. Last, future research needs are highlighted, and the paper concludes with policy implications of the roles of property rights and capital in strengthening people’s ability to derive forest health benefits.
2. Literature Review: Property Rights and Natural, Physical, Human, Social and Financial Capital as Means of Access to Forest Health Benefits in Rural LMICs
This review built on a series of workshops by the Global Forest Expert Panel (GFEP) on Forests and Human Health organized by the International Union of Forestry Research Organizations (IUFRO) in 2021 and 2022 [5]. It is specifically based on the section about the management of forest access in the fifth chapter of the GFEP report [5]. The literature discussed in this article was identified through two systematic reviews on the impacts of forest-based and forest property rights interventions on social outcomes [14,19]. Studies reporting nutritional and health-related outcomes were specifically selected. Workshop discussions involving the 44 scientists of the GFEP on Forests and Human Health from diverse backgrounds (forestry, ecology, landscape design, psychology, medicine, epidemiology, and public health) provided additional relevant studies; 10 independent experts who had reviewed a draft of the GFEP report were also consulted [5].
2.1. Property Rights
Rights can be understood as claims to benefits that are acknowledged and supported by society through law, custom, or convention [8]. Securing the property rights of local communities to forest resources matters for ethical reasons, as these communities have often customarily owned these resources for many generations and their wellbeing and way of life depend on access to them [20]. Furthermore, secure property rights can empower local communities to make their own long-term forest management decisions, which are tailored to local needs and circumstances, locally supported, and thus more likely to benefit both community and forest wellbeing [20]. In the context of forest health benefits, property rights represent one of the means that ensure local communities have direct access to health-related forest products, such as forest foods and medicinal plants, as well as timber and non-timber products that are sources of income that people can then use for health care.
Yet, data from 33 LMICs show that only 24.1% of forest areas are legally owned by local communities and indigenous peoples [21]. Ownership grants access control to local communities and indigenous peoples, i.e., they can mediate or exclude others’ access to forest resources [18]. Local forest owners also have rights to due process and compensation in case of conflicts [21]. An additional 4.0% of the 33 LMICs’ forest areas are designated for local communities and indigenous people, where their rights can range from the use of forest resources to the control of access to these resources [21]. The majority (63.7%) of forests in LMICs are still owned and administered by governments [21].
Where local communities do not have legal ownership of forests, they often contest forests through customary ownership [21]. Such overlap of legal (government) and customary (community) ownership can result in access ambiguity that, in turn, leads to conflicts [8]. Moreover, whenever local communities have no legal ownership, their access to forest resources, including those associated with health benefits, remains insecure, as the government, which legally owns forests, is the ultimate access mediator, adjudicator, and power holder [8].
Of particular interest is the continuing expansion of protected areas for biodiversity conservation that are often administered by governments. Approximately 18% of the world’s forests come within the boundaries of legally established protected areas [22]. Furthermore, the Global Biodiversity Framework (GBF) adopted by the 15th Conference of Parties to the United Nations Convention on Biological Diversity includes a target (Target 3) to protect 30% of the world’s land area by 2030 [23]. Protected areas can have beneficial effects on health outcomes by delivering ecosystem services of direct (e.g., forest food, water purification, medicinal plants) or indirect (e.g., forest income) relevance to human health that would have been lost without protection. Protected areas can also bring new livelihood opportunities (e.g., tourism-related employment) that can be used to support health outcomes [24]. However, displacements of local communities and restrictions of access to forest resources imposed by the establishment of protected areas could counter these potential benefits [24]. While the majority of the protected areas established during the recent decades allow multiple uses of forest resources (categories V–VI in the International Union for Conservation of Nature (IUCN) protected area categorization), access to resources within many of these protected areas is still contested by local communities [25]. Additionally, there are still many protected areas where access to forest resources is strictly limited (IUCN categories I–IV).
Evidence suggests that more extensive property rights are more likely to be associated with improved socio-economic outcomes—including health benefits—than more limited rights [14]. For example, devolution of forest management rights (rights to make rules for internal use and to transform forest resources by making improvements) to communities in Bhutan was associated with increased calorie intake by individuals in participating households, protecting them against the health risk of malnutrition [26]. In Namibia, people living in communal conservancies—areas under customary property rights, where rights to benefit from natural resources are devolved to local communities—had higher ownership of bed nets (for malaria prevention) than people in non-conservancy comparison areas [27]. There, however, was no significant difference between the two groups (conservancy vs. non-conservancy) in the prevalence of diarrheal diseases [27]. Communities around the Loita forest in Kenya, which is managed under traditional property rights in which local communities are the owners of forests and have the right to exclude others, perceived that the control of access to forest resources granted to the communities improved their health status [28]. In the context of protected areas, a study covering 34 LMICs indicated that forest use rights in multiple-use protected areas (IUCN categories V–VI) were associated with stronger child growth (higher height-for-age) [29]. In Uganda, restricted rights to forest resources by the Budongo and Rwensama Forest Reserves were linked to psychological distress among households bordering the reserves through the negative effects of the restrictions on material wealth and food security [30].
However, there are also studies indicating stronger associations between enhanced health benefits and limited rights than extensive rights. In Tanzania, for example, Pailler et al. [31] detected significant positive associations between community forest management rights and child nutritional status (height-for-age, weight-for-age), where rights grant more limited control of access. No significant association was detected where the management rights allow for more extensive control of access [31]. In the same country, local communities perceived improvement in access to forest medicinal plants, and hence health, where there were more limited rights, but not where there were more extensive rights [32]. The inconsistent findings on the associations between variation in forest property rights (limited vs. extensive) and health benefits might be explained by the fact that, though property rights are important, they represent only one means by which to derive forest health benefits. Other contextual factors act in parallel or interact with property rights to determine access to these benefits [8].
2.2. Contextual Factors Shaping Access to Forest Health Benefits: Capital
Access to forest health benefits is enhanced or constrained by a wide range of socio-economic contexts within which access is sought. These contextual factors complement or conflict with each other and property rights to shape people’s ability to derive forest health benefits. These contextual factors can be categorized into the different types of capital (natural, physical, human, social, and financial) defined in the Sustainable (Rural) Livelihoods Framework [33,34] and used to organize factors that constrain or enhance access to benefits from environmental resources [15,16,17]. The Sustainable Livelihood Framework has been widely used in development research and policy [35].
2.2.1. Natural Capital
Natural capital comprises the natural resources people depend on for their livelihoods [17]. The conditions of forest resources (here, the natural capital) shape people’s ability to access the health benefits they provide. The number of forests and their configuration across landscapes were significantly associated with diet quality, a key determinant of nutritional status, in Ethiopia, Malawi, Nigeria, Tanzania, and Uganda [36]. Another example in which forest conditions can affect access to forest health benefits is in areas where women are the primary collectors of forest products such as firewood and fodder [37]. In Indian villages, women used to walk 1–2 km every day to gather sufficient firewood for cooking. After forest degradation, they needed to walk 8–10 km for the same purpose [38]. Such a shift in time and energy allocation by women, who are also the primary household caregivers, takes their time and energy away from food preparation, more careful child feeding behaviors, income generation, and health care, and thus can impact the health of household members [39]. As an example for infectious diseases, Rasolofoson et al. [40] suggest that good upstream forest conditions can render chlorination more effective at reducing diarrhea prevalence in Haiti and Honduras. They indicated that when forests in upstream areas of watersheds are degraded, the quality of downstream raw water can become poor, which limits the effectiveness of chlorination in dealing with diarrhea [40]. Preservation of forests through the establishment of protected areas in upstream watersheds was associated with a reduced downstream prevalence of diarrhea on the island of Flores in Indonesia [41].
2.2.2. Physical Capital
Physical capital includes infrastructure that people need or tools and equipment that they use to make a living [17]. Roads, for example, can shape the relationship between forests and human health in different ways. Roads open ways for alternative food and health services that can reduce communities’ dependence on forest resources [6]. Roads can also enhance access to markets and equipment, which facilitates the transformation of forest benefits into health benefits. For example, a study covering 27 LMICs suggests that living near roads supports forest-dependent communities in converting forest benefits to nutritional benefits [42]. However, road development is also a driver of deforestation and forest degradation [43] and thus can affect human health through the impact of these roads on forests (natural capital). The positive and negative effects on human health of the change in relationships between local communities and forests caused by roads can be illustrated by the construction of the Interoceanic Highway in the Peruvian Amazon, which increased food diversity and healthcare access, but reduced access to natural resources and hunting, and increased infectious disease (dengue) and consumption of junk food [44,45].
Tools and equipment can enhance access to forest health benefits. For example, in the northeastern Democratic Republic of Congo, where hunting is carried out primarily with shotguns, ownership of such tools enabled richer community members to derive health benefits from bushmeat consumption [46]. Evidence suggests that bushmeat consumption is associated with the reduced prevalence of nutritional deficiencies (e.g., anemia) [47]. Forests can also benefit human health through conservation programs that build physical capital to incentivize local communities to conserve forests. In the Gunung Palung National Park in Indonesia, for example, a program that established a health clinic and offered discounts to communities conditional on the reduction of illegal logging saw an increase in clinic usage [48].
The role of physical capital in enhancing access to the health benefits of forests can also be illustrated by the multiple-barrier approach to clean drinking water provision. From source watersheds to water distribution, multiple consecutive barriers to pollutants and contaminants are needed to ensure safe drinking water [49]. By filtering raw water, forested watersheds can act as early barriers, increasing the effectiveness and lowering the cost of clean drinking water provision [50]. Additional infrastructure is, however, needed at point-of-use or source (e.g., point-of-use chlorination, water treatment plants) to enhance the benefits of water filtration by forested watersheds in providing clean drinking water and preventing waterborne disease. For example, chlorination was still needed to reduce the prevalence of diarrhea in Haiti and Honduras, but the presence of upstream forests could increase its effectiveness [40].
2.2.3. Human Capital
Key indicators of human capital include skills, education, knowledge, and health [17]. The level of education has been positively associated with the effects of forests on diet quality, as more educated people may be more diet-conscious and, thus, more likely able to translate forest benefits into a nutritious diet [42]. Women’s nutrition knowledge is of high significance for forest nutritional benefits, given that decisions regarding household food use and practices are mostly made by women [51]. Traditional knowledge of forest medicinal herbs is a type of human capital commonly used in traditional medicine practice, particularly in forest-dependent communities [28,32]. Forests—through conservation activities involving education, training, and skills development—can also generate health benefits. A conservation project that involved education on family planning was associated with increased contraceptive use among women in a national park in Madagascar [52]. In Cameroon, the development of skills needed for indigenous tree domestication and agroforestry was associated with higher consumption of nutritious fruits and use of medicinal plants, which in turn was reported to result in a reduction in the frequency of sickness and hospitalization [53].
2.2.4. Social Capital
Social capital is composed of the network of social relationships people have, including relationships with either more powerful individuals or with others like themselves, or the membership of groups or organizations [54]. Privileged relationships with authoritative individuals or institutions that design, implement, or enforce forest use rules can strongly influence who benefits from forest resources [8]. In Madagascar, for example, there are reported cases in which community elites, thanks to better skills and education (human capital) that are required for the establishment of legally recognized community forest management, have developed relationships with state authorities and implementing organizations. Such relationships have led to rules favoring these community elites, allowing them to capture forest benefits and other resources (e.g., support for livelihood alternatives) [55,56]. Group membership can also affect the distribution of benefits from forest resources. Some persons are subject to rules, while others may be exempt because of their group membership [8]. For example, in cases of participatory forest management in Ethiopia, membership of forest user groups, which is required for livestock grazing and timber harvesting, was associated with increased livestock assets and income. Non-members, who lost access to forest products and grazing, experienced income shocks [57], which can have repercussions on household health care.
Markets, as exchange relations [8], are a type of social capital. The ability to derive cash income from forest resources depends on access to markets. The collection and sale of forest products can provide support, especially for those who lack the means to engage in other livelihood activities (women and the most disadvantaged members of a community) [58]. Cash income in turn can be used for health care. Forest-based programs involving the improvement of market access, such as forest certification, showed positive or neutral associations with socio-economic outcomes [59]. Specifically, a study in Indonesia suggested that forest certification was associated with reduced firewood dependence, air pollution, respiratory infections, and malnutrition while having no relationship with the number of healthcare facilities [60]. The creation of producer business groups that linked smallholder indigenous fruit farmers to wholesale buyers was reported to result in farmers’ income increase in Kenya and Uganda [61].
2.2.5. Financial Capital
Financial capital includes cash income and remittances, credit, and savings in kind and cash [54]. In lowland forests in Bolivia and mangrove forests in Bangladesh, financial capital was positively correlated with the extraction of forest products, given that wealthier households (i.e., with higher financial capital) were able to invest more in such extraction [17,62]. The status and power afforded by financial capital could be used to acquire other means of access [8]. Financial capital can be used to purchase property rights, pay for rents or access fees, tools or equipment (physical capital) for resource extraction, acquire education and knowledge (human capital), and invest in relationships with or buy the influence of people with authority (social capital). A study in the Democratic Republic of Congo, for example, reported that poor households consumed less bushmeat and fish because they could not afford the high-capital tools (e.g., shotguns and nets) necessary to exploit these resources [46]. In a community forest management case in Uganda, wealthy households saw significant gains in income from forests because they were able to extract and commercialize illegally harvested timber by offering bribes to forest officials responsible for monitoring and rule enforcement [63].
3. Conceptual Framework: Roles of Means of Access in Moderating the Effects of Forests on Human Health Outcomes
The review presented in the preceding sections indicates that variations in means of access (property rights and capital) are associated with a varying ability to derive forest health benefits. These associations are, however, mixed, with increasing levels of means of access both positively and negatively associated with forest effects on human health outcomes. A conceptual framework for understanding how means of access shape the human health effects of forests is therefore needed to support the design of configurations of means of access that will enhance the effects of forests on health outcomes. A conceptual framework is also useful to help researchers and practitioners generate strong evidence on how means of access moderate the effects of forests on health outcomes.
3.1. Existing Forest–Health Conceptual Frameworks
To date, there is no conceptual framework that specifically describes factors which modify the health effects of forests in rural communities in LMICs that are highly dependent on forest resources. To develop such a framework, existing forest–health conceptual frameworks are reviewed to identify gaps and justify the need for a new conceptual framework. This section presents a brief discussion of those frameworks and how to expand upon them.
The International Union of Forest Research Organizations (IUFRO) and the World Wildlife Fund (WWF) have each developed a forest–health conceptual framework with global scope [1,5]. Both of these frameworks distinguish between three groups of beneficiaries of forest health benefits: forest-dependent, rural, and urban communities. Such distinction recognizes that different groups benefit from forests in different ways. While these global frameworks provide general tools for analyzing forest–health relationships, due to harmonization across contexts (e.g., high-income countries and LMICs), they are less sensitive to context-specific aspects and factors that shape forest–health relationships. There is therefore a need to refine these conceptual frameworks when applied to high-income countries or LMICs.
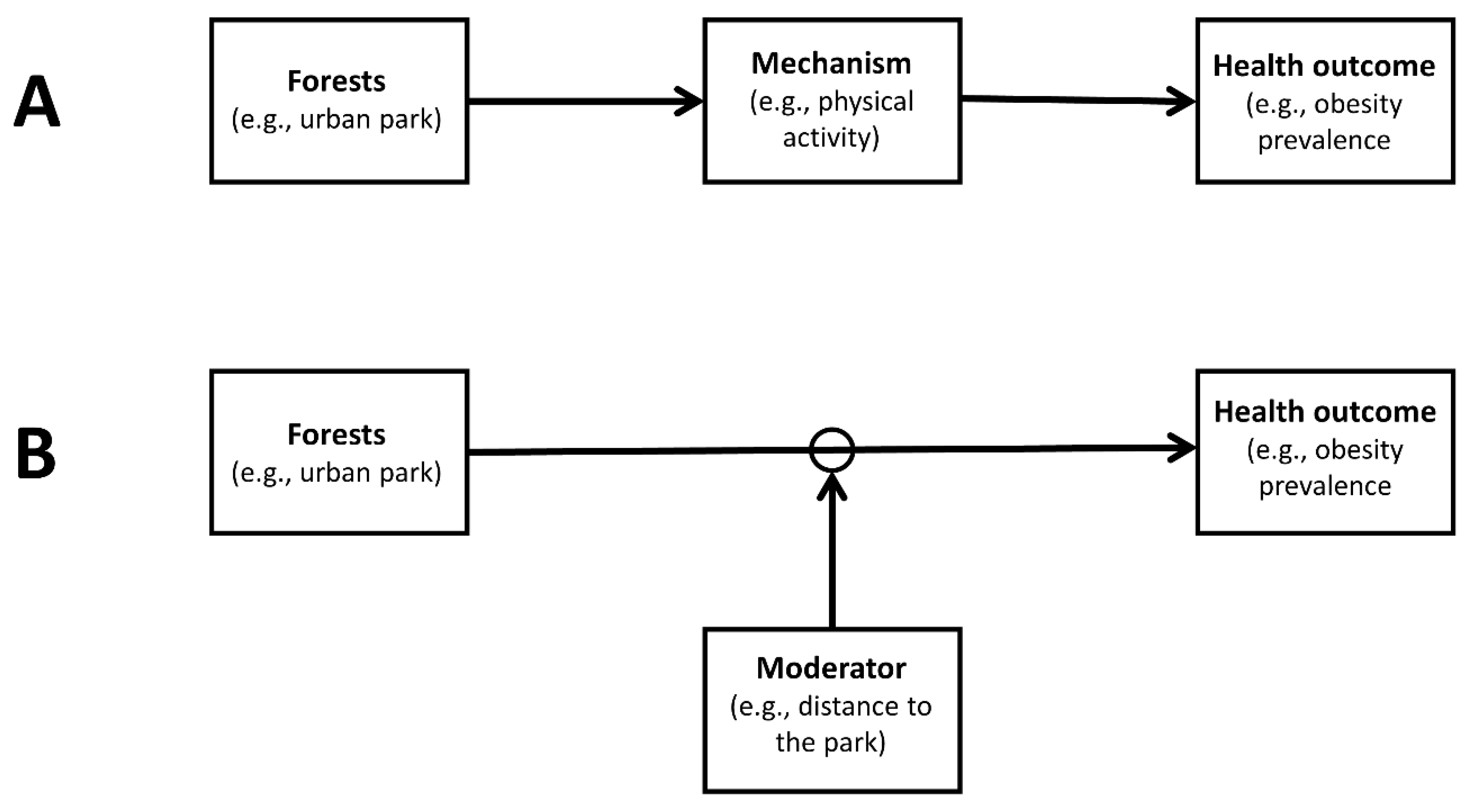
In high-income countries, many conceptual frameworks distinguish between two types of variables that can explain the effects of forests and urban greenspaces on human health outcomes: mechanisms (also known as mediators) and moderators (e.g., [9,10,11]). A mechanism is an intermediate outcome that lies on the causal pathway between forests and a human health outcome. Once affected by forests, a mechanism affects the health outcome (Figure 1A). For example, urban greenspaces can lead to increased physical activity, which in turn reduces obesity [64]. Physical activity is therefore a mechanism through which urban greenspaces affect obesity. A moderator, however, does not lie on a causal pathway but alters the magnitude or direction of the effects of forests on a health outcome (Figure 1B). For example, Coombes et al. [65] reported that people living closer to greenspaces were more likely to do more physical activity and less likely to be obese, suggesting that distance between homes and greenspaces can be a moderator of the effects of greenspaces on obesity. Differences between mechanisms and moderators have critical implications for the choices of study designs [66].
However, the conceptual frameworks on the effects of forests and urban greenspaces on human health outcomes in high-income countries are of limited use for understanding the links between forests and human health in rural communities in LMICs [13]. They mainly drew from studies on the health benefits of recreational exposure to or experience of forests or urban greenspaces, including opportunities for increased physical activities and psychological benefits of engaging with the natural environment. Relevant moderators include distance to forests or greenspaces, weather, safety, occupation, lifestyle, time availability, and relatedness to nature [9,10,11]. There can be overlaps between forest health benefits and moderators in high-income countries and LMICs (e.g., in urban areas [12]). However, rural communities in LMICs depend directly on forest resources for their livelihood, health services, and cultural and spiritual practices [67]. The literature reviewed in previous sections therefore shows that studies in rural communities in LMICs tend to focus more on forest health benefits provided through ecosystem services (e.g., water purification, forest foods, medicinal plants) or conservation initiatives designed to incentivize local communities to conserve forests. Relevant moderators include means of access, such as property rights [14], as well as natural, physical, human, social, and financial capital [15,17]. There is therefore a need for a conceptual framework that specifically accounts for a rural LMIC context.
Finally, a number of conceptual frameworks for analyzing the relationships between ecosystems and human wellbeing are more sensitive to an LMIC context (e.g., [16,68,69,70]). These frameworks point to the importance of property rights or capital in shaping people’s access to ecosystem services or nature’s benefits to people. However, they do not differentiate between mechanisms and moderators and do not specifically focus on human health as an outcome.
3.2. A New Conceptual Framework for Understanding Access to Forest Health Benefits in Rural LMICs
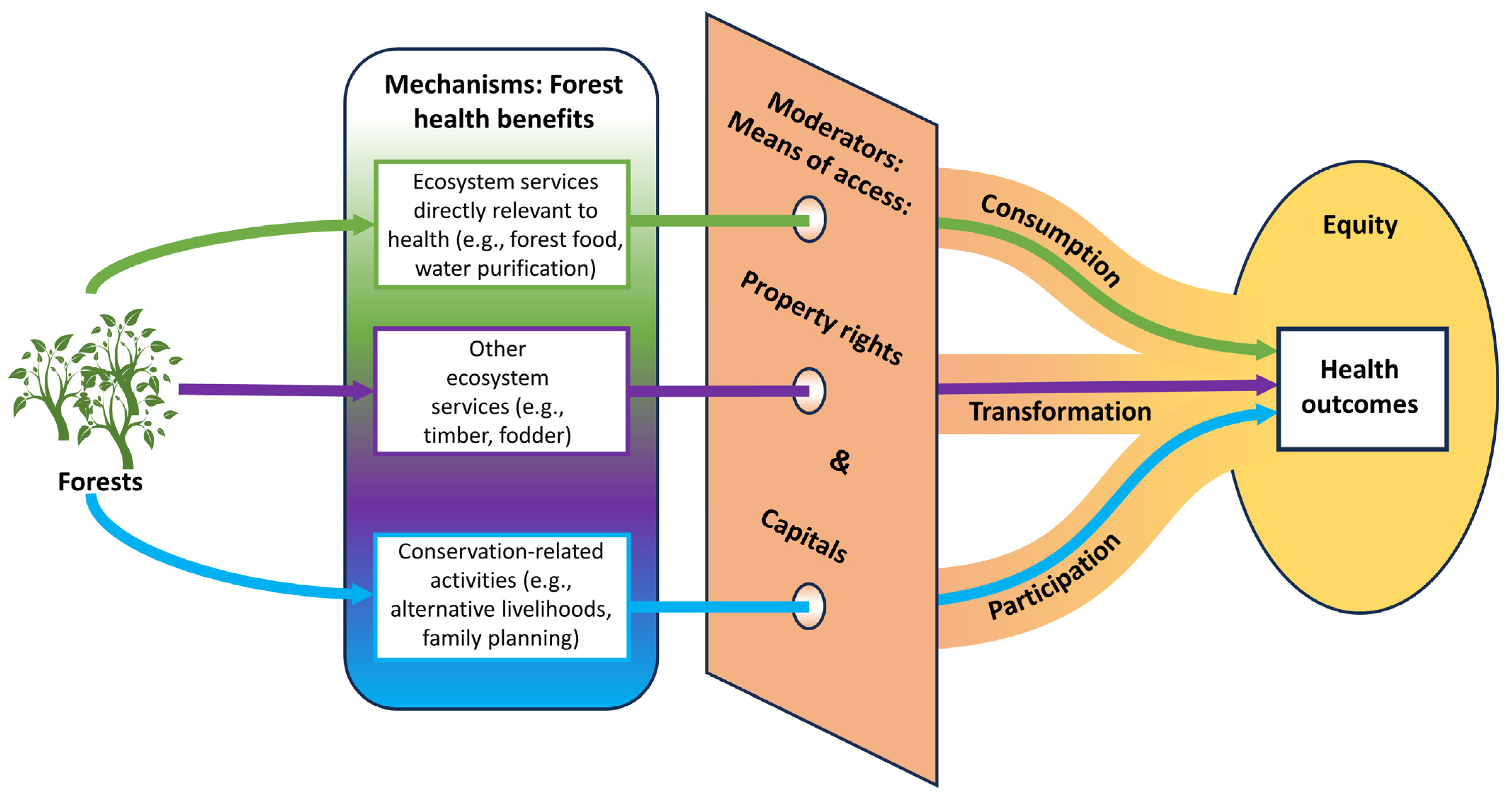
Drawing elements from the aforementioned conceptual frameworks, a new conceptual model (Figure 2) has been developed to provide a framework for understanding how means of access (property rights and capital) moderate the effects of forests on human health outcomes in the rural communities of LMICs. Based on the IUFRO and WWF global frameworks’ categorization of beneficiaries of forest health benefits [1,5], rural communities are the focus of the newly developed conceptual framework. Distinctions between mechanisms and moderators are also emphasized following the conceptual frameworks on the effects of forests and urban greenspaces on human health outcomes in high-income countries [9,10,11]. The importance of means of access in ecosystem –wellbeing frameworks [16,68,69,70] informs the description of property rights and capital as moderators of the effects of forests on human health outcomes in LMICs. The conceptual framework depicted in Figure 2 is therefore more specific and targeted than the IUFRO and WWF global frameworks and the ecosystem–wellbeing frameworks by focusing on rural communities in LMICs and human health outcomes. Nevertheless, it advances the understanding of overlooked forest–health relationships among some of the world’s most vulnerable communities lacking vital health services and infrastructure and thus highly dependent on forest resources.
3.2.1. Mechanisms through Which Forests Affect Human Health Outcomes
Mechanisms in the pathways between forests and human health can be intertwined and work together in different ways [9]. Presenting such complexity is not the primary focus of the conceptual framework in Figure 2. Other forest–health conceptual frameworks (and related frameworks: biodiversity–health, nature–health) discuss these complex interactions between mechanisms (e.g., [1,5,9,10,71,72,73]). Here, the mechanisms are grouped into three categories corresponding to three different ways in which means of access moderate the effects of forests on health outcomes (see section on moderators below).
Forests can affect health outcomes through the provision of ecosystem services of direct relevance to human health (e.g., nutritious forest food [42], medicinal plants [32], and water purification [40]) (Figure 2). Forest ecosystem services that are not directly relevant to human health can also be transformed to impact health outcomes (Figure 2). For example, timber products can be sold for cash income [63], which can then be used for health care. Finally, forests can affect health outcomes through conservation initiatives intended to foster conservation-related behavior (Figure 2). While some of these initiatives are directly linked to human health (e.g., health education [52], health clinics [48]), for others the link to human health is indirect (e.g., alternative livelihoods [74]).
3.2.2. Moderators of the Effects of Forests on Human Health Outcomes: Means of Access
In the causal inference literature, a moderator alters the magnitude or direction of the effect of a causal variable (e.g., forests) on an outcome variable (e.g., a human health outcome) by regulating (constraining or enhancing) the different mechanisms in the pathways between these variables [66]. Means of access to forest health benefits (property rights and capital) moderate the effects of forests on human health outcomes by regulating the consumption or transformation of ecosystem services, and participation in conservation activities (Figure 2). By depicting how moderators regulate mechanisms to deliver outcomes, the conceptual framework in Figure 2 can support the identification of mechanisms to be strengthened to enhance the health effects of forests, given a configuration of means of access. Conversely, the framework can also support the design of means of access configurations needed to promote specific mechanisms that will lead to improved health outcomes.
3.2.3. Equity of the Health Effects of Forests
Because of the regulating roles of means of access, the magnitude or direction of the effects of forests on human health outcomes varies as a function of their levels. Such variation or heterogeneity has equity implications (Figure 2). Vulnerable rural people or communities in LMICs often have limited means (rights and capital) to derive benefits from forest resources [14]. However, they are highly dependent on these resources for critical services directly (e.g., forest foods, water purification) and indirectly (e.g., forest income) relevant to human health because they lack essential infrastructure and markets for the provisioning of health-related services [6,75]. Health benefits from forest resources are therefore inequitably distributed, with studies reporting more benefits to wealthier, better-educated, or male-headed households [26,31,32,42,46].
3.2.4. Health Outcomes
Health is defined as “a state of complete physical, mental, and social wellbeing and not merely the absence of disease or infirmity” [76]. From the literature reviewed in previous sections, most of the studies in rural communities in LMICs examine health outcomes related to forest health benefits (e.g., water purification, forest foods) that fill the gap caused by the lack of health services and infrastructure (e.g., water treatment plants, markets) prevalent in these communities or provided through forest conservation programs. Examples of such health outcomes include prevalence of diarrheal diseases [40,41] and nutritional status (e.g., height-for-age [29,31], anemia [47]). Much of the literature, however, uses proximate determinants of health as outcomes (e.g., calorie intake [26], diet quality [36,42], ownership of bed nets [27], women’s time allocation [39], health clinic visit [48], contraceptive use [52], and the use of medicinal plants [53]). There is a dearth of research investigating how forests and means of access interact to affect psychological or mental health outcomes in rural LMICs [13]. Perceived health conditions are also used as outcomes [28,32].
4. Research Needs
In line with the scarcity of evidence about the effects of forests on human health in LMICs [5], the evidence on the roles of means of access (property rights and capital) in shaping these effects is thin [14,19]. In addition to generating more general evidence on the effects of forests on human health in LMICs to raise awareness and motivate policies, there is a need for more research producing actionable knowledge on factors that ensure that forest health benefits are enhanced and accessed equitably by vulnerable communities. The conceptual framework presented here can guide researchers and practitioners to identify configurations of property rights, and natural, physical, human, social, and financial capital that strengthen pathways to enhanced and equitable human health outcomes from forests.
The major challenge in establishing the causal relationship between a causal variable and an outcome variable is the elimination of rival explanations of the observed pattern between these two variables [77]. Many of the studies reviewed in this paper do not adequately address rival explanations [14,19]. The observed patterns in much of the existing evidence on the roles of means of access in shaping the health effects of forests are therefore difficult to interpret. Approaches to address rival explanations include experimental and rigorous quasi-experimental study designs [77]. Such study designs are requisite to strengthen the evidence on the roles of means of access in shaping the effects of forests on human health outcomes. These study designs seek to identify what would have happened without intervention (i.e., the counterfactual). The impact of the intervention is then the difference between observed outcomes exposed to the intervention and counterfactual outcomes [77].
Significant advances have been made in strengthening the evidence on the impacts of conflicts (e.g., civil wars, civil conflicts) on nutrition-related outcomes [78]. Contributing to these advances is the ability of conflict–health scholars to apply rigorous quasi-experimental study designs to publicly available large survey datasets, such as the Demographic and Health Surveys (DHS) data administered by the U.S. Agency for International Development (USAID) (e.g., [79,80,81,82,83,84,85,86,87,88,89]). There are few studies attempting to apply rigorous quasi-experimental designs to the DHS data to examine the impacts of forest-related interventions on health-related outcomes [27,29,31,90]. Drawing from the conflict–health scholarship, specifically how they use the DHS data to address the rival explanations of the observed pattern between conflicts and nutritional outcomes, would be a way to strengthen the evidence on the health impacts of forest-based interventions involving property rights or capital.
In published studies, differences between mechanisms and moderators are often not clear. They are conflated. For example, studies that use forest attributes, property rights, and capital among the explanatory variables of regressions often interpret some of the variables’ coefficients as mechanism (or mediating) effects and others as moderating effects. Different empirical designs are, however, needed to examine the effects of mechanisms and moderators [66]. To select appropriate empirical designs, data, and methods, researchers must clearly distinguish between mechanisms and moderators [66]. The conceptual framework presented here can help researchers to differentiate mechanisms from mediators and how they interact to affect health outcomes.
To promote the application of forest-based interventions involving property rights or capital as nature-based solutions in public health, more studies that look at actual health outcomes are needed (e.g., prevalence of a disease). Proximate determinants of health (e.g., diet quality, health clinic visits), which are preponderant outcomes in existing studies, can indicate health outcomes. However, relationships between proximate determinants of health and actual health outcomes can be affected by many factors. Effects on proximate outcomes do not necessarily result in effects on human health outcomes. For example, an improved child diet due to enhanced access to forest resources will not necessarily result in improved linear growth (height-for-age). Other factors such as infectious disease (e.g., diarrhea), water safety, sanitation, and hygiene also contribute to a child’s linear growth [91]. We therefore need more research on actual human health outcomes.
Last, to advance a more holistic approach to human health in forest-dependent rural communities in LMICs, further research on the effects of the interaction of forests and means of access on mental health is needed. There generally is a lack of research on the relationships between natural systems and mental health in the LMIC context [13,67]. For example, a systematic review of studies on mental health and wellbeing outcomes of climate change mitigation and adaptation strategies in LMICs only includes fifteen studies [92], of which only one investigates the psychological health effects of a forest-related intervention in a rural setting [93]. Research on the effects of urban forests and greenspaces on mental health is catching up, particularly in upper-middle-income countries [12]. Research on forest-dependent rural communities lags behind [13]. However, these communities do not only depend on forests for their livelihood and health services (e.g., water purification, forest foods, medicinal plants), but also attach personal, societal, historical, cultural, and spiritual meanings to forests [94]. Accordingly, access to forest resources can affect the mental health of forest-dependent rural communities in LMICs, particularly given that changes in people’s immediate environment can cause psychological distress [95]. There is therefore a need for further equitable research that not only promotes the understanding of the mental health effects of forests in rural communities in LMICs, but also informs policy and action regarding factors that enhance the mental health benefits of forests in such communities.
5. Conclusions: Policy Implications
The paucity and weakness of existing evidence constrain attempts to draw generalizable conclusions about the roles of means of access (property rights, capital) in shaping the effects of forests on human health outcomes in the rural communities of LMICs. Policy recommendations are therefore difficult to formulate. However, policies, regulations, legislation, and interventions aimed at improving access to forest health benefits need to consider a wide range of interconnected factors including property rights, and natural, physical, human, social, and financial capital. Efforts to address just one or a few of these factors do not guarantee the enhancement of the effects of forests on health outcomes and could even result in tradeoffs and unintended consequences, including disproportionate adverse impacts on the most vulnerable groups and unsustainable use of forest resources. There is therefore a need to develop integrative and cross-sectoral approaches (combining, for example, environment, public health, economics, education, culture, and law enforcement) that not only enhance people’s ability to derive forest health benefits but also ensure that these benefits are equitably distributed. Transdisciplinary approaches involving research organizations, local communities, and local, regional, and national governments will also develop a better understanding of how these different factors interact with forests to affect human health outcomes and its translation into effective policy. The conceptual framework provided can contribute to promoting such multisectoral and transdisciplinary approaches by providing the understanding of how a wide range of interconnected factors shape forest–health relationships.
Funding
This work was supported by the International Union of Forest Research Organizations (IUFRO).
Acknowledgments
I thank the International Union of Forestry Research Organizations (IUFRO) for organizing the workshops upon which this work has built. I am also grateful to the members of the Global Forest Expert Panel (GFEP) on Forests and Human Health for their input. I thank Siddharth Sareen for reviewing a draft of the manuscript.
Conflicts of Interest
The author declares no conflicts of interest.
References
- Beatty, C.R.; Stevenson, M.; Pacheco, P.; Terrana, A.; Folse, M.; Cody, A. The Vitality of Forests: Illustrating the Evidence Connecting Forests and Human Health; World Wildlife Fund: Washington, DC, USA, 2022; p. 54. [Google Scholar]
- Butchart, S.H.M.; Walpole, M.; Collen, B.; van Strien, A.; Scharlemann, J.P.W.; Almond, R.E.A.; Baillie, J.E.M.; Bomhard, B.; Brown, C.; Bruno, J.; et al. Global Biodiversity: Indicators of Recent Declines. Science 2010, 328, 1164–1168. [Google Scholar] [CrossRef]
- Mitchard, E.T.A. The Tropical Forest Carbon Cycle and Climate Change. Nature 2018, 559, 527–534. [Google Scholar] [CrossRef]
- Razafindratsima, O.H.; Kamoto, J.F.M.; Sills, E.O.; Mutta, D.N.; Song, C.; Kabwe, G.; Castle, S.E.; Kristjanson, P.M.; Ryan, C.M.; Brockhaus, M.; et al. Reviewing the Evidence on the Roles of Forests and Tree-Based Systems in Poverty Dynamics. For. Policy Econ. 2021, 131, 102576. [Google Scholar] [CrossRef]
- Konijnendijk, C.; Devkota, D.; Mansourian, S.; Wildburger, C. Forests and Trees for Human Health: Pathways, Impacts, Challenges and Response Options. A Global Assessment Report; IUFRO World Series Volume 41; International Union of Forest Research Organizations (IUFRO): Vienna, Austria, 2023; p. 232. [Google Scholar]
- Myers, S.S.; Gaffikin, L.; Golden, C.D.; Ostfeld, R.S.; Redford, K.H.; Ricketts, T.H.; Turner, W.R.; Osofsky, S.A. Human Health Impacts of Ecosystem Alteration. Proc. Natl. Acad. Sci. USA 2013, 110, 18753–18760. [Google Scholar] [CrossRef]
- Vancutsem, C.; Achard, F.; Pekel, J.-F.; Vieilledent, G.; Carboni, S.; Simonetti, D.; Gallego, J.; Aragão, L.E.O.C.; Nasi, R. Long-Term (1990–2019) Monitoring of Forest Cover Changes in the Humid Tropics. Sci. Adv. 2021, 7, eabe1603. [Google Scholar] [CrossRef] [PubMed]
- Ribot, J.C.; Peluso, N.L. A Theory of Access. Rural Sociol. 2003, 68, 153–181. [Google Scholar] [CrossRef]
- Hartig, T.; Mitchell, R.; de Vries, S.; Frumkin, H. Nature and Health. Annu. Rev. Public Health 2014, 35, 207–228. [Google Scholar] [CrossRef]
- Lachowycz, K.; Jones, A.P. Towards a Better Understanding of the Relationship between Greenspace and Health: Development of a Theoretical Framework. Landsc. Urban Plan. 2013, 118, 62–69. [Google Scholar] [CrossRef]
- Zhang, L.; Tan, P.Y.; Diehl, J.A. A Conceptual Framework for Studying Urban Green Spaces Effects on Health. J. Urban Ecol. 2017, 3, jux015. [Google Scholar] [CrossRef]
- Nawrath, M.; Guenat, S.; Elsey, H.; Dallimer, M. Exploring Uncharted Territory: Do Urban Greenspaces Support Mental Health in Low- and Middle-Income Countries? Environ. Res. 2021, 194, 110625. [Google Scholar] [CrossRef]
- Pienkowski, T.; Keane, A.; Kinyanda, E.; Knizek, B.L.; Asiimwe, C.; Muhanguzi, G.; Milner-Gulland, E.J. Exploring Links between Socio-Ecological Systems and Psychological Distress: A Case Study in Rural Uganda. Oryx 2024, Accepted. [Google Scholar] [CrossRef]
- Miller, D.; Rana, P.; Nakamura, K.; Irwin, S.; Cheng, S.; Ahlroth, S.; Perge, E. A Global Review of the Impact of Forest Property Rights Interventions on Poverty. Glob. Environ. Chang. 2021, 66, 102218. [Google Scholar] [CrossRef]
- Costanza, R.; de Groot, R.; Sutton, P.; van der Ploeg, S.; Anderson, S.J.; Kubiszewski, I.; Farber, S.; Turner, R.K. Changes in the Global Value of Ecosystem Services. Glob. Environ. Chang. 2014, 26, 152–158. [Google Scholar] [CrossRef]
- Fisher, J.A.; Patenaude, G.; Giri, K.; Lewis, K.; Meir, P.; Pinho, P.; Rounsevell, M.D.A.; Williams, M. Understanding the Relationships between Ecosystem Services and Poverty Alleviation: A Conceptual Framework. Ecosyst. Serv. 2014, 7, 34–45. [Google Scholar] [CrossRef]
- Kibria, A.S.M.G.; Costanza, R.; Groves, C.; Behie, A.M. The Interactions between Livelihood Capitals and Access of Local Communities to the Forest Provisioning Services of the Sundarbans Mangrove Forest, Bangladesh. Ecosyst. Serv. 2018, 32, 41–49. [Google Scholar] [CrossRef]
- Peluso, N.L.; Ribot, J. Postscript: A Theory of Access Revisited. Soc. Nat. Resour. 2020, 33, 300–306. [Google Scholar] [CrossRef]
- Cheng, S.H.; MacLeod, K.; Ahlroth, S.; Onder, S.; Perge, E.; Shyamsundar, P.; Rana, P.; Garside, R.; Kristjanson, P.; McKinnon, M.C.; et al. A Systematic Map of Evidence on the Contribution of Forests to Poverty Alleviation. Environ. Evid. 2019, 8, 3. [Google Scholar] [CrossRef]
- Mollett, S.; Kepe, T. Land Rights, Biodiversity Conservation and Justice: Rethinking Parks and People; Routledge: London, UK, 2018; ISBN 978-0-367-82086-2. [Google Scholar]
- Ginsburg, C.; Keene, S. At a Crossroads: Consequential Trends in Recognition of Community-Based Forest Tenure from 2002–2017. China Econ. J. 2020, 13, 223–248. [Google Scholar] [CrossRef]
- FAO; UNEP. The State of the World’s Forests: Forests, Biodiversity and People; FAO: Rome, Italy, 2020; ISBN 978-92-5-132419-6. [Google Scholar]
- Gurney, G.G.; Adams, V.M.; Álvarez-Romero, J.G.; Claudet, J. Area-Based Conservation: Taking Stock and Looking Ahead. One Earth 2023, 6, 98–104. [Google Scholar] [CrossRef]
- Terraube, J.; Fernández-Llamazares, Á.; Cabeza, M. The Role of Protected Areas in Supporting Human Health: A Call to Broaden the Assessment of Conservation Outcomes. Curr. Opin. Environ. Sustain. 2017, 25, 50–58. [Google Scholar] [CrossRef]
- Sunderland, T.C.; Vasquez, W. Forest Conservation, Rights, and Diets: Untangling the Issues. Front. For. Glob. Chang. 2020, 3, 29. [Google Scholar] [CrossRef]
- Rahut, D.B.; Ali, A.; Behera, B. Household Participation and Effects of Community Forest Management on Income and Poverty Levels: Empirical Evidence from Bhutan. For. Policy Econ. 2015, 61, 20–29. [Google Scholar] [CrossRef]
- Riehl, B.; Zerriffi, H.; Naidoo, R. Effects of Community-Based Natural Resource Management on Household Welfare in Namibia. PLoS ONE 2015, 10, e0125531. [Google Scholar] [CrossRef]
- Mbuvi, M.T.E.; Musyoki, J.K.; Ongugo, P.O. Equity Mechanisms in Traditional Forest Management Systems: A Case Study of Loita Forest in Kenya. J. Sustain. For. 2015, 34, 380–405. [Google Scholar] [CrossRef]
- Naidoo, R.; Gerkey, D.; Hole, D.; Pfaff, A.; Ellis, A.M.; Golden, C.D.; Herrera, D.; Johnson, K.; Mulligan, M.; Ricketts, T.H.; et al. Evaluating the Impacts of Protected Areas on Human Well-Being across the Developing World. Sci. Adv. 2019, 5, eaav3006. [Google Scholar] [CrossRef]
- Pienkowski, T.; Keane, A.; Kinyanda, E.; Asiimwe, C.; Milner-Gulland, E.J. Predicting the Impacts of Land Management for Sustainable Development on Depression Risk in a Ugandan Case Study. Sci. Rep. 2022, 12, 11607. [Google Scholar] [CrossRef]
- Pailler, S.; Naidoo, R.; Burgess, N.D.; Freeman, O.E.; Fisher, B. Impacts of Community-Based Natural Resource Management on Wealth, Food Security and Child Health in Tanzania. PLoS ONE 2015, 10, e0133252. [Google Scholar] [CrossRef]
- Vyamana, V.G. Participatory Forest Management in the Eastern Arc Mountains of Tanzania: Who Benefits? Int. For. Rev. 2009, 11, 239–253. [Google Scholar] [CrossRef]
- Scoones, I. Sustainable Rural Livelihoods: A Framework for Analysis; Institute of Development Studies (IDS): Brighton, UK, 1998; p. 22. [Google Scholar]
- Carney, D. Sustainable Rural Livelihoods: What Contribution Can We Make? Department for International Development: London, UK, 1998. [Google Scholar]
- Natarajan, N.; Newsham, A.; Rigg, J.; Suhardiman, D. A Sustainable Livelihoods Framework for the 21st Century. World Dev. 2022, 155, 105898. [Google Scholar] [CrossRef]
- Rasmussen, L.V.; Fagan, M.E.; Ickowitz, A.; Wood, S.L.R.; Kennedy, G.; Powell, B.; Baudron, F.; Gergel, S.; Jung, S.; Smithwick, E.A.H.; et al. Forest Pattern, Not Just Amount, Influences Dietary Quality in Five African Countries. Glob. Food Secur. 2020, 25, 100331. [Google Scholar] [CrossRef]
- Sunderland, T.; Achdiawan, R.; Angelsen, A.; Babigumira, R.; Ickowitz, A.; Paumgarten, F.; Reyes-García, V.; Shively, G. Challenging Perceptions about Men, Women, and Forest Product Use: A Global Comparative Study. World Dev. 2014, 64, S56–S66. [Google Scholar] [CrossRef]
- Wan, M.; Colfer, C.J.P.; Powell, B. Forests, Women and Health: Opportunities and Challenges for Conservation. Int. For. Rev. 2011, 13, 369–387. [Google Scholar] [CrossRef]
- Johnson, K.B.; Jacob, A.; Brown, M.E. Forest Cover Associated with Improved Child Health and Nutrition: Evidence from the Malawi Demographic and Health Survey and Satellite Data. Glob. Health Sci. Pract. 2013, 1, 237–248. [Google Scholar] [CrossRef]
- Rasolofoson, R.A.; Ricketts, T.H.; Johnson, K.B.; Jacob, A.; Fisher, B. Forests Moderate the Effectiveness of Water Treatment at Reducing Childhood Diarrhea. Environ. Res. Lett. 2021, 16, 064035. [Google Scholar] [CrossRef]
- Pattanayak, S.K.; Wendland, K.J. Nature’s Care: Diarrhea, Watershed Protection, and Biodiversity Conservation in Flores, Indonesia. Biodivers. Conserv. 2007, 16, 2801–2819. [Google Scholar] [CrossRef]
- Rasolofoson, R.A.; Hanauer, M.M.; Pappinen, A.; Fisher, B.; Ricketts, T.H. Impacts of Forests on Children’s Diet in Rural Areas across 27 Developing Countries. Sci. Adv. 2018, 4, eaat2853. [Google Scholar] [CrossRef]
- Busch, J.; Ferretti-Gallon, K. What Drives Deforestation and What Stops It? A Meta-Analysis. Rev. Environ. Econ. Policy 2017, 11, 3–23. [Google Scholar] [CrossRef]
- Riley-Powell, A.R.; Lee, G.O.; Naik, N.S.; Jensen, K.E.; O’Neal, C.; Salmón-Mulanovich, G.; Hartinger, S.M.; Bausch, D.G.; Paz-Soldan, V.A. The Impact of Road Construction on Subjective Well-Being in Communities in Madre de Dios, Peru. Int. J. Environ. Res. Public Health 2018, 15, 1271. [Google Scholar] [CrossRef]
- Tallman, P.S.; Riley-Powell, A.R.; Schwarz, L.; Salmón-Mulanovich, G.; Southgate, T.; Pace, C.; Valdés-Velásquez, A.; Hartinger, S.M.; Paz-Soldán, V.A.; Lee, G.O. Ecosyndemics: The Potential Synergistic Health Impacts of Highways and Dams in the Amazon. Soc. Sci. Med. 2022, 295, 113037. [Google Scholar] [CrossRef]
- de Merode, E.; Homewood, K.; Cowlishaw, G. The Value of Bushmeat and Other Wild Foods to Rural Households Living in Extreme Poverty in Democratic Republic of Congo. Biol. Conserv. 2004, 118, 573–581. [Google Scholar] [CrossRef]
- Golden, C.D.; Fernald, L.C.H.; Brashares, J.S.; Rasolofoniaina, B.J.R.; Kremen, C. Benefits of Wildlife Consumption to Child Nutrition in a Biodiversity Hotspot. Proc. Natl. Acad. Sci. USA 2011, 108, 19653–19656. [Google Scholar] [CrossRef] [PubMed]
- Jones, I.J.; MacDonald, A.J.; Hopkins, S.R.; Lund, A.J.; Liu, Z.Y.-C.; Fawzi, N.I.; Purba, M.P.; Fankhauser, K.; Chamberlin, A.J.; Nirmala, M.; et al. Improving Rural Health Care Reduces Illegal Logging and Conserves Carbon in a Tropical Forest. Proc. Natl. Acad. Sci. USA 2020, 117, 28515–28524. [Google Scholar] [CrossRef] [PubMed]
- Ernst, C.; Gullick, R.; Nixon, K. Conserving Forests to Protect Water. Opflow 2004, 30, 1–7. [Google Scholar] [CrossRef]
- Cunha, D.G.F.; Sabogal-Paz, L.P.; Dodds, W.K. Land Use Influence on Raw Surface Water Quality and Treatment Costs for Drinking Supply in São Paulo State (Brazil). Ecol. Eng. 2016, 94, 516–524. [Google Scholar] [CrossRef]
- Vira, B.; Wildburger, C.; Mansourian, S. Forests, Trees and Landscapes for Food Security and Nutrition: A Global Assessment Report; International Union of Forest Research Organizations (IUFRO): Vienna, Austria, 2015; ISBN 978-3-902762-40-5. [Google Scholar]
- Korhonen, K.; Rahkonen, O.; Hemminki, E. Implications of Integrated Nature Conservation for Human Reproductive Health: A Case Study from Ranomafana National Park, Madagascar. Dev. South. Afr. 2004, 21, 603–621. [Google Scholar] [CrossRef]
- Tchoundjeu, Z.; Degrande, A.; Leakey, R.R.; Nimino, G.; Kemajou, E.; Asaah, E.; Facheux, C.; Mbile, P.; Mbosso, C.; Sado, T.; et al. Impacts of Participatory Tree Domestication on Farmer Livelihoods in West and Central Africa. For. Trees Livelihoods 2010, 19, 217–234. [Google Scholar] [CrossRef]
- Serrat, O. The Sustainable Livelihoods Approach. In Knowledge Solutions: Tools, Methods, and Approaches to Drive Organizational Performance; Serrat, O., Ed.; Springer: Singapore, 2017; pp. 21–26. ISBN 978-981-10-0983-9. [Google Scholar]
- Pollini, J.; Lassoie, J.P. Trapping Farmer Communities within Global Environmental Regimes: The Case of the GELOSE Legislation in Madagascar. Soc. Nat. Resour. 2011, 24, 814–830. [Google Scholar] [CrossRef]
- Rasolofoson, R.A.; Ferraro, P.J.; Ruta, G.; Rasamoelina, M.S.; Randriankolona, P.L.; Larsen, H.O.; Jones, J.P.G. Impact of Community Forest Management on Human Economic Well-Being across Madagascar. Conserv. Lett. 2017, 10, 346–353. [Google Scholar] [CrossRef]
- Ameha, A.; Nielsen, O.J.; Larsen, H.O. Impacts of Access and Benefit Sharing on Livelihoods and Forest: Case of Participatory Forest Management in Ethiopia. Ecol. Econ. 2014, 97, 162–171. [Google Scholar] [CrossRef]
- Vinceti, B.; Termote, C.; Ickowitz, A.; Powell, B.; Kehlenbeck, K.; Hunter, D. The Contribution of Forests and Trees to Sustainable Diets. Sustainability 2013, 5, 4797–4824. [Google Scholar] [CrossRef]
- Burivalova, Z.; Allnutt, T.F.; Rademacher, D.; Schlemm, A.; Wilcove, D.S.; Butler, R.A. What Works in Tropical Forest Conservation, and What Does Not: Effectiveness of Four Strategies in Terms of Environmental, Social, and Economic Outcomes. Conserv. Sci. Pract. 2019, 1, e28. [Google Scholar] [CrossRef]
- Miteva, D.A.; Loucks, C.J.; Pattanayak, S.K. Social and Environmental Impacts of Forest Management Certification in Indonesia. PLoS ONE 2015, 10, e0129675. [Google Scholar] [CrossRef]
- Jamnadass, R.H.; Dawson, I.K.; Franzel, S.; Leakey, R.R.B.; Mithöfer, D.; Akinnifesi, F.K.; Tchoundjeu, Z. Improving Livelihoods and Nutrition in Sub-Saharan Africa through the Promotion of Indigenous and Exotic Fruit Production in Smallholders’ Agroforestry Systems: A Review. Int. For. Rev. 2011, 13, 338–354. [Google Scholar] [CrossRef]
- Uberhuaga, P.; Smith-Hall, C.; Helles, F. Forest Income and Dependency in Lowland Bolivia. Environ. Dev. Sustain. 2012, 14, 3–23. [Google Scholar] [CrossRef]
- Jagger, P. Forest Incomes after Uganda’s Forest Sector Reform: Are the Rural Poor Gaining? CAPRi Working Paper No. 92; International Food Policy Research Institute: Washington, DC, USA, 2008. [Google Scholar]
- Lachowycz, K.; Jones, A.P. Greenspace and Obesity: A Systematic Review of the Evidence. Obes. Rev. 2011, 12, e183–e189. [Google Scholar] [CrossRef]
- Coombes, E.; Jones, A.P.; Hillsdon, M. The Relationship of Physical Activity and Overweight to Objectively Measured Green Space Accessibility and Use. Soc. Sci. Med. 2010, 70, 816–822. [Google Scholar] [CrossRef]
- Ferraro, P.J.; Hanauer, M.M. Through What Mechanisms Do Protected Areas Affect Environmental and Social Outcomes? Philos. Trans. R. Soc. B Biol. Sci. 2015, 370, 20140267. [Google Scholar] [CrossRef]
- Kusumaning Asri, A.; Lee, H.-Y.; Pan, W.-C.; Tsai, H.-J.; Chang, H.-T.; Candice Lung, S.-C.; Su, H.-J.; Yu, C.-P.; Ji, J.S.; Wu, C.-D.; et al. Is Green Space Exposure Beneficial in a Developing Country? Landsc. Urban Plan. 2021, 215, 104226. [Google Scholar] [CrossRef]
- Potschin, M.B.; Haines-Young, R.H. Ecosystem Services: Exploring a Geographical Perspective. Prog. Phys. Geogr. Earth Environ. 2011, 35, 575–594. [Google Scholar] [CrossRef]
- Mace, G.M.; Norris, K.; Fitter, A.H. Biodiversity and Ecosystem Services: A Multilayered Relationship. Trends Ecol. Evol. 2012, 27, 19–26. [Google Scholar] [CrossRef]
- Díaz, S.; Demissew, S.; Carabias, J.; Joly, C.; Lonsdale, M.; Ash, N.; Larigauderie, A.; Adhikari, J.R.; Arico, S.; Báldi, A.; et al. The IPBES Conceptual Framework—Connecting Nature and People. Curr. Opin. Environ. Sustain. 2015, 14, 1–16. [Google Scholar] [CrossRef]
- Markevych, I.; Schoierer, J.; Hartig, T.; Chudnovsky, A.; Hystad, P.; Dzhambov, A.M.; de Vries, S.; Triguero-Mas, M.; Brauer, M.; Nieuwenhuijsen, M.J.; et al. Exploring Pathways Linking Greenspace to Health: Theoretical and Methodological Guidance. Environ. Res. 2017, 158, 301–317. [Google Scholar] [CrossRef]
- Wolf, K.L.; Lam, S.T.; McKeen, J.K.; Richardson, G.R.A.; van den Bosch, M.; Bardekjian, A.C. Urban Trees and Human Health: A Scoping Review. Int. J. Environ. Res. Public Health 2020, 17, 4371. [Google Scholar] [CrossRef]
- Marselle, M.R.; Hartig, T.; Cox, D.T.C.; de Bell, S.; Knapp, S.; Lindley, S.; Triguero-Mas, M.; Böhning-Gaese, K.; Braubach, M.; Cook, P.A.; et al. Pathways Linking Biodiversity to Human Health: A Conceptual Framework. Environ. Int. 2021, 150, 106420. [Google Scholar] [CrossRef]
- Wright, J.H.; Hill, N.A.O.; Roe, D.; Rowcliffe, J.M.; Kümpel, N.F.; Day, M.; Booker, F.; Milner-Gulland, E.J. Reframing the concept of alternative livelihoods. Conserv. Biol. 2016, 30, 7–13. [Google Scholar] [CrossRef]
- Fisher, B.; Herrera, D.; Adams, D.; Fox, H.E.; Gallagher, L.; Gerkey, D.; Gill, D.; Golden, C.D.; Hole, D.; Johnson, K.; et al. Can Nature Deliver on the Sustainable Development Goals? Lancet Planet. Health 2019, 3, e112–e113. [Google Scholar] [CrossRef]
- World Health Organization. Basic Documents: Forty-Ninth Edition (Including Amendments Adopted up to 31 May 2019); World Health Organization: Geneva, Switzerland, 2020. [Google Scholar]
- Ferraro, P.J.; Hanauer, M.M. Advances in Measuring the Environmental and Social Impacts of Environmental Programs. Annu. Rev. Environ. Resour. 2014, 39, 495–517. [Google Scholar] [CrossRef]
- Martin-Shields, C.P.; Stojetz, W. Food Security and Conflict: Empirical Challenges and Future Opportunities for Research and Policy Making on Food Security and Conflict. World Dev. 2019, 119, 150–164. [Google Scholar] [CrossRef]
- Minoiu, C.; Shemyakina, O.N. Armed Conflict, Household Victimization, and Child Health in Côte d’Ivoire. J. Dev. Econ. 2014, 108, 237–255. [Google Scholar] [CrossRef]
- Darrouzet-Nardi, A.F. Nonviolent Civil Insecurity Is Negatively Associated with Subsequent Height-for-Age in Children Aged <5 y Born between 1998 and 2014 in Rural Areas of Africa. Am. J. Clin. Nutr. 2017, 105, 485–493. [Google Scholar] [CrossRef]
- Wagner, Z.; Heft-Neal, S.; Bhutta, Z.A.; Black, R.E.; Burke, M.; Bendavid, E. Armed Conflict and Child Mortality in Africa: A Geospatial Analysis. Lancet 2018, 392, 857–865. [Google Scholar] [CrossRef]
- Mansour, H.; Rees, D. Armed Conflict and Birth Weight: Evidence from the al-Aqsa Intifada. J. Dev. Econ. 2012, 99, 190–199. [Google Scholar] [CrossRef]
- Li, J.; Yamazaki, K.; Ito, T. Probing Indirect Effects of Civil Conflict on Child Health in Non-Conflict Zones: Evidence from Sri Lanka; Graduate School of International Cooperation Studies; Kobe University: Kobe, Japan, 2019; p. 27. [Google Scholar]
- Tsujimoto, T.; Kijima, Y. Effects of Conflict on Child Health: Evidence from the 1990–1994 Northern Mali Conflict. Health Econ. 2020, 29, 1456–1474. [Google Scholar] [CrossRef]
- Bridges, S.; Scott, D. Early Childhood Health during Conflict: The Legacy of the Lord’s Resistance Army in Northern Uganda. Oxf. Bull. Econ. Stat. 2022, 84, 694–718. [Google Scholar] [CrossRef]
- Goli, S.; Mavisakalyan, A.; Rammohan, A.; Vu, L. Exposure to Conflict and Child Health Outcomes: Evidence from a Large Multi-Country Study. Confl. Health 2022, 16, 52. [Google Scholar] [CrossRef]
- Grace, K.; Verdin, A.; Brown, M.; Bakhtsiyarava, M.; Backer, D.; Billing, T. Conflict and Climate Factors and the Risk of Child Acute Malnutrition among Children Aged 24–59 Months: A Comparative Analysis of Kenya, Nigeria, and Uganda. Spat. Demogr. 2022, 10, 329–358. [Google Scholar] [CrossRef]
- Kreif, N.; Mirelman, A.; Suhrcke, M.; Buitrago, G.; Moreno-Serra, R. The Impact of Civil Conflict on Child Health: Evidence from Colombia. Econ. Hum. Biol. 2022, 44, 101074. [Google Scholar] [CrossRef]
- Le, K.; Nguyen, M. The Impacts of Armed Conflict on Child Health: Evidence from 56 Developing Countries. J. Peace Res. 2023, 60, 243–257. [Google Scholar] [CrossRef]
- Naidoo, R.; Johnson, K. Community-Based Conservation Reduces Sexual Risk Factors for HIV among Men. Glob. Health 2013, 9, 27. [Google Scholar] [CrossRef]
- Li, Z.; Kim, R.; Vollmer, S.; Subramanian, S.V. Factors Associated with Child Stunting, Wasting, and Underweight in 35 Low- and Middle-Income Countries. JAMA Netw. Open 2020, 3, e203386. [Google Scholar] [CrossRef]
- Flores, E.C.; Brown, L.J.; Kakuma, R.; Eaton, J.; Dangour, A.D. Mental Health and Wellbeing Outcomes of Climate Change Mitigation and Adaptation Strategies: A Systematic Review. Environ. Res. Lett. 2024, 19, 014056. [Google Scholar] [CrossRef]
- Weston, P.; Hong, R.; Kaboré, C.; Kull, C.A. Farmer-Managed Natural Regeneration Enhances Rural Livelihoods in Dryland West Africa. Environ. Manag. 2015, 55, 1402–1417. [Google Scholar] [CrossRef]
- Halla, T.; Holz, J.; Karhunkorva, R.; Laine, J. The Concept of the Human-Forest Relationship (HFR)–Definition and Potentials for Forest Policy Research. For. Policy Econ. 2023, 153, 102995. [Google Scholar] [CrossRef]
- Albrecht, G.; Sartore, G.-M.; Connor, L.; Higginbotham, N.; Freeman, S.; Kelly, B.; Stain, H.; Tonna, A.; Pollard, G. Solastalgia: The Distress Caused by Environmental Change. Australas Psychiatry 2007, 15, S95–S98. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
Types of variables explaining the effects of forests on health outcomes. (A) A mechanism: an intermediate outcome on the pathway between forests and a health outcome; (B) a moderator: outside the pathway but altering the magnitude or direction of the effects of forests on a health outcome (→: causal pathway).
Figure 1.
Types of variables explaining the effects of forests on health outcomes. (A) A mechanism: an intermediate outcome on the pathway between forests and a health outcome; (B) a moderator: outside the pathway but altering the magnitude or direction of the effects of forests on a health outcome (→: causal pathway).

Figure 2.
A conceptual framework for the moderating effects of means of access on the health impacts of forests. The means of access regulate the pathways between forests and health outcomes, resulting in heterogenous health impacts with equity implications.
Figure 2.
A conceptual framework for the moderating effects of means of access on the health impacts of forests. The means of access regulate the pathways between forests and health outcomes, resulting in heterogenous health impacts with equity implications.

Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the author. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
MDPI and ACS Style
Rasolofoson, R.A. Access to Human Health Benefits of Forests in Rural Low and Middle-Income Countries: A Literature Review and Conceptual Framework. Challenges 2024, 15, 12. https://doi.org/10.3390/challe15010012
AMA Style
Rasolofoson RA. Access to Human Health Benefits of Forests in Rural Low and Middle-Income Countries: A Literature Review and Conceptual Framework. Challenges. 2024; 15(1):12. https://doi.org/10.3390/challe15010012
Chicago/Turabian StyleRasolofoson, Ranaivo A. 2024. "Access to Human Health Benefits of Forests in Rural Low and Middle-Income Countries: A Literature Review and Conceptual Framework" Challenges 15, no. 1: 12. https://doi.org/10.3390/challe15010012
Note that from the first issue of 2016, this journal uses article numbers instead of page numbers. See further details here.